Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
65 Cards in this Set
- Front
- Back
|
Hip joint
|
Synovial ball and socket joint; articulation of head of femur within the actebabulum of pelvis
|
|
|
Hip flexors
|
1. Iliopsoas (iliacus + psoas)
2. Rectus femoris 3. Sartorius Anterior compartment muscles The femoral nerve innervates all of the hip flexors |
|
|
Flexion of hip vs. extension of hip
|
Flexion = thigh moves forward
Extension = thigh moves backward |
|
|
Internal rotation of hip vs external rotation
|
Internal rotation = foot turns inward
External rotation = foot turns outward |
|
|
Iliopsoas
|
2 muscles: iliacus + psoas
A: Hip flexion N: femoral nerve; ventral rami L1-L3 O: L1-L5; iliac crest I: lesser trochanter of femur |
|
|
Iliopsoas
|

|
|
|
Quadriceps muscles
|
1. Vastus lateralis
2. Vastus intermedius 3. Vastus medialis 4. Rectus femoris A: hip flexion (rectus femoris only); knee extension N: femoral nerve (L2-L4) O: RF- AIIS; VL- linea aspera; VI-femur; VM- linea aspera I: Tibial tuberosity |
|
|
Sartorius
|
A: Hip flexion & external rotation; knee flexion
N: femoral nerve (L2-L4) O: ASIS I: medial to the tibial tuberosity |
|
|
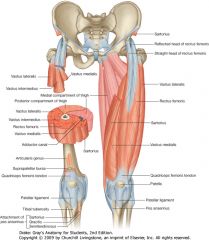
Muscles of the thigh
|
|
|
|
Hip extensors
|
1. Gluteus maximus
2. Hamstring muscles Posterior compartment muscles |
|
|
Gluteus maximus
|
A: Hip extension when hip is flexed; ADD lower fibers; ABD upper fibers
N: inferior gluteal nerve (L5-S2) O: sacrum & ilium I: gluteal line & IT band |
|
|
Hamstring muscles
|
1. Biceps femoris
2. Semitendinous 3. Semimembranosus A: hip extension and knee flexion N: branches of the sciatic nerve (L5, S1, S2): tibial nerve does all three; peroneal nerve does just the short head of the biceps femoris O: ischial tuberosity I: BF - head of the fibula; ST - medial to the tibial tuberosity; SM - medial tibial condyle |
|
|
Hamstrings
|

|
|
|
Hip adductors
|
1. Gracilis
2. Adductor longus 3. Adductor brevis 4. Adductor magnus 5. Pectineus Medial compartment muscles |
|
|
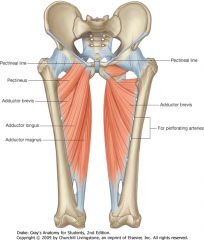
Hip adductors
|
|
|
|
Gracilis
|
A: hip adduction
N: obturator nerve (L2-L4) O: pubis I: medial to the tibial tuberosity |
|
|
Adductor longus
Adductor brevis Adductor magnus |
A: hip adduction
N: obturator nerve (L2-L4) O: AL & AB - pubis; AM - ischium I: linea aspera |
|
|
Pectineus
|
A: hip adduction, flexion & IR
N: femoral nerve; 20% obturator nerve O: pubis I: linea aspera |
|
|
Hip abductors
|
1. Gluteus medius
2. Gluteus minimus |
|
|
Gluteus medius
|
A: hip abduction
N: superior gluteal nerve (L4 - S1) O: ilium I: greater trochanter |
|
|
Gluteus minimus
|
A: hip abduction
N: superior gluteal nerve (L4 - S1) O: ilium I: greater trochanter |
|
|
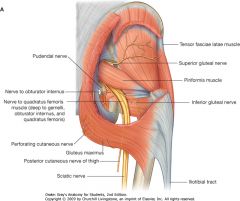
Superior & inferior gluteal nerves
|
|
|
|
Tensor fasciae lata
|
A: abduction, flexion, IR of hip
N: superior gluteal (L4 - S1) O: iliac crest I: IT band (lateral aspect of proximal tibia) |
|
|
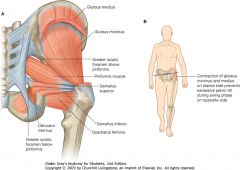
Trendelenburg’s sign or gait
|
Caused by weakness of hip abductors (gluteus medius and minimus)
Normal: when wieght is borne by one limb, the muscles on the supported side fix (contract to isometrically resist adduction) the pelvis so that it does not sag to the unsupported side If the right gluteus minimus and medius muscles are paralyzed, the unsupported left side (sound side) of the pelvis falls (sags) instead of rising to stay level |
|
|
External hip rotators
|
1. Piriformis
2. Superior gamellus 3. Inferior gamellus 4. Obturator internus 5. Quadratus femoris 6. Obturator externus (anterior muscle) A: external hip rotation (stabilizes pelvis during gait by resisting internal rotation) N: ventral rami L1-S2 O: PI- sacrum; SG & IG - ischium; OI - obturator foramen; QF ischium I: greater trochanter |
|
|
External hip rotators
|
|
|
|
Obturator externus
|
A: external rotator of the hip
N: obturator nerve (post. branch) O: obturator foramen I: greater trochanter |
|
|
Anterior compartment of thigh
|
Femoral a.
