Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
75 Cards in this Set
- Front
- Back
|
What muscles are in the anterior compartment of the thigh? Innervation? Action?
|
IPSquad: Iliacus, Pectineus, Sartorius, Quads
- Femoral n. - Flex at hip and extend at knee |
|
|
What muscles are in the medial compartment of the thigh? Innervation? Action?
|
POAAAG: Pectineus, Obturator Ext., 3 Adductors, Gracilis
- Obturator n. - Adduct leg towards midline |
|
|
What muscles are in the posterior compartment of the thigh? Innervation? Action?
|
BSASB: Biceps long, Semitendinosus, Adductor Magnus, Semimembranosus, Biceps short
- Sciatic n. - Flexion at knee, extension at hip |
|
|
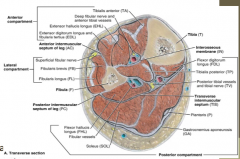
What muscles are in the posterior compartment of the lower leg? Innervation? Action?
|
PGPS(TFF): Popliteus, Gastroc, Plantaris, Soleus, Tib post, FDL, FHL
- Tibial n. - Flex at knee and plantarflex (stand on tip toes) |
|
|
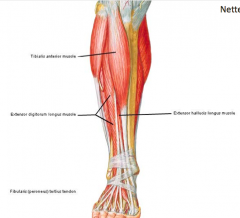
What muscles are in the anterior compartment of the lower leg? Innervation? Action?
|
TEEP(F)EE: Tib ant., EDL, EHL, Fib tertius, EDB, EHB
- Deep fibular nerve - Dorsiflex (walk on heels) |
|
|
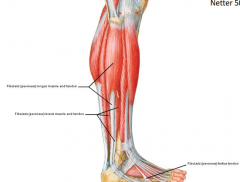
What muscles are in the lateral compartment of the lower leg? Innervation? Action?
|
FF: Fibularis long and Fibularis brev
- Superficial fibular n. - Evert ankle |
|
|
What muscles are intrinsic to the foot? Innervation?
|
- Medial Plantar n.: Abductor hallucis, Flexor digitorum brevis, Flexor hallucis brevis, most medial Lumbrical
- Lateral Plantar n.: all others |
|
|
Slipped Capital Femoral Epiphysis (SCFE):
- History - Etiology - Presentation - Treatment |

- History – classically an overweight early adolescent with history of groin or knee pain, which may be referred to anteromedial thigh. Often occurs bilaterally (but not simultaneously)
- Etiology – repetitive overload - Presentation – Vague symptoms, worse with activity. Limitation of internal rotation. - Treatments – plain x-rays, surgical fixation |
|
|
Transient Synovitis of the Hip:
- History - Etiology - Presentation - Treatment |
- History: Ages 3-10
- Etiology - usually viral, post-vaccine or drug-induced - Examination - usually hold hip slightly flexed & external rotation; resistance to abduction and internal rotation. Any motion at joint causes pain; child refuses to bear weight; otherwise looks okay - Treatment - Sed rate 35-60mm/hr & CBC - mild leukocytosis; NSAIDs for 1-3 wks |
|
|
Septic Joint:
- History - Etiology - Presentation - Treatment - Complication |
- History / Presentation
a) Swollen, extremely painful joint b) Passive & active ROM very painful c) Red, hot joint d) Usually has systemic signs, but may be absent in diabetic patient or immunosuppressed patient - Etiology - Gonorrhea or skin flora - Treatment - often requires surgical incision and drainage followed by IV antibiotics - Complication - articular surface destruction |
|
|
13 yo soccer player complains of knee pain; denies any known injury; pain to palpation of tibial tubercle and pain w/ resisted knee extension.
What is the underlying pathology? |
- Relative weakness of immature skeleton compared to the mature skeleton
- Osgood-Schlatter Condition |
|
|
What is the cause of Osgood-Schlatter Condition?
|
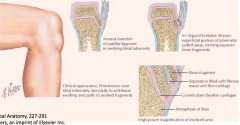
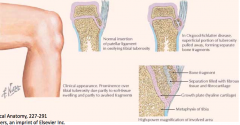
- Following an adolescent growth spurt, repeated stress from contraction of the quadriceps is transmitted through the patellar tendon to the immature tibial tuberosity.
- This can cause multiple partial avulsion fractures (pulling the tibial tuberosity away from tibia) - Also, inflammation of the tendon can lead to excess bone growth in the tuberosity and producing a visible lump which can be very painful, especially when hit |
|

