![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
77 Cards in this Set
- Front
- Back

Describe Weber Test |
Test for lateralization (normally heard in midline) ex: sound localizes to right ear, indicates: - right-sided conductive hearing loss, or - left-sided sensorineural hearing loss |
|

Describe Rinne Test |
Compares sound conduction of air to bone. Normally air > bone conduction |
|

Describe Sinus Transillumination |
Opacified sinus does not transilluminate well (fluid) useful in excluding maxillary sinusitis, but specificity is poor may be applied to frontal sinus |
|
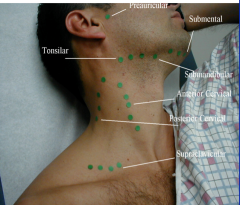
Describe a lymph node exam |
Describe the size and quality of nodes malignant nodes often are rock-hard and fixed to underlying structures |
|
|
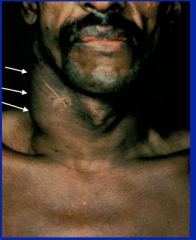
Miliary Tuberculosis adenopathy |
|
|
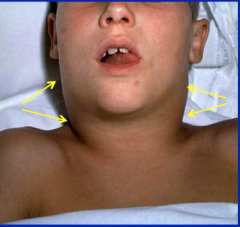
Diphtheria adenopathy = bull neck lymphadenopathy |
|
|
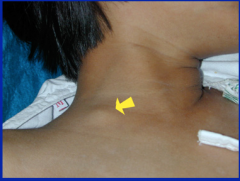
Hodgkin's disease adenopathy = unilateral, firm, thick |
|

|
Keloid = exuberant scar formation following skin trauma - can reoccur |
|

|
Relapsing polychondritis: inflamed external ear, inflammation of underlying cartilage, red |
|

|
Psoriasis: auditory canal involvement |
|

|
Ramsay Hunt syndrome: zoster of geniculate ganglion w/facial nerve palsy |
|

|
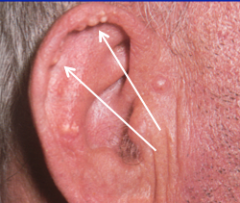
Frank's sign: diagonal earlobe crease associated with CAD |
|
|
Tophaceous gout: urate crystal deposition. Nontender, firm |
|

|
|
|
|
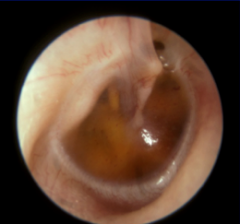
Serous otitis media = eustatian tube dysfunction, not infected; usu associated with viral infections and allergies. |
|

|
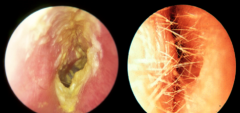
purulent otitis media = red bulging membrane with purulent material behind TM - eustation tube dysfunction that leads to infection; usu by S. pneumo, S. pyogenes, S. aureus, H. influenza Sx: earache and fever and eventually long term hearing loss, mastoiditis can occur (common in adults) |
|

|
mastoiditis = long standing purulent otitis media that leads to infection in the mastoid requiring surgical drainage |
|
|
otitis externa cellulitis can occur in swimmers if you manipulate the pinna or tragus it is tender with otitis externa (but not with otitis media) |
|
|
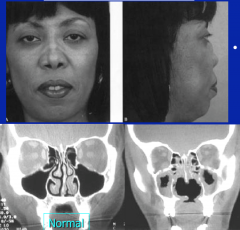
Septal perforation and saddle nose deformity (obliteration of nasal septum leading to drop in the bridge of the nose). Both conditions relate to destruction of nasal cartilage, cause include: - local trauma (performation) - cocaine abuse (vasoconstriction leads to ischemia and erosion of cartilage) - relapsing polychondritis - granulomatosis with polyangiitis (Wegner's granulomatosis) - congenital syphilis - sarcoidosis |
|
|
polyps = soft, jelly-like overgrowths produced in patients with repeated sinus inflammation (allergic rhinitis) - produce symptoms through obstruction (sinusitis, anosmia) but overall painless - asthma is a frequent concomitant condition |
|
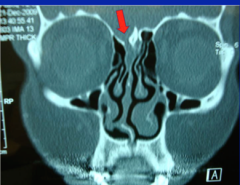
Define. Symptoms. Exam. Complications. |
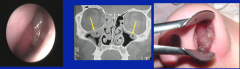
Ethmoid sinusitis = complication of sinus ostia obstruction (ex: nasal polyp) Sx: facial and maxillary tooth pain, sinus congestion exam: facial and maxillary tooth tenderness; abnormal transillumination complications: periorbital cellulitis, meningitis, subdural empyema, cranial sinus thrombosis |
|
|
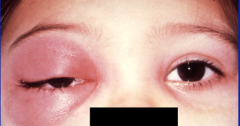
Periorbital cellulitis due to ethmoid sinusitis. Infection escapes from sinus and produces periorbital inflammation if it gets into the orbital cavity. pretty rare, but should be a concern. |
|

