![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
130 Cards in this Set
- Front
- Back
|
Outline the 9 main aetiologies of malabsorption and give an archetypal example of each |
Unavailability of pancreatic enzymes Pancreatic insufficiency Unavailability of bile secretion Cholestasis Other stuff on the way Bacterial preabsorption Primary mucosal cell abnormalities Disaccharidases deficiency Reduced intestinal surface area Coeliac/Crohn's disease Lymphatic obstruction Lymphoma Infection Giardia lamblia Iatrogenic Gastrectomy Resection of small bowel |
|
|
Course of blood to and from the oesophageal varices |
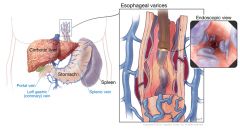
Portal vein ➙ Coronary (left gastric) veins ➙ Oesophageal vein ➙ Azygous veins ➙ vena cavae |
|
|
Course of blood to and from the caput medusae |
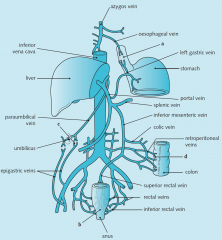
Portal vein ➙ Paraumbilical vein ➙ Superficial epigastric veins ➙ External iliac vein ➙ Common iliac vein ➙ IVC |
|
|
Name one factor that precipitates cirrhosis in liver diseases |
Binge drinking (this is the same that also precipitate hepatitis in alcoholic liver disease) |
|

Name the following sign, explain its pathogenesis and significance. |
Grey Turner's sign: Bleeding in the retroperitoneal space Indicative of damage to retroperitoneal organs. Typically due to acute pancreatitis wherein pancreatic enzymes digest blood vessels. |
|
|
2 early complications of acute pancreatitis |
Multi-organ failure (e.g. renal failure, ARDS) DIC (due to systemic inflammation) Sepsis Hypocalcaemia Hyperglycaemia |
|
|
What function of the pancreas is mostly affected by pancreatitis? |
Exocrine (digestive enzymes) |
|
|
3 signs and symptoms of chronic pancreatitis |
Non-acute epigastric pain radiating to the back relieved by sitting forward Bloating Steatorrhoea |
|

These red areas have been appearing at different places in the body and look inflamed. What is the name of the sign, its pathogenesis and its significance? |
Trousseau's sign of malignancy Due to thrombophlebitis (inflammation caused by thrombus) |
|
|
Three most likely cause of acute pancreatitis in the UK |
Gallstones (60%) Alcohol (20%) Idiopathic (10%) |
|
|
Four outcomes of acute pancreatitis |
Chronic pancreatitis Pancreatic necrosis Pancreatic abscess Pseudocyst (fluid filled cavity without epithelium) Resolution |
|
|
4 aetiologies of chronic pancreatitis |
(Thinks of alcohol and obstruction as the two aetiologies of acute pancreatitis) Chronic alcoholism Chronic duct obstruction Repeated acute pancreatitis Idiopathic |
|
|
3 stimuli of pancreatic exocrine function |
Secretin (secreted by the duodenum in response to acid) Cholecystokinin (secreted by the duodenum in response to fatty acids and amino acids) Acid, AA, peptides in duodenum |
|
|
Presentation of acute pancreatitis |
Sudden onset of severe epigastric pain radiating to the back relieved by sitting forward accompanied by vomiting (prominent) |
|
|
11 causes of pancreatitis |
I GET SMASHED Idiopathic Gallstones Ethanol Trauma Steroids Microorganisms (mostly viral: Coxsackie B, mumps, hepatitis, HIV) Autoimmune Scorpion stings Hypercalcaemia/hyperlipidaemia/hypothermia ERCP Drugs |
|
|
Name 3 drugs that may cause pancreatitis |
Furosemide (low volume ⇒ ischaemia) Corticosteroids Cimetidine (anti-H2) Antiretrovirals |
|
|
Name and compare two biochemical tests useful in diagnosing pancreatitis |
Amylase Peaks at 12 hours Returns to normal at 4 days Good specificity Average sensitivity Cheap Lipase (all x2) Peaks at 24 hours Returns to normal at 8 days Very good specificity Very good sensitivity Expensive |
|
|
High amylase and high lipase: 3 differential diagnosis |
Pancreatitis Intestinal obstruction Perforation |
|
|
What electrolytes disturbance may be observed in severe acute pancreatitis and why? |