What is seen in this image?
|
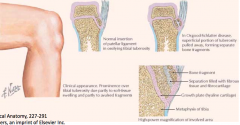
Osgood-Schlatter Disease (OSD) - tibial tuberosity elongated and fragmented, with overlying soft tissue swelling
|
|
|
What happens in Apophysitis?
|
- Pain and inflammation of ossification centers from repetitive tension
- E.g., Osgood-Schlatter Disease |
|
|
How should Apophysitis (e.g., Osgood-Schlatter disease) be treated?
|
- Activity as tolerated
- Stretching - Ice ± NSAIDs |
|
|
What are some common sites of Apophysitis?
|
- Tibial tubercle (Osgood-Schlatter)
- Calcaneus (Sever's) - Distal patellar pole (Sinding-Larsen-Johnson) - Sartorius (ASIS) - Rectus Femoris (AIIS) - Medial Epicondyle (little leaguer's elbow) |
|
|
What is the term for excessive fluid in a joint?
|
Effusion
|
|
|
What is the term for a synovial lined sac that contains fluid and acts to reduce friction between structures? Examples?
|
Bursa - Achilles, olecranon, subacromial, prepatellar, and other knee locations
|
|
|
What is the term for fluid filled soft tissue mass filled with a collection of synovial or peritendinous fluid that arises from a joint or tendon sheath? Example?
|

Ganglion
E.g., wrist |
|
|
What are the characteristics of an effusion?
|
- Uniform and diffuse fluid around a joint
- Does not move independently (non-mobile) since it is "attached" to joint |
|
|
What are the characteristics of bursitis?
|
- Localized, mobile
- Small or large - Located throughout the body - Usually feels "squishable" |
|
|
What are the characteristics of a ganglion?
|

- Usually relatively small <2 cm
- Usually near joints - Usually fairly tense - Chronic non-painful swelling in wrist, gets larger and smaller, but never completely goes away |
|
|
58 yo mentally handicapped women is brought in because she is "walking slower and less often than normal" since a fall 4 months ago; she was seen in ER and diagnosed w/ a small fibular avulsion fracture; had been doing PT w/ improvement in ankle pain.
Exam: uneven gait, tends to lean toward R, favoring L leg; L leg is more externally rotated than R and 2 cm shorter; increased ER and decreased IR on L; normal strength, mild pain with abduction and flexion. What do you suspect / what should you do? |