Femoral n. |
|
|
Medial compartment of thigh
|
Obturator a.
Obturator n. |
|
|
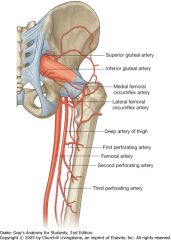
Posterior compartment of thigh
|
Profunda femoris art
Perforationg vessels Sciatic n |
|
|
Muscle compartment of the lower extremity
|
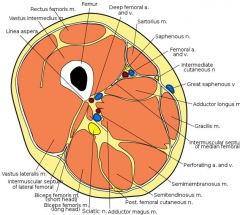
Thigh muscles
|
|
|
Lateral cutaneous femoral nerve
|
L2-L4
Cutaneous anterior and lateral thigh Crosses ASIS and can be compressed there meralgia parasthetica |
|
|
Femoral nerve
|
Sensory to anteromedial thigh via ant/intermed cut. nerves
L2-L4 Motor to psoas, articularis genu, and anterior thigh muscles (quads + sartorius) |
|
|
Obturator nerve
|
L2-L4
Sensory to inferomedial thigh Anterior branch: medial thigh compartment (add longus & brevis, gracilis, and pectineus) Posterior branch: obturator externus, adductor magnus |
|
|
Sciatic nerve
|
L2-S3
Hamstrings by tibial division, short head of biceps by common fibular (peroneal) Bifurcates into tibial nerve and peroneal nerves just above pop fossa |
|
|
Muscles that extend the knee
|
Quadriceps
1. Rectus femoris 2. Vastus lateralis 3. Vastus intermedius 4. Vastus All insert onto the patella Rectus is the only one that crosses the hip too (and thus flexes it) N: femoral A: femoral (LCFA - RF, VL, VI; Profunda - VM) |
|
|
Flexion of the knee
|
Flexion:
Sartorius - ASIS Gracilis - Inferior pubic ramus Semitendinosus - IT Semimembranosus - IT Biceps Femoris- IT (Long Head & Short Head) Popliteus - LFC Gastrocnemius - MFC/LFC Plantaris LFC |
|
|
Tibial nerve (L4 - S3)
|
Tibial nerve innervates the muscles of the posterior thigh (hamstrings) and posterior leg (calf muscles)
EXCEPT: -Short head of biceps femoris (common peroneal n) -Sartorius (femoral n) -Gracilis (obturator n) |
|
|
The one muscle of the medial thigh compartment that crosses the hip and knee joint is?
|
The gracilis
A: adduction & flexion of hip; flexion & internal rotation of knee N: obturator nerve (L2, L3) O: inferior pubic ramus I: tibia (medial tuberosity) |
|
|
The short head of the biceps femoris is innervated by?
|
The common peroneal (fibular) nerve?
