![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
- 3rd side (hint)

Definition. Causes. |
Miosis: Both small <3mm - narcotic-related - pontine stroke - neurosyphilis - Wernicke's encephalopathy |
|
|

Definition. Causes. |
Mydriasis: both large >5mm - sympathomimetic drugs (cocaine) - reactive to light - medullary stroke = fixed, dilated - anticholinergic drugs (atropine = fixed, belladonna) |
|
|

|
Aniscoria: > 0.5mm difference (if less = normal) - anticholinergic drops - CN3 palsy - Holmes-Adie syndrome - Horner's syndrome - Glaucoma crises |
|
|
|
What is a Glaucoma Crisis? |
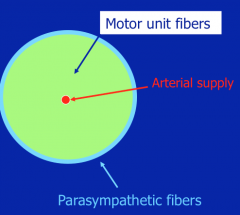
pain, red, cloudy cornea, external pressure kills the parasympathetic fibers first producing change in pupillary size. |
|
|
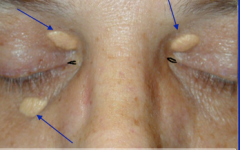
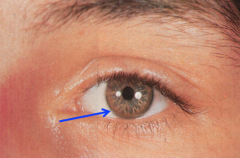
Define. Cause. |
Xanthelasma = hypercholesterolemia Subcutaneous accumulation of cholesterol around the lacrimal gland. |
|
|
Define. Cause. |
Periorbital edema = Graves' Disease |
|
|

Define. Cause. |
Periorbital edema in diffuse edematous state = anasarca (accumulation of albumin) Nephrotic syndrome. |
|
|

Define. Cause. |
Lacrimal gland enlargement. Bilateral: - alcoholism (usu with parotid gland enlargement) - Sjogren's syndrome - sarcoidosis |
|
|

Define. Cause. |
(oculomotor palsy) CN 3 palsy: eye deviated laterally and inferiorly (CN 4 - depression and intorsion; CN 6 - abduction). May also have dilated pupil (loss of parasympathetic innervation). Ptosis (loss of levator). Nerve infarction occurs from compromised vascular supply (inside out) may spare pupillary function - diabetes External Pressure (outside-in) will usually effect pupillary size initially then motor fibers -Tumor - uncal herniation (greatest fear) - aneurysm - infarct |
|
|

Define. Cause. |
(abducens palsy) CN 6: failure to abduct due to increased intracranial pressure. Causes include: - meningeal processes (carcinomatous and infectious meningitis) - tumor - cavernous sinus process = carotid artery aneurysm or rhino cerebral mucormycosis - diabetes (CN VI is the longest and most likely to be involved in neuroapthy) - vascular disease with focal brainstem ischemia (involving the nucleus in the pons) - NOT MS: no increase in intracranial pressure and does not involve cranial nerves (limited to white matter) but involvement of nuclei of the nerves does occur |
|
|
|
Rhinocerebral mucormycosis - definition, exam and treatment |
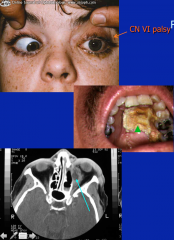
- Devastating fungal infection seen in immunocompromised patients and poorly controlled DM - begins as sinus infection but spreads to involve orbit, palate and brain - look for necrotic eschar (on palate), CN palsies and facial asymmetry - management: antifungal and aggressive surgery |
|
|

Define. Causes. |
intranuclear opthalmoplegia (INO): failure to adduct. Due to involvement of medial longitudinal fasciculus. Causes include: - brainstem stroke (unilateral) - multiple sclerosis (bilateral) - diabetes |
|
|

Define. Causes. |
Bilateral ptosis: diffuse weakness. Causes include: - myasthenia gravis = weakness us beginning with muscles of the face (ptosis, EOM weakness, dysphagia) - Guillain-Barre syndrome (Miller Fisher variant) - Botulism |
|
|

