![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
122 Cards in this Set
- Front
- Back
|
Name the three processes that cause airway obstruction in asthma. |
Bronchial muscle contraction (variety of modulators) Mucosal oedema caused by mast cell and eosinophil degranulation Increase mucus production |
|
|
Name 6 precipitants of asthma |
Cold air Exercise Allergens (dust mite, pollen, fur) – only in atopic Infections Smoking (including passive) Pollution NSAIDs Beta-Blockers |
|
|
When (during the day) is peak flow the lowest? |
In the morning (6AM). But asthma symptoms are worse at night due to exposure to dust mite, and other irritants)
|
|
|
Name 3 signs of moderate asthma |
Tachypnoea Hyperinflated chest Hyperresonant percussion note |
|
|
Name 3 signs of severe asthma |
Inability to complete sentences HR > 110 PEF < 50% predicted |
|
|
Name 3 signs of life-threatening asthma |
Silent chest Confusion Exhaustion Cyanosis (low PaO2 but PaCO2 normal or high) Bradycardia PEF < 33% predicted |
|
|
Relate HR to asthma |
Moderate => Normal/High Severe => High Life-threatening => Low |
|
|
How are the result of ABG in asthma |
Moderate - Alkalosis PO2 normal or ➘ PCO2 ➘ Severe - Mixed (early stage of respiratory failure) PO2 ➘ PCO2 normal Life-threatening - Respiratory acidosis PO2 ➘ PCO2 normal or ➚ (Remember that CO2 has a higher diffusivity at the exchange membrane) |
|
|
Significance of a normal PCO2 in a clearly asthmatic patient and management. |
Failing ventilatory effort => Transfer to ITU for ventilation |
|
|
What two tests would you do to diagnose chronic asthma? |
1. PEF monitoring (as diurnal variations exist) Dx: PEF variation > 20% on ≥3/7 for 2 weeks 2. Spirometry => Low FEV1/VC and raised RV (due to hyperinflation) and rising FEV1 following beta2 agonist |
|
|
What two findings do you expect on spirometry in asthma |
Low FEV1/VC High RV (residual volume) due to hyperinflation |
|
|
Name one common disease that is often associated with asthma |
Gastro-oesophageal reflux disease (GORD) |
|
|
Name the 4 pathological hallmarks of asthma |
Intermittent and reversible airway obstruction Chronic bronchialinflammation with eosinophils Bronchial smooth muscle cellhypertrophy and hyperreactivity Increased mucus secretion |
|
|
What is the pathological process of atopic asthma? |
Type I IgE–mediatedhypersensitivity reaction (That is the definition of atopy) |
|
|
What test can be done specifically in atopic asthma? |
Skin prick test |
|
|
What is the common pathway of atopic and non-atopic asthma? |
Humour and cellular mediators of bronchoconstriction (e.g. eosinophils) |
|
|
Pathogenesis of sensitisation phase of IgE-mediated allergy |
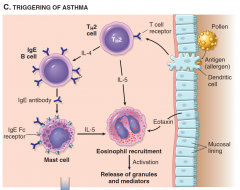
1. Allergen presented by APC |
|
|
Pathogenesis of re-exposure phase of IgE-mediated allergy |
1. Allergen cross-link on IgE mast cells and basophils 3. Immediate release of histamine |
|
|
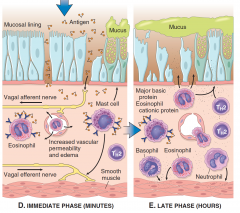
What is the late/chronic phase of IgE-mediated allergy? |
Long-acting mediators (leukotrienes, prostaglandins, PAF) attract more eosinophils, T-cells and other inflammation-mediating cells => Further inflammation. |
|
|
Name four aetiologies in asthma and their relative prevalence. |
Extrinsic Allergic – 60% Drug-induced (e.g. aspirin) – < 1% Intrinsic No obvious trigger – 30% |
|
|
What is status asthmaticus? |
Episodes of acute severe asthma that are not controlled by medication |
|
|
How does status asthmaticus present? |
Acute breasthlesness and wheeze |
|
|
What investigations would help you assess the severity of a status asthmaticus episode? |
PEF (but may be too ill) O2 Sats Ability to speak RR HR |
|
|
What 3 treatments should you start asap in status asthmaticus (also name the route of administration) |
Salbutamol nebulizer Hydrocortisone IV, Prednisolone PO or both |
|
|
Status asthmaticus is acute severe asthma. Besides treatment for status asthmaticus, what other 4 elements would you add to the management if there was features of life-threatening asthma? |
