![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
224 Cards in this Set
- Front
- Back
|
What does pulsatile tinnitus suggest? |
A vascular tumour or malformation |
|
|
What might be the cause of popping or cracking noise in the ears? |
Eustachian tube dysfunction |
|
|
What causes conductive hearing loss? |
Blockage of the middle/outer ear e.g. XS wax Abnormality in the structure of the outer eat/ear canal/middle ear Ruptured ear drum |
|
|
What causes sensorineural hearing loss? |
Presbycusis Ototoxic drugs Infectious diseases Birth complications Trauma Auditory neuromas Genetic predisposition Menieres Disease |
|
|
Name 4 methods of diagnosing conductive hearing loss in children |
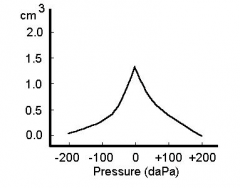
Audiometry - subjective test to determine patient's threshold Audiometry brainstem response (ABR) - objective test, can identify central hearing loss. No response from pt is necessary Otoacoustic emmisions - screening of neonates and children Typanometry - Stiffness/compliance of eardrum |
|
|
Type A: normal peak with normal compliance |
|
|
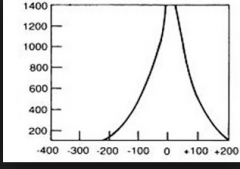
Type Ad: hyperflaccid ear drum or disruption of ossicles |
|
|
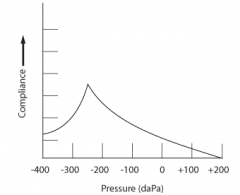
Type C: Indicates negative middle ear pressure e.g. with developing or resolving otitis media |
|
|
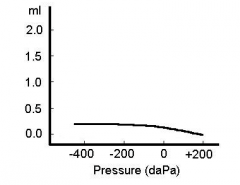
Type B (low compliance): Indicates fluid in the middle ear making the drum stiff |
|
|
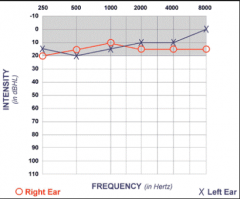
Normal hearing audiogram |
|
|
Right ear congestion --> conductive hearing loss. Difference in bone and air conduction |
|

|
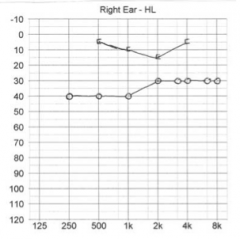
Left sided Menieres. Low frequency sensorineural loss. |
|
|
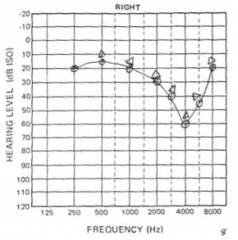
Noise induced hearing loss in right ear. Note the dip at 4kHz |
|

|
Otosclerosis - Carhaarts notch at 2kHz on masked bone conduction. |
|

|
Presbyacusis - bilateral, symmetrical, high frequency sensori-neural hearing loss |
|

|
Cookie bite hearing loss - usually congenital so check siblings |
|
|
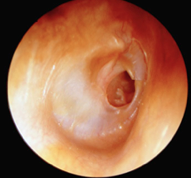
Tympanosclerosis - calcification of tissue in tyrannic membrane and middle ear e.g. after infection or trauma. |
|
|
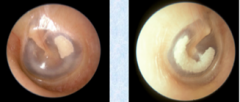
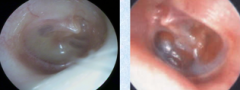
Glue ear - otitis media with effusion. May have fluid level and prominence of blood vessels |
|
|
Cholesteatoma - sac/cyst of epidermal and connective tissue in the middle ear. Usually in attic/epitypanic part of middle ear. |
|

|
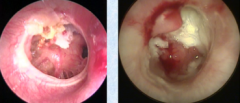
Granulation - red, raised lesion on posterior aspect of drum. May indicate underlying pathology |
|

