Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
244 Cards in this Set
- Front
- Back
|
What can cause Cushing syndrome? |
Excess cortisol due to a variety of causes:
- Exogenous steroids - Primary adrenal adenoma, hyperplasia, or carcinoma - ACTH-secreting pituitary adenoma |
|
|
What is the number one cause of Cushing syndrome? Characteristics?
|
Exogenous corticosteroids: results in ↓ ACTH and bilateral adrenal atrophy
|
|
|
What causes of Cushing syndrome result in ↓ ACTH? Effect on adrenals?
|
- Exogenous steroids - bilateral adrenal atrophy
- Primary adrenal adenoma, hyperplasia, or carcinoma - atrophy of uninvolved adrenal gland |
|
|
What can primary adrenal adenoma / hyperplasia / carcinoma produce?
|
- ↑ Cortisol (= Cushing Syndrome)
OR - ↑ Aldosterone (1° Aldosteronism = Conn Syndrome) |
|
|
What is Conn Syndrome?
|
1° Aldosteronism (due to primary adrenal adenoma, hyperplasia, or carcinoma)
|
|
|
What causes of Cushing syndrome result in ↑ ACTH? Effect on adrenals?
|
ACTH-secreting pituitary adenoma (Cushing disease)
- Paraneoplastic ACTH secretion: small cell lung cancer, bronchial carcinoids - Bilateral adrenal hyperplasia |
|
|
What is responsible for the majority of the endogenous cases of Cushing Syndrome?
|
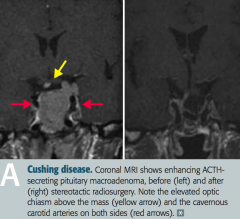
Cushing Disease
- ACTH-secreting pituitary adenoma - Paraneoplastic ACTH secretion: small cell lung cancer, bronchial carcinoids |
|
|
What are the findings associated with Cushing Syndrome?
|

- Hypertension
- Weight gain - Moon facies - Truncal obesity - Buffalo hump - Hyperglycemia (insulin resistance) - Skin changes (thinning, striae) - Osteoporosis - Amenorrhea - Immune suppression |
|
|
How do you screen for Cushing Syndrome?
|
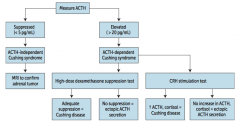
** Measure serum ACTH **
You can also evaluate: - ↑ Free cortisol on 24-hr urinalysis - Midnight salivary cortisol - Overnight low-dose dexamethasone suppression test (measure serum ACTH) |
|
|
What should you suspect / do if a patient you suspect of having Cushing Syndrome has a low ACTH (<5 pg/mL)?
|
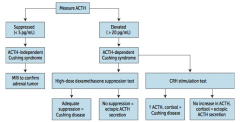
Suspect ACTH-independent Cushing Syndrome (primary adrenal adenoma, hyperplasia, or carcinoma)
* Order MRI to confirm adrenal tumor |
|
|
What should you suspect / do if a patient you suspect of having Cushing Syndrome has a high ACTH (>20 pg/mL)?
|
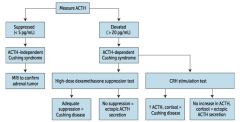
Suspect ACTH-dependent Cushing Syndrome
* Order high-dose dexamethasone suppression test * Order CRH stimulation test |
|
|
What diagnosis does a patient you suspect of having Cushing Syndrome, with an elevated ACTH, and adequate suppression via high-dose dexamethasone suppression test?
|
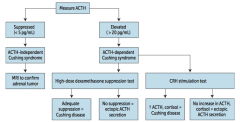
Cushing Disease (ACTH-secreting pituitary adenoma)
|
|
|
What diagnosis does a patient you suspect of having Cushing Syndrome, with an elevated ACTH, and no suppression via high-dose dexamethasone suppression test?
|
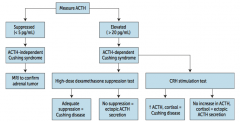
Ectopic ACTH secretion (paraneoplastic syndrome: small cell lung cancer or bronchial carcinoids)
- Ectopic secretion will not decrease with dexamethasone because the source is resistant to negative feedback |
|
|
What diagnosis does a patient you suspect of having Cushing Syndrome, with an elevated ACTH, and after after a CRH stimulation test there was ↑ ACTH and cortisol?
|
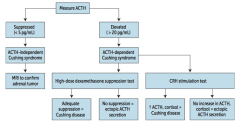
Cushing Disease (ACTH-secreting pituitary adenoma)
|
|
|
What diagnosis does a patient you suspect of having Cushing Syndrome, with an elevated ACTH, and after after a CRH stimulation test there was no increase in ACTH and cortisol?
|
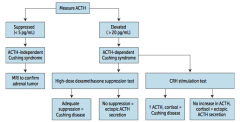
Ectopic ACTH secretion
- Ectopic secretion will not increase with CRH because pituitary ACTH is suppressed |
|
|
What are the causes of primary hyperaldosteronism?
|
- Adrenal hyperplasia
- Aldosterone secreting adrenal adenoma (Conn syndrome) (May be unilateral or bilateral) |
|
|
What are the consequences of adrenal hyperplasia or aldosterone-secreting adrenal adenoma?
|
Primary Hyperaldosteronism:
- Hypertension - Hypokalemia - Metabolic alkalosis - Low plasma renin - Normal Na+ due to aldosterone escape → no edema |
|
|
How do you treat primary hyperaldosteronism?
|
Surgery to remove the tumor and/or spironolactone (K+ sparing diuretic that acts as an aldosterone antagonist)
|
|
|
What are the causes of secondary hyperaldosteronism?
|
- Renal artery stenosis
- Congestive Heart Failure - Cirrhosis - Nephrotic Syndrome |
|
|
What are the consequences of renal artery stenosis, CHF, cirrhosis, or nephrotic syndrome?
|
Secondary Hyperaldosteronism
- Renal perception of low intravascular volume → over-active renin-angiotensin system - Associated with high plasma renin |
|
|
How do you treat secondary hyperaldosteronism?
|
Spironolactone (K+ sparing diuretic that acts as an aldosterone antagonist)
|
|
|
What form of hyperaldosteronism is associated with a high plasma renin?
|
Secondary Hyperaldosteronism
- In primary, there is negative feedback to decrease renin - In secondary, the high renin is what is causing the high aldosterone |
|
|
What are the causes of primary adrenal insufficiency?
|
Addison Disease - CHRONIC process
- Atrophy of adrenals - Destruction by disease: auto-immune, TB, metastasis Waterhouse-Friderichsen Syndrome - ACUTE process - Adrenal hemorrhage associated with Neisseria meningitidis, septicemia, DIC, and endotoxic shock |
|
|
What are the implications of Addison Disease?