1. Inform ICU 2. Monitor ECG for arrhythmias 3. Add ipratropium (mAChR antagonist) in nebulizer (think "atropine" as ipratropium is a derivative of atropine) |
|
|
Name 4 side effects of salbutamol |
Tachycardia Arrhythmias Hypokalaemia |
|
|
What is the normal PO2 and PCO2 |
PaO2 > 10.6kPa PaCO2 in [4.7-6.0] kPa |
|
|
Name three genetic disorders that predispose to bleeding and three that predispose to thromboembolism |
Bleeding Haemophilia A Haemophilia B von Willebrand disease Thrombosis Factor V Leiden Protein S deficiency |
|
|
Name an inflammatory mediator that is well recognised to play a role in asthma and is a target for drugs in common use. |
Leukotriene |
|
|
What persistent abnormality can be seen on a FBC in asthma? |
Persistent eosinophilia |
|
|
Name 3 conditions of each of the following: |
Respiratory acidosis Any failure of ventilation (MG, ALS, GBS, Muscular dystrophy, life-threatening asthma, COPD) Respiratory alkalosis Anxiety, Pain, High altitude |
|
|
Management of tension pneumothorax |
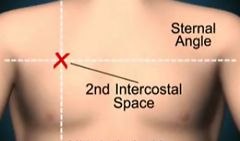
Large (14-16G) needle with a syringe partially filled with saline into the 2nd intercostal space in the midclavicular line on the suspected side.
|
|
|
Name two actions that need to be taken before discharging a (now stable) patient who has sustained an episode of life threatening asthma. |
Check inhaler technique with her Make a GP appointment within 1 wk |
|
|
You have given a patient with life threatening asthma salbutamol and ipratropium nebulizer, hydrocortisone IV, prednisolone PO, O2, and MgSO4. What two other treatments may you consider while waiting for ICU admission? |
Aminophylline IV salbutamol |
|
|
Name 3 complications of asthma |
Pneumonia (in particular, consider Aspergillus) |
|
|
What sign related to BP can be found in severe asthma? |
Pulsus paradoxus (SBP decreases by >10mmHg during inspiration) |
|
|
What is pulsus paradoxus ? Name 3 situation when it occurs |
SBP decreases by >10mmHg during inspiration |
|
|
Explain why SBP decreases on inspiration. |

|
|
|
Mechanism of pulsus paradoxus |
Pressure equalizes between all the chambers of the heart ⟹ Right ventricle gets more volume ⟹ Further reduction of the volume of the left ventricle ⟹ Cardiac output ➘ ⟹ Further decline in BP |
|
|
Name 3 behavioural components of the management of chronic asthma |
- Help quit smoking - Avoid precipitants - Educate to use peak flow meter - Educate to enable self-management to alter medication in regard to PEF - Give instructions about what to do in an emergency |
|
|
Outline the medical management of chronic asthma |
Stage 1 – β2-agonists PRN Stage 2 – Add steroids inhaled Stage 3 – Add long-acting β2-agonist Stage 4 – Test other stuff (increase steroid dose, theophylline, oral β2-agonist, oral leukotriene receptor antagonist) Stage 5 – Add prednisolone PO OD |
|
|
Name three "mechanical" treatments that can (possibly, i.e. it's in the syllabus but pretty much nowhere else) be used in status asthmaticus. |
Mucolytics (although it's mostly used in COPD) Humidification Physiotherapy |
|
|
Name 5 types of pleural effusion based on their content. |
Transudate (fluid with little proteins) Exudate (fluid with proteins) Haemothorax (blood) Haemopneumothorax (blood and air) Empyema (pus) Chylothorax (lymph with fat) |
|
|
Name 5 causes of transudates and 5 causes of exudates pleural effusion |
Transudates (Think Starling's forces) Infection (Pneumonia, TB) Inflammation (Pulmonary infarction, RA, SLE) Malignancy (Lung carcinoma, mets, lymphoma, mesothelioma) |
|
|
What are the two possible clinical presentations of pleural effusion? |
1) Asymptomatic (Same as pneumothorax) |
|
|
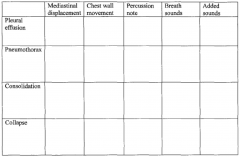
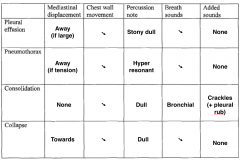
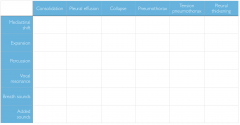
Name 4 signs of pleural effusion on examination |
Decreased chest expansion Stony dull percussion note Diminished breath sounds Decreased vocal resonance (and tactile vocal fremitus) – Unreliable - Bronchial breathing above the effusion - Tracheal deviation if severe - Signs of underlying cause (heart failure, malignancy, SLE...) |