|
Polyp |
|
|
How can you differentiate between otitis externa and a middle ear infection? |
Otitis externa produces watery discharge as there are no mucinous glands. |
|
|
What is a positive Rinne's test? |
Normal hearing, when air conduction is louder than bone conduction. |
|
|
When might someone have false negative cross hearing? |
With severe sensorineural deafness in 1 ear the bone conduction may travel through the skull and be "heard" in the opposite ear indicating a negative Rinne's |
|
|
What is meant when the sound from Weber's test lateralises to the worse ear? |
A conductive loss in that ear. |
|
|
What is meant when it lateralises to the better ear? |
A sensorineural hearing loss in the hard of hearing ear. |
|
|
Describe the presentation of cholesteatoma |
Peak age 5-15 years. Foul discharge +/- deafness, headache, pain, facial paralysis and vertigo which indicate impending CNS complications |
|
|
List some complications of cholesteatoma - think about why they happen! |
Facial paralysis Meningitis/Intracranial abcess Conductive deafness (ossicle erosion) Vertigo (erosion through labyrinth/semi circular canal) Sensorineural deafness Sinus thrombosis (erosion in to the sigmoid sinus) |
|
|
What causes otosclerosis? |
Spongy bone formation around the oval window --> conductive deafness May progress to replies labyrinth --> sensorineural deafness It is an inherited autosomal dominant disorder. |
|

|
Schwartze's sign = reddish blue discolouration over promontory and oval window niche due to vascular hyperaemia of abnormal immature bone. |
|
|
How might you manage a patient with otosclerosis? |
Watchful waiting Stapedectomy Hearing aid |
|
|
What kind of deafness is associated with noise exposure? |
Usually sensorineural deafness but may be conductive if tympanic membrane ruptures. Also causes tinnitus |
|
|
Patient has difficulty hearing speech in the presence of background noise but normal hearing test results. Diagnosis? |
Obscure auditory dysfunction (King Kopetzky syndrome) |
|
|
What is obscure auditory dysfunction? |
A type of auditory processing disorder affecting the way the brain processes auditory information. |
|
|
Management of obscure auditory dysfunction? |
Audiometry, neurologic electrophysiological tets, behavioural tests, dichotic speech tests Environmental modifications Auditory training |
|
|
Name 3 causes of objective tinnitus |
Palatal myoclonus Vascular bruits Insect in middle ear |
|
|
A patient has unilateral tinnitus. How would you Investigate? |
MRI to rule out acoustic neuroma. Audiogram to rule out deafness. |
|
|
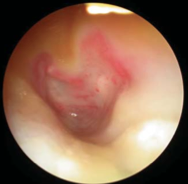
Perforation |
|
|
What is the classic triad of Meniere's disease? |
Recurrent vertigo attacks Tinnitus Fluctuating and progressive sensorineural deafness (gets worse with every attack |
|
|
If you suspect Meniere's how might you investigate? |
MRI - rule out acoustic neuroma VDRL - rule our otosyphillis |
|
|
How might you treat Meniere's medically? |
Vestibular sedatives - diazepam Antiemetics - Prochlorpromazine Phenothiazines Betahistine - vasodilatation and fluid resorption in middle ear Chlortalidine - diuretic |
|
|
How might you manage medically resistant Meniere's? |
Chemical neurectomy - intratympanic gentamicin Endolymphatic sac decompression Vestibular nerve section - spares hearing Labyrinthectomy - total ipsilateral deafness |
|
|
What neurological problems may be caused by an acoustic neuroma (schwannoma of the auditory nerve) |
Brainstem compression CN V, IX, X, XI compression IVth ventricle compression --> raised ICP |
|
|
What are the 3 types of otitis externa? |
Diffuse Furuncle Malignant |
|
|
Patient presents with severe pain of pinner with wet desquamation of keratin and black granules. Diagnosis? |
Fungal otitis externa |
|
|
What is the chief organism that causes otitis extern? |
Pseudomonas |
|