Define. Causes |
Unilateral ptosis: CN3 palsy. Causes include: - uncal herniation - diabetes - infarct |
|
|
Define. Causes. |
Unilateral ptosis: Horner's syndrome. Ipsilateral involvement of sympathetic chain - ptosis, miosis, and anhydrosis. Affected pupil reacts to light. Causes: - cancer (lung cancer with spinal mets) - spinal cord disease - neck mass - vascular aneurysm/dissection |
|
|

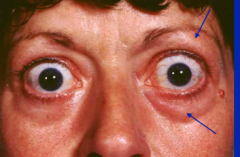
Define. Causes. |
Bilateral proptosis = Eyes pushed out. Graves' disease - not simply hyperthyroidism, not lid lag. |
|
|

Define. Causes. |
Unilateral proptosis: causes include: - retro-ocular tumor - periorbital infection - cavernous sinus infection |
|
|

Define. Causes. |
Scleral icterus/jaundice (yellow): causes include: - hepatobilliary disease - brisk hemolysis - congenital liver disease syndromes: Crippler-Najjar, Rotor, Dubin-Johnson, Wilson's diseaes - melanoma can metastasize to the liver which may produce jaundice to to functional compromise (also can involve the eye producing therapeutic enucleation with subsequent placement of glass prosthesis) |
|
|

Define. Causes. |
Blue Sclera: osteogenesis imperfecta |
|
|
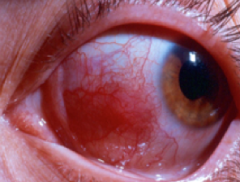
Define. Causes. |
Scleritis/episcleritis = deep inflammation of the sclera and the vessels. Begins with red, inflamed sclera and later may cause scleral thinning with ability to see urea. causes include: - rhematoid arthritis - vasculitis |
|
|
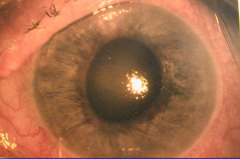
Define. |
Glaucoma crisis with corneal edema = cloudy/steamy |
|
|

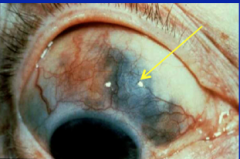
Define. Causes. |
Corneal arcus = arcus senilis. Hyperlipidemia (less than 40 yo) |
|
|
Define. Causes. |
Keiser-Fleisher ring = Wilson's disease (copper deposition) |
|
|
Define. Causes. What is another thing that this disease can produce?
|
Roth spots = hemorrhage with a white center corresponding to a cotton wool spot. Infectious endocarditis Infectious endocarditis can also produce endophthalmitis via hematogenous spread of infection (produces a painful, red eye) |
|
|