Hypocalcaemia Pancreatic enzymes in the circulation damage fat cells which release TAGs. TAGs are then broken down to free FA by free pancreatic lipase in the circulation. Free FA have 2 negative charges and therefore bind calcium (precipitation of calcium). Note: hypercalcaemia is a cause of pancreatitis |
|
|
What imaging should be used in pancreatitis? |
USS of RUQ to check for stones (if AST raised) CT to monitor progression and check for potential carcinoma |
|
|
Where should the stone be to cause pancreatitis? |
At the sphincter of Oddi |
|
|
How would you assess the severity of acute pancreatitis? |
Glasgow criteria – PANCREAS (Notice that amylase is not part of it) PaO2 (< 8kPa due to respiratory failure) Age (> 55) Neutrophilia Calcium (Low due to binding to free FA but watch out for correction due to low albumin) Renal function (High urea due to possible thrombus in the renal artery and dehydration secondary to chemical burn oedema) Enzymes (High LDH as it is present in pancreatic cells and high AST if there is a stone) Albumin (Low due to malabsorption) Sugar (High blood glucose due to low insulin) |
|
|
Name 4 physical signs of acute pancreatitis |
Grey Turner's sign (digestion of blood vessels) Cullen's sign (same as Cullen but ventrally) Tachycardia Fever Jaundice Tenderness in abdomen Shock Ileus |
|
|
What investigations would you do to confirm pancreatitis and assess its severity? |
Amylase Then, think of Glasgow criteria: ABG Blood: FBC, U&E, Calcium, AST, LDH, Albumin BM |
|
|
What does U&E typically contain? |
Urea Creatinine eGFR Potassium Sodium |
|
|
Outline the management of pancreatitis |
1. Assess severity with Glasgow score 2. NBM and NG tube 3. IVI with lots of saline to counter third-space sequestration 4. Analgesia: pethidine* (morphine would contract the sphincter of Oddi more) 5. Monitor: BP, HR, PaO2 6. ERCP for gallstone removal |
|
|
It is often said that pancreatitis causes third-spacing. What do you understand by this and what causes it in pancreatitis? |
Third space is the transcellular space wherein fluid does not usually accumulate (e.g. peritoneal cavity). |
|
|
What analgesia should be given in acute pancreatitis? |
Pethidine (an opioid) |
|
|
Two complications of chronic pancreatitis |
Diabetes mellitus Malabsorption |
|
|
5 RF for pancreatic tumour |
Smoking Alcohol High fat diet Diabetes mellitus Chronic pancreatitis |
|
|
How is the presentation of pancreatic cancer related to its location |
Painless jaundice => Head Epigastric pain radiating to the back and relieved by sitting forward => Body or tail |
|
|
A patient presents with painless jaundice. You suspect pancreatic tumour but on examination, he has a palpable gallbladder. What is the diagnosis? |
It can still be pancreatic tumour. The gallbladder is typically palpable (My guess: swollen due to backflow due to obstruction) |
|
|
Name 4 physical signs of pancreatic tumour |
"Everything swells" Jaundice Palpable gallbladder Hepatomegaly Splenomegaly Lymphadenopathy Ascites |
|
|
What results do you expect to see in blood tests of pancreatic cancer? |
Cholestatic jaundice GGT raised ALP raised Conjugated bilirubin raised |
|
|
What specific blood test may you request to confirm the diagnosis of pancreatic cancer? |
CA 19-9 |
|
|
What initial imaging would you use in a patient in whom you suspect pancreatic cancer? |
USS (or CT) |
|
|
Which imaging would you use to confirm diagnosis of and assess staging of pancreatic cancer? |
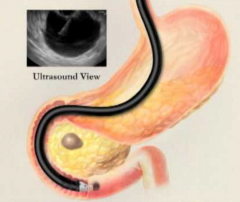
Endoscopic ultrasonography (EUS) |
|
|
When is pancreatoduodenectomy indicated? |
Consider in pPancreatic cancer with no mets and patient fit (but most won't be suitable) |
|
|
What is the most common management of pancreatic cancer? |
Palliative 1. Refer to palliative team 2. Stent to reduce jaundice 3. Big doses of opiates |
|
|
Lifetime incidence of appendicitis? |
6% |
|
|
How does appendicitis occur? |