|
Gingival hyperplasia caused by antiseizure medication (phenytoin, Nifedipine). also seen with cyclosporin and calcium channel blockers. Leukemic infiltration (acute myelogenous leukemia) may mimic this finding. |
|

|
Apthous ulceration = painful shallow ulcers with white base and red margin. May follow minor trauma. Idiopathic etiology (HHV 6 may be a factor in pathogenesis). |
|
|
What is Behcet's disease? |
multi system disease with diffuse recurrent mucosal aphthous ulceration, vasculitis and CNS involvement, eye inflammation (iritis) venous thrombosis and skin lesions also noteworthy. common in turkey middle and far east. |
|
|
Oral leukoplakia = white plaques anywhere on the oral mucosa. In response to chronic irritation, a pre-malignant lesion from oral tobacco use, and is associated oral cancer. |
|

|
Hair leukoplakia = corrugate white lesion seen on the lateral aspect of the tongue. Reflects EBV-induced epithelial hyperplasia. suspect HIV/AIDS, think cell mediated immune-compromised. |
|
|

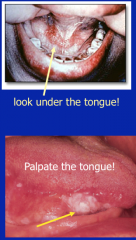
Oral cancer = most are squamous cell carcinoma from smoking and smokeless tobacco. Associated with low SES, alcohol and HPV. It is a firm lesion and may need to palpate, move tongue and remove dentures. |
|

|
Atrophic glossitis = smooth tonuge due to loss of papillae. May be painful or painless. |
|

|
Angular Cheilitis = look for signs of vitamin or mineral deficiency - stomatitis, peripheral neuropathy. Could be involved with a malabsorbative state of the GI tract. |
|

|
Tongue coating = overgrowth of tongue papillae, accumulation of dead cells, bacteria and debris or inflamed papillae. Can be scraped off. Causes include: - poor oral hygiene - dry mouth (mouth breathing) - intravascular volume depletion (shock) - smoking and chewing tobacco - low dietary roughage - Febrile illness (due to poor oral intake) |
|

|
Candidiasis (thrush) = painless white plaque usu involving tongue and/or palate. Difficult to scrape off. Process may spread to pharynx and esophagus where pain may occur. Predisposing conditions include: - steroid use - diabetes - immunocompromised states (HIV/AIDS) - pt with thrush often have risk factors for condyloma lata |
|

|
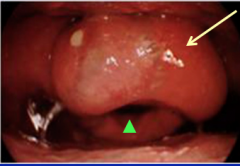
Acute pharyngitis with purulent exudate. Sx: sore throat, odynophagia (painful swallowing), possible fever and HA. Tender anterior cervical adenopathy usu with acute strep pharyngitis. Multiple causes, exudate limits considerations to: - GAS - also groups C, G (untx GAS at risk for rheumatic fever) - Fusobacterium - EBV (mononucleosis) - gonorrhea |
|

|
Pseudomembrane of diphtheria = infection due to C. diphtheria (gram + bacillus) most symptoms due to toxin elaboration. Involves pharynx and nasal mucosa. Sx: sore throat, fever, malaise, hoarseness. Exam: pharyngitis +/- pseudomembrane, bull's neck LAD, carditis, neuropathy |
|