|
- Deficiency of aldosterone and cortisol
- Hypotension (hyponatremic volume contraction) - Hyperkalemia - Acidosis - Skin and mucosal hyperpigmentation |
|

What causes the skin hyperpigmentation in Addison Disease?
|

MSH (melanocyte stimulating hormone): by-product of ↑ ACTH production from pro-opiomelanocortin (POMC)
|
|
|
How is Addison Disease characterized?
|
- Adrenal Atrophy
- Absence of hormone production, involving all three cortical divisions (but spares medulla) |
|
|
How do you distinguish primary adrenal insufficiency from secondary?
|
Secondary adrenal insufficiency would have:
- ↓ Pituitary ACTH production - No skin/mucosal hyperpigmentation - No hyperkalemia |
|
|
What are the electrolyte and acid/base balance changes in primary adrenal insufficiency?
|
- Hyponatremia
- Hyperkalemia - Acidosis |
|
|
What is the name of the syndrome causing ACUTE 1° adrenal insufficiency? Cause?
|
Waterhouse-Friderichsen Syndrome
- Adrenal hemorrhage associated with Neisseria meningitidis septicemia, DIC, and endotoxic shock |
|
|
What is the most common tumor of the adrenal medulla in children? When specifically?
|
Neuroblastoma
- Usually <4 years old |
|
|
What is the origin of a neuroblastoma?
|
Neural crest cells
|
|
|
Where can a neuroblastoma appear?
|
Occurs anywhere along the sympathetic chain
|
|
|
What is the most common presentation of Neuroblastoma?
|
- Abdominal distension
- Firm, irregular mass that can CROSS THE MIDLINE - Usually in children < 4 years old - Less likely to develop hypertension |
|
|
When you have a firm, irregular mass that crosses the midline of a young child, what diagnosis should you think of?
|
Neuroblastoma
|
|
|
When you have a smooth mass that does not cross the midline of a young child, what diagnosis should you think of?
|
Wilms tumor (nephroblastoma)
- Most common renal malignancy of early childhood (ages 2-4) |
|
|
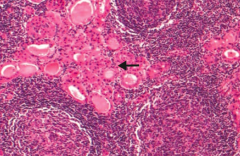
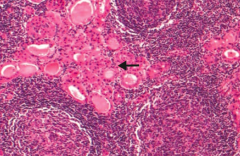
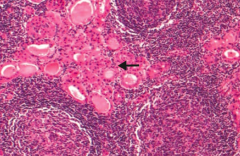
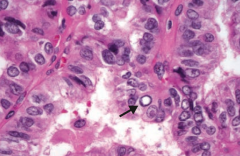
What lab studies are associated with a Neuroblastoma?
|
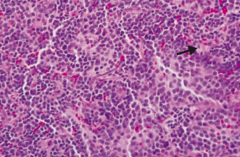
- Homovanillic acid (HVA), a breakdown product of dopamine, is increased in urine
- Bombesin (+) - LM: rosettes (arrow) and classic small, round, blue/purple nuclei |
|
|
What genetic change is associated with Neuroblastoma?
|
Over-expression of the N-myc oncogene
|
|
|
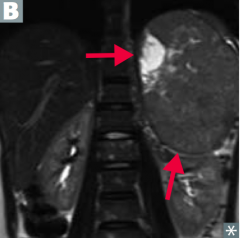
What is the most common tumor of the adrenal medulla in adults?
|
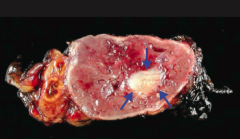
Pheochromocytoma
|
|
|
What is a pheochromocytoma derived from?
|
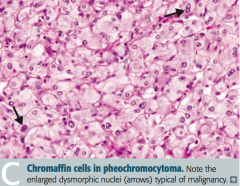
Chromaffin cells (arise from neural crest)
|
|
|
What rule can you use to remember characteristics of a pheochromocytoma?
|
Rule of 10s:
- 10% malignant - 10% bilateral - 10% extra-adrenal - 10% calcify - 10% in kids |
|
|
What does a pheochromocytoma do?
|
Most tumors secrete epinephrine, norepinephrine, and dopamine → episodic hypertension
|
|
|
What genetic change is pheochromocytoma associated with?
|
- Von Hippel-Lindau disease
- MEN 2A - MEN 2B |
|
|
What symptoms are typical of pheochromocytoma?
|
Symptoms occur in "spells" - relapse and remit:
Episodic hyperadrenergic symptoms (5 P's): - Pressure (↑ BP) - Pain (headache) - Perspiration - Palpitations (tachycardia) - Pallor |
|
|
What are the lab findings associated with a pheochromocytoma?
|
- ↑ Urinary VMA (breakdown product of NE and Epi)
- ↑ Plasma catecholamines (NE, Epi, etc) |
|
|
How do you treat pheochromocytoma?
|
1. Irreversible α-antagonist (phenoxybenzamine)
2. β-blockers 3. Tumor resection ** α-blockade must be achieved before giving β-blockers to avoid a hypertensive crisis ** |
|
|
For what diagnosis must you treat the patient first with α-antagonists before β-blockers? Why?
|
For treatment of Pheochromocytoma:
This is necessary to avoid a hypertensive crisis |
|
|
What are the characteristic signs / symptoms of hypothyroidism?
|
- Cold intolerance (↓ heat production)
- Weight gain, ↓ appetite - Hypoactivity, lethargy, fatigue, weakness - Constipation - ↓ Reflexes - Myxedema (facial / periorbital) - Dry, cool skin with coarse, brittle hair - Bradycardia, dyspnea on exertion |
|
|
What are the characteristic signs / symptoms of hyperthyroidism?
|
- Heat intolerance (↑ heat production)
- Weight loss, ↑ appetite - Hyperactivity - Diarrhea - ↑ Reflexes - Pretibial myxedema (Graves disease), periorbital edema - Warm, moist skin with fine hair - Chest pain, palpitations, arrhythmias, ↑ number and sensitivity of β-adrenergic receptors |
|
|
How do patients with hypothyroidism vs hyperthyroidism compare in terms of their bowel habits?
|
- Hypothyroidism: constipation
- Hyperthyroidism: diarrhea |
|
|
How do patients with hypothyroidism vs hyperthyroidism compare in terms of their reflexes?
|
- Hypothyroidism: decreased reflexes
- Hyperthyroidism: increased reflexes |
|
|
How do patients with hypothyroidism vs hyperthyroidism compare in terms of myxedema (swelling of the skin and underlying tissues giving a waxy consistency)?
