Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
85 Cards in this Set
- Front
- Back
|
Neutrophils
|
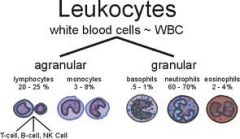
Help protect the body against infections by ingesting bacteria and debris
Normal count - 40-70% |
|
|
Lymphocytes
|
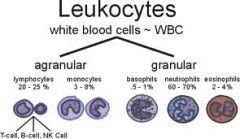
3 types
T lymphocytes & natural killer cells - help protect against viral infections and can detect and destroy some cancer cells B lymphocytes - develop into cells that produce antibodies Normal count - 20-50% |
|
|
Monocytes
|
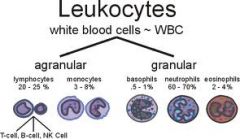
Ingest dead or damaged cells and help defend against infectious organisms
Normal count - 4-8% |
|
|
Eosinophils
|
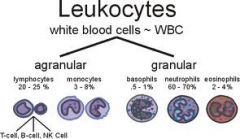
Kill parasites, destroy cancer cells, and are involved in allergic responses
Normal count - 0-6% |
|
|
Basophils
|
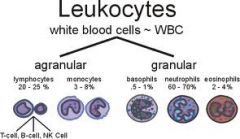
Participate in allergic responses
Normal count - 0-2% |
|
|
TLC
|
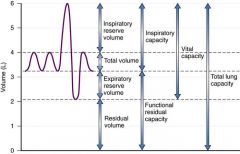
Total lung capacity = RV + VC
or TLC = FRC + IC |
|
|
FRC
|
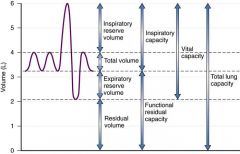
Functional residual capacity
Volume of air in lungs after normal exhalation = ERV + RV 40% |
|
|
IRV
|
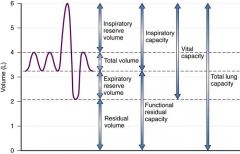
Inspiratory Reserve Volume
Maximal volume of air that can be inspired after normal tidal volume inhalation. 50% |
|
|
ERV
|
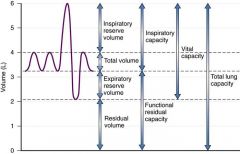
Expiratory Reserve Volume
Air that can be exhaled after normal tidal exhalation 15% |
|
|
VC
|
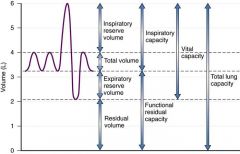
Vital capacity = ERV + TV + IRV
75% |
|
|
Blood pressure values for adults
|
Normal - <120/80
Pre - 120-139/80-89 Stage I HTN - 140-159/90-99 Stage II HTN - >160/100 |
|
|
pH
|
7.4 (7.35-7.45)
Acidemia - <7.35 Alkalemia - >7.45 |
|
|
PaCO2
|
40 mmHg at sea level breathing ambient air
(35-45) Eucapnia - normal CO2 Hypercapnia - >45 Hypocapnia - <45 |
|
|
PaO2
|
97 mmHG at sea level breathing ambient air
(80-100) Mild hypoxemia - 60-79 Moderate hypoxemia - 40-59 Severe hypoxemia - <40 |
|
|
HCO3-
|
24 mEq/L
(22-26) |
|
|
SaO2
|
95-98%
|
|
|
ABG
|
Arterial Blood Gas
Commonly written: pH/PaCO2/PaO2/HCO3 |
|
|
Hypoxia
|
Low O2 in tissues despite adequate perfusion of the tissue
|
|
|
Systematic Analysis of Arterial Blood Gas
|
STEP 1 - Examine pH to assess acid-base balance
STEP 2 - Examine PaCO2 as an indicator of ventilatory status STEP 3 - Interpret PaCO2 in relation to pH STEP 4 - Interpret HCO3- in relation to pH STEP 5 - Interpret PaO2 and SaO2 |
|
|
Erythrocyte Count
|
Males - 4.3-5.6 x 10^6/ml
Females - 4.0 - 5.2 x 10^6/ml |
|
|
Leukocyte Count
|
3.45-9.06 x 10^3/mm^3
|
|
|
Platelet Count
|
165-415x10^3/mm^3
|
|
|
Partial Thromboplastin Time (PTT)
|
26.3-39.4 sec
|
|
|
Hematocrit
|
Males - 38.8-46.4%
Females - 35.4-44.4% |
|
|
