![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
What can cause Cushing syndrome? |
Excess cortisol due to a variety of causes: |
|
|
What is the number one cause of Cushing syndrome? Characteristics? |
Exogenous corticosteroids: results in ↓ ACTH and bilateral adrenal atrophy |
|
|
What causes of Cushing syndrome result in ↓ ACTH? Effect on adrenals?
|
- Exogenous steroids - bilateral adrenal atrophy
- Primary adrenal adenoma, hyperplasia, or carcinoma - atrophy of uninvolved adrenal gland |
|
|
What can primary adrenal adenoma / hyperplasia / carcinoma produce?
|
- ↑ Cortisol (= Cushing Syndrome)
OR - ↑ Aldosterone (1° Aldosteronism = Conn Syndrome) |
|
|
What is Conn Syndrome?
|
1° Aldosteronism (due to primary adrenal adenoma, hyperplasia, or carcinoma)
|
|
|
What causes of Cushing syndrome result in ↑ ACTH? Effect on adrenals?
|
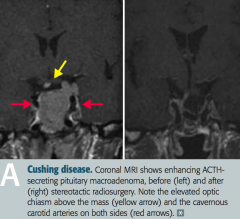
ACTH-secreting pituitary adenoma (Cushing disease)
- Paraneoplastic ACTH secretion: small cell lung cancer, bronchial carcinoids - Bilateral adrenal hyperplasia |
|
|
What is responsible for the majority of the endogenous cases of Cushing Syndrome?
|
Cushing Disease
- ACTH-secreting pituitary adenoma - Paraneoplastic ACTH secretion: small cell lung cancer, bronchial carcinoids |
|
|
What are the findings associated with Cushing Syndrome?
|

- Hypertension
- Weight gain - Moon facies - Truncal obesity - Buffalo hump - Hyperglycemia (insulin resistance) - Skin changes (thinning, striae) - Osteoporosis - Amenorrhea - Immune suppression |
|
|
How do you screen for Cushing Syndrome?
|
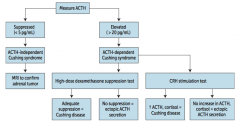
** Measure serum ACTH ** |
|
|
What should you suspect / do if a patient you suspect of having Cushing Syndrome has a low ACTH (<5 pg/mL)?
|
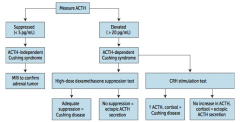
Suspect ACTH-independent Cushing Syndrome (primary adrenal adenoma, hyperplasia, or carcinoma)
* Order MRI to confirm adrenal tumor |
|
|
What should you suspect / do if a patient you suspect of having Cushing Syndrome has a high ACTH (>20 pg/mL)?
|
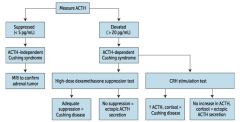
Suspect ACTH-dependent Cushing Syndrome |
|
|
What diagnosis does a patient you suspect of having Cushing Syndrome, with an elevated ACTH, and adequate suppression via high-dose dexamethasone suppression test?
|
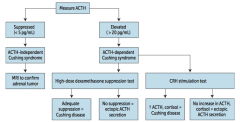
Cushing Disease (ACTH-secreting pituitary adenoma)
|
|
|
What diagnosis does a patient you suspect of having Cushing Syndrome, with an elevated ACTH, and no suppression via high-dose dexamethasone suppression test?
|
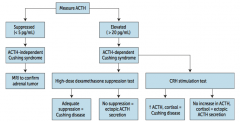
Ectopic ACTH secretion (paraneoplastic syndrome: small cell lung cancer or bronchial carcinoids)
- Ectopic secretion will not decrease with dexamethasone because the source is resistant to negative feedback |
|
|
What diagnosis does a patient you suspect of having Cushing Syndrome, with an elevated ACTH, and after after a CRH stimulation test there was ↑ ACTH and cortisol?
|
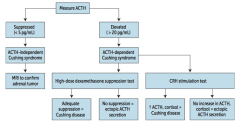
Cushing Disease (ACTH-secreting pituitary adenoma) |
|
|
What diagnosis does a patient you suspect of having Cushing Syndrome, with an elevated ACTH, and after after a CRH stimulation test there was no increase in ACTH and cortisol?
|
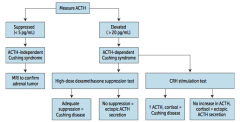
Ectopic ACTH secretion
- Ectopic secretion will not increase with CRH because pituitary ACTH is suppressed |
|
|
What are the causes of primary hyperaldosteronism?
|
- Adrenal hyperplasia
- Aldosterone secreting adrenal adenoma (Conn syndrome) (May be unilateral or bilateral) |
|
|
What are the consequences of adrenal hyperplasia or aldosterone-secreting adrenal adenoma?
|
Primary Hyperaldosteronism:
- Hypertension - Hypokalemia - Metabolic alkalosis - Low plasma renin - Normal Na+ due to aldosterone escape → no edema |
|
|
How do you treat primary hyperaldosteronism?
|
Surgery to remove the tumor and/or spironolactone (K+ sparing diuretic that acts as an aldosterone antagonist)
|
|
|
What are the causes of secondary hyperaldosteronism?
|
- Renal artery stenosis |
|
|
What are the consequences of renal artery stenosis, CHF, cirrhosis, or nephrotic syndrome?
|
Secondary Hyperaldosteronism |
|
|
How do you treat secondary hyperaldosteronism?
|
Spironolactone (K+ sparing diuretic that acts as an aldosterone antagonist)
|
|
|
What form of hyperaldosteronism is associated with a high plasma renin?
|
Secondary Hyperaldosteronism
- In primary, there is negative feedback to decrease renin - In secondary, the high renin is what is causing the high aldosterone |
|
|
What are the causes of primary adrenal insufficiency?
|
Addison Disease - CHRONIC process
- Atrophy of adrenals - Destruction by disease: auto-immune, TB, metastasis Waterhouse-Friderichsen Syndrome - ACUTE process - Adrenal hemorrhage associated with Neisseria meningitidis, septicemia, DIC, and endotoxic shock |
|
|
What are the implications of Addison Disease?
|
- Deficiency of aldosterone and cortisol
- Hypotension (hyponatremic volume contraction) - Hyperkalemia - Acidosis - Skin and mucosal hyperpigmentation |
|