|
Sniff sign in acute epiglottitis. leaning forward, extending neck to breathe better. |
|
Cause. Exam. |
Inflammed and edematous epiglottis with narrowed airway. Medical emergency caused by H. influenzae. Children present with fever, drooling, dysphagia, odynophagia. Exam: enlarged, red epiglottis. |
|
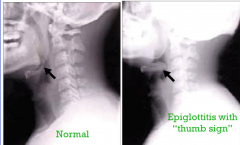
Treatment. |
Do not swab or manipulate! immediate surgical consultation indicated due to possible need for emergent airway. Get an X-ray. |
|

|
Parotitis in Mumps. Usually bilateral with high fever. Another bilateral parotitis condition is an inflammatory etiology such as sarcoidosis. |
|

|
Staphylococcal parotitis. Unilateral tender gland. drain the pus and give them antibiotics |
|

|
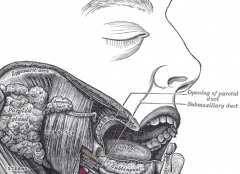
Purulent discharge from Stensen's duct |
|
|
• Aphthous ulceration
|
painful lesion of unknown etiology, often triggered by minor trauma. They are shallow and white-centered with erythematous border. Behcet’s disease is a multisystem disorder with diffuse mucosal aphthous ulceration, systemic vasculitis and CNS involvement.
|
|
|
• Coating (tongue)
|
white coating of the tongue is usually benign, caused by accumulation of dead cells and microbial colonization (often correlated with illness, poor oral intake and lack of oral hygiene). Other diagnoses to consider include candidiasis (aka thrush); often with burning pain, leukoplakia (see below) and secondary syphilis (aka condyloma lata).
|
|
|
• Epiglottitis
|
classically caused by H. influenza infection in childhood, this is a medical emergency. The patient will have a sore throat, difficult phonation, dysphagia, odynophagia, dyspnea and drooling. Exam reveals a red, enlarged epiglottis. Get immediate surgical consultation and do not swab the area; you may precipitate acute airway occlusion!
|
|
|
• Epistaxis (nosebleed)
|
the nasal mucosa is very vascular and subject to frequent local trauma and inflammation, explaining the frequency of its occurrence. Epistaxis is divided into anterior and posterior sites: anterior bleeding presents at the nares in the upright person, while posterior bleeding drains through the pharynx where it may be “coughed” up. Most cases will be benign in origin, but as with any clinical bleeding, the patient should be queried about possible bleeding diathesis (e.g. cirrhosis, anticoagulant medication, blood dyscrasia). Recurrent bleeding may also be a clue to more serious local pathology (e.g. tumor, vasculitis).
|
|
|
• Frank’s sign (aka diagonal earlobe crease)
|
has been associated with coronary artery disease (CAD) and peripheral vascular disease, the associated relative risk for this sign is debated, although bilateral, deep creases may convey a higher risk.
|
|
|
• Gingival hyperplasia
|
the most common cause is chronic use of phenytoin (Dilantin®). Other drugs to be considered include calcium channel blockers and cyclosporine. Leukemic infiltration (due to acute myelogenous leukemia) may mimic this condition.
|
|
|
• Glossitis
|
an abnormality of the tongue resulting in inflammation (often painful), there are multiple causes (often benign disorders). Chronic glossitis with atrophy may be a clue to a more widespread nutritional disorder (e.g. vitamin and mineral deficiency). Look for other signs of nutritional deficiency (e.g. angular cheilitis, anemia, peripheral neuropathy, dermatitis).
|
|
|
• Gorlin sign
|
the ability to touch the nose with tongue occurs in ~50% of subjects with Ehlers-Danlos syndrome, but < 10% of normal subjects can perform this feat.
|
|
|
• Hoarseness
|
encompassed change in voice character or strength and implies pathology of the vocal cords. This may be due to focal damage/neoplasm or nerve damage. Hoarseness persisting beyond (3) weeks demands evaluation, including in most cases direct laryngoscopic examination.
|
|
|
• Kaposi sarcoma
|
immunocompromised patients (esp. AIDS) may develop this neoplasm related to Human Herpes Virus 8 infection. It appears as raised or flat purple-red lesions anywhere on the oral mucosa (e.g. gingiva, tongue, palate).
|
|
|
• Koplik’s spot
|
white lesion on a red base found on the buccal mucosa and lips in measles.
|
|
|
• Lead lines
|
actually a series of grey-black dots observed 1 mm from the free margin of the gum. Lead lines are seen with heavy metal toxicity, including lead, bismuth, mercury, gold, silver, thallium and copper. Lead lines are not seen where teeth are absent.
|
|
|
• Leukoplakia
|
these are pre-malignant lesions associated with tobacco use. Hairy leukoplakia is a lesion generally found on the lateral aspect of the tongue in immunocompromised patients, esp. HIV/AIDS. This lesion reflects Epstein-Barr Virus induced epithelial hyperplasia. Unlike oral leukoplakia this is not pre-malignant. Discovering hairy leukoplakia in a patient should suggest HIV testing if status unknown.
|
|
|
• Lemierre’s syndrome (aka septic jugular vein thrombophlebitis)