Hemoglobin
|
Males - 133-162 gm/dL
Females - 120-158 gm/dL |
|
|
Total Serum Cholesterol
|
<200 mg/dL - Desirable
200-239 - Borderline >240 - High |
|
|
LDL Cholesterol Levels
|
<100 mg/dL - Optimal
100-129 - Near optimal 130 - 159 - Borderline 160 - 189 - High '3E190 - Very High |
|
|
HDL cholesterol
|
<40 - Low
>60 - High |
|
|
Triglyceride levels
|
<150 mg/dL - Desirable
150-199 - Borderline 200 - 499 - High >500 - Very high |
|
|
BMI
|
Body Mass Index = weight (kg) / height (m ^ 2)
OR BMI = weight (lb) / height (in ^ 2) x 703 <18.5 = Underweight 18.5-24.9 - Normal 25.0 - 29.9 - Overweight 30.0 - 34.9 - Obesity (Class I) 35.0 - 39.9 - Obesity (Class II) >40.0 - Extreme obesity (Class III) |
|
|
Borg Dyspnea Scale
|
0 - No breathlessness
0.5 - Very, very slight 1 - Very slight 2 - Slight breathlessness 3 - Moderate 4 - Somewhat severe 5 - Severe breathlessness 6 7 - Very severe breathlessness 8 9 - Very, very severe breathlessness 10 - Maximal |
|
|
Prinzmetal (variant) angina
|
occurs due to coronary artery spasm most often associated with coronary artery disease
|
|
|
Angina pain pattern
|
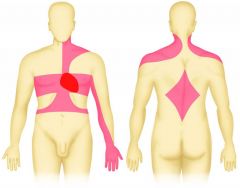
Usually described as pressure, heaviness, fullness, squeezing, burning, or aching behind the sternum
May also be felt in neck and back, jaw, shoulders, and arms. May involve difficulty breathing, nausea, vomiting, sweating, anxiety or fear Pain may not be felt until 70% of the lumen is occluded. |
|
|
Intermittent claudication
|
a clinical diagnosis given for muscle pain (ache, cramp, numbness or sense of fatigue) classically in the calf muscle, which occurs during exercise, such as walking, and is relieved by a short period of rest
|
|
|
Cardiomyopathy
|
Many causes including CAD, valvular heart disease
s/s - may be absent in early stages. Later -> breathlessness with exertion or even at rest, swelling of LE ankles or feet, abdominal distention, fatigue, irregular heartbeat, dizziness 3 Types: - Dilated - Hypertrophic - Restrictive |
|
|
Chronic Venous Insufficiency (CVI)
|
A condition in which the veins and valves in the lower extremity are damaged and cannot keep blood flowing toward the heart. This causes veins to remain filled with blood.
s/s - leg swelling, varicose veins, heaviness or cramping, itching, redness, skin ulcers Tx - compression stockings and elevation of legs |
|
|
Atrial Septal Defect (ASD)
|
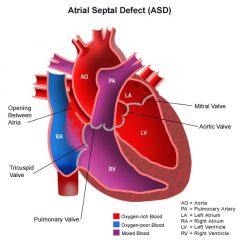
Hole in the wall separating the R and L atria. Failure of foramen ovale to close.
May be asymptomatic up to 30 years old. Surgical closure recommended if hole is large, heart is swollen, or symptoms occur. |
|
|
Coarcation of the aorta
|
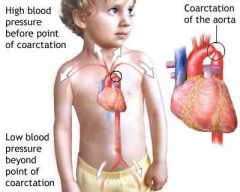
Congenital heart defect in which the aorta is narrowed near the ductus arteriosus.