The long head is the tibial nerve |
|
|
Pes anserina
|
Insertion of the sartorius, gracilis, semitendinosus onto the antero-medial surface of the tibia
|
|
|
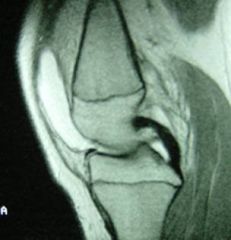
ACL
|
Anterior cruciate ligament
Comes off the posterior portion of the lateral femoral condyle, and crosses in front of the PCL in the intercondylar notch to attach to the middle of the anterior tibia at the intercondyloid eminance Primary restraint to anterior tibial translation, ie it prevents the tibia from moving forward relative to the femur |
|
|
ACL
|

|
|
|
PCL
|
Posterior cruciate ligament
originates at the AL aspect of the medial femoral condyle in the intercondylar notch and attaches to the posterior intercondylar area of the middle of the tibia Primary restraint to posterior tibial translation, ie it prevents the tibia from moving back relative to the femur |
|
|
PCL
|
|
|
|
ALC and PCL
|

|
|
|
MCL
|
Medial collateral ligament
Extends from the femur to the tibial metaphysis Primary restraint to valgus (inward stress) Has superficial and deep fibers; deep fibers attach to the meniscus A mild sprain of the superficial fibers will not cause the joint to swell, but a sprain of the deep fibers will also affect the meniscus and cause joint effusion So if you have a swollen joint, that r/o a superficial sprain |
|
|
LCL
|
Lateral collateral ligament
Femur to fibula Stabilizes the lateral side of the joint to varsus (outside) stress |
|
|
Menisci of knee
|
Medial and lateral
Fibrocartilage discs 98% type I collagen Vascularized peripherally but not in middle (deep injury will not heal) Load bearing |
|
|
Gluteal tears
|
Older patient, +/- trauma
Trendelenberg's sign due to weakness or paralysis of gluteus medius and minimus muscle; inability to abduct the hip and the unsupported (sound) side of the hip falls Tx: Non-Operative - PT NSAIDs Injections (cortisone) Operative Debridement Repair |
|
|
Greater trochanteric pain syndrome
|
Greater trochanteric bursitis
Bursa becomes inflammed due to mechanical irritation; can be associated with other pathology around the hip Localized tenderness over the greater trochanter Tx: injections, PT, bursectomy |
|
|
Gerdy's tubercle
|
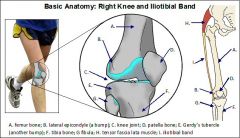
Lateral tubercle of the tibia where the IT band and tensor fascia latae insert
|
|
|
Internal snapping hip
|
Interna Coxa Sultans
Pain in groin associated with popping Popping reproduced when extending the hip from a flexed, externally rotated position Iliopsoas snapping over the pelvic brim or femoral head, or lesser trochanter of the femur Diagnosed with physical exam or dynamic ultrasound tx: NSAIDs and PT, surgical release |
|
|
Meralgia Paresthetica
|
Compression of the lateral cutaneous femoral nerve (L2-L4) that causes pain & sensory deficitis; usually worsened with leg extension
Tender over inguinal ligament by ASIS Tight pants & belts; construction workers; thin, young & healthy; obese or pregnant Diagnosis - physical exam is usually sufficient; EMG; selective nerve injections tx: correct underlying disorder- lose weight, deliver baby, different clothes NSAIDs, neurolysis (release fibers over the nerve), transection (leaves patch withou sensation) |
|
|
Piriformis syndrome
|
Compression of the sciatic nerve by the piriformis (hypertrophy, extension bands, ect.)
Lower back, buttock, posterior thigh pain; worse with sitting, squatting, stairs Pain with flexion, adduction, IR Pace Sign - pain and weakness with resisted ABD when seated Sometimes the sciatic nerve splits before the piriformis, with the tibial branch passing under the piriformis and the peroneal branch passing through Buzz words- cyclist, runners; buttock pain, localized tenderness; reproduced pain with flexion, ADD, IR; studies and further work up negative; diagnosis of exclusion tx: NSAIDs, muscle relaxants; PT: stretching and strengthening, muscle balance, gluteus strengthening; local injections; surgical- Piriformis release |
|
|
Hamstring tear
|
Mechanism - Activities of quick acceleration/deceleration
Waterskiing - Hip flexion/knee extension History Tightness Pop Exam Ecchymosis Tenderness at ischial tuberosity May have palpable defect Radiographs Normal Avulsion in skeletally immature MRI Treatment Non-Operative Return to sports 4-6 weeks Operative Direct repair |
|
|
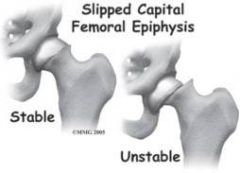
Slipped Capital Femoral Epiphysis
|
Presentation can be (a) unstable - inability to bear weight, acute onset of severe pain, or (worse prognosis)osseous necrosis; or (b) stable - limp, +/- pain