|
- Hypothyroidism: facial and periorbital myxedema
- Hyperthyroidism: pretibial myxedema (Graves disease), periorbital edema |
|
|
How do patients with hypothyroidism vs hyperthyroidism compare in terms of their skin and hair?
|
- Hypothyroidism: dry, cool skin with coarse, brittle hair
- Hyperthyroidism: warm, moist skin with fine hair |
|
|
How do patients with hypothyroidism vs hyperthyroidism compare in terms of cardiac symptoms?
|
- Hypothyroidism: bradycardia and dyspnea on exertion
- Hyperthyroidism: chest pain, palpitations, arrhythmias, ↑ number and sensitivity of β-adrenergic receptors |
|
|
Why do patients with hyperthyroidism sometimes have chest pain, palpitations, and arrhythmias?
|
↑ number and sensitivity of β-adrenergic receptors
|
|
|
What are the lab findings associated with hypothyroidism?
|
- ↑ TSH (sensitive for 1° hypothyroidism)
- ↓ free T3 and T4 - Hypercholesterolemia (due to ↓ LDL receptor expression) |
|
|
What are the lab findings associated with hyperthyroidism?
|
- ↓ TSH (if 1°)
- ↑ free or total T3 and T4 - Hypocholesterolemia (due to ↑ LDL receptor expression) |
|
|
How do thyroid disorders affect cholesterol? Mechanism?
|
- Hypothyroidism: hypercholesterolemia due to ↓ LDL receptor expression
- Hyperthyroidism: hypocholesterolemia due to ↑ LDL receptor expression |
|
|
What is the most common cause of hypothyroidism in iodine-sufficient regions?
|
Hashimoto Thyroiditis
|
|
|
What causes Hashimoto Thyroiditis?
|
Auto-immune disorder
- Anti-thyroid peroxidase and anti-thyroglobulin antibodies - Associated with HLA-DR5 |
|
|
What is there increased risk of in patients with Hashimoto Thyroiditis?
|
Non-Hodgkin Lymphoma
|
|
|
What may be an early, contradictory finding seen in patients with Hashimoto Thyroiditis?
|
May be hyperthyroid early in course due to thyrotoxicosis during follicular rupture
|
|
|
What are the histologic findings of Hashimoto Thyroiditis?
|
Hürthle cells, lymphoid aggregate with germinal centers
|
|
What does this histology indicate?
|
Hürthle cells, lymphoid aggregate with germinal centers → Hashimoto Thyroiditis
|
|
|
What are the expected thyroid findings on physical exam in a patient with Hashimoto Thyroiditis?
|
Moderately enlarged, non-tender
|
|
|
The presence of Hürthle cells should make you think of what?
|
Hashimoto Thyroiditis
|
|
|
What can cause severe fetal hypothyroidism (congenital hypothyroidism)?
|
- Maternal hypothyroidism
- Thyroid agenesis - Thyroid dysgenesis (most common cause in US) - Iodine deficiency - Dyshormonogenic goiter |
|
|
What are the findings of a patient with congenital hypothyroidism?
|

6 P's:
- Pot-bellied - Pale - Puffy-faced child - Protruding umbilicus - Protuberant tongue - Poor brain development |
|
|
What is cretinism?
|
Congenital hypothyroidism
|
|
|
What is the most common cause of congenital hypothyroidism in the US?
|
Thyroid Dysgenesis
|
|
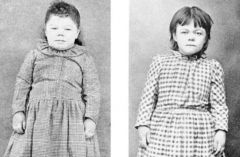
What is wrong with the child on the left (before) and after treatment on the right?
|
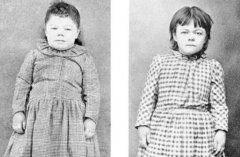
Congenital hypothyroidism
|
|
|
What is the term for the self-limited hypothyroidism often following a flu-like illness?
|
Subacute Thyroiditis (de Quervain)
|
|
|
What happens in Subacute Thyroiditis (de Quervain)?
|
- May be hyperthyroid early in course
- Self-limited hypothyroidism often following a flu-like illness |
|
|
What is the appearance of the thyroid histologically in Subacute Thyroiditis (de Quervain)?
|
Granulomatous inflammation
|
|
|
What cause of hypothyroidism is associated with a very tender / painful thyroid?
|
Subacute Thyroiditis (de Quervain)
*de QuerVAIN is associated with PAIN* |
|
|
What are the findings in Subacute Thyroiditis (de Quervain)?
|
- ↑ ESR
- Jaw pain - Early inflammation - Very tender thyroid - Granulomatous inflammation of thyroid |
|
|
What causes granulomatous inflammation of the thyroid?
|
Subacute Thyroiditis (de Quervain)
|
|
|
What disease causes the thyroid to be replaced with fibrous tissue? What does this cause?
|
Riedel Thyroiditis - causes hypothyroidism
|
|
|
What happens in Riedel Thyroiditis?
|
- Thyroid replaced by fibrous tissue (hypothyroid)
- Fibrosis may extend to local structures (eg, airway), mimicking anaplastic carcinoma |
|
|
What is Riedel Thyroiditis considered a manifestatoin of?
|
Manifestation of IgG4-related systemic disease
|
|
|
What are the findings of a patient's thyroid in Riedel Thyroiditis on physical exam?
|
- Fixed
- Hard (rock-like) - Painless goiter |
|
|
What are some other causes of hypothyroidism?
|
- Iodine deficiency
- Goitrogens - Wolff-Chaikoff effect - Painless thyroiditis |
|
|
What are the causes of hyperthyroidism?
|
- Toxic multinodular goiter
- Graves disease - Thyroid storm |
|
|
What pathology is associated with focal patches of hyper-functioning follicular cells that work independently of TSH due to a mutation in the TSH receptor?
|
Toxic Multinodular Goiter
|
|
|
What is wrong in Toxic Multinodular Goiter?
|
- Focal patches of hyper-functioning follicular cells
- Work independently of TSH due to mutation in TSH receptor - ↑ Release of T3 and T4 |
|
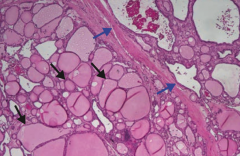
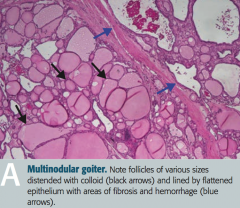
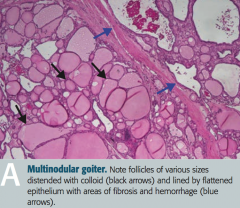
What does this histologic image of the thyroid show?
|
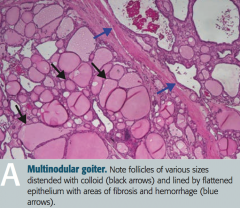
Toxic Multinodular Goiter
- Follicles of various sizes distended with colloid (black arrows) - Follicles are lined by flattened epithelium with areas of fibrosis and hemorrhage (blue arrows) - Nodules are rarely malignant |
|
|
What is the term for thyrotoxicosis when a patient with iodine deficiency suddenly is made iodine replete?
|
Jod-Basedow Phenomenon
|
|
|
What happens in the Jod-Basedow Phenomenon?
|
Thyrotoxicosis if a patient with iodine deficiency goiter is made iodine replete
|
|
|
What is the most common cause of hyperthyroidism?
|
Graves disease
|
|
|
What is the underlying pathophysiology responsible for Graves disease?
|
Auto-antibodies (IgG) stimulate TSH receptors on thyroid, retro-orbital fibroblasts, and dermal fibroblasts
|
|
|
What kind of antibodies are associated with Graves disease? Hashimoto Thyroiditis?
|
- Graves disease: IgG auto-Abs that stimulate TSH receptors
- Hashimoto Thyroiditis: anti-thyroid peroxidase and anti-thyroglobulin auto-Abs |
|
|
What are the implications of auto-antibodies (IgG) stimulating the TSH receptors on the thyroid?
|
- Hyperthyroidism
- Diffuse goiter |
|
|
What are the implications of auto-antibodies (IgG) stimulating the TSH receptors on retro-orbital fibroblasts?
|
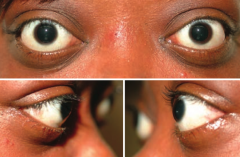
Exophthalmos: proptosis, extraocular muscle swelling
|
|
|
What are the implications of auto-antibodies (IgG) stimulating the TSH receptors on dermal fibroblasts?
|
Pretibial myxedema
|
|
|
When does Graves disease often present?
|
During stress (eg, childbirth)
|
|
|
What is the name for the stress-induced catecholamine surge seen as a serious complication of Graves disease and other hyperthyroid disorders?
|
Thyroid Storm
|
|
|
What causes a Thyroid Storm?
|
Stress-induced catecholamine surge seen as a serious complication of Graves disease and other hyperthyroid disorders
|
|
|
What are the symptoms of a Thyroid Storm?
|
- Agitation
- Delirium - Fever - Diarrhea - Coma - Tachyarrhythmia (cause of death) |
|
|
What lab value is possibly elevated in Thyroid Storm? Why?
|
↑ ALP due to ↑ bone turnover
|
|
|
How do you treat Thyroid Storm?
|
Treat with the 3 P's:
- β-blockers (eg, Propranolol) - Propylthiouracil - Corticosteroids (eg, Prednisolone) |
|
|
What are the indications for thyroidectomy?
|
Treatment option for thyroid cancers and hyperthyroidism
|
|
|
What are the potential complications of thyroid cancer?
|
- Hoarseness: due to recurrent laryngeal nerve damage
- Hypocalcemia: due to removal of parathyroid glands - Transection of inferior thyroid artery |
|
|
What are the types of thyroid cancers?
|
- Papillary carcinoma
- Follicular carcinoma - Medullary carcinoma - Undifferentiated / anaplastic carcinoma - Lymphoma |
|
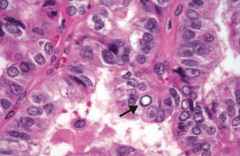
If you see this on a sample of the thyroid, what diagnosis do you need to think of?
|
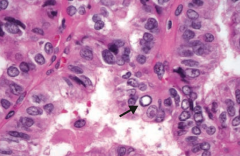
Papillary Carcinoma of the thyroid
- Empty appearing nuclei ("Orphan Annie" eyes) |
|
|
What is the most common type of thyroid cancer? Associations?
|
- Empty-appearing nuclei (Orphan Annie eyes), psamomma bodies, nuclear grooves
- Increased risk with RET and BRAF mutations and childhood irradiation - Excellent prognosis |
|
|
What are the histologic findings of Papillary Carcinoma of the thyroid?
|
- Empty-appearning nuclei ("Orphan Annie" eyes)
- Psammoma bodies - Nuclear grooves |
|
|
What can increase your risk of getting Papillary Carcinoma of the Thyroid?
|
- RET mutations
- BRAF mutations - Childhood irradiation |
|
|
Which types of thyroid cancer are associated with a good prognosis?
|
- Papillary Carcinoma (excellent prognosis, most common type)
- Follicular Carcinoma (good prognosis) |
|
|
Which type of thyroid cancer has a very poor prognosis?
|
Undifferentiated / Anaplastic Carcinoma of thyroid
|
|
|
What are the characteristics of a Follicular Carcinoma of the thyroid?
|
- Good prognosis
- Invades thyroid capsule (unlike follicular adenoma) - Uniform follicles |
|
|
What type of thyroid cancer arises from parafollicular "C cells"?
|
Medullary Carcinoma of the thyroid
|
|
|
What is the origin of Medullary Carcinoma of the thyroid? What does it produce?
|
- From parafollicular "C cells"
- Produces calcitonin |
|
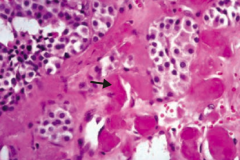
If you see this on a sample of the thyroid, what diagnosis do you need to think of?
|
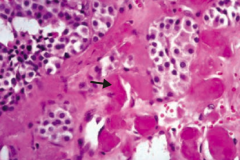
Medullary Carcinoma of the thyroid
- Solid sheets of cells with amyloid deposition (arrow) - Amyloid stroma |
|
|
What is Medullary Carcinoma of the thyroid associated with?
|
- MEN 2A and 2B
- RET mutations |
|
|
What type of thyroid cancer is more common in older patients?
|
Undifferentiated / Anaplastic Carcinoma of thyroid
|
|
|
What are the characteristics of Undifferentiated / Anaplastic Carcinoma of thyroid?
|
- Affects older patients
- Invades local structures - Very poor prognosis |
|
|
Which type of thyroid cancer is associated with Hashimoto thyroiditis?
|
Lymphoma
|
|
|
What are the types of hyperparathyroidism? Levels of Calcium in each?
|
- Primary: hypercalcemia
- Secondary: hypocalcemia - Tertiary: hypercalcemia |
|
|
What is the most common cause of primary hyperparathyroidism?
|
Parathyroid Adenoma
|
|
|
How are hormones / electrolytes affected by Primary Hyperparathyroidism?
|
- ↑ Ca2+: hypercalcemia and hypercalciuria
- ↓ PO4-: Hypophosphatemia - ↑ PTH - ↑ ALP - ↑ cAMP in urine |
|
|
What are the most common symptoms of Primary Hyperparathyroidism?
|
- Most often asymptomatic
- May present with symptoms of hypercalcemia: weakness and constipation ("groans"), abdominal / flank pain (kidney "stones", or acute pancreatitis), depression ("psychiatric overtones") |
|
|
What mnemonic helps you remember the symptoms of hypercalcemia?
|
"Stones, bones, groans, and psychiatric overtones"
- Renal stones → abdominal / flank pain - Bones → osteitis fibrosa cystica (cystic bone spaces filled with brown fibrous tissue causing bone pain) - Groans → weakness and constipation - Psychiatric overtones → depression |
|
|
What happens in Osteitis Fibrosa Cystica? Cause?
|
- Cystic bone spaces are filled with brown fibrous tissue → bone pain
- Caused by hyperparathyroidism |
|
|
What causes Secondary Hyperparathyroidism?
|
- Secondary hyperplasia due to ↓ gut Ca2+ absorption and ↑ PO4(3-)
- Most often in chronic renal disease (causes hypovitaminosis D → ↓ Ca2+ absorption) |
|
|
What are the hormone / electrolyte findings in Secondary Hyperparathyroidism?
|
- ↓ Ca2+: hypocalcemia
- ↑ PO4-: hyperphosphatemia in chronic renal failure, although most other causes have hypophosphatemia - ↑ ALP - ↑ PTH |
|
|
How are the bones affected by Secondary Hyperparathyroidism or Tertiary Hyperparathyroidism?
|
Bone lesions occur in 2° or 3° hyperparathyroidism due in turn to renal disease = Renal Osteodystrophy
|
|
|
What causes Tertiary Hyperparathyroidism?
|
Refractory (autonomous) hyperparathyroidism resulting from chronic renal disease
|
|
|
What are the hormone / electrolyte findings in Tertiary Hyperparathyroidism?
|
- ↑ Ca2+
- ↑↑ PTH |
|
|
What is the difference between secondary and tertiary hyperparathyroidism?
|
Both commonly due to chronic renal disease
- 2°: ↓ Ca2+ and ↑ PTH - 3°: ↑ Ca2+ and ↑↑ PTH Both associated with renal osteodystrophy (bone lesions) |
|
|
What are the most common causes of hypoparathyroidism?
|
Hypoparathyroidism:
- Accidental surgical excision of parathyroid glands - Auto-immune destruction - DiGeorge syndrome Pseudohypoparathyroidism (Albright Hereditary Osteodystrophy) - Autosomal dominant unresponsiveness of kidney to PTH |
|
|
What are the findings associated with hypoparathyroidism?
|
- Hypocalcemia
- Tetany - Chvostek sign - Trousseau sign |
|
|
How do you check for a Chvostek sign? What does it indicate if it is positive?
|
- Tap the facial nerve (tap the cheek)
- Positive: contraction of facial muscles - Sign of hypoparathyroidism |
|
|
How do you check for a Trousseau sign? What does it indicate if it is positive?
|
- Occlusion of brachial artery with BP cuff (cuff the TRiceps)
- Positive: carpal spasm - Sign of hypoparathyroidism |
|
|
What is the other name for pseudohypoparathyroidism? Cause?
|
Albright Hereditary Osteodystrophy
- Autosomal dominant unresponsiveness of kidney to PTH |
|
|
What are the symptoms of Albright Hereditary Osteodystrophy? Cause?
|
- Hypocalcemia, shortened 4th/5th digits, and short sature
- Caused by autosomal dominant unresponsiveness of kidney to PTH (pseudo-hypoparathyroidism) |
|
|
Which PTH / Calcium pathology is associated with a low Ca2+ and a low PTH? Cause?
|
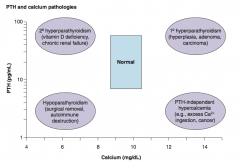
Hypoparathyroidism:
- Surgical removal - Autoimmune destruction |
|
|
Which PTH / Calcium pathology is associated with a low Ca2+ and a high PTH? Cause?
|
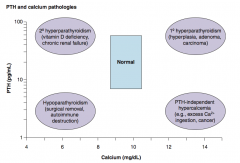
2° Hyperparathyroidism
- Vitamin D deficiency - Chronic renal failure |
|
|
Which PTH / Calcium pathology is associated with a high Ca2+ and a low PTH? Cause?
|
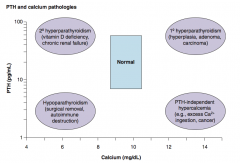
PTH-independent hypercalcemia:
- Excess Ca2+ ingestion - Cancer |
|
|
Which PTH / Calcium pathology is associated with a high Ca2+ and a high PTH? Cause?
|
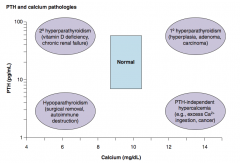
1° Hyperparathyroidism:
- Hyperplasia - Adenoma - Carcinoma |
|
|
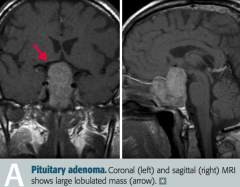
What is the most common form of pituitary adenoma? Symptoms?
|
Prolactinoma
- Amenorrhea - Galactorrhea - Low libido - Infertility |
|
|
How do you treat a prolactinoma (pituitary adenoma)?
|
Dopamine agonists:
- Bromocriptine - Cabergoline |
|
|
What are the types of pituitary adenomas?
|
- Functional (hormone producing, eg, prolactinoma)
- Non-functional (silent, present with mass effect) |
|
|
What is most likely wrong in a patient with amenorrhea, galactorrhea, low libido, and infertility?
|
Prolactinoma (type of functioning pituitary adenoma)
|
|
|
What is most likely wrong in a patient with bitemporal hemianopia, hypopituitarism, and a headache?
|
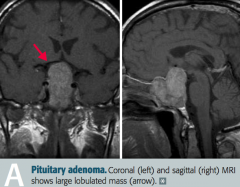
Non-functional pituitary adenoma, causing problems due to mass effect
|
|
|
What are the symptoms of a non-functional pituitary adenoma with mass effect?
|
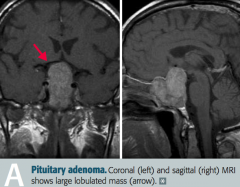
- Bitemporal hemianopia
- Hypopituitarism - Headache |
|
|
What are the symptoms of a somatotropic pituitary adenoma?
|
Acromegaly
|
|
|
What is the cause of acromegaly?
|
Excess GH in adults, typically caused by a pituitary adenoma
|
|
|
What are the characteristic findings in a patient with Acromegaly?
|

- Large tongue with deep furrows
- Deep voice - Large hands and feet - Coarse facial features - Impaired glucose tolerance (insulin resistance) |
|
|
What is the name of the syndrome caused by increased GH in children? Symptoms? Cause of death?
|
Gigantism
- ↑ Linear bone growth - Cardiac failure most common cause of death |
|
|
How do you confirm a diagnosis of Acromegaly?
|
- ↑ Serum IGF-1
- Failure to suppress serum GH following oral glucose tolerance test - Pituitary mass seen on brain MRI |
|
|
How do treat a patient with Acromegaly?
|
- Pituitary adenoma resection
- If not cured, treat with Octreotide (somatostatin analog) or Pegvisomant (GH receptor antagonist |
|
|
What drug is a GH receptor antagonist?
|
Pegvisomant
|
|
|
What drug is a somatostatin analog?
|
Octreotide
|
|
|
What drugs are dopamine agonists?
|
- Bromocriptine
- Cabergoline |
|
|
If you have a patient with intense thirst, polyuria, and inability to concentrate urine, what diagnosis should you think of?
|
Diabetes Insipidus
|
|
|
What are the types of Diabetes Insipidus? Basic issue?
|
- Central DI: lack of ADH
- Nephrogenic DI: insensitivity to ADH |
|
|
What are possible causes of Central Diabetes Insipidus?
|
- Pituitary tumor
- Auto-immune process - Trauma - Surgery - Ischemic encephalopathy - Idiopathic |
|
|
What are possible causes of Nephrogenic Diabetes Insipidus?
|
- Hereditary (ADH receptor mutation)
-2° to hypercalcemia, lithium, demeclocycline (ADH antagonist) |
|
|
If you have a patient with intense thirst, polyuria, and inability to concentrate urine, and you get the following lab results, what diagnosis should you make?
- ↓ ADH - Urine specific gravity <1.006 - Serum osmolarity >290 mOsm/L - Hyperosmotic volume contraction |
Central Diabetes Insipidus
* Only way to distinguish from Nephrogenic is based on ↓ ADH |
|
|
If you have a patient with intense thirst, polyuria, and inability to concentrate urine, and you get the following lab results, what diagnosis should you make?
- Normal ADH - Urine specific gravity <1.006 - Serum osmolarity >290 mOsm/L - Hyperosmotic volume contraction |
Nephrogenic Diabetes Insipidus
* Only way to distinguish from Central is based on normal ADH |
|
|
What are the following values in diabetes insipidus:
- ADH level - Urine specific gravity - Serum osmolarity - Type of volume contraction |
- ADH: ↓ if central or normal if nephrogenic
- Urine specific gravity: < 1.006 (dilute) - Serum osmolarity >290 mOsm/L (concentrated) - Hyperosmotic volume contraction |
|
|
How do you diagnose Central Diabetes Insipidus?
|
Water restriction test:
- No water intake for 2-3 hours - Followed by hourly measurements of urine volume / osmolarity and plasma Na+ concentration / osmolarity * Central: >50% ↑ in urine osmolarity * Nephrogenic: no change in urine osmolarity |
|
|
What should you do if after a water restriction test normal values are not clearly reached?
|
Give DDAVP (ADH analog) - this will improve central diabetes insipidus
|
|
|
How do you treat central diabetes insipidus?
|
- Intranasal DDAVP (ADH analog)
- Hydration |
|
|
How do you treat nephrogenic diabetes insipidus?
|
- HCTZ, indomethacin, amiloride
- Hydration |
|
|
What can cause excessive water retention, hyponatremia, urinary Na+ excretion, and urine osmolarity > serum osmolarity?
|
SIADH: Syndrome of Inappropriate Anti-Diuretic Hormone
|
|
|
What are the findings of SIADH?
|
- Excessive water retention
- Hyponatremia w/ continued urinary Na+ exretion - Urine osmolarity > serum osmolarity |
|
|
How does the body normally respond to water retention?
|
↓ Aldosterone (hyponatremia) to maintain near-normal volume status
|
|
|
What are the possible consequences of the hyponatremia in SIADH?
|
Can lead to cerebral edema and seizures
|
|
|
When correcting hyponatremia in SIADH, what do you need to do? Why?
|
Correct hyponatremia slowly to prevent central pontine myelinolysis
|
|
|
What are the possible causes of SIADH?
|
- Ectopic ADH (small cell lung cancer)
- CNS disorders / head trauma - Pulmonary disease - Drugs (eg, cyclophosphamide) |
|
|
How do you treat SIADH?
|
- Fluid restriction
- IV hypertonic saline - Conivaptan (ADH inhibitor) - Tolvaptan (ADH receptor antagonist) - Demeclocycline (ADH antagonist) |
|
|
What can cause under-secretion of pituitary hormones (hypo-pituitarism)?
|
- Non-secreting pituitary adenoma, craniopharyngioma
- Sheehan syndrome - Empty sella syndrome - Brain injury, hemorrhage - Radiation |
|
|
What tumors can cause hypo-pituitarism?
|
- Non-secreting pituitary adenoma
- Craniopharyngioma |
|
|
What is Sheehan syndrome?
|
Ischemic infarct of pituitary following post-partum bleeding, usually presents with a failure to lactate (no prolactin being released because of pituitary damage)
|
|
|
What causes empty sella syndrome? Effect?
|
- Atrophy or compression of pituitary, often idiopathic
- Common in obese women - Leads to hypopituitarism |
|
|
What kind of brain injury can cause hypo-pituitarism?
|
- Hemorrhage (pituitary apoplexy)
- General brain trauma - Radiation |
|
|
How do you treat hypo-pituitarism?
|
Hormone replacement therapy:
- Corticosteroids - Thyroxine - Sex steroids - Human growth hormone |
|
|
What cause of hypo-pituitarism is common in obese women?
|
Empty Sella Syndrome
- Atrophy or compression of pituitary, often idiopathic |
|
|
What are the acute manifestations of diabetes mellitus?
|
- Polydipsia
- Polyuria - Polyphagia - Weight loss - DKA (diabetic ketoacidosis) (type 1) - Hyperosmolar coma (type 2) |
|
|
What can, although rarely, cause Diabetes Mellitus?
|
Unopposed secretion of GH and Epinephrine
|
|
|
What are the immediate consequences of an insulin deficiency (and glucagon excess)?
|
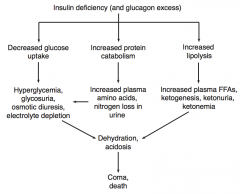
- Decreased glucose uptake
- Increased protein catabolism - Increased lipolysis |
|
|
What is the effect of decreased glucose uptake (due to insulin deficiency / glucagon excess)?
|
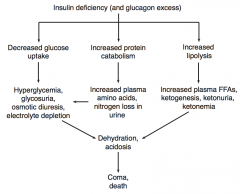
- Hyperglycemia
- Glycosuria (excess of sugar in the urine) - Osmotic diuresis - Electrolyte depletion |
|
|
What is the effect of increased protein catabolism (due to insulin deficiency / glucagon excess)?
|
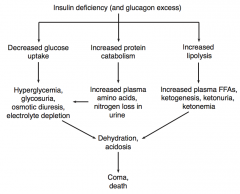
- Increased plasma amino acids
- Nitrogen loss in urine |
|
|
What is the effect of increased lipolysis (due to insulin deficiency / glucagon excess)?
|
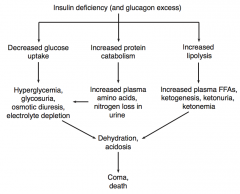
- Increased plasma FFAs
- Ketogenesis - Ketonuria - Ketonemia |
|
|
What is the combined effect of decreased glucose uptake, increased protein catabolism, and increased lipolysis (due to insulin deficiency / glucagon excess)?
|
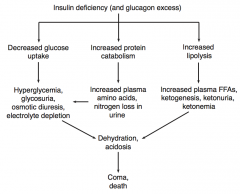
Dehydration and acidosis, which can cause coma or death
|
|
|
What are the types of damage due to chronic diabetes?
|
- Non-enzymatic glycosylation: small vessel and large vessel disease
- Osmotic damage: neuropathy, cataracts |
|
|
What are the manifestations of non-enzymatic glycosylation on small vessels in patients with chronic diabetes?
|
Diffuse thickening of basement membrane of small vessels leads to:
- Retinopathy - Glaucoma - Nephropathy |
|
|
How are the eyes of patients with chronic diabetes affected?
|

Small vessel disease due to diffuse thickening of basement membrane via non-enzymatic glycosylation:
- Retinopathy (picture): hemorrhage, exudates, microaneurysms, vessel proliferation - Glaucoma |
|
|
How are the kidneys of patients with chronic diabetes affected?
|
Small vessel disease (diffuse thickening of basement membrane) via non-enzymatic glycosylation:
- Nephropathy: nodular sclerosis, progressive proteinuria, chronic renal failure, arteriolosclerosis leading to HTN, Kimmelstiel-Wilson nodules) |
|
|
What are the manifestations of retinopathy in chronic diabetes mellitus?
|
- Hemorrhage
- Exudates - Microaneurysms - Vessel proliferation |
|
|
What are the manifestations of nephropathy in chronic diabetes mellitus?
|
- Nodular sclerosis
- Progressive proteinuria - Chronic renal failure - Arteriolosclerosis leading to HTN - Kimmelstiel-Wilson nodules |
|
|
What are the manifestations of non-enzymatic glycosylation on large vessels in patients with chronic diabetes?
|
- Large vessel atherosclerosis → cerebrovascular disease
- CAD → MI (most common cause of death) - Peripheral vascular occlusive disease - Gangrene → limb loss |
|
|
What is the most common cause of death in patients with Diabetes Mellitus?
|
Myocardial Infarction
|
|
|
What causes osmotic damage in patients with chronic diabetes?
|
Sorbitol accumulates in organs with aldose reductase and ↓ or absent sorbitol dehydrogenase
|
|
|
What are the manifestations of osmotic damage in patients with chronic diabetes?
|
- Neuropathy: motor, sensory, and autonomic degeneration
- Cataracts |
|
|
What tests can be used to assess a patient's diabetes mellitus?
|
- Fasting serum glucose
- Oral glucose tolerance test - HbA1c (reflects average blood glucose over prior 3 months) |
|
|
What is the primary defect in T1DM vs T2DM?
|
- T1DM: auto-immune destruction of β cells
- T2DM: ↑ resistance to insulin, progressive pancreatic β-cell failure |
|
|
Is insulin necessary in treatment of T1DM and T2DM?
|
- T1DM: always
- T2DM: sometimes |
|
|
What is the typical age of onset for patients with T1DM vs T2DM?
|
- T1DM: <30 years
- T2DM: >40 years *Exceptions commonly occur |
|
|
What is the association with obesity for T1DM vs T2DM?
|
- T1DM: none
- T2DM: associated |
|
|
Is there a genetic predisposition for T1DM vs T2DM?
|
- T1DM: relatively weak (50% concordance in identical twins), polygenic
- T2DM: relatively strong (90% concordance in identical twins), polygenic |
|
|
What is the association with HLA system for T1DM vs T2DM?
|
- T1DM: associated with HLA-DR3 and -DR4
- T2DM: no association |
|
|
What is the relative glucose intolerance in T1DM vs T2DM?
|
- T1DM: severe
- T2DM: mild to moderate |
|
|
What is the relative insulin sensitivity in T1DM vs T2DM?
|
- T1DM: high
- T2DM: low |
|
|
How common is ketoacidosis in T1DM vs T2DM?
|
- T1DM: common
- T2DM: rare |
|
|
How many β-cells are there in the islets relatively in T1DM vs T2DM?
|
- T1DM: ↓ β-cell numbers
- T2DM: variable (with amyloid deposits) |
|
|
What is the relative serum insulin level in T1DM vs T2DM?
|
- T1DM: ↓
- T2DM: Variable |
|
|
Are the classic symptoms of polyuria, polydipsia, polyphagia, and weight loss seen in T1DM vs T2DM?
|
- T1DM: common
- T2DM: sometimes |
|
|
What is the histologic appearance of the Islets of Langerhans in T1DM vs T2DM?
|
- T1DM: islet leukocytic infiltrate (auto-immune process)
- T2DM: islet amyloid polypeptide (IAPP) deposits |
|
|
What is one of the most important complications of diabetes (usually type 1)?
|
Diabetic Ketoacidosis
|
|
|
What causes diabetic ketoacidosis?
|
- Complication of diabetes (usually type 1)
- Usually due to ↑ insulin requirements from ↑ stress (eg, infection) - Excess fat breakdown and ↑ ketogenesis from ↑ FFAs, when are converted into ketone bodies |
|
|
What are the types of ketone bodies? Which is more common in diabetic ketoacidosis?
|
β-Hydroxybutyrate > Acetoacetate
|
|
|
What are the signs / symptoms of diabetic ketoacidosis?
|
- Kussmaul respirations (rapid / deep breathing)
- Nausea / vomiting - Abdominal pain - Psychosis / delirium - Dehydration - Fruity breath odor (due to exhaled acetone) |
|
|
What are Kussmaul respirations? Sign of?
|
- Rapid / deep breathing
- Sign of diabetic ketoacidosis |
|
|
What causes the fruity breath odor in diabetics?
|
Diabetic ketoacidosis → exhaled acetone
|
|
|
What are the lab findings associated with diabetic ketoacidosis?
|
- Hyperglycemia
- ↑ H+ and ↓ HCO3- (anion gap metabolic acidosis) - ↑ Blood ketone levels - Leukocytosis - Hyperkalemia, but depleted intracellular K+ d/t transcellular shift from ↓ insulin |
|
|
What kind of acid/base disturbance occurs with diabetic ketoacidosis?
|
Anion gap metabolic acidosis
- ↑ H+ - ↓ HCO3- |
|
|
How are WBCs affected in diabetic ketoacidosis?
|
Leukocytosis
|
|
|
How is K+ balance affected in diabetic ketoacidosis?
|
- Hyperkalemia
- Depleted intracellular K+ because of transcellular shift from ↓ insulin |
|
|
What are the potenial complications of diabetic ketoacidosis?
|
- Life-threatening mucormycosis (usually caused by Rhizopus infection)
- Cerebral edema - Cardiac arrhythmias - Heart failure |
|
|
How do you treat diabetic ketoacidosis?
|
- IV fluids
- IV insulin - K+ (to replete intracellular stores) - Glucose if necessary to prevent hypoglycemia |
|
|
What is the source of an insulinoma? What is its effect?
|
- Tumor of β cells of pancreas
- Over-produces insulin → hypoglycemia |
|
|
What are the common symptoms with an insulinoma?
|
Whipple triad of episodic CNS symptoms:
- Lethargy - Syncope - Diplopia |
|
|
What lab values are associated with insulinoma?
|
- ↓ Blood glucose
- ↑ C-peptide (vs exogenenous insulin use which would cause similar findings but have low/normal C-peptide) |
|
|
How do you treat an insulinoma?
|
Surgical resection of tumor in pancreas
|
|
|
What is the most common malignancy in the small intestine?
|
Carcinoid Syndrome
|
|
|
What causes Carcinoid Syndrome?
|
Rare syndrome caused by carcinoid tumors (neuroendocrine cells), especially metastatic small bowel tumors, which secrete high levels of serotonin (5-HT)
|
|
|
What is necessary for a carcinoid tumor of the small intestine to cause Carcinoid Syndrome?
|
- Tumor secretes high levels of serotonin (5-HT)
- Tumor must not be restricted to the GI tract because 5-HT undergoes first pass metabolism in the liver |
|
|
What are the symptoms of Carcinoid Syndrome?
|
- Recurrent diarrhea
- Cutaneous flushing - Asthmatic wheezing - Right sided valvular disease |
|
|
What are the lab changes associated with Carcinoid Syndrome?
|
- ↑ 5-hydroxyindoleacetic acid (5-HIAA) in urine
- Niacin deficiency (pellagra - diarrhea, dementia, dermatitis) |
|
|
How do you treat Carcinoid Syndrome?
|
- Resection of carcinoid tumor
- Somatostatin analog (eg, octreotide) |
|
|
What is the rule of 1/3 for Carcinoid Syndrome?
|
- 1/3 metastasize
- 1/3 present with 2nd malignancy - 1/3 are multiple |
|
|
What causes Zollinger-Ellison Syndrome?
|
- Gastrin-secreting tumor of pancreas or duodenum
- Leads to acid hyper-secretion → recurrent ulcers in distal duodenum and jejunum |
|
|
Zollinger-Ellison Syndrome leads to ulcers where?
|
Distal duodenum and jejunum
|
|
|
What symptoms does a patient with Zollinger-Ellison Syndrome typically present with?
|
- Abdominal pain (peptic ulcer disease, distal ulcers)
- Diarrhea (malabsorption) |
|
|
What may Zollinger-Ellison Syndrome be associated with?
|
MEN 1
|
|
|
What are the types of Multiple Endocrine Neoplasias?
|
- MEN 1 (Wermer syndrome)
- MEN 2A (Sipple syndrome) - MEN 2B |
|
|
What kind of tumors are associated with MEN 1?
|
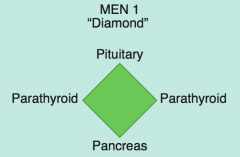
MEN 1 = 3 P's (diamond):
- Pituitary tumors (prolactin or GH) - Parathyroid tumors - Pancreatic endocrine tumors (Zollinger Ellison syndrome, insulinomas, VIPomas, glucagonomas-rare) |
|
|
Besides pituitary tumors, parathyroid tumors, and pancreatic endocrine tumors, what else is associated with MEN 1?
|
- Kidney stones
- Stomach ulcers |
|
|
What kind of tumors are associated with MEN 2A?
|
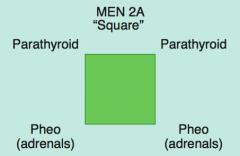
MEN 2A: 2 P's (square):
- Parathyroid (hyperplasia) - Pheochromocytoma (adrenals) - Medullary Thyroid Carcinoma (secretes calcitonin) |
|
|
Besides medullary thyroid carcinoma, pheochromocytoma, and parathyroid hyperplasia, what else is associated with MEN 2A?
|
Associated with RET gene mutations
|
|
|
What kind of tumors are associated with MEN 2B?
|
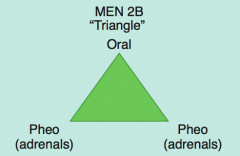
MEN 2B: 1 P (triangle):
- Pheochromocytoma (adrenals) - Oral / intestinal ganglioneuromatosis (mucosal neuromas) - Medullary Thyroid Carcinoma (secretes calcitonin) |
|
|
Besides medullary thyroid carcinoma, pheochromocytoma, and oral/intestinal ganglioneuromatosis (mucosal neuromas), what else is associated with MEN 2B?
|
Marfanoid habitus
- Resembling symptoms of Marfan Syndrome - Long limbs, arachnodactyly, and hyperlaxity - Arm span is greater than the height of the individual Associated with RET gene mutation |
|
|
How are MEN syndromes inherited? Other associated genetic changes?
|
- All are autosomal dominant (think "MEN are dominant" - or so they think)
- Associated with RET gene mutation in MEN 2A and 2B |