Ranges from mild to severe and may not be detected until adulthood. s/s include SOB during exercise, intermittent claudication weakness, headache. High blood pressure in the arms, but low blood pressure in the legs. Tx usually consists of surgical repair or balloon angioplasty. |
|
|
Ductus arteriosus
|
A blood vessel connecting the pulmonary artery to the proximal descending aorta. It allows most of the blood from the right ventricle to bypass the fetus's fluid-filled non-functioning lungs. Upon closure at birth, it becomes the ligamentum arteriosum.
|
|
|
Patent ductus arteriosus (PDA)
|
Ductus arteriosus does not close after birth.
s/s - small could be asymptomatic; large - tacycardia, respiratory distress, poor eating, weight loss, CHF Non surgical tx for small hole include diuretics and idomethacin. Large may require surgical repair |
|
|
Ventricular septal defect (VSD)
|
Hole in R/L ventricles. If too large, extra blood will be pumped to the lungs, leading to heart failure.
Small defect - hole may eventually close Large - may cause cyanosis of skin, lips, fingernails, poor eating/failure to thrive, fast breathing or breathlessness, fatigue, swelling of legs, feet, or abdomen, rapid heart rate Tx - surgery |
|
|
Tetralogy of Fallot
|
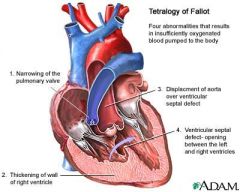
1) VSD
2) pulmonary stenosis 3) right ventricular hypertrophy 4) aorta overriding the ventricular septal defect Death or disability common by early adulthood. Tx - surgery to patch VSD and widen the pulmonary valve and arteries |
|
|
Cor Pulmonale
|
Also known as pulmonary heart disease
Hypertrophy of R ventricle caused by altered structure or function of the lungs. s/s - progressive SOB especially with exertion. Also fatigue, palpitations, atypical chest pain, swelling of LE, dizziness, syncope Tx - supplemental oxygen to maintain SaO2 >90% and or PaO2 >60mmHg. Diuretics and anticoagulation |
|
|
Endocarditis
|
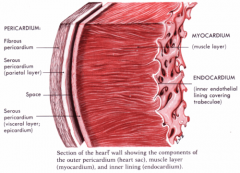
Inflammation of endothelium that lines that heart and cardiac valves.
Can damage or destroy valves and become life-threatening. Caused by bacteria from catheters, needles, dental procedures, gum disease, STD, or inflammatory bowel disease. Tx - antibiotics and potential surgery to repair damaged heart valve |
|
|
Myocarditis
|
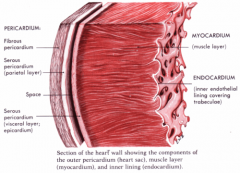
Inflammation and weakness of the myocardium. It can become thick and swollen, which can lead to symptoms of heart failure.
Usually caused by viral or bacterial infection. |
|
|
Pericarditis
|
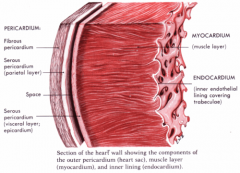
Inflammation of the pericardium
Often, fluid builds up between the inner and outer layers, resulting in pericardial effusion. Often, cases will clear up with rest and simple tx. More severe cases can lead to cardiac tamponadeq |
|
|
Exercise tx for peripheral artery disease
|
minimum of 30-45 minutes, at least 3x per week for minimum of 12 weeks
|
|
|
Rheumatic Fever
|
Inflammatory disease that can develop as a complication of untreated or poorly treated strep throat. Can damage the heart valves and cause heart failure.
|
|
|
ARDS
|
Acute Respiratory Distress Syndrome
Sudden respiratory failure due to fluid in the alveoli. Typically occurs in people who are already critically ill or who have significant injuries. Fatal in 25-50% Inflammation disrupts the integrity of alveolar wall causing fluid leakage First goal of tx is to get O2 to lungs and tissues |
|
|
Atelectasis
|
lung collapse in one or more areas
Caused by conditions that prevent deep breathing and coughing, such as post-op pain, pleural effusion, tumor, ARDS, asthma, COPD, and cystic fibrosis |
|
|
Bronchiectasis
|
Progressive obstructive lung disease that produces abnormal dilation of a bronchus. This is an irreversible condition usually associated with chronic infections, aspiration, cystic fibrosis, or immune system impairment. Th bronchial walls waken over time due to infection and allow for permanent dilation of bronchi and bronchioles.