Pain - groin; may be isolated referred pain to the knee (usually to the medial side) Radiographs AP view - Kleins line will help detect slipped epiphysis; frog legs lateral view - abduction of hip joint, can make it easier to see Tx: surgery - in situ pinning (rod); Reorientation Osteotomies - wedge osteotomy, remove wedge, reposition femur, insert screw |
|
|
Slipped Capital Femoral Epiphysis
|
|
|
|
Legg-Calve-Perthes Disease
|
Idiopathic osseous necrosis of the femoral head
LCPD usually occurs in children aged 4-10 years. The disease has an insidious onset and may occur after an injury to the hip. In the vast majority of instances, the disorder is unilateral Males:females = 5:1 Presentation: limp, pain, loss of motion Over the age of 8 years old the prognosis is worse; younger children tend to do well with this 50% do well with conservative treatment Delayed DJD from aspherical joint – if severe --> early arthritic changes Tx: medical is to keep hip contained --> maintaining the femur abducted and internally rotated so that the femoral head is held well inside the rounded portion of the acetabulum or surgery --> femoral/pelvic osteotomies |
|
|
Blood supply to femoral head
|
|
|
|
Hip dysplasia
|
Shallow acetabulum (socket)
Types: Infantile Adult |
|
|
Developmental dysplasia of the hip (infantile type)
|
Displacement of the femoral head from the acetabulum causing disruption of normal hip development
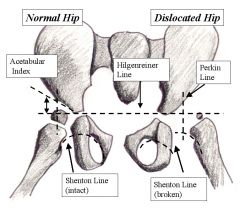
Common findings: Left hip (fetal positioning?) Female sex predominence (5:1) Breech delivery First born Positive family history White or Navajo Indian race Screening exam: Barlow's Ortolani's - click in hip adduction Galeazzi's sign - look at knee height (is one lower than the other?) Leg lengths & skin folds - look for assymetry Hip motion Radiology: Ultrasound if < 3 months because epiphysis not there when born, shows up in 4-6 months Hilgenreiner’s line Perkin’s line Shenton’s line Tx: Containment Pavlik harness – pclced to abduct, flex and externally rotate to bring head into acetabalum Closed reduction and casting Open reduction Pelvic and femoral osteotomies |
|
|
Hilgreiner's line - From an anteroposterior radiograph of the hips, a horizontal line (Hilgenreiner line) is drawn between the triradiate epiphyses.
Perkin line - Next, lines are drawn perpendicular to the Hilgenreiner line through the superolateral edge of the acetabulum (Perkin line), dividing the hip into 4 quadrants. The proximal medial femur should be in the lower medial quadrant, or the ossific nucleus of the femoral head, if present (usually observed in patients aged 4-7 mo), should be in the lower medial quadrant. The acetabular index is the angle between the Hilgenreiner line and a line drawn from the triradiate epiphysis to the lateral edge of the acetabulum. Typically, this angle decreases with age and should measure less than 20° by the time the child is 2 years old. Shenton line - a line drawn from the medial aspect of the femoral neck to the inferior border of the pubic rami (assesses obturator foramen). The line should create a smooth arc that is not disrupted. If disrupted, it indicates some degree of hip subluxation is present. |
|
|
Adult form of hip dysplasia
|
The most common cause of hip arthritis in adults
Shallow acetabulum -> reduced joint contact area -> overload of the anterosuperior joint surface (more pressure on a smaller area) -> cartilage breakdown The first sign of hip dysplasia in an adolescent or young adult is usually hip pain, or occasionally clicking and popping Radiographic findings: 1. Central edge angle 25 -40 degrees - AP radiograph - angle formed by a line drawn from center of femoral head to outer edge of the acetabular roof, and a verticle line drawn thru center of femoral head; - angles greater than 25 deg are considered normal;- less than 20 deg indicates severe dysplasia 2. Shentons line 3. Tonnis angle (Acetabular Index) <10 degrees is normal; increased in hip dysplasia Surgical treatment reserved for symptomatic dysplasia; -Joint preserving acetabular osteotomies Goal: improve quality of life and alter progression of the disease |
|
|
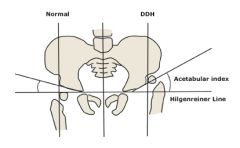
The acetabular index is the angle formed between Hilgenreiner line (a horizontal line through the upper margin of the radiolucent triradiate cartilage) and a tangential line to the lateral ossific margin of the roof of the acetabulum
|