|
usually begins as pharyngitis due to Fusobacterium necrophorum infection that invades tissue and spreads to the carotid sheath, producing the septic thrombosis of the jugular vein (resides in sheath). Patients present with fever, neck stiffness and dysphagia. Important exam findings are tenderness over jaw angle and sternocleidomastoid muscle. The infected thrombus may embolize to lung producing mass lesions that may cavitate (aka septic pulmonary embolism).
|
|
|
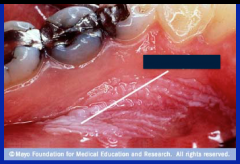
• Ludwig’s angina (aka submandibular space infection)
|
begins as an infection of mandibular teeth with extension into submandibular space. Expanding infection of this space elevates the floor of the mouth and tongue leading to airway compromise.
|
|
|
• Macroglossia (aka large tongue)
|
most commonly due to trauma or inflammation from caustic ingestions or allergic reactions (e.g. angioedema); however, can also be a finding in hypothyroidism, acromegaly and amyloidosis.
|
|
|
• Nasal pruritis (aka Wartenburg symptom)
|
intense and unrelieved nasal pruritis has been associated with brain tumor, esp. with involvement of the floor of the 4th ventricle.
|
|
|
• Nasal septal perforation and saddle nose deformity
|
processes that destroy the nasal cartilages produce these findings, including intranasal cocaine abuse, Granulomatosis with polyangiitis (formerly Wegener’s granulomatosis), congenital syphilis, sarcoidosis and relapsing polychondritis. The saddle nose deformity is a depression over the nasal bridge caused by collapse of the underlying cartilage.
|
|
|
• Parotitis
|
these glands may be inflamed and tender in multiple conditions including viral infections (e.g. mumps), inflammatory conditions (e.g. sarcoidosis, systemic lupus erythematosus), and many others. Unilateral swelling, tenderness, and fever suggests acute bacterial parotitis (see above), a condition caused by an impacted calculus usually seen in chronically ill patients (Staph. aureus is the usual causative organism). Painless parotid and lacrimal gland enlargement is a finding in alcoholism.
|
|
|
• Pharyngeal exudate
|
although Streptococcus pyogenes (group A, β-hemolytic) is the best known pathogen, fusobacterium, EBV, gonorrhea, and other pathogens are considerations. Most cases occur in children, where the child presents with abrupt fever, sore throat, headache, and difficulty swallowing. Exam findings include the classic triad of objective fever, exudative pharyngitis (exudate is not mandated), and tender anterior cervical adenopathy. Untreated there is a risk of rheumatic fever.
|
|
|
• Pharyngeal pseudomembrane
|
typically caused by Corynebacterium diphtheria infection, this disease can be confused with more common causes of pharyngitis. The throat is red initially, but may later develop a pseudomembrane. This complication can be life threatening as it may obstruct the airway. Other findings include cervical adenopathy (bull’s neck), fever, weakness, heart failure, neuropathy and malodorous breath. Throat culture should identify the pathogen.
|
|
|
• Rhinorrhea (aka “runny nose”)
|
may be part of acute rhinitis occurring in the context of viral infection, or be non-infectious in origin (i.e. allergic rhinitis). CSF rhinorrhea is a rare and serious condition to consider in the setting of prior facial/skull injury or surgery; this reflects a fistula between the nose and subarachnoid space, and as such places the patient at risk for bacterial meningitis.
|
|
|
• Tooth tenderness
|
use a tongue blade to assess for focal tooth tenderness, which is to be expected if dental caries are present. Tooth tenderness is also a useful finding if tooth abscess is suspected, such as in a diabetic with unexplained ketoacidosis. Maxillary teeth may also be tender when maxillary sinusitis is present.
|
|
|
• Tragus sign
|
tenderness with depression of tragus suggests otitis externa (as will pulling on the involved pinna), usually a bacterial infection of the epidermis of the ear canal. These signs are not present with otitis media (differential feature).
|
|
|
• Vertigo
|
the feeling of unsteadiness with motion, most often rotary in nature. The patient may fall down or have great difficulty remaining upright during the symptom. Associated symptoms may include nausea, pallor, and sweating. With true vertigo dysfunction of the vestibular system is present. This includes the inner ear structures, CN VIII, and the brainstem. Thus, the exam should focus on evaluating these systems (e.g. neurologic exam), and drug and alcohol use should be assessed.
|
|
|
Corynebacterium Diphtheria |
person-to-person spread <1wk incubation period + lack of immunization; clinical findings include: - fever, sore throat, weakness and odynophagia - grayish membrane formation is very specific - complications include myocarditis, neuritis and death due to airway obstruction |
|
|
Lead line aka halo Saturnis |