|
|
|
Bronchitis
|
Ain't nobody got time for that
|
|
|
Bronchitis
|
Inflammation of the bronchi, with hypertrophy of mucus secreting glands, increased mucous production, and insufficient oxygenation due to mucus blockage
Acute or chronic |
|
|
COPD
|
Chronic Obstructive Pulmonary Disease
Emphysema + Chronic Bronchitis Impaired air flow and narrowing of bronchial tree Alveolar destruction and air trapping Increased TLC and RV |
|
|
Cystic Fibrosis
|
Autosomal recessive disease of the exocrine glands that primarily affects the lungs, pancreas, liver, intestines, sinuses, and sex organs.
Must inherit one faulty genes from each parent. Body produces thick, sticky mucous that leads to life-threatening lung infections, obstructs the pancreas, and inhibits normal digestion and absorption of food. |
|
|
Emphysema
|
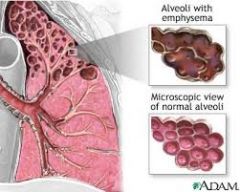
Destruction of alveolar walls
Elastic fibers that hold bronchioles open are destroyed, so that they collapse during exhalation, not letting air escape from the lungs. Increased dead space Primarily caused by smoking |
|
|
Pleural Effusion
|
Buildup of fluid in pleural space between lungs and chest cavity.
Can push against lungs making inhalation difficult, and in severe cases can cause atelectasis. If fluid gets infected it's called empyema. |
|
|
Pneumonia
|
Inflammation of lungs, typically caused by bacterial, viral, fungal, or parasitic infection.
|
|
|
Pulmonary edema
|
LIFE THREATENING MEDICAL EMERGENCY
When fluid collects in alveoli making it different to breathe. Often occurs when left ventricle is unable to pump properly. May also occur from pneumonia, toxin inhalation, ARDS s/s include - extreme SOB - a bubbly, wheezing or gasping sound during breathing - a cough that produces frothy sputum that may be tinged with blood - cyanotic skin color - rapid, irregular pulse - severe drop in BP |
|
|
s/s of pulmonary edema
|
- extreme SOB
- a bubbly, wheezing or gasping sound during breathing - a cough that produces frothy sputum that may be tinged with blood - cyanotic skin color - rapid, irregular pulse - severe drop in BP |
|
|
s/s of pulmonary embolism
|
sudden onset SOB,
chest pain that becomes worse with deep breathing, coughing, eating, or bending; coughing up bloody sputum, wheezing, LE swelling, excess sweating, rapid or irregular pulse, lightheadedness or fainting |
|
|
Prevention of pulmonary embolism
|
Compression stockings, pneumatic compression, physical activity, and drinking fluids
|
|
|
Pulmonary fibrosis
|
Microscopic damage to alveoli causes irreversible scarring of the interstitial tissue. This decreases lung elasticity, making breathing more difficult.
Most cases are idiopathic. However, can be caused by chronic exposure to irritants (silica dust, asbestos, grain dust, sugar cane, animal droppings) Lung scarring is irreversible |
|
|
Restrictive Lung Disease
|
An abnormal reduction in lung expansion and pulmonary ventilation.
Causes: - abnormal parenchyma (atelectasis, pneumonia, PF, pulmonary edema, ARDS), - abnormal pleura (pleural effusion, pleural fibrosis, pneumothorax, hemothorax) - disorders affecting ventilatory pump function (decreased respiratory drive, neurologic and neuromuscular diseases, muscle disease or weakness, thoracic deformity or trauma, connective tissue disorders affecting thoracic joints, pregnancy, obesity, ascites) |
|
|
Artery that supplies the right atrium
|
Sinus node artery
|
|
|
Artery that supplies the right ventricle
|

Right marginal artery
|
|
|
Supply the inferior walls of both ventricles
and inferior portion of the interventricular septum |

Posterior descending artery
|
|
|
Supplies left atrium, posterior and lateral walls of left ventricle, and anterior/inferior walls of left ventricle
|

Circumflex artery
|
|
|
Supply anterior portion of interventricular septum
|

Left anterior descending artery
|
|
|
Muscles of inhalation
|
Diaphragm (primary)
Internal/external intercostals - elevates the ribs, increases AP chest diameter, and elevation of lower ribs increases transverse diameter Also SCM, scalenes, pec major (sternocostal portion), pec minor, and serratus during high levels of ventilation |
|
|
Muscles of exhalation
|
Tidal breathing - exhalation results from passive recoil of lungs and rib cage.