|
Diffuse otitis externa |
|

|
Furuncle |
|
|
Bullous myringitis – This is another cause of severe pain. Viral (probably influenzal) infection causes haemorrhagic blistering of the eardrum |
|
|
What types of patients tend to get necrotising otitis externs? |
Elderly, diabetics and immunocompromised
|
|
|
What is the causative organism in necrotising otitis externs? |
Pseudomonas auriginosa |
|
|
How can you treat diffuse otitis externa? |
Aural toilet If severe and the meatus is narrowed can insert pope wick Can use topical drops but only in short term as fungal infections can arise In cases involving the whole pinna - systemic antibiotics |
|
|
Treatment of a furuncle? |
Staphylococcal abcess Analgesia Astringents (alluminium acetate, glycerin and ichthammol) Systemic antibiotics if sever with lymphadenopathy |
|
|
Treatment of necrotising otitis externa? |
High dose I.V. ABx, surgical debridement, IgGs, hyperbaric oxygen therapy |
|

|
Haematoma - blood tracks between the perichondrium and the cartilage |
|
|
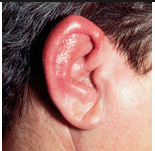
When does cauliflower ear arise? |
Following a haematoma. The clot can get infected --> necrosis of the cartilage and gross deformity |
|
|
Treatment of a haematoma? |
Aspiration or incision and drainage Apply pressure and give antibiotic cover |
|
|
What is the perichondrium? |
Connective tissue surrounding the cartilage |
|
|
Perichondritis Treat with antibiotics |
|