Gut organisms invade the appendix wall after lumen obstruction (lymphoid hyperplasia, feacaloma, worms) |
|
|
Beside the characteristic pain, name two other features of the presentation of appendicitis. |
Anorexia Constipation (or sometimes diarrhoea) |
|
|
Name three specific tests that can be used to help the diagnosis of appendicitis |
Rebound tenderness Rovsing's sign Pain in RIF > Pain in LIF when LIF is pressed. Psoas sign Pain when extending the hip (if retrocaecal appendix) Cope sign Pain on flexion and internal rotation of the right hip |
|
|
Name two blood results expected in appendicitis |
Raised WCC (neutrophils) Raised CRP |
|
|
Name 3 signs of appendicitis elicited on general inspection |
All due to pain on moving: Pain on coughing Immobile Shallow breaths |
|
|
Course of action if suspected appendix |
Laparoscopic appendicectomy (20% will be false positives and removed anyway) + ABx pre-op (metronidazole) |
|
|
26 year old female presents with symptoms of appendicitis. Name 3 tests that you would do. |
FBC (raised neutrophils) CRP Pregnancy test Urinalysis (very important as UTI may mimic appendicitis) |
|
|
Three complications of appendicitis |
Perforation Appendix mass (inflamed appendix covered by omentum => Exclude colonic tumour) Appendix abscess (if appendix mass fails to resolve) |
|
|
A patient had symptoms of appendicitis 1 week ago but controlled it well with analgesia. He now presents to the hospital as he has higher fever and pain. His temperature is 38°C. Explain what may have happened. What would you do? |
Appendix abscess Try drainage (USS-guided) or ABx |
|
|
Why is the pain of the appendicitis initially located in the epigastric region? Why is it not lateralised? |
Viscera (and visceral peritoneum) have no somatic innervation. The brain associates the pain to a location whose dermatome corresponds to the same spinal level as the entry point of the C-fibres (from viscera). The C-fibres enter the spinal cord on both sides preventing any laterality and at multiple levels (=> Multiple dermatomes are possibly involved). |
|
|
What physical event causes the pain from appendicitis to move from periumbilical to McBurney's point? |
The peritoneum overlying the appendix gets progressively irritated. As long as only the visceral peritoneum is affected, the pain remains referred to periumbilicum (the visceral peritoneum does not have somatic innervation). |
|
|
Outline the separation of the foregut, midgut and hindgut and name their arterial supply, the main nerve and the location of the referred pain. |
Foregut – Proximal to D2 Coeliac trunk Greater splanchnic nerve => Epigastrium referral Midgut – D3 (distal to bile duct) to 2/3 of transverse colon SMA Lesser splanchnic nerve => Periumbilical referral Hindgut – 2/3 of transverse colon to upper anal canal IMA Lumbar splanchnic nerve => Suprapubic referral |
|
|
Explain one reason why appendicitis may present without pain at the specific location. What would you do then? |
Ectopic appendix: Retrocaecal (gas-filled caecum protects the appendix) Entirely within the pelvis |
|
|
Name 2 differential diagnosis of appendicitis in children |
Mesenteric adenitis* Meckel's diverticulitis* |
|
|
Name 5 differential diagnosis of appendicitis in adults |
Ectopic pregnancy Ovarian cyst Crohn's disease Meckel's diverticulitis Gastroenteritis Pancreatitis Renal colic |
|
|
Name 3 differential diagnosis of appendicitis in elderly |
Sigmoid diverticulitis Caecal tumour Caecal diverticulitis Ovarian tumour Ovarian cyst Ovarian infection |
|
|
Why should you do a DRE in patients with suspected appendicitis (2)? |
Elicit pain in ectopic appendix Rule out other differentials which may present with steatorrhoea due to malabsorption (pancreatitis, Crohn's coeliac) or with rectal bleeding (diverticulitis, tumour) |
|
|
How would you distinguish appendicitis from mesenteric adenitis? |