Grey black dots 1mm from free margin of gum consistent with headlines (Not seen if teeth are absent) - can be seen in various heavy metal toxicities including lead, bismuth, mercury, gold, silver, thallium and copper |
|

|
Canchrum oris = facial necrosis in severely malnourished patients (usu in developing world) |
|
|
Kaposi's Sarcoma |
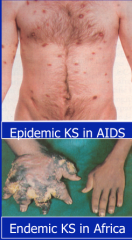
raised reddish lesions are angioproliferative tumors occurring in AIDS patients reflecting infections with HHV 8. Variants: - epidemic (AIDS) - classic (elderly mediterranean men) - endemic (sub Saharan Africa) |
|

|
Oral actinomycosis produces oral facial ulceration with draining fistulas |
|

|
small faint white elevations on red background = Koplik spots in Measles. Best seen opposite lower molars. Appear 1-2 d prior to rash Measles is caused by RNA virus (10-14d incubation) usu occurring before age 5 around developing world. Begins with coryza (running nose) cough and conjunctivitis - progresses to rash and high fever |
|

|
erythroplakia = pre-malignant/malignant orla lesion but reddish in color |
|
|
acute meningitis |
high fever, headache, stiff neck and + Kernig sign (thigh flexed to 90 degrees with pain on leg extension. - subarachnoid hemorrhage does not have high fever, but everything else yes |
|
|
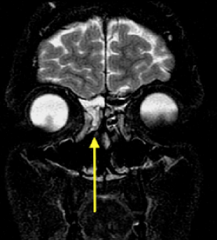
Bony defect leading to CSF rhinorrhea - persistent clear nasal drainage following head/facial trauma and/or craniomaxillofacial surgery |
|
|
pituitary apoplexy |
infarction of pituitary usu in setting of underlying pituitary adenoma. patients become very ill and hypotensive. no meningeal signs |
|

|
erythema and swelling of the submandibular space indicating Ludwig's angina |
|
|
Lemierre's syndrome |
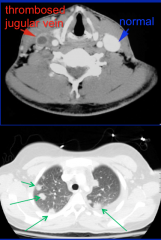
Septic thrombophlebitis of internal jugular vein. Begins as pharyngitis +/- peritonsillar abscess usu due to fusobacterium necrophorum infection. Infected thrombus may embolus to lungs producing nodular lung lesions |