Forceful breathing - rectus, internal/external oblique, and TrA depress lower ribs and compress abdominal contents, pushing diaphragm up |
|
|
Upper respiratory tract
|
Larynx and superior
|
|
|
Lower respiratory tract
|
Larynx and inferior
Airways divide ~23 times |
|
|
Baroreceptor Reflex
|
Maintains blood pressure
Low pressure (cardiopulmonary receptors) -> Sympathetic activation -> increased cardiac contractility, incrased HR, venoconstriction, arterial vasoconstriction, to increase cardiac output and peripheral resistance -> increased BP High blood pressure (arterial baroreceptors) -> parasympathetic activation -> decreased HR, small dec in contractility -> dec BP The Bainbridge reflex and the baroreceptor reflex act antagonistically to control heart rate. The baroreceptor reflex acts to decrease heart rate when blood pressure rises. When blood volume is increased, the Bainbridge reflex is dominant; when blood volume is decreased, the baroreceptor reflex is dominant. |
|
|
Bainbridge reflex
|
Increased venous return -> stretches receptors in R atrium -> afferent vagal signals -> medulla inhibits parasympathetic activity -> increased heart rate
The Bainbridge reflex and the baroreceptor reflex act antagonistically to control heart rate. The baroreceptor reflex acts to decrease heart rate when blood pressure rises. When blood volume is increased, the Bainbridge reflex is dominant; when blood volume is decreased, the baroreceptor reflex is dominant. |
|
|
Chemoreceptor reflex
|
Decreased pH (acidosis) or dec partial oxygen pressure leads to increased rate and depth of ventilation
|
|
|
Valsalva maneuver
|
Increases intrathoracic pressure, decreasing venous return. This decreases CO and BP
This is sensed by baroreceptors, which respond by increasing HR and contractility via sympathetic stimulation |
|
|
Cardiac conduction
|
|
|
|
Pacemaker Codes
|
I - Chamber Paced
V = ventricle; A = atrium; D = dual; O=none II - Chamber Sensed same III - Response sensed T = Triggered; I=Inhibited; D=dual, O = none IV - Rate modulation R - Rate modulation; O=none V - Multisite pacing V = ventricle; A=atrium; D=dual; O=none |
|
|
Artherectomy
|
similar to angioplasty but instead the catheter removes plaque with a rotating shaver
|
|
|
Cardiac Ablation
|
surgical procedure that uses radiofrequencies or chemicals to destroy areas of the myocardium that have been identified to be causing cardiac arrhythmia
|
|
|
Enhanced Extracorporeal Graft Surgery
|
Inflation of pressure cuffs on LEs compresses veins and assists w venous return to heart
|
|
|
Ventricular Assist Devices
|
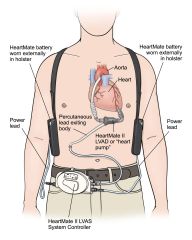
miniature pump that is implanted in the chest to provide mechanical support to the ventricle
|
|
|
Angina Pain Scale
|
1 - Mild, barely noticable
2 - Moderate, bothersome 3 - Moderately severe, very uncomfortable 4 - Most severe or intense pain ever experienced |
|
|
Ankle Brachial Index (ABI)
|
Compares systolic BP at ankle and arm to check for peripheral artery disease
Divide higher of two systolic LE BP measurements by higher of arm BP > 1.30 - rigid arteries and need for an ultrasound to check for PAD 1-1.3 normal, no blockage .8-.99 - mild, beginnings of PAD .4-0.79 - moderate block; may be associated with intermittent claudication during exercise <0.4 - severe blockage suggesting severe PAD; may have claudication pain at rest |