Mesenteric adenitis will usually present in children with history of recent viral illness and lymphadenopathy. |
|
|
Where is Meckel's diverticulum located? What is it the remnant of? |
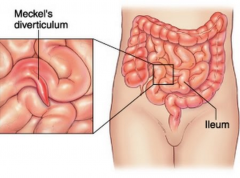
Distal ileum Remnant of the yolk sac |
|
|
Why can Meckel's diverticulum cause GI bleeding? What type of bleed does it cause? |
The yolk sac remnant may contain gastric and secrete gastric acid causing the bleed. Blood can be either bright red or occult. |
|
|
Name 3 complications of Meckel's diverticulum |
Haemorrhage (25%) Obstruction (25%) Diverticulitis (15%) |
|
|
Blood in the stool in a 2 year old boy but no haematemesis. Likely diagnosis? |
Meckel's divericulum |
|
|
Define hernia |
Abnormal protrusion of a viscus (singular of viscera) out of its normal cavity |
|
|
Surface anatomy of the deep inguinal ring |
Mid-point of the inguinal ligament (The mid-inguinal point is the femoral artery) |
|
|
How do we differentiate a direct from an indirect hernia. Explain the surface anatomy of any structure you name. |
1) Reduce hernia 2) Occlude deep ring with two fingers (mid-point of the inguinal ligament) 3) Ask pt to cough. If hernia pops out, then it’s a direct hernia |
|
|
What is the internal inguinal ring? |
A synonym of the deep inguinal ring The external ring is the superficial ring |
|
|
Which inguinal hernia is usually more present in children and younger adults? |
Indirect |
|
|
Which inguinal hernia is usually more present in elderly? |
Direct (weakness) |
|
|
Which inguinal hernia is usually more present in males? |
Both direct and indirect but more marked difference in indirect |
|
|
Which inguinal hernia is usually bilateral? |
Direct |
|
|
Which inguinal hernia is usually unilateral? |
Indirect |
|
|
Which inguinal hernia can be painful? |
Indirect |
|
|
Which inguinal hernia may extend in scrotum? |
Indirect (it goes down the inguinal canal) |
|
|
Which inguinal hernia can obstruct? |
Indirect |
|
|
Where do inguinal hernia originate? |
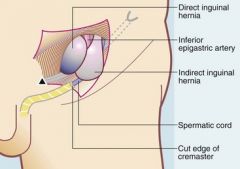
Indirect: Lateral to inferior epigastric artery Direct: Medial to inferior epigastric artery |
|
|
What is meant by incarceration of a hernia? |
Content of the hernial sac is stuck inside by adhesion |
|
|
What is meant by strangulated hernia? |
Ischaemia occurs (need for urgent surgery as the patient becomes toxic) |
|
|
Commonest abdominal hernia |
Inguinal hernia (and among them indirect are commonest–80%) |
|
|
Which inguinal hernia can obstruct is most common? |
Indirect |
|
|
Which inguinal hernia can strangulate? |
Indirect |
|
|
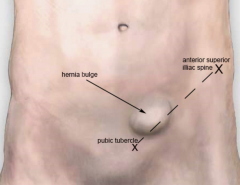
How can inguinal and femoral hernia be distinguished (3)? |
Location (#1) Femoral: neck is inferior to the inguinal ligament Inguinal: neck is superior to the inguinal ligament Orientation (#2) Femoral points down Inguinal points to the groin Gender (#3) Femoral are more likely in female Inguinal are more likely in guys. |
|
|
Name 5 characteristics of a hernia that you should elicit on examination |
Side Unilateral or bilateral Origin (neck) Reducibility Incarceration Obstruction Strangulation Note: Obstruction typically precedes strangulation (exception: Richter's hernia) Incarceration ⟹ Irreducible and painful Strangulation ⟹ Irreducible, painful and toxic |
|
|
Surface anatomy of the superficial inguinal ring |
1cm superior and medial to the pubic tubercle |
|
|
If you had to choose to have either a direct inguinal hernia, an indirect inguinal hernia or a femoral hernia, which one would you choose first, second and third and why? |
1. Direct inguinal hernia Rarely strangulate 2. Indirect inguinal hernia Can strangulate 3. Femoral hernia Often strangulate |
|
|
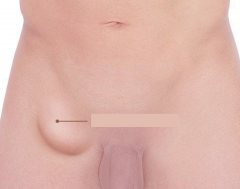
Name 5 differentials for a lump in the groin |
Femoral hernia Direct inguinal hernia Indirect inguinal hernia Saphena varix Lipoma Femoral aneurysm Psoas abscess |
|
|
