![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
135 Cards in this Set
- Front
- Back
|
What is the purpose of the inflammation response? What is the goal of inflammation? |
DEFINITION - Protective response
It is part of the innate immunity
What is the goal?
|
|
|
What are the components of inflammation? |

|
|
|
Why does the inflammatory reaction need to be balanced? |
The subsequent repair process can cause considerable harm and can cause injury of normal tissue.
Therefore, pro-inflammatory reactions need to be balanced with anti-inflammatory responses. Pathology might become the dominant feature of the inflammatory reaction if:
|
|
|
What are the basic forms of inflammation? Give a brief description of inflammation. |
Acute Inflammation
Chronic inflammation
|
|
|
What are the cardinal sings of acute inflammation? |
|
|
|
Define exudate. Define edema. |
Exudate - extracellular fluid collection rich in proteins and/or cells Edema - an excess of watery fluid collecting in the cavities or tissues of the body |
|
|
What are possible stimulus of inflammation |
Physical - cuts, burns, fracture, foreign bodies Chemical - acids, alkialis, industrial chemicals Microbial - bacterial/fungal toxins and products, viral induced cell death, parasites Immunological - normal immune response to infectious agents, hypersensitivity reactions (I-IV) |
|
|
What are the main changes occurring due to the acute inflammatory reactions? |
Vascular Response
Exudation of Fluid - Inflammatory edema
|
|
|
What are inflammatory mediators? Where are they found? What is their job? What happens when their job is done? Give examples of cellular mediators. |
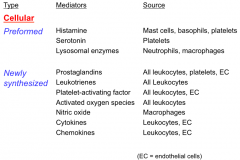
Found
Job
After they are used
|
|
|
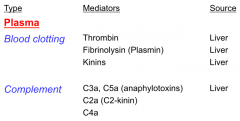
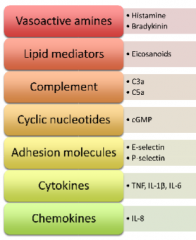
Give examples of plasma mediators? |
|
|
|
What are some important inflammatory cytokines? |
Tumor necrosis factor alpha (TNF-a)
Interleukin-1 (IL-1a and IL-1b)
Interleukin-6 (IL-6)
|
|
|
How does histamine act as an inflammatory mediator? What is it? What are its effects? How is it made? |
|
|
|
How do kinins act as an inflammatory mediator?What is it? What are its effects? How is it made? |
Biologically active polypeptides produced by the action of enzymes called kallikreins on a precursor molecule call kininogen
Effects of bradykinin
Kalikrein enzymes
C2-kinin
Plasmin
|
|
|
How do Prostaglandins (PG) and Leukotrienes (LT) act as an inflammatory mediator?What is it? What are its effects? How is it made? |
Phospholipase A2
Role of PG and LT in Delayed Phase
|
|
|
How do Platelet Activating Factors (PAF) act as an inflammatory mediator?What is it? What are its effects? How is it made? |
Synthesized by activated mast cells from membrane phospholipds Causes platelets to degranulate |
|
|
How does the Complement System act as an inflammatory mediator? What is it? What are its effects? How is it made? |
Activation of the complement system is inter-related with the kinin and coagulation/plasmin systems. Complement fragments C3a and C5a (anaphylotoxins) cause the release of histamine from mast cells, and are important in aggregate anaphylaxis and other immune complex lesions |
|
|
How do mediators released by neutrophils act as an inflammatory mediator? What is it? What are its effects? How is it made? |
Two types of cytoplasmic granules
|
|
|
How do mediators released by platelets act as an inflammatory mediator? What is it? How is it made? |
Two types of granules
Activated
|
|
|
How do peptides act as an inflammatory mediator? What is it? What are its effects? How is it made? |
These result from the digestion of exudate proteins by proteolytic enzymes derived from plasma, tissue cells, and neturophils They are capable of increasing vascular permeability in some cases |
|
|
How do microbial products act as an inflammatory mediator? What is it? What are its effects? How is it made? |
Bacteria may produce a variety of inflammatory products
Some of these have substantial influence on the development of the associated inflammatory reaction |
|
|
How do cytokines act as an inflammatory mediator? What is it? What are its effects? How is it made?
|
These are protein mediators produced by local cells that are induced following tissue insults Action
Examples
|
|
|
How do cheomkines act as an inflammatory mediator? What is it? What are its effects? |
These are also proteins and act as chemo attractants for leukocytes |
|
|
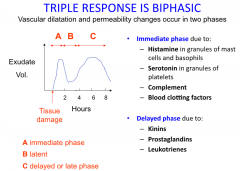
What are the phases of vascular dilation and permeability? How do mediators relate to these phases? |
|
|
|
Describe serous exudate. |