|
Chondrodermatitis nodularis helicus - Painful inflamed nodule of ear usually on the apex of the helix or antihelix. |
|
|
A 50 year old builder presents with a tender lump on the apex of his helix which has scaling. Diagnosis? Management? |
Chondrodermatitis nodularis helicus. Avoid cold, pressure and trauma (CNH ear protection). Can freeze with liquid nitrogen, use topical GTN/cortisone/collagen. Surgical excision biopsy |
|
|
Rhinosinusitis lasting >12 weeks is considered to be what? |
Chronic rhinosinusitis |
|
|
Rinosinusitis lasting <4 weeks is considered to be what? |
Acute (4-12 = subacute) |
|
|
Where do the maxillary, frontal and anterior ethmoid sinuses drain? |
The middle meatus between the inferior and middle turbinate |
|
|
Where do the posterior ethmoid sinuses drain? |
Superior meatus |
|
|
Where does the sphenoid sinus drain to? |
Sphenoethmoidal recess in the posterior nasal cavity |
|
|
What causes the majority of acute rhino sinusitis cases? |
They usually follow a viral URTI --> hyperaemia and oedema of the mucosa --> blocked sinus drainage and a secondary bacterial infection |
|
|
What are the commonest organisms of bacterial rhino sinusitis? |
Streptococcus pneumoniae Haemophillus influenzae |
|
|
A lady comes in with a 2 week history of severe, unilateral pain on her face and pain when she chews, pyrexia, nasal obstruction and poor smell. Diagnosis? |
Acute rhino sinusitis of the maxillary sinuses |
|
|
How might you treat an episode of acute rhino sinusitis? |
Simple analgesia Steam inhalations Decongestant - for no longer than 5 days in topical as will cause rebound congestion Antibiotics rarely prescribed but in severe, persistent cases may use penicillin or amoxicillin. Be aware in penicillin resistant areas to use alternative |
|
|
What signs and symptoms of ARS indicate the need for sinus drainage |
Progressive pain and resistance to medical treatment |
|
|
What are the complications of ARS? |
Periorbital cellulitis Severe headaches Focal neurological signs Meningial symptoms |
|
|
What microbial pathogens are responsible for chronic rhino sinusitis? |
Predominantly gram -ve and anaerobic bacteria Staph aureus Coag-negative staph Anaerobic usually produce foul smelling discharge and are from dental disease |
|
|
4 key points in the history of sinogenic pain? |
1. Exacerbation of pain during an URTI 2. Association with rhinological symptoms 3. Worse on flying 4. Response to medical treatment |
|
|
Alternative diagnosis to facial pain in the absence of rhinological symptoms? |
Mid-facial pain Migraine Cluster headaches Atypical facial pain
NB vascular causes of headaches may --> clear discharge due to vasodilatation |
|
|
How can you differentiate between the inferior turbinate and a nasal polyp? |
Inferior turbinate is red and sensitive Polyp = pale, pendulous, opalescent and painless |
|
|
Patient presents with nasal obstruction, hyposmia, nasal irritation and sneezing. They have yellowish nasal mucus. Diagnosis? |
Allergic rhinitis - mucus is yellow due to staining by eosinophils |
|
|
How might you treat chronic rhinosinusitis? |
Broad spectrum antibiotics e.g. coamoxiclav, clindamycin for at least 3 weeks Topical nasal steroids e.g. betamethasone - 2 months followed by a nasal steroid spray Instructions on how to nasal douche |
|
|
When would you refer for surgical treatment? |
If there is no improvement from medical therapy after 8 weeks. |
|
|
Explain nasal douching |
1/2 teaspoon of salt 1/2 teaspoon of sugar 1/2 teaspoon of bicarb of soda 2 pints of boiled water left to cool Sniff mixture up one nostril with syringe and let it run out. Use topical sprays and drops after douching. |
|
|
A patient with a 6 week history of rhinosinusitis is complaining of not being able to see red as they used to and some blurring of their vision. What does this suggest? |
Orbital abcess |
|
|
Patient has a history of rhinosinusitis but presents with a swollen eye, fever, a severe headache and some double vision. Diagnosis? |
Cavernous sinus thrombosis - due to spreading of thrombophlebitis from RS. High dose antibiotics required |
|
|
What type of abcesses may occur as a consequence of frontal sinusitis? |
Brain abcess Extradural Abcess - dehiscence of posterior wall of frontal sinus Subdural abcess - meningism signs |
|
|
Name the branches of the facial nerve |
Temporal Zygomatic Buccal Marginal mandibular Cervical |
|
|
Important innervations of the facial nerve |
Greater petrosal: Taste from palate, parasympathetic fibbers to the lacrimal gland Branch from ganglion: Secretomotor fibbers to parotid Branch to stapedius: Restricts excessive movement of tympanic membrane Chorda tympani: Taste fibers from tongue Postauricular nerve: Muscles of ear and occipitofrontalis belly Muscles of facial expression Cutaneous branches: both sides of pinna, EAM and tympanic membrane. Run with CN VIII - pharyngeal pathology can therefore --> otalgia and palatal vesicles can --> herpes oticus |
|
|
Man presents with weakness of his mm of facial expression but is able to lift his eyebrows. Diagnosis? |
Stoke causing UMN lesion of facial nerve |
|
|
A man presents with some facial palsy and on examination: Has normal V-->VIII and lower cranial nerve function No signs of infection or trauma to his ear Oropharynx - displaced tonsil medially but no signs of infection. Diagnosis? |
Deep parotid tumour |
|
|
Management of VII nerve palsy? |
Eye care - reduced eye closure - artificial teats, lacrilube ointment, eyelid sutures or gold weight General - treat underlying cause e.g. infection and treat asymmetry with e.g. facial slings |
|
|