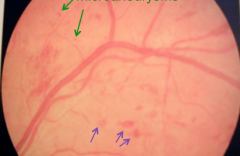
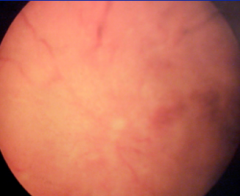
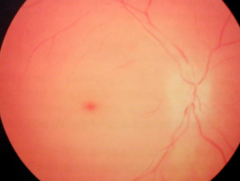
Define. Causes. |
Cotton Wool Spots = reflect the edge of a micro-retinal infarct associated with: - type II DM - hypertension - systemic lupus - venous infarcts |
|
|
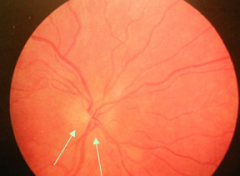
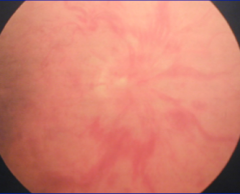
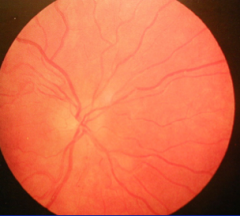
Define. Causes. |
Papilledema = blurring of the optic disk Increased intracranial pressure |
|
|
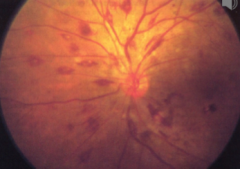
Define. Causes. |
Diabetic retinopathy. Purple = Flame hemorrhages green = microaneurysms dot and blot retinopathy = reflects retinal capillary microanaerysms and intra-retinal hemorrhages |
|
|
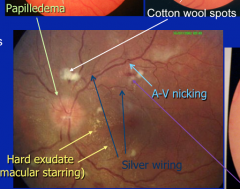
Define. |
Hypertensive retinopathy, grade 4 papiledema cotton wool spots A-V nicking flame hemorrhages silver wiring hard exudate = macular starring |
|
|
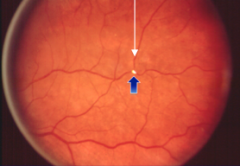
Define. Cause. |
Hollenhorst crystal - reflecting cholesterol embolization from atherosclerotic plaque |
|
|
|
What is Multiple sclerosis? |
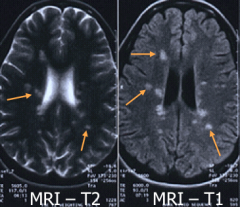
White matter disease caused by autoimmunity directed against myelin. |
|
|
|
What are the symptoms of MS? What is Lhermitte's sign? |
Symptoms vary depending on area of involvement including: - weakness - sensory deficits - visual loss- diplopia - gait disorders - generalized fatigue Lhermitte's sign = transient electric shock-like sensation produced by neck flexion, indicating cervical spinal cord pathology |
|
|
|
What is the Argyll Robertson Pupil? Which nucleus is involved? |
Involvement of the Edinger-Westphal nucleus. Small, irregular pupils that do not react to light, but do constrict during accommodation. |
|
|
|
What diseases are associated with an Argyll Robertson pupil? |
Diagnostic of neurosyphilis (tabes dorsalis) now commonly seen in DM, lyme disease and MS.NOT with myasthenia gravis and ALS which produce muscle weakness (via different mechanisms) but NOT associated with pupillary abnormalities. |
|
|
|
What is the Marcus Gunn pupil? |