|
|
|
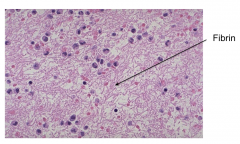
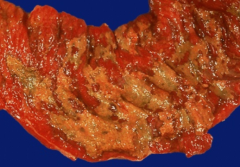
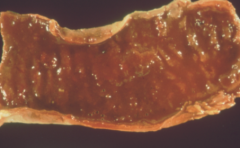
Describe fibrinous exudate. |
|
|
|
Describe catarrhal exudate. |

|
|
|
Describe Suppurative/purulent exudate. |
|
|
|
Describe hemorrhagic exudate. |
|
|
|
Describe necrotising exudate. |
|
|
|
What is the role of the lymphatics and lymph nodes in inflammation? |
In Acute inflammation
In sever reactions
In bacterial inflammation
|
|
|
What is leukocyte migration? |

Active process of two stages.
Both endothelial cells and leukocytes undergo rapid changes in the presence of inflammatory mediators, elaborating a variety of cell adhesion molecules which determine the kinetcs of migration for each type of leukocyte |
|
|
How does the tethering and rolling portion of leukocyte migration work? |

|
|
|
What cells are involved in leukocyte migration and what is their timing? |
|
|
|
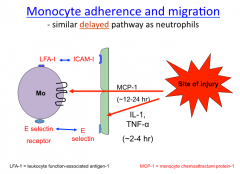
What is neutrophil adhesion? What are the two basic pathways of neutrophil arrest in the circulation near inflammatory sties? |

Immediate Pathway
Delayed Pathways
|
|
|
What is monocyte adhesion? |
|
|
|
What is chemotaxis? How does it work? What is its purpose? Give examples of chemoattractants. |
Examples A variety of chemotactic and migration promoting factors for neutrophils are known
HOW IT WORKS. Neutrophils follow chemoattractant gradient concentrations and hence move in the direction of the source of the chemoattractant
Purpose
Phagocytosis is promoted by opsonins such as antibodies and complement components and suitable scaffolding
|
|
|
What are the pros and cons of neutrophils and macrophages as phagocytic cells? |
Netrophils are short-lived end-stage cells and cannot resynthesize their lysosomal enzymes. Macrophages, however, are long-lived and resynthesize a variety of lysosomal enzymes, some of which are likely to be appropriate to the particular material which has been phagocytozed. |
|
|
Why does phagocytosis not always work for bacterial infections? |
In bacterial infections, it is important to appreciate that phagocytosis is not automatically followed by bacterial disintegration Some organisms cause rapid death of the ingesting cell (via release of toxins) whilst other adapt to the intracellular environment, and such infected cells (esp macrophages) may plan an important role in the dissemination of infection in the body. |
|
|
What is the role of macrophages in acute inflammation and host defense? |
|
|
|
What is the function of exudate? |
|
|
|
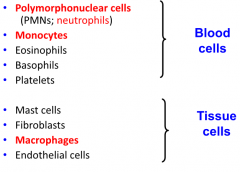
What are the main cell types involved in acute inflammation? What type of cells are they? |
|
|
|
What is a PMN? |
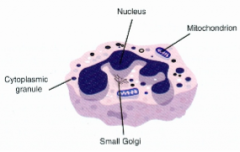
Polymorphonuclear neutrophil granulocyte
|
|
|
Summarize what happens during inflammation. |
|
|
|
Summarize the types of inflammatory mediators. |
|
|
|
What are eicosanoids? |
Lipid mediators
|
|
|
What are essential fatty acids (EFAs)? |
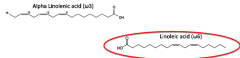
Omega 3 = antiinflammatroy Omega 6 = proinflammatory |
|
|
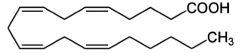
What is arachidonic acid (AA)? |
|
|
|
How are prostaglandins synthesized? |

Cyclooxygenase (COX)
|
|
|
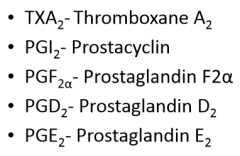
Give examples of prostaglandins. |
|
|
|
What is the mechanism of action for prostaglandin? Which prostaglandin is produced when? |

Order of diagram: Cell Type, Produce Produced; Effect; Result
Which prostaglandin?
|
|
|
What are leukotrienes? |
Eicosanoids Certain cells associated with production
|
|
|
How are leukotrienes synthesized? |

|
|
|
What are the mechanisms of action and effects of leukotrienes? |
|
|
|
Which drugs modify the PGs and LTs? |
Prostaglandin production
These drugs are widely used in Vet Med
5-Lipoxygenase inhibitors and receptor antagonist
|
|
|
What is histamine? |
|
|
|
How is histamine produced? |
|
|
|
How is histamine stored? |
|
|
|
What are the effects after histamine is released? |
There are species differences
|
|
|
How is histamine released from its storage granules? |
Causes anaphylaxis and allergy |
|
|
How do drugs and other chemicals effect histamine? |
Certain drugs may cause direct degranulation and release of histamine from mast cells
Endogenous mediators such as bradykinin, kallidin, and substance P |
|
|
How does histamine respond to physical injury? |
|
|
|
What are the receptor subtypes and system effects of histamine? |
Designation/delineation of the specific effects of histamine to a specific receptor subtype is difficult Cardiovascular System
Respiratory
Intestinal smooth muscle
Uterine smooth muscle
Exocrine glands
Other system effects
|
|
|
How do H1 and H2 receptors work? What type of receptors are they? |
H1
H2
|
|
|
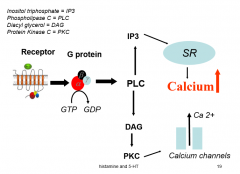
What does a GPCR look like? |

|
|
|
How does a GPCR effect calcium levels? |
|
|
|
What is the effect of histamine on chronic inflammation? |
Histamine can affect the function of macropahges, T lymphocytes, B lymphocytes, cytokine production, expression of MHC class II antigens on cell surface |
|
|
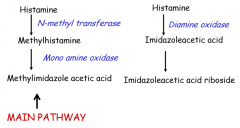
How is histamine metabolized? |
|
|
|
What are anti-histamines? How are they received in the animal? |
Most of the classic anti-histamines are H1 receptor antagonists
Pharmacokinetics and Pharmacodynamics
|
|
|
What is the purpose of anti-histamines? |
Counteract the effects of
Have no effect on H2 receptor mediated effects
|
|
|
What are some specific anti-histamines? What are they used for? |
Uses
|
|
|
What is Serotonin? |
Serotonin = 5-hydroxytryptamine (5-HT) 5-HT derived from dietary tryptophan
Concentrated in enterochromaffin cells in the GI tract, in platelets, and in the CNS |
|
|
How is serotonin synthesized and metabolized? |
Synthesis
Metabolism
|
|
|
What are the receptors for serotonin? |
Four subgroups of receptor with additional subtypes within each family
|
|
|
What are the effects of serotonin? |
Platelets
GI tract
CNS
Role in Inflammation
|
|
|
How are agonists and antagoinsts of serotonin used in the clinical setting? |
|
|
|
What is leukocytosis? |
An increase in the concentration of leukocytes in blood.
This usually occurs with specific types of leukocyte depending on the cause of the inflammation
|
|
|
What is the process the results in neutrophil leucocytosis? What happens if this process is prolonged? |
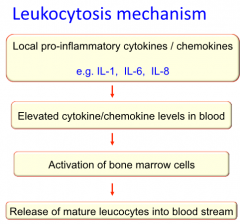
If this process is prolonged, immature neutrophils are released into the blood resulting in a "shift to the left"
Similar mobilization of monocytes occurs resulting in monocytosis. In parasite infections, the main leukocytes involved in protection is the eosinophil.
|
|
|
What are the systemic effects of acute inflammation? |
|
|
|
What is pyrexia? What are its benefits? How is it induced? |

Fever!
Benefits
Induction - two main ways
|
|
|
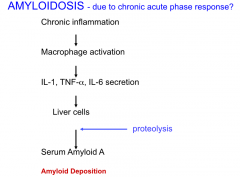
What is acute phase response? How does it differ between acute and chronic inflammation? What is its mechanism of action? |
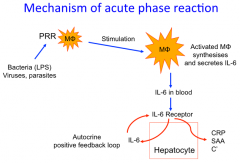
Systemic manifestation that occurs in most forms of inflammation, infection, and tissue injury
Acute inflammation
Chronic Inflammation
Mechanism of Action
|
|
|
What is anemia? What is its mechanism of action? What happens during acute inflammation? |
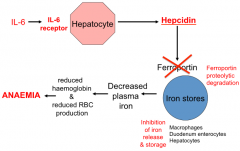
Transient reduction in erythrocytes in blood. Mechanism
Ferroportin is required to transport iron from
Without ferroportin: no iron is released into plasma and red blood cell production is shut off. In acute inflammation, resolution of the inflammation results in hepcidin production being switched off, allowing ferroportin expression and normal iron release into plasma resumes. |
|
|
What is septic shock? What are some characteristic features of septic shock? What are its mechanisms of action? What induces septic shock? How can it be controlled? |
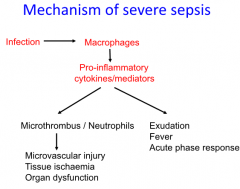
Infection-induced syndrome characterized by a generalized inflammatory state
Characteristic features
Mechanisms
Induction
Control Pro-inflammatory reactions in the developing sepsis can be controlled by endogenously released glucocorticoid and other hormones as part of a stress response. |
|
|
What is disseminated intravascular coagulation? |
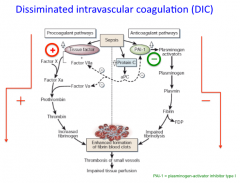
DIC Sepsis disturbs the normal homeostatic balance between the pro coagulant pathway and the anticoagulant pathways leading to widespread thrombosis and impaired tissue perfusion This results in tissue damage, resulting in multiple organ dysfunction and multiple organ failure often with fatal consequences. |
|
|
What is hypotensive shock? How is it induced? |
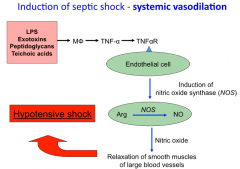
Lack of blood to brain The action of TNF-a on endothelial cells causes the production of nitric oxide which induces vascular smooth muscle to relax |
|
|
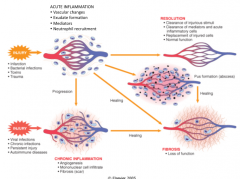
What are the sequelae of acute inflammation? What determines the sequelae which follow an acute inflammatory reaction? |
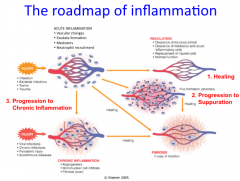
What follows
|
|
|
What are the two outcomes of healing sequelae? |
Resolution - return to normal architecture and removal of dead cellular debris
Repair - formation of scar tissue if inflammatory reaction is extensive
|
|
|
How does the Resolution program work and lead to the healing process? |

|
|
|
What is the demolition phase? How does it work? |
Part of healing sequelae - resolution process
Fibrinolysis may also assist in the removal of larger masses of fibrin and the excess cells and exudate pass out of the area along the lymphatics |
|
|
What are the anti-inflammatory mediators involved in the resolution phase? |
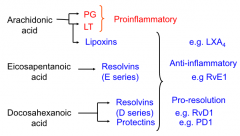
Lipoxins
Resolvines and Protectins
Other factors
|
|
|
How is the site regenerated during the healing sequelae -resolution phase? |
Lost tissue is replaced by proliferation of cells of the same type Mediated by wound cytokines secreted by Mphi
Wound cytokines act as growth factors for:
Original architecture is reconstructed |
|
|
What is granulation tissue? |
|
|
|
How is the site repaired during the healing sequelae - repair phase? |
|
|
|
What is fibrosis? |
Sign of connective tissue replacement of function tissue Occurs with serious protein exudates, lots of fibrin exudation from plasma, and areas where the exudate cannot be adequate absorbed. |
|
|
What is suppuration? |
Pus formation
Characterized by an intense and prolonged neutrophil emigration resulting in the accumulation of large numbers of these cells in the tissues at the site of damage.
|
|
|
How is an abscess formed? |
Liquefaction (caused by dead neutrophils) results in the formation of a potential space (the abscess cavity) at the center of the lesion which is filled with highly cellular fluid exudate (pus) composing mainly of dead and dying neutrophils with necrotic tissue cells ,debris, fibrin, erythocytes, and bacteria.
|
|
|
What is a sinus track? |
Where the site of surface discharge is at some distance from the original abscess cavity, the tube-like connecting track is called a "sinus track" |
|
|
How does the direction of abscess pointing impact healing? |
Gravitational pointing
Anti-gravitational
Externally- end infection Internally - spread infection |
|
|
What is granulation tissue? Describe the encapsulation process. |
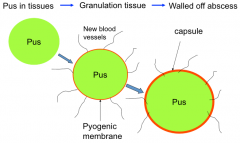
If the growth of bacteria is checked during the development of the abscess, (either by natural defenses or with the help of antibiotic drugs) the abscess will stop enlarging and the accumulated pus will become enclosed by a layer of new cellular and vascular tissue - granulation tissue Encapsulation Process
|
|
|
How do abscess heal? |
Initiated by granulation tissue - angiogenesis, fibroblast proliferation, leukocyte filtration (Mphi)
By resolution if abscess is small By repair if abscess is large (avascular scar tissue) |
|
|
How does an injury progress to chronic inflammation? How does the nature of the causal agent impact response? |
When tissue injury is due to:
The features of the reaction become altered
Some chemical agents give rise to prolonged low-grade irritation
Other agents- particularly some bacteria and fungi (which persist as large aggregated colonies)- give rise to lesions in which acute suppurative inflammation occurs inn the immediate vicinity of the colonizing pathogens |
|
|
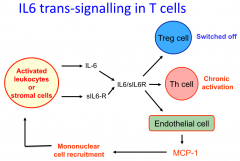
What is the mechanism that allows acute inflammation to develop into chronic inflammation? |

Thought to involve chronic production of IL-6 in the acute phase response.
|
|
|
What is chronic inflammation? |
Definition: immune reactions of prolonged duration (weeks to months to years) in which active inflammation, tissue injury, and healing proceed simultaneously. Associated with:
Some infections may initiate chronic inflammatory reactions without a prior acute inflammatory reaction. |
|
|
What are the dominant leukocytes in chronic inflammation? |
Tend to be lymphocytes and macrophage, though neutrophils persist in some forms as for example in chronic abscesses. |
|
|
How do mononuclear cells migrate into tissues? |
|
|
|
What are the cellular events of chronic inflammation? |
Mphi and DC present antigen to T cells
Plasma cells secrete antibodies locally
Cytotoxic T cells and NK cells kill infected cells IGN-y secreted by T cells and NK cells is pro-inflammatory
|
|
|
What are the characteristic features of most types of chronic inflammation? |
Dense cellular infiltration and proliferation of lymphocytes and macrophages rather than exudation
The tissue becomes thickened
|
|
|
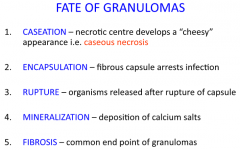
What are granulomas? |
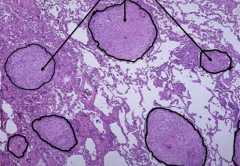
Granulation tissue may occur and in some cases granulomas may develop. Granulomas consist of aggregation of T cells and macrophages.
|
|
|
What are giant cells? |
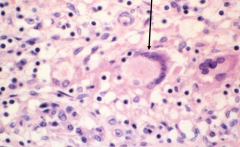
Giant cells may contain up to 200 nuclei due to fusion of macropahges. Their function is unknown, though they are thought to be more efficient than macrophages at clearing infection. |
|
|
What happens during a foreign body response? What are the monocellular functional pathway in response to a foreign body? |
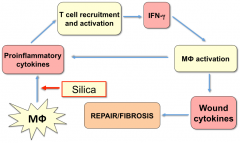
The reaction is mediated mainly by macrophage, since the irritant material is not antigenic (for example silica or asbestos)
The persistent nature of such irritant materials results in persistent activation of macrophages and lymphocytes, and leads to widespread scarring |
|
|
How is tissue damage mediated in chronic infections? |
The tissue damage is often mediated by macrophage and T cell cytotoxic reactions, but can involve humoral immune responses. However, in some infection and some types of autoimmune disease, tissue damage is mediated by long-term production of auto-antibodies (Type II hypersensitivity) or antigen/antibody complexes (Type III hypersensitivity) via complement activation and involvement of neutorphils predominantly. |
|
|
What are the systemic manifestations of chronic inflammation? |
Leukocytosis
Pyrexia
Acute Phase Response
Cachexia
Anemia
Amyloidosis
|
|
|
What are hypersensitivity diseases? |
Inflammation and injury mediated by the immune system Inappropriate reaction to antigens by the immune system - cause tissue injury and disease
|
|
|
What are some general characteristics of hypersensitivity reactions? |
Sensitation Phase
|
|
|
What are the four types of hypersensitivity reactions? What are they mediated by? |
Type I - mediated by IgE antibodies Type II - mediated by IgG or IgM antibodies Type III - mediated by Ag/Ab complexes (IgG or IgM Ab) Type IV - mediated by antigen-specific T cells and macrophages (Th1 cells, Th2 cells, cytotoxic CD8+ T cells) |
|
|
What is Type I Hypersensitivity? What are the different types of Type I? What are general causes of Type I? |
Types of Type I
Typical allergens:
|
|
|
How do genetic mechanisms regulate Type I responses? |
They regulate:
|
|
|
Give examples of Type I atopic allergies. |
|
|
|
What is general or systemic anaphylaxis? What organs are commonly effected? |
A condition that occurs relatively rarely, but is often fatal
Shock organs
|
|
|
What is local anaphylaxis? What are common causes of local anaphylaxis? |
Operates via the binding of the allergen to IgE antibodies on the surface of mast cells or basophils resulting in degranulation Mechanism
Common causes
|
|
|
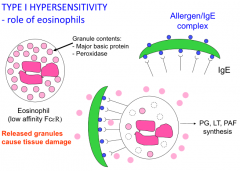
What is the mechanism for Type I hypersensitivity? |

|
|
|
What is the role of eosinophils in Type I hypersensitivity? |
|
|
|
What is the difference between immediate and late phase responses to allergic reactions? |
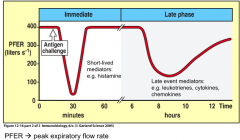
Immediate
Late
|
|
|
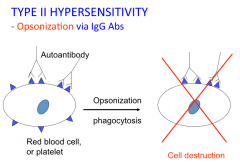
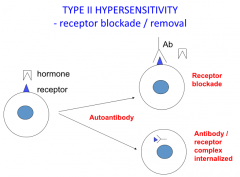
What is Type II Hypersensitivity? What are the 4 main modes of cell destruction? |
Cytotoxic
4 main modes of cell destruction
|
|
|
What is the mechanism for Type II Hypersensitivity via opsonization by IgG Abs? |
|
|
|
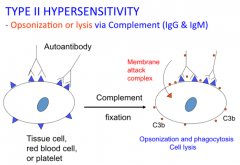
What is the mechanism for Type II Hypersensitivity via opsonization or lysis by complement (IgG and IgM)? |
|
|
|
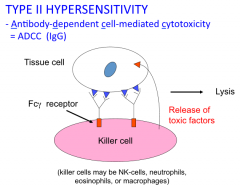
What is the mechanism for Type II Hypersensitivity via ADCC (IgG)? |
|
|
|
What is the mechanism for Type II Hypersensitivity via receptor blockade/removal? |
|
|
|
What is Type III Hypersensitivity? |
Immune Complex Disease Basis is combination of soluble antigen with circulating IgG or IgM antibodies to form "immune complexes"
This type of reaction occurs with certain types of chronic infection and in some autoimmune diseases. |
|
|
What is the pathogenesis of Type III Hypersensitivity? |
|
|
|
What are the different types of Type III Hypersensitivity? |
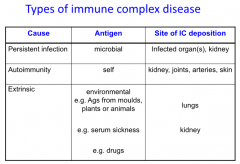
Examples of extrinsic IC disease:
|
|
|
What determines where the immune complex ( of Type III Hypersensitivity) will be deposited? |
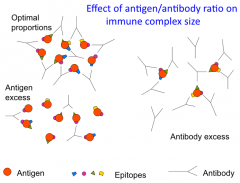
Hemodynamic Process
Antigen/antibody ratio
|
|
|
What is the mechanism that causes an Arthus reaction? |
|
|
|
What is Type IV Hypersensitivity? What are the different types of Type IV? What causes Type IV? |
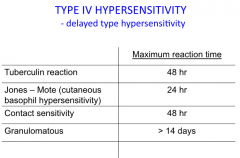
Cell Mediated Delayed Type Hypersensitivity or DTF
Types of DTH reactions
Causes:
|
|
|
What is the mechanism for Type IV Hypersensitivity? |
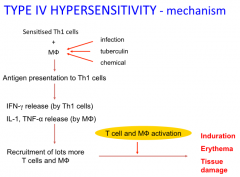
Illustrated by the tuberculin reaction
|
|
|
What happens in chronic Type IV Hypersensitivity reactions? |
Due to persistent infection
|