Man presents with foul smelling discharge from ear, facial palsy, vertigo and headaches. Diagnosis? |
Cholesteatoma |
|
|
What causes Bell's Palsy? |
Idiopathic = diagnosis of exclusion - no CNS or ear pathology. |
|
|
How might you manage a patient with Bell's Palsy? |
Oral steroids might help speed up recovery Eye protection |
|
|
Patient presents with facial palsy, pain and painful vesicles in ear canal and pinna. What might be the cause and who would you manage it? |
HZV infection. Treat with high dose anti-vitals + steroids. |
|
|
Symptoms of Bell's Palsy |
Ipsilateral numbness around ear, reduced taste, hypersensitivity to sounds, unilateral sagging of mouth, drooling, difficulty eating, speech difficulty, failure to close eyes. Forehead spared. |
|
|
How might a transverse temporal fracture differ to a longitudinal one? |
Transverse - usually involve labyrinth --> sensorineural hearing loss and vertigo. 50% --> facial nerve palsy. Longitudinal fractures - spare the labyrinth but fractures often involve EAM and roof of middle ear --> conductive hearing loss through ossicle dislocation, bleeding or tympanic membrane rupture. |
|
|
What structure will you identify at the level of the upper 2nd molar? |
Parotid duct |
|
|
How can you examine the submandibular glands? |
Bimanual palpation |
|
|
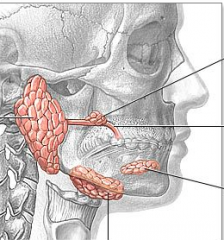
Left to Right Parotid gland Submandibular gland Sublingual gland |
|
|
Which cells are thought to transform in to salivary neoplasms? |
Reserve cells - found in the intercalated and excretory duct systems |
|
|
Common causes of xerostomia? |
Depression Anxiety Drugs - antimuscarinic activity Atropine, hyoscine, ipratropium TCAs MOIs Phenothiazides Anti-parkinson drugs Cold cures e.g. decongestants Bronchodilators Appetite suppressants Sjogren's syndrome Radiotherapy of the head and neck |
|
|
What is Ludwig's angina? |
A cellulitic facial infection usually caused by untreated dental infection |
|
|
What bacteria cause parotitis? |
Staphylococcal infection - generally seen in debilitated, dehydrated patients with poor dental hygiene |
|
|
How would you manage bacterial parotitis? |
Sialogogues e.g. lemon juice to increase salivary flow +/- drainage + high dose ABx |
|
|
What is sialectasis? |
Dilatation, stenosis and necrosis of acini --> cysts. Often cause is sialolithiasis (calculus formation) |
|
|
What is the incidence of benign tumours? Where are they most commonly found and in which sex and age group? |
1 per 100,000 80% of salivary tumours are found in the parotid and 80% of these are benign Benign usually seen in adult females. |
|
|
What is the most common salivary gland tumour? |
Pleomorphic adenoma - more often in superficial lobe of parotid |
|
|
How would you manage a patient with a suspected pleomorphic adenoma? |
FNAC Ultrasound or CT Superficial parotidectomy if in parotid |
|
|
What is the name of the tumour present in men (8:1) over the age of 40? |
Warthin's Tumour aka adenolymphoma - soft, cystic masses in the tail of the parotid. NOT a lymphoma |
|
|
What are the symptoms that indicate a parotid malignancy? |
Facial palsy Pain Lymph node mets |
|
|
Where are malignant tumours most common? |
Sublingual and minor salivary glands therefore swellings in these areas require a high index of suspicion. |
|
|
What sex and age group are mucoepidermoid carcinomas most prevalent? |
5th decade in women (2-4:1) Is the commonest salivary gland carcinoma in children |
|
|
What kind of cell differentiation would be seen in a high grand mucoepidermoid carcinoma? |
Poorly differentiated |
|
|
Where is a mucoepidermoid carcinoma most likely to spread to? |
Local lymph nodes, lungs, bones and brain. |
|
|
What percentage of parotid tumours are acinic cell carcinomas? |
2-4% |
|
|
How do acinic carcinomas behave? |
As low grade tumours, can occur bilaterally. |
|
|
What is the commonest salivary malignant tumour? |
Adenoid cystic carcinoma
|
|
|
Where are adenoid cystic carcinomas most likely to occur? |
Sublingual glands |
|
|
Describe the growth of adenoid cystic carcinomas |
Grow slowly and insidiously with nerve infiltration and skip lesions. Perineural infiltration is common causing palsies and pain |
|
|
What is the 15 year survival rate of patients with adenoid cystic carcinomas? |
10-26% |
|
|
What malignant cancer can develop within a pleomorphic adenoma? |
Carcinoma ex-pleomorphoic adenoma |
|
|
What cancer of the salivary glands has a very poor prognosis of 10% at 5 years? |
Adenocarcinoma - accounts for 2.5-4% of all parotid neoplasms |
|
|
What is the commonest type of lymphoma found in the salivary glands? |
Non-hodgkin's lymphoma - present with firm, rapidly enlarging mass in 5-7th decade |
|
|
Where to salivary tumours commonly metastise to? |
Lung, breast, kidney, upper GI tract and locally in skin as melanoma and SCC |
|
|
How would you investigate a salivary swelling? |
Examination: Entire neck and oral cavity plus cranial nerves esp CNVII Routine blood tests Virology Angiotensin converting enzyme (ACE) SSA and SSB - Sjorgrens X-ray, sialogram, CT-sialogram, CXR -mets USS and doppler MRI Schirmer's test and carlson crittenden test to monitor lacrimal tear flow FNAC Biopsy of gland if skin ulcerated or if in minor gland Labial biopsy - sjogrens |
|
|
Why perform an ACE blood test? |
Monitors for sarcoidosis |
|
|
Patient with previous pleomorphic adenocarcinoma experiences sweating over parotid gland when eating. What is this and how would you manage it? |
Frey's syndrome. Manage with antiperspirants and botox injections to skin |
|
|
Which nerves may be damaged during a submandibular gland excision? |
Marginal mandibular nerve Lingual nerve |
|