Abnormality of the swinging light test producing a large pupil. It is an afferent abnormality. |
|
|
|
What is Holmes-Adie Syndrome? How does it present? |
Irregular dilated pupil (Aniscoria) - initially unilateral, may progress to bilateral involvement over time. Delayed constriction to accommodation takes about 5-10 minutes. Reacts to instilled medications. Associated with loss of deep tendon reflexes. |
|
|
Cause. |
Papilledema from Malignant hypertension. High pressure transmitted through optic nerve due to elevated systemic arterial pressure. |
|
|
Cause. |
Papilledema from Central retinal vein occlusion. Indicates high pressure transmitted through optic nerve due to venous pressure (eye DVT) |
|
|
Cause. |
Papilledema from brain tumor. Indicates high pressure transmitted through optic nerve through high intracranial pressure (brain tumor, meningitis) |
|
|
|
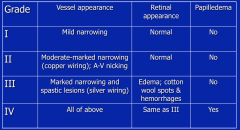
Describe the 4 grades of hypertensive retinopathy evaluated by fundoscopy in terms of vessel appearance, retinal appearance and papilledema. |
|
|
|
|
What is copper wiring indicative of? |
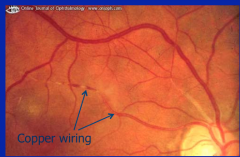
Hypertensive retinopathy |
|
|
|
Central Reitnal artery occlusion. Pale and avascular retina. |
|
|
|
Most common variant of Osteogenesis Imperfecta and its clinical features. |
Disorder of collagen production. Most common variant (type 1) has AD inheritance. Clinical features include recurrent fractures (usu before puberty) triangular shaped face, blue sclera, hearing loss, scoliosis, loose joints and brittle teeth. Hearing loss, not visual impairment is typical. |
|
|
|
• Abducens palsy (CN 6)
|
presents as an inability to abduct the involved eye. This nerve has a relatively long course in the subarachnoid space and cavernous sinus, and as such, may be involved by meningeal processes (e.g. infectious meningitis), diseases associated with neuropathy (e.g. diabetes mellitus), cavernous sinus diseases (e.g. carotid artery aneurysm, rhinocerebral mucormycosis) and diseases that cause increased intracranial pressure (e.g. brain tumor).
|
|
|
|
• Arcus senilis
|
white corneal ring associated with hyperlipidemia in patients < 40 years of age (normal finding in older patients).
|
|
|
|
• Argyll Robertson pupil
|
caused by damage to the Edinger-Westphal nucleus, this was originally described in neurosyphilis. The pupils are small and do not react to light but do constrict (if closely examined) to the accommodation maneuver.
|
|
|
|
• Blue sclera
|
although rarely reported in other entities, this finding strongly suggests osteogenesis imperfect, a disease associated with recurrent bone fracture, short stature, scoliosis, hearing loss and skin laxity.
|
|
|
|
• Cotton wool spot
|
white retinal lesion reflecting a micro-infarct, this can be seen in many diseases including diabetes and hypertension.
|
|
|
|
• Diabetic retinopathy
|
as for hypertension, the fundoscopic exam may reveal microvascular complications in diabetes. Potential finding may include microaneurysms and intraretinal microhemorrhages (aka dot and blot changes), cotton wool spots, flame hemorrhages, and vessel proliferation, but diabetes alone should not produce papilledema.
|
|
|
|
• Hollenhorst crystal
|
a small bright lesion in a small retinal artery indicating cholesterol embolization and atherosclerosis.
|
|
|
|
• Holmes-Adie syndrome
|
part of a systemic neurologic syndrome manifested as an irregular dilated pupil that has a delayed constriction to light. Initially unilateral, this frequently progresses to involve both eyes and can be associated with a lack of deep tendon reflexes (areflexia). These pupils respond briskly to instilled medications, underscoring that the pathogenesis involves denervation.
|
|
|
|
• Hypertensive retinopathy
|
the fundoscopic exam allows direct assessment of the microvascular effects of hypertension. The slideshow provides a table showing the grading of hypertensive retinopathy. Papilledema in conjunction with the other findings denotes grade IV.
|
|
|
|
• Intranuclear ophthalmoplegia (INO)
|
this disorder is produced by damage to the medial longitudinal fasciculus running in the brainstem – this is not a cranial nerve palsy! The exam finding is the inability to adduct the involved side – it may be unilateral or bilateral
|
there may be nystagmus of abducting eye. Multiple sclerosis is the most common cause of INO, but brainstem stroke and rarer pathology can potentially produce this finding.
|
|
|
• Marcus Gunn pupil (afferent pupillary abnormality)
|
the involved eye does not react to light directly but does constrict to light directed to the opposite eye (consensual response).
|
|
|
|
• Oculomotor palsy (CN 3)
|
a complete Oculomotor palsy presents with (3) components: 1) a downward and laterally deviated eye, 2) unilateral ptosis and 3) dilated pupil (mydriasis). The parasympathic fibers mediating pupillary constriction tend to run on the outside of the nerve, and the fibers innervating extraocular muscles in the nerve core. As such, partial Oculomotor palsy can occur with nerve core infarction (spares pupillary function) or early in the course of external compression (only a “blown” pupil).
|
|
|
|
• Papilledema
|
blurring of the optic disc margins produced by increased pressure transmitted through the optic nerve. As such, any disorder leading to increased intracranial pressure (ICP) may produce this: hypertensive crisis (aka malignant hypertension), brain tumor or abscess, meningitis – retinal vein occlusion can produce papilledema without increased ICP.
|
|
|
|
• Roth spot
|
representing hemorrhage within a cotton wool spot, this finding was initially described in infective endocarditis, but also can be seen in systemic lupus, diabetes and leukemia (and others).
|
|
|
|
• Xanthelasma
|
yellowish subcutaneous lipid collection adjacent to medial canthus of eye that is indicative of hyperlipidemia.
|
|