|
|
What signs of lung malignancy can be elicited on examination? |
Cachexia Clubbing Lymphadenopathy Radiation marks Mastectomy scar (if breast mets) |
|

|
Pneumothorax |
|
|
Pleural effusion |
|
|
How is a pneumothorax distinguished from a pneumonia on a CXR? |

Presence of bronchogram in pneumonia |
|
|
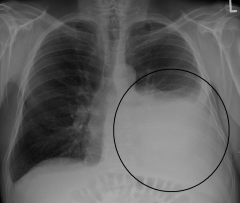
The following conditions may present as a white area on a CXR. Name one distinguishing features of each. - Pleural effusion - Consolidation - Pneumonectomy - Lung collapse |
- Pleural effusion: necessarily at the bottom, blunt costophrenic angles - Pneumonectomy: Bone fractures and damage due to operation - Lung collapse: otherwise |
|
|
Besides CXR to confirm its presence, what other imaging modalities can be used in a pleural effusion. What's its value? |
USS to guide diagnostic or therapeutic aspiration |
|
|
Outline the diagnosis process of pleural effusion |
1. Examination 3. Diagnostic aspiration: identify area by percussion or USS, draw 10-30mL and send to the lab for: - Biochemistry (protein, glucose, pH, LDH, amylase) - Cytology - Immunology if indicated (for RA, ANA, complement) |
|
|
A patient with pleural effusion confirmed on CXR has an inconclusive pleural aspiration. What is the next line of investigation? |
Pleural biopsy (parietal pleura) |
|
|
What is the indication for drainage of a pleural effusion? |
Symptomatic |
|
|
Name 4 features of pleural effusion expected on CXR |
- Blunting of the costophrenic angle - Blunting of the cardiophrenic angle - Fluid within the horizontal or oblique fissures - Meniscus (curved upper surface of a liquid in a tube) - Mediastinal shift away from the effusion (if large) |
|
|
Name two conditions in which cytological analysis of pleural effusion reveals raised neutrophils. |
Infection (pneumonia, abscess, bronchiectasis) PE |
|
|
Name two conditions in which cytological analysis of pleural effusion reveals raised lymphocytes. |
Malignancy RA SLE Sarcoidosis |
|
|
Name one condition in which cytological analysis of pleural effusion reveals raised mesothelial cells. |
Pulmonary infarction (Note: mesothelioma would present with abnormal mesothelial cells but not raised) |
|
|
Define chronic bronchitis |
Chronic cough producing of sputum for 3 months/year, for 2 years |
|
|
What two diseases form COPD |
Emphysema Chronic bronchitis |
|
|
What is the PaO2, PaCO2, RR, respiratory drive and underlying disease in the pink puffer COPD patient? |
PaO2 - normal PaCO2 - normal or low RR - high Hypercapnic drive Emphysema |
|
|
What is the PaO2, PaCO2, RR, respiratory drive and underlying disease in the blue bloater COPD patient? |
PaO2 - low PaCO2 - high RR - normal Hypoxic drive Chronic bronchitis |
|
|
Define emphysema |
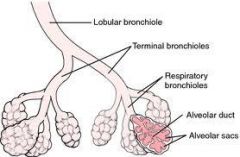
Abnormal permanent dilation and wall destruction of the air space distal to the terminal bronchiole |
|
|
Asthma and COPD somehow present similarly. Name 3 features of the history that may favour COPD. |
Age of onset ≥ 35 Smoking Chronic dyspnoea Minimal FEV1 variation (diurnal or day-to-day) Sputum production |
|
|
Name 4 symptoms of COPD |
Dyspnoea Cough |
|
|
Name 4 signs of COPD |
Tachypnoea Use of accessory muscles Hyperinflation Decreased cricosternal distance (< 3cm) Decreased expansion Resonant of hyperresonant percussion note Quiet breath sounds Wheeze Cyanosis Cor pulmonale |
|
|
Name one cause of COPD exacerbation |
Infection |
|
|
Besides exacerbations, name 4 complications of COPD |
Bronchiectasis Emphysema Cor pulmonale Pneumothorax Lung carcinoma |
|
|
Name one sign of COPD on FBC |
Polycythaemia |
|
|
In what direction would the following lung function variables be in COPD: FEV1, FEV1/FVC, TLC, RV? Which ones are measurable with spirometry? |
Measured by spirometry: FEV1 ➘ FEV1/FVC ➘ Others: TLC ➚ RV ➚ |
|
|
What is the target Sats in a healthy individual and in COPD? |
Healthy: 94-98% |
|
|
How is the severity of COPD staged? |
FEV1 as a percentage of predicted |
|
|
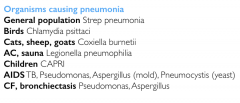
In the following groups of patients, which organism should be considered causative of pneumonia: - General population - Birds owner - Cats, sheep, goats owners - Exposure to AC and sauna - Children - AIDS - CF and Bronchiectasis |
|
|
|
A 7 year old is receiving ABx for pneumonia but is not improving. He had the flu 2 weeks ago which led to the pneumonia. What is the possible reason for his lack of improvement? |
Community-acquired MRSA pneumonia |
|
|
How do we typically establish that pneumonia was hospital acquired and not community acquired? |
> 48h after admission => Hospital acquired |
|
|
Most common organisms for HAP |
Gram negative enterobacteria (e.g. Klebsiella pneumoniae) |
|
|
3 conditions at risk of aspiration pneumoniae |
Stroke Decreased consciousness (e.g. drunk) Myasthenia gravis Bulbar palsies Oesophageal diseases (achalasia, reflux) |
|
|
Name two indications for bronchoalveolar lavage |
Pneumonia in ITU patient Immunocompromised Suspected malignancy Interstitial lung disease (e.g. sarcoidosis) |
|
|
Name and describe one score used to established the severity of pneumonia |
CURB-65 Confusion Urea RR > 30 BP < 90 systolic 65 (age)
≥ 3 => Admit |
|
|
What is the significance of raised urea in pneumonia? |
Sign of dehydration |
|
|
Outline the ABx you would use for CAP and HAP |
CAP: Amoxicillin + Clarithromycin (if ≥ moderate) HAP: Co-amoxiclav |
|
|
Name 4 possible complications of pneumonia |
Empyema Pleural effusion Lung abscess Respiratory failure Septicaemia Respiratory acidosis |
|
|
What can be the ABG results in a patient with pneumonia? |
Respiratory acidosis (if severe) |
|
|
A patient with unresolving pneumonia has now developed a new heart murmur. What may have happened? |
Septicaemia => metastatic infection (endocarditis in this case) |
|
|
A patient with unresolving pneumonia has now developed jaundice. What may have happened? |
Septicaemia => cholestasis |
|
|
Broadly speaking, how do organisms causing lobar pneumonia differ from those causing bronchopneumonia? |
Bronchopneumonia: wider variety |
|
|
How do bronchopneumonia and lobar pneumonia differ in terms of aetiology? |
Lobar pneumonia: primary pneumonia Bronchopneumonia: secondary pneumonia (e.g. aspiration, cancer,...) |
|
|
What pattern of infection does aspiration pneumonia lead to? |
Bronchopneumonia |
|
|
How is the diagnosis of pneumonia confirmed? |
Chest X-ray and sputum culture |
|
|
How do bronchopneumonia and lobar pneumonia differ in terms of demographics? |
Bronchopneumonia: extremes of age (think secondary to cancer, aspiration...) |
|
|
Name 4 signs of pneumonia that can be elicited on inspection and palpation |
Tachycardia Tachypnoea Pyrexia Cyanosis Decreased chest expansion Dull percussion note |
|
|
Name 3 signs of pneumonia that can be elicited on auscultation |
Increased vocal resonance (or tactile vocal fremitus) Bronchial breathing Pleural rub Crepitations |
|
|
Graphically represent what is meant by bronchial breathing. When is it heard? |
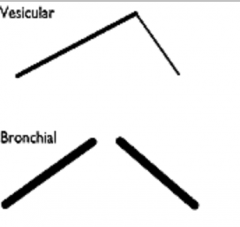
Consolidation or fibrosis |
|
|
Name three lifestyle factors that may contribute to pneumonia |
Immobility Smoking Malnutrition |
|
|
|
|
|
Name 4 conditions in which you may hear crepitations. For each, name one distinguishing feature. |
- Pulmonary oedema: Bilateral inspiratory fine - Pulmonary fibrosis: Bibasal coarse late inspiratory - Consolidation: Unilateral - Bronchiectasis: Bilateral coarse late inspiratory |
|
|
Significance of stridor |
Obstruction of airway in or near the larynx => Medical emergency |
|
|
Name 2 conditions in which you expect to hear pleural rub |
Pneumonia with pleurisy (NOT pleural effusion) |
|
|
Define respiratory failure |
Inability to maintain normal blood oxygen (PaO2 < 8kPa) |
|
|
Name the two types of respiratory failure and briefly outline the reason why they differ. |
Type 1 – PCO2 is normal because there is compensatory hyperventilation. |
|
|
Why can PCO2 be normal with PO2 low in respiratory failure compensated by hyperventilation? |
For 2 reasons: |
|
|
Name 5 causes of Type 1 respiratory failure (low PO2, normal PCO2) |
Think "compensated by hyperventilation" - Pneumonia - Pulmonary oedema - PE - Asthma (not life-threatening) - Emphysema - Pulmonary fibrosis - Acute respiratory distress syndrome |
|
|
Name 5 causes of Type 2 respiratory failure (low PO2, high PCO2) |
Reduced respiratory drive - Sedatives - CNS tumour Neuromuscular - Cervical cord lesion - Phrenic nerve damage - Polio - MG - GBS Lung diseases (typically end-stage, uncompensated ones): - COPD (blue bloater) - Life threatening asthma - End-stage pulmonary fibrosis - Severe pneumonia - Foreign body |
|
|
A three year old boy is found to have difficulty breathing, a barking cough and a fever. On examination, he is cyanosed and has a stridor. His blood gas reveals PO2 of 7.5kPa and PCO2 of 7.2kPa. Describe the blood gas results and name one diagnosis and explain the pathogenesis. |
Type 2 respiratory failure (PaCO2 is high) |
|
|
A patient of yours is found to have central cyanosis and is suspected to have respiratory failure. Name 4 signs or symptoms that would point towards Type 2 respiratory failure (PaCO2 high rather than normal). |
Signs and symptoms of hypercapnia: Headache Tachycardia Bounding pulse CO2 retention flap Papilloedema Confusion Drowsiness Peripheral vasodilation |
|
|
Outline the management of respiratory failure. |
1. Treat the underlying cause 2. O2 therapy: 2.1) Type 1: - Give 35-60% by facemask. - Assist ventilation if PaO2 < 8 kPa despite 60% O2. 2.2) Type 2 (hypoxia may be the only respiratory drive): - Start at 24% O2 - Recheck ABG after 20min. - If PaCO2 is steady or lower, increase O2 to 28% - If PaCO2 has risen, consider assisted ventilation - If all failed, consider intubation and ventilation or respiratory stimulant (e.g. doxapram) |
|
|
What is absolutely contraindicated in patients with respiratory failure? |
Sedatives |
|
|
Name 3 sites of primary tumour that metastasise to the lung. |
Breast/Prostate Kidney |
|
|
Most common aetiology of pneumothorax in a previously healthy young man |
Idiopathic |
|
|
What causes idiopathic pneumothorax (the end of the pathway) |
Rupture of a subpleural bulla |
|
|
Name 6 diseases that predispose to pneumothorax |
Asthma COPD TB Pneumonia Lung abscess Carcinoma CF Lung fibrosis Sarcoidosis Connective tissue disorders (Marfan's) |
|
|
Name 4 iatrogenic causes of pneumothorax |
Pleural aspiration Pleural biopsy Transbronchial biopsy Liver biopsy Positive pressure ventilation Subclavian CVP line insertion |
|
|
What are the two possible clinical presentations of pneumothorax? |
1) Asymptomatic 2) Pleuritic chest pain and dyspnoea (Same as pleural effusion more typically more sudden) |
|
|
Patient with asthma (or COPD) presents with a vey sudden deterioration of dyspnoea (but no fever or no extra sputum). What condition should you consider? |
Pneumothorax |
|
|
Name 5 signs of pneumothorax expected on examination |
The two that come for free: Reduced chest expansion Reduced breath sounds Hyperresonant percussion note Tracheal deviation (if tension) Decreased vocal resonance |
|
|
A patient who is mechanically ventilated suddenly becomes hypoxic. What should you consider as the potential cause? |
Pneumothorax |
|
|
Following examination, what is the course of action in a patient in whom you suspect pneumothorax? |
1) Suspected tension pneumothorax => Treat 2) Otherwise: expiratory CXR + ABG |
|
|
What happens if a tension pneumothorax is not treated promptly? |
Cardiovascular arrest |
|
|
Name 3 signs that would make you worry that the suspected pneumothorax is a tension pneumothorax |
Tracheal deviation away Tachycardia Hypotension Distended neck veins |
|
|
What is the indication for aspiration of a simple pneumothorax |
It depends whether the pneumothorax is primary or secondary. Primary pneumothorax Aspirate if SOB or Rim of air > 2cm on CXR Otherwise discharge. Secondary pneumothorax Drain if SOB and Age > 50 and Rim of air > 2cm on CXR Otherwise, aspirate. |
|
|

|