Name two treatments that would be recommended/considered in femoral hernias |
Surgery recommended either as: 1. Herniotomy: ligation and excision 2. Hernia repair: repair of the hernial defect |
|
|
Inguinal hernia |
|
|
Femoral hernia |
|
|
Why may hernia occur in the femoral canal? |
Femoral canal is loose allowing the adjacent femoral vein to dilate during exercise enabling adequate blood return |
|
|
What forms the borders of the inguinal canal? |
Floor: inguinal ligament Roof: transverse abdominal muscle and internal oblique muscles Posterior wall: Transverse fascia (aponeurosis of transverse abdominis and parietal peritoneum) |
|
|
Content of the inguinal canal in males and females |
Ilioinguinal nerve Spermatic cord (males) - Vas deferens - Obliterated processus vaginalis - Lymphatics - Arteries to the vas, cremaster and testis - Pampiniform plexus and venous from vas, cremaster and testis - Genital branch of the genitofemoral nerve and sympathetic nerve Round ligament of the uterus (females) |
|
|
What forms the borders of the femoral canal? |
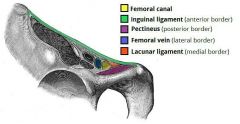
Anteriorly: Inguinal ligament Posteriorly: Pectineal ligament and pectineus (muscle for adduction of the leg) Medially: lacunar ligament and pubic bone Laterally: femoral vein |
|
|
Content of femoral canal |
CLoquet's lymph node Fat |
|
|
How do direct inguinal hernia occur (mechanism and predisposition)? |
Abdominal content pushes their way directly through the posterior wall of the inguinal canal. Predispositions: increased intraabdominal pressure (constipation, heavy lifting, obesity, chronic cough, ascites, urinary obstruction...) |
|
|
Why is it important to know how to differentiate between a direct and an indirect inguinal hernia? |
For OSCE. |
|
|
Why is it important to know how to differentiate between a reducible and an irreducible inguinal hernia? |
Irreducible require surgery |
|
|
What 3 information/advice should you impart to patients before surgical repair of inguinal hernias? |
Advice to diet (if over-weight) Stop smoking before operation Warn that hernias may recur (< 2%) |
|
|
What is the surgical approach to repair an inguinal hernia? |
Mesh repair |
|
|
What is an incisional hernia? How are they treated? |
Hernia caused by the breakdown of muscle closure after surgery (occurs in 10% of laparotomy) Mesh repair (✔︎ less recurrence ✘ more infection) Suture |
|
|
Name 4 factors that predispose to incisional hernia |
Wound infection (=> weaken the wall) Steroid use, anaemia, or malnutrition at the time of original surgery Midline laparotomy Poor surgical techniques in abdominal sutures |
|
|
When do incisional hernias occur after surgery? |
Up to 5 years after |
|
|
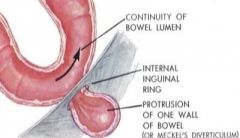
What is a Richter's hernia? |
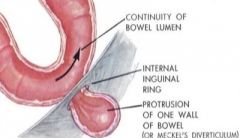
A hernia that involves only part of the bowel wall so that bowel obstruction (and its signs and symptoms) does not occur |
|
|
True or false: Richter's hernia are benign |
False, because they cannot lead to obstruction, they may present late when they result in strangulation and necrosis in the absence of obstructive symptoms. |
|
|
Outline the pathological mechanism that leads to strangulation. |
Venous and lymphatic occlusion ➙ oedema and raised venous pressure ➙ impeding arterial flow ➙ bowel necrosis andperforation |
|
|
Name and describe one surface anatomy area through which direct hernia pass. |
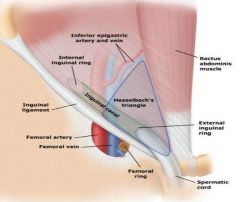
Hesselbach triangle Inguinal ligament Rectus muscle Epigastric artery |
|
|
Indication for the surgical repair of inguinal hernia |
Symptoms Episodes of irreducibility Bowelobstruction |
|
|
Name 4 cardinal features of intestinal obstruction (both large and small bowel) |
Constipation Colicky pain Vomiting Distension |
|
|
Characterise the obstruction in intestinal obstruction |
Solid only if proximal (~ small intestine) Absolute if distal (~ large intestine) |
|
|
Outline the timing of colic pain, distension and vomiting in intestinal obstruction. |
Colic pain – Early in obstruction then diseappears Vomiting – Occurs earlier if small bowel obstruction than large bowel Distension – Worsens with time (worse with large bowel obstruction) |
|
|
How can small and large bowel obstruction typically be differentiated? |
AXR |
|
|
Outline 5 differences between small and large bowels seen on AXR |

|
|
|
Outline how pain, vomiting, constipation and distension differ between small and large bowel obstruction |
Constipation: solid only in small bowel, everything in large (this is not clear cut) Pain: less constant in small bowel (peristalsis) and higher up Vomiting: occurs earlier in small bowel obstruction Distension: less bad in small bowel obstruction |
|
|
What two clinical features would point to ileus rather than mechanical obstruction? |
No pain Bowel sounds absent (no tinckling) |
|
|
Besides the location (small or large bowel) and the mechanism (functional or mechanical), what other question should you address in the clinical examination of bowel obstruction? |
Is the obstruction simple, closed loop or strangulated? Closed loop – Two point obstruction (e.g. volvulus) Strangulated – Blood supply is compromised and there is sharper more localised pain (peritonism) |
|
|
Besides cardinal signs of obstruction in general, what is the cardinal sign of strangulated obstruction specifically? |
Peritonism |
|
|
Two most likely causes of small bowel obstruction and four most likely causes of large bowel obstruction |
Small bowel Adhesions (#1) Hernia Large bowel Colon cancer (#1) Constipation Diverticular strictures Volvulus (sigmoid or caecal) |
|
|
What specific cause of small bowel obstruction should you suspect in a patient who has had a abdominal surgery (4)? |
Adhesions (even if surgery long in the past) Hernia (incisional) Paralytic ileus Pseudo-obstruction |
|
|
What specific cause of bowel obstruction should you suspect in a patient who has Crohn's disease? |
Crohn's stricture |
|
|
What specific cause of bowel obstruction should you suspect in a patient who has a history of gallstones? |
Gallstones ileus |
|
|
What specific cause of bowel obstruction should you suspect in a patient who is from the developing world? |
TB |
|
|
What is the mechanism of sigmoid volvulus? |
Sigmoid colon twists on its mesentery |
|
|
Complication of sigmoid volvulus |
Perforation => Peritonitis => Death |
|
|
Common treatment of sigmoid volvulus |
Sigmoidoscopy and insertion of a flatus tube |
|
|
What is the first line of management in intestinal obstruction? |
Drip and suck IV fluid to rehydrate and correct electrolyte imbalance (Drip) NGT (to empty – Suck) Analgesia Erect CXR and AXR Catheterise to monitor fluid balance Blood tests |
|
|
Outline the classic presentation of gastro-oesophageal obstruction |
Classic triad Vomiting (then retching) Pain Failed attempt to pass NGT |
|
|
How does acute vs chronic intestinal obstruction influence your differential diagnosis? |
Chronic is more likely to be functional (ileus or pseudo-obstruction) |
|
|
True or false: colonic pseudo-obstruction presents with no feature on AXR. |

False, the "pseudo" only refers to the absence of cause found. |
|
|
Distinguish paralytic ileus from pseudo-obstruction |
Paralytic ileus Established absence of peristalsis (e.g. after abdominal surgery, spinal injury, hypokalaemia, hyponatraemia, TCA...) Pseudo-obstruction Presents like a mechanical obstruction but without an identified cause. Predisposition: surgery, trauma, post-partum |
|
|
What specific cause of bowel obstruction should you suspect in a patient who has sustained spinal cord injury? |
Paralytic ileus |
|
|
What specific cause of bowel obstruction should you suspect in a patient who is hypokalaemic? |
Paralytic ileus |