What causes the skin hyperpigmentation in Addison Disease?
|

MSH (melanocyte stimulating hormone): by-product of ↑ ACTH production from pro-opiomelanocortin (POMC) |
|
|
How is Addison Disease characterized?
|
- Adrenal Atrophy
- Absence of hormone production, involving all three cortical divisions (but spares medulla) |
|
|
How do you distinguish primary adrenal insufficiency from secondary?
|
Secondary adrenal insufficiency would have:
- ↓ Pituitary ACTH production - No skin/mucosal hyperpigmentation - No hyperkalemia |
|
|
What are the electrolyte and acid/base balance changes in primary adrenal insufficiency?
|
- Hyponatremia
- Hyperkalemia - Acidosis |
|
|
What is the name of the syndrome causing ACUTE 1° adrenal insufficiency? Cause?
|
Waterhouse-Friderichsen Syndrome
- Adrenal hemorrhage associated with Neisseria meningitidis septicemia, DIC, and endotoxic shock |
|
|
What is the most common tumor of the adrenal medulla in children? When specifically?
|
Neuroblastoma
- Usually <4 years old |
|
|
What is the origin of a neuroblastoma?
|
Neural crest cells
|
|
|
Where can a neuroblastoma appear?
|
Occurs anywhere along the sympathetic chain
|
|
|
What is the most common presentation of Neuroblastoma?
|
- Abdominal distension
- Firm, irregular mass that can CROSS THE MIDLINE - Usually in children < 4 years old - Less likely to develop hypertension |
|
|
When you have a firm, irregular mass that crosses the midline of a young child, what diagnosis should you think of?
|
Neuroblastoma
|
|
|
When you have a smooth mass that does not cross the midline of a young child, what diagnosis should you think of?
|
Wilms tumor (nephroblastoma)
- Most common renal malignancy of early childhood (ages 2-4) |
|
|
What lab studies are associated with a Neuroblastoma?
|
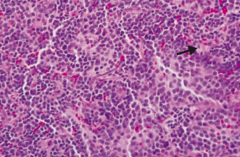
- Homovanillic acid (HVA), a breakdown product of dopamine, is increased in urine
- Bombesin (+) - LM: rosettes (arrow) and classic small, round, blue/purple nuclei |
|
|
What genetic change is associated with Neuroblastoma?
|
Over-expression of the N-myc oncogene
|
|
|
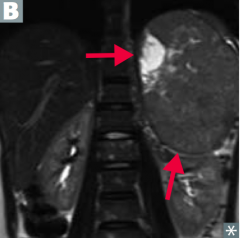
What is the most common tumor of the adrenal medulla in adults?
|
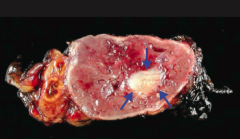
Pheochromocytoma
|
|
|
What is a pheochromocytoma derived from?
|
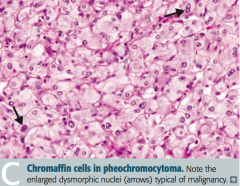
Chromaffin cells (arise from neural crest)
|
|
|
What rule can you use to remember characteristics of a pheochromocytoma?
|
Rule of 10s:
- 10% malignant - 10% bilateral - 10% extra-adrenal - 10% calcify - 10% in kids |
|
|
What does a pheochromocytoma do?
|
Most tumors secrete epinephrine, norepinephrine, and dopamine → episodic hypertension |
|
|
What genetic change is pheochromocytoma associated with?
|
- Von Hippel-Lindau disease
- MEN 2A - MEN 2B |
|
|
What symptoms are typical of pheochromocytoma?
|
Symptoms occur in "spells" - relapse and remit:
Episodic hyperadrenergic symptoms (5 P's): - Pressure (↑ BP) - Pain (headache) - Perspiration - Palpitations (tachycardia) - Pallor |
|
|
What are the lab findings associated with a pheochromocytoma?
|
- ↑ Urinary VMA (breakdown product of NE and Epi)
- ↑ Plasma catecholamines (NE, Epi, etc) |
|
|
How do you treat pheochromocytoma?
|
1. Irreversible α-antagonist (phenoxybenzamine)
2. β-blockers 3. Tumor resection ** α-blockade must be achieved before giving β-blockers to avoid a hypertensive crisis ** |
|
|
For what diagnosis must you treat the patient first with α-antagonists before β-blockers? Why?
|
For treatment of Pheochromocytoma:
This is necessary to avoid a hypertensive crisis |