Femoral neck fracture
|
|
|
What are femoral neck fractures associated with?
|
- Young: trauma
- Elderly: osteoporosis + fall |
|
|
What are the four femoral neck fracture types?
|
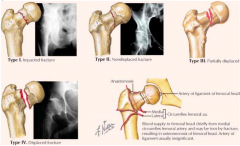
- I: impaction of superior portion of femoral neck (incomplete)
- II: non-displaced fracture (complete) - III: partial displacement between femoral head and neck - IV: complete displacement between femoral head and neck |
|
|
What is an "enthesopathy"?
|
Disorder of muscular or tendinous bony attachment
|
|
|
What is the difference between Tendinitis and Tendinosis?
|
- Tendinitis - acute inflammation of tendon (trauma - blow or pull)
- Tendinosis - chronic degenerative condition of tendon (submaximal repetitive irritation) |
|
|
What happens in a strain? What is the cause? Symptoms?
|
- Muscle fiber damage from overstretching
- Eccentric loading (muscle lengthening during firing) - Sx: stiffness, bruising, swelling, soreness |
|
|
What happens in a sprain? What is the cause? Symptoms?
|
- Ligamentous damage from overloading
- Sx: instability or laxity, swelling |
|
|
A football player gets hurt during a play causing his knee to bend backwards, what do you suspect? What are you most concerned about damage to?
|
- Knee multi-ligament tears
- Most concerned about damage to vessels (without this, you will need an amputation) |
|
|
What would most patients with an ACL injury complain of?
|
Buckling of the knee - no stability in knee (PCL alone is not enough to support sudden changes in direction)
|
|
|
What are the three knee articulations?
|
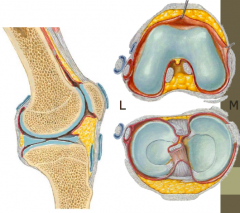
- Femoral condyles
- Tibial plateau - Patella |
|
|
What are the ligaments of the knee?
|
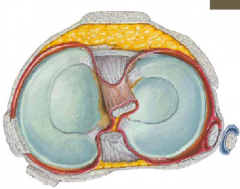
- Medial meniscus (c-shaped)
- Lateral meniscus (o-shaped) - Cruciates: ACL and PCL - Medial (tibial) collateral - Lateral (fibular) collateral |
|
|
In what direction can the tibia move relative to the femur if the ACL is torn? PCL is torn?
|
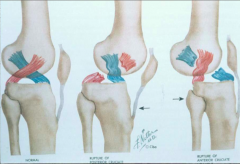
- ACL tear - move tibia anterior relative to femur
- PCL tear - move tibia posterior relative to femur |
|
|
What are the different degrees of sprains of the knee ligaments?
|
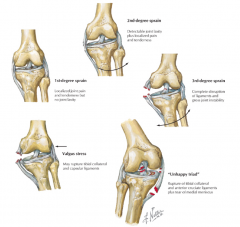
- 1st degree: stretched ligament w/ little or no tearing
- 2nd degree: partial tearing of ligament w/ joint laxity - 3rd degree: complete rupture of ligament, resulting in an unstable joint |
|
|
What happens in the "Unhappy Triad"?
|
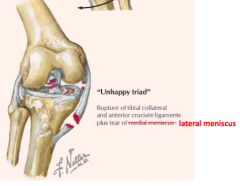
Force to lateral side of knee causes:
- Damage to ACL and MCL - Also damage to lateral meniscus (compression injury) |
|
|
Anterior Cruciate Ligament Sprain:
- Etiology - History - Exam |
- Etiology - twisting non-contact, deceleration or hyperextension injury
- History a) Acute - pop and rapid effusion b) Chronic - instability - Exam - (+) Lachmann – knee at 20-30° flexion; stabilize femur; check anterior translation & endpoint of tibia |
|
|
What can cause the menisci to tear?
|

Twisting injuries to knee
|
|
|
If a knee is "locking" what should you suspect?
|

Meniscal tear because pieces of meniscus can get in the way of the condyles and lock up a joint
|
|
|
Meniscal Tear:
- Etiology - History - Exam - Treatment |

- Etiology - usually occur with twisting on a loaded (weight-bearing) knee in athletes; degenerative tears are common in older patients
- History - locking & effusion - Exam - pain over joint line; pain with circumduction tests (McMurray is best known) - Treatment a) Locked - needs reduction; referral to orthopaedic surgeon b) No locking - physical therapy and relative rest |
|
|
35 yo runner complains of foot drop when running sub-5 minute/mile pace and great toe "numbness". He has no problems at slower speeds or with ADLs. No recent change in exercise regimen.
What do you suspect / what should you do? |
- Exertional compartment syndrome of anterior calf
- When working harder, increases pressure in anterior compartment, leads to swelling - At lower intensity the pressure is lower - Cutting off circulation - Foot drop (d/t compression of deep fibular nerve) |
|
|
Compartment Syndrome:
- Pathology - Etiology - Presentation |
- Pathology – elevation of pressures in a muscular compartment high enough to interfere with perfusion
- Etiology: a) Acute – severe bleed – usually caused by fracture b) Chronic exertional – from hypertrophied muscle in tight compartment with exercise (which increases muscle bulk up to 20%) c) Common locations – leg>>forearm - Presentation (6P’s): Pain, Paresthesia, Poikilothermia (coolness), Paralysis, Pallor, Pulselessness |
|
|
What are the 6 P's of Compartment Syndrome? Early or late signs?
|
1. Pain out of proportion (early sign)
2. Paresthesia (early sign) 3. Poikilothermia (coolness) 4. Paralysis (late) - footdrop d/t compression of deep fibular nerve 5. Pallor (late) 6. Pulselessness (late & rare) |
|
|
What causes anterior tibial compartment syndrome? Lateral compartment system?
|
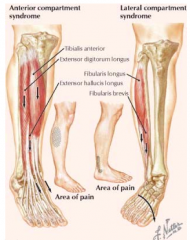
- Anterior: excessive contraction of anterior compartment muscles
- Lateral: excessively mobile ankle joint in which hypereversion irritates the lateral compartment muscles |
|
|
What are the normal / elevated / compartment syndrome pressures?
|
- Normal: 0-10 mm Hg
- Elevated, but not dangerous: 10-30 mm Hg - Acute compartment syndrome (potentially dangerous): 30-40 mm Hg - Usually dangerous, usually requires compartment release: 40-60 mm Hg - Consistently dangerous, requires urgent release: >60 mm Hg |
|
|
24 yo male sustains a GSW to lateral aspect of left knee; exam reveals that the deep fibular nerve has been damaged. Which muscles will be affected?
|
TEEP(F)EE:
- Tib ant. - EDL - EHL - Fib tertius - EDB - EHB |
|
|
30 yo runner is struck on the side of the leg by a bicyclist. Exam reveals the inability to evert her foot and diminished sensation on the dorsum of her foot. Which muscles are affected?
|
- Fibularis longus
- Fibularis brevis |
|
|
50 yo male was working with his chain saw when he slipped and sustained a laceration down to his bone on the posterior aspect of his medial malleolus. Nerve deficits could include which of the following?
|
Medial plantar nerve
|
|
|
Which compartment is least likely to get exertional compartment syndrome?
|
Superificial posterior
|
|
|
What compartment is most likely to get a compartment syndrome?
|
- Anterior: 40-50%
- Deep posterior: 30% - Lateral: 20% |
|
|
What happens in Deep Vein Thrombosis?
|
- Clots, commonly in vein of lower limb
- Clot can break loose from leg and flow to lungs and cause PE |
|
|
What three events account for the pathogenesis and risk for a Deep Venous Thrombosis?
|

- Stasis
- Venous wall injury - Hypercoagulability |
|
|
What are the risk factors for a Deep Venous Thrombosis?
|
- Postsurgical immobility
- Paralysis - Vessel trauma - Malignancy - Infection - Trauma |
|
|
How does a pressure ulcer (bedsore) occur?
|
- Soft tissue compressed between bony eminence (e.g., greater trochanter) and bed or wheelchair
- Comatose, paraplegic, or debilitated patients cannot sense discomfort caused by pressure from prolonged contact |
|
|
What are the most common sites of pressure ulcers?
|
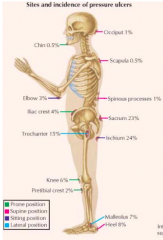
- Pelvic girdle: sacrum, iliac crest, ischium, greater trochanter of femur
- Other bony prominences |
|
|
What are the four stages of pressure ulcers?
|
- I: changes in skin temp, consistency, or sensation; persistent redness
- II: partial-thickness skin loss, similar to an abrasion w/ shallow crater or blister - III: full-thickness skin loss w/ SUBCUTANEOUS tissue damage and a deep crater - IV: full-thickness skin loss w/ necrosis or damage to MUSCLE, BONE, or adjacent structures |
|
|
Where can the pulse from the femoral artery be felt?
|
Just inferior to the inguinal ligament as it is compressed against the femoral head; lateral to the femoral vein
|
|
|
Where does the tibia most commonly get fractured?
|
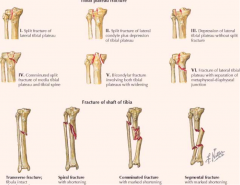
- Lateral tibial condyle most common site of tibial plateau fractures
- Tibial shaft (most common fracture of a long bone) |
|
|
What is a common patellar injury?
|
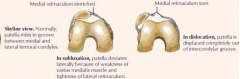
Subluxation of patella / dislocation
|
|
|
Patellar Dislocation
- Epidemiology - History - Exam - Treatment |
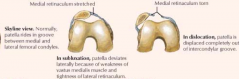
- Epidemiology - usually lateral dislocation, more common in adolescent girls / young women
- History - cutting with active quadriceps contraction, immediate pain & swelling, tenderness along medial aspect - Examination - ecchymosis, effusion; sometimes atrophy of quadriceps tendon; Positive apprehension test – feeling of instability with stressing of the joint - Treatment – physical therapy. If recurrent may eventually need surgery |
|
|
What can happen to the patellar / quadriceps tendons?
|

Rupture of patellar tendon (d/t direct trauma in younger person) or quadriceps tendon (d/t minor trauma or age-related degeneration in older adults)
|
|
|
What changes can cause an older adult to be at increased risk for a quadriceps tendon rupture?
|

- Arthritis
- Arteriosclerosis - Chronic renal failure - Corticosteroid therapy - Diabetes - Hyper-PTH - Gout |
|
|
What are the common symptoms of Osteoarthritis in the knee?
|
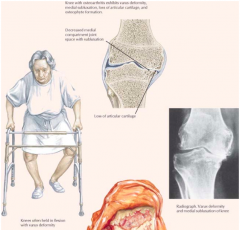
- Painful associated w/ activity
- Weather may precipitate painful episodes - Stiffness after inactivity - Decreased ROM - Subluxation of knee may occur w/ a varus (bowleg) deformity |
|
|
What causes Shin Splints?
|
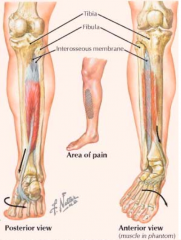
- Repetitive pulling of tibialis posterior tendon as one pushes off the foot in running
- Stress on muscle occurs at attachment to tibia and interosseus membrane |
|
|
What are the symptoms of shin splints?
|
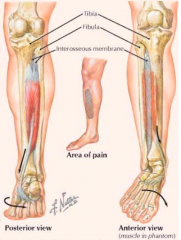
- Pain along inner distal 2/3 of tibial shaft
- Chronic conditions can cause periostitis and bone remodeling or stress fractures |
|
|
What is the most common malignant bone tumor of mesenchymal origin?
|

Osteosarcoma
|
|
|
Who gets Osteosarcoma more commonly? Where?
|

- Males
- Usually before 30 years - Distal femur or proximal tibia (also proximal humerus, proximal femur, pelvis) - Metaphysis of long bones at areas of greatest growth |
|
|
What is the normal orientation of the knee (varus vs valgus)? What do these terms mean?
|
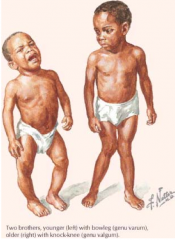
- Normal: slight valgus (knock knee)
- Genu Valgum - knock-knee (tall boy) - Genu Varus - bowleg (short boy) |
|
|
What is the cause of genu valgum and genu varum? Treatment?
|
Usually d/t Rickets, skeletal dysplasia, or trauma (most resolve w/o treatment)
|
|
|
Who is most likely to get Achilles Tendinitis? Why?
|
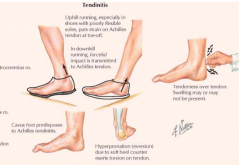
- Runners who run on hills or uneven surfaces
- Repetitive stress on tendon occurs as heel strikes ground and when plantarflexion lifts foot and toes |
|
|
Achilles tendon rupture:
- Epidemiology - History - Exam - Treatment |
- Typical patient – middle aged male ruptures while playing basketball
- History – heard pop & felt like someone hit them in back of ankle with golf club. Difficulty walking - Exam: Defect in Achilles and pain & weakness with plantar flexion - Treatment – either acute immobilization (heals slowly) or surgery |
|
|
What happens in Retrocalcaneal Bursitis?
|
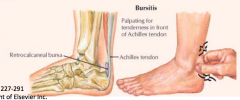
- Inflammation of subtendinous bursa between the overlying tendon and the calcaneus
- Presents as a tender area just anterior to tendon attachment |
|
|
How do most ankle sprains occur? Which ligaments are injured?
|
- INversion injury when foot is plantarflexed, placing stress on components of lateral collateral ligament
- Anterior to posterior (most commonly injured ligaments): first anterior talofibular ligament, then calcneofibular ligament, and finally, posterior talofibular ligament |
|
|
How do you examine a potential ankle sprain?
|
- Anterior drawer test – tibia held steady while heel is pulled anteriorly w/ foot at 10-20 deg plantarflexion; abnormal is 3-5 mm more than uninjured side; may also fell softer end point on injured side (indicates anterior talofibular ligament)
- Squeeze test – squeeze the tibia & fibular together mid-shaft; pain at ankle suspicious for high ankle sprain; pain at knee suspicious for Maisonneuve fracture – fracture of the proximal fibula associated with ankle injury - External rotation test (+) suspicious for high ankle sprains |
|
|
What are the stages of ankle fractures?
|

|