|
Erythroplakia in coffins corner |
|

|
Leukoplakia |
|
|
What spinal levels does the thyroid overlie? |
C5-T1 deep to the sternohyoid and sternothyroid |
|
|
What spinal level is the hyoid bone at? |
C3 |
|
|
What spinal level does the cricoid cartilage lie? |
C6-C7 |
|

|
Branchial cyst |
|
|
How do you differentiate between a thyroglossal cyst and a thyroid mass? |
Thyroid masses will not move when the patient sticks out their tongue |
|
|
What is the most common cause of bilateral parotid gland enlargement? |
Mumps caused by the paramyxovirus. Pain is due to the stretching of the parotid capsuleW |
|
|
What is sialadenitis? |
Inflammation of a salivary gland. Viral, bacterial, fungal, other. |
|
|
In which major salivary gland are calculi most likely to form? |
Submandibular gland due to it's thicker, more calcium rich secretions. |
|
|
How might sialolithiasis present? |
Post parandial pain and swelling with recurrent sialadenitis caused by infections. |
|
|
What is sialectasis? |
Dilation, stenosis and necrosis of acini --> cyst formation. |
|
|
What is stridor? How might the following sound: 1. Laryngeal stridor? 2. Expiratory stridor? 3. Mixed |
Noisy breathing 1. High pitched produced on inspiration 2. The wheeze of asthma 3. Tracheal breathing or laryngeal and lower airway |
|
|
What is stertor? |
Noises produced from the oro/nasopharynx such as in snoring |
|
|
Clinical signs of upper airway obstruction? |
Stridor Stertor Colour - blue? Resp rate - increased? climbing? Intercostal recession/tracheal tug? Able to talk in full sentences? |
|
|
Commonest cause of stridor during infancy? |
Laryngomalacia - soft tissue cartilage collapses during inhalation --> obstruction |
|
|
Laryngeal web - a congenital cause of upper airway obstruction |
|
|
Narrowing of the airway below the glottis that is congenital |
Subglottic stenosis |
|

|
Singer's nodules - presents with a husky voice with increased use Treat: Voice therapy and excision if necessary |
|

|
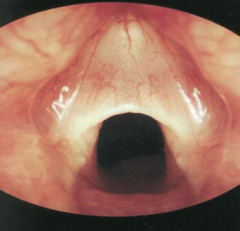
Reinke's oedema - bilateral grey swelling along entire length of membrane portion of vocal cord |
|
|
What causes Reinke's oedema? |
Smoking, talking, GORD |
|
|
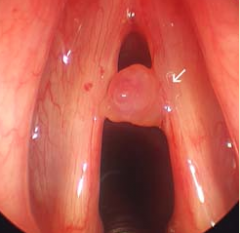
Chordal polyp |
|
|
Presentation of laryngitis Treatment? |
Hoarse voice/aphonia with reddened, oedematous vocal cords. Voice rest - discourage whispering Analgesