Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
61 Cards in this Set
- Front
- Back
|
Phases of healing and duration |
Inflammatory - 1-10 days - clotting and debris removal/bactieral elimination
Proliferative - 3-21 days - capillary buds and granulation tissue form; collagen matrix formed. Wound closed and skin integrity restored Maturation - 7 days to 2 years - fiber reorganization, scar tissue remodeling |
|
|
Newly repaired tissues have ___ % of original tensile integrity
|
15%
Up to 80% after maturation phase and full remodeling |
|
|
Primary intention
|
wound heals by edges touching each other. sutures, staples, or adhesives, or healing by epithelial migration.
Minimal scarring |
|
|
Secondary intention
|
Wounds close on their own without superficial closure.
When wound edges cannot be approximated due to infection debris, necrotic tissue, etc. These require ongoing wound care and often have larger scars than primary intention |
|
|
Tertiary Intention
|
Delayed primary intention
- wound temporarily left open then closed by primary intention |
|
|
Contaminated, colonized, or infected
|
Contaminated - non-replicating bacteria present. No additional tissue injury
Colonized - replicating bacteria on a wound surface that does not invade or further injure tissues. Does not stimulate inflammatory immune response Infection - replicating bacteria that invade viable tissue in and beyond the wound |
|
|
How to assess protective sensation
|
Failure to perceive 10 gm monofilament applied perpendicular to target area indicates loss of protective sensation
|
|
|
Arterial Insufficiency Ulcers
|
Result from inadequate circulation of oxygenated blood.
Recommendations: - Rest - Limb protection - Risk reduction education - Inspect legs and feet daily - Avoid unnecessary leg elevation - Avoid using heating pads or soaking feet in hot water - Wear appropriately sized shoes with clean, seamless socks - Lack granulation tissue; tend to be deep - Severe pain - Diminished or absent pedal pulses - Decreased skin temperature - Leg elevation increases pain - Hair loss |
|
|
Venous Insufficiency Ulcers
|
Inadequate circulation secondary to imparied functioning of the venous system leads to eventual tissue damage and ulceration.
- Proximal to medial malleolus - Irregular shape; shallow - Moderate/heavy exudate - Increased edema - Skin temperature normal - Leg elevation lessens pain |
|
|
Neuropathic Ulcers
|
Usually associated with a combination of ischemia and neuropathy, particularly in diabetes mellitus
- Good granulation tissue - Diminished or absent pedal pulses - Skin temperature decreased - Loss of protective sensation |
|
|
Superficial Wound
|
Epidermis intact
Ex. non-blistering sunburn Heals by inflammatory process |
|
|
Partial-thickness wound
|
Through epidermis and part of the dermis
Ex. Abrasions, blisters, skin tears Heals by re-epithelialization or epidermal resurfacing depending of depth of injury |
|
|
Full-thickness wound
|
Through epidermis, dermis, and into deeper tissues such as subcutaneous fat
Usually over 4 mm Heal by secondary intention |
|
|
Subcutaneous wound
|
Through integumentary tissues, involving deeper structures such as subcutaneous fat, muscle, tendon, or bone
Heal by secondary intention |
|
|
Wagner Ulcer Grade Classification Scale - for neuropathic, eschemic, or arterial etiology
|
0 - No open lesion, but may possess pre-ulcerative lesions; healed ulcers; presence of bony deformity
1 - Superficial ulcer not involving subcutaneous tissue 2 - Deep ulcer with penetration through subcutaneous tissue; potentially exposing bone, tendon, ligament, or joint capsule 3 - Deep ulcer with osteitis, abscess or osteomyelitis 4 - Gangrene of digit 5 - Gangrene of foot required disarticulation |
|
|
Pressure Ulcer Staging
|
Stage I - Intact skin with non-blanchable redness
Stage II - partial thickness tissue loss; shallow open ulcer with red or pink wound bed Stage III - Full thickness tissue loss with possible subcutaenous fat exposure. No bone, tendon, or muscle exposure Stage IV - Full thickness tissue loss with exposred bone, tendon, or muscle that is visible or directly palpable. Slough or eschar may be present Unstageable - Full thickness tissue loss with base of ulcer covered by slough and/or eschar. |
|
|
Don't remove eschar where?
|
On the heel
|
|
|
Components of wound examination and documentation
|
- Etiology
- Location - Wound type/classification - Clinical signs of infection - Area, depth, and shape of wound - Condition of wound margins/edges - Undermining or tunnelling - Involvement of underlying structures - Stage of healing - Color of base - Odor - Exudate type and volume - Chronicity - Response to previous tx - Surrounding skin/scar assessment - Presence of necrosis |
|
|
Hyperkeratosis
|
Callus
|
|
|
Which modalities have shown to improve wound healing?
|
Pulsed (non-thermal) ultrasound - used during inflammatory and proliferative phases. Enhances strength and elasticity of scar tissue
High-volt pulsed current - enhances healing for multiple types of wounds. Stiulates angiogenesis and epithelial migration Also - Negative pressure wound therapy (NPWT) - Hyperbaric Oxygen - Growth factors |
|

Hydrocolloids
|
Consist of gel-forming polymers backed by a strong film or foam adhesive.
Attaches to surrounding skin Used for partial and full-thickness wounds Advantages: - Provides a moist environment for wound healing - Enables autolytic debridement - Offers protection from microbial contamination - Provides moderate ABSORPTION - Does not require a secondary dressing - Provides a waterproof surface Disadvantages: - May traumatize surrounding intact skin upon removal - May tend to roll in areas of excessive friction - Cannot be used on infected wounds |
|

Hydrogels
|
Moisture-retentive and commonly used on superficial and partial-thickness wounds that have minimal drainage
- Moist environment - Cannot be used on wounds w significant drainage - Typically requires secondary dressing |
|

Foam Dressings
|
Provide protection and absorption over partial and full-thickness wounds with varying levels of exudate. Can be used as secondary dressings of hydrogels
- Moist environment - Protection and cushioning - Moderate absorption - May roll - May traumatize periwound area on removal - Lack of transparency makes wound inspection difficult |
|

Transparent film
|
- Water resistant
- Usfeful for superifical and partial-thickness wounds with minimal drainage - Moist environment - Allow visualization of the wound - Cost effective over time - May result in periwound maceration |
|

Gauze
|
- Used on infected or non-infected wounds of any size
- Can be wet-to-wet, wet-to-moist, wet-to-dry - Cost effective and available - Tendency to adhere to wound bed, traumatizing viable tissue on removal - Requires frequent dressing changes - Increased infection rate compared to occlusive dressings |
|

Alginates
|
- Derived from seaweed extraction
- Highly absorptive, highly permeable - Often used on infected wounds - May require frequent dressing changes depending on amount of exudate - Require a secondary dressing |
|
|
Sidelying - Bony Prominences
|
Ears
Acromion Lateral head of humerus Lateral epicondyle Greater trochanter Head of fibula Lateral malleolus Medial malleolus |
|
|
Supine - Bony Prominences
|
Occiput
Spine of scapula Inferior angle of scapula Vertebral spinous processes Medial epicondyle Posterior iliac crest Sacrum Coccyx Heel |
|
|
Prone - Bony Prominences
|
Forehead
Anterior portion of acromion Anterior head of humerus Sternum ASIS Patella Dorsum of foot |
|
|
Sitting - Bony prominences
|
Spine of scapula
Vertebral spinous processes Ischial tuberosities |
|
|
Exudate classifications
|
Serous - clear, watery. Normal
Sanguineous - red, watery. Indicates new blood vessel growth or disrution of blood vessels Serosanguineous - light red or pink, watery. Normal Seropurulent - cloudy or opaque. Yellow or tan, watery. Indicates impending infection Purulent - yellow or green, thick. Infection. |
|
|
Dressings - from most occlusive to non-occlusive
|
Hydrocolloids
Hydrogels Semipermeable film Semmipermeable foam Impregnated gauze Alginates Traditional gauze |
|
|
Dressings - from most to least moisture retentive
|
Alginates
Semipermeable foams Hydrocolloids Hydrogels Semipermeable films |
|
|
Contusion
|
Injury that does not disrupt skin integrity
Pain, edema, discoloration caused by blood seepage under surface of skin |
|
|
Dehiscence
|
Separation, rupture, or splitting of a wound closed by primary intention
|
|
|
Desquamation
|
Peeling or shedding of outer layers of epidermis. Normally occurs in small scales, although certain conditions, injuries, and medications may cause peeling in largrr scales or sheets and extend into deeper layers of skin
|
|
|
Ecchymosis
|
Discolration occuring below intact skin resulting from trauma to underlying blood vessels
Bruise |
|
|
Erythema
|
Diffuse redness of the skin often resulting from capillary dilation and inflammation
|
|
|
Friable
|
Tissue that readily tears, fragments, or bleeds
|
|
|
Hematoma
|
Localized swelling or mass of clotted blood confined to a tissue, organ, or space usually caused by a break in a blood vessel
|
|
|
Keloid
|

Abnormal scar formation comprised of irregularly distributed collagen bands. Typically exceeds boundaries of original wound appearing red, thick, raised, and firm
|
|
|
Maceration
|
Skin softening and degeneration that results from prolonged exposure to water or other fluids
|
|
|
Normotrophic scar
|
Scar with organized formation of collagen fibers that align in a parallel fashion
|
|
|
Turgor
|
The relative speed with which the skin resumes its normal appearance after being lightly pinched. An indicator of skin elasticity and hydration which normally occurs more slowly in older adults.
|
|
|
Zones of injury
|
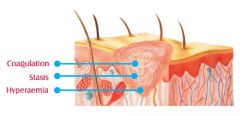
Zone of coagulation - irreversible cell damage
Zone of stasis - area of less severe injury with reversible damage Zone of hyperemia - inflammation |
|
|
Superficial Burn
|
Involves only epidermis. May be red with slight edema.
Heals in 2-5 days |
|
|
Superficial Partial-Thickness Burn
|
Epidermis and outer layer of dermis
Extremely painful. May blister Heals in 5-21 days with minimal to no scarring |
|
|
Deep Partial-Thickness Burn
|
Complete destruction of epidermis and majority of dermis
Blisters and edema Moderate levels of pain due to damaged nerve endings. Heals in 21-35 days and may scar |
|
|
Full-Thickness Burn
|
Complete destruction of epidermis and dermis, with partial damage to subcutaneous fat.
Typically presents with eschar and minimal pain Skin grafts required |
|
|
Subdermal burn
|
Through epidermis, dermis, and subcutaneous fat.
May involve muscle/bone |
|
|
Rule of 9's
|
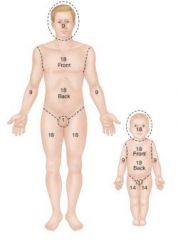
9 - Head and neck
18 - anterior trunk 18 - posterior trunk 9 - bilateral anterior or posterior arm (18 for total arms) 18 - bilateral anterior or posterior leg (36 total for legs) |
|
|
Child values - rule of 9's
|
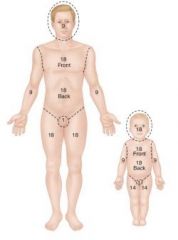
9% taken from LE and added to head and neck region.
Each year of life, 1% is distributed to the back en LE until age 9 when head is same proportion as adult. |
|
|
Compression Garments - Pressure and wearing schedule
|
15-35 mm Hg
Worn for 22-23 hours/day until the scar has matured |
|
|
Cellulitis
|
Fast spreading inflammation that occurs as a result of bacterial infection of the skin and connective tissues.
|
|
|
Contact Dermatitis
|
Superficial irritation of skin resulting from localized irritation (poison ivy, latex, etc)
|
|
|
Eczema
|

Also known as dermatitis
Chronic skin inflammation typicall due to an immune system abnormality, allergic reaction, or external irritant. |
|
|
Gangrene (dry)
|
loss of vascular supply resulting in local tissue death.
Hardened tissue is not painful, but may be painful along edges. Occurs in DM or atherosclerosis |
|
|
Gangrene (wet)
|
When there is a bacterial infection.
Can develop after a severe burn, frostbite, etc Requires immediate tx because it can spread quickly and be fatal. |
|
|
Onychomycosis
|

Fungal infection of toenails and nailbeds
|
|
|
Plaque Psoriasis
|

Chronic autoimmune disease
Skin cells accumulate in raised red patches on the skin |
|
|
Tinea Pedis
|

Athlete's foot
Superficial fungal infection which causes epidermal thickening and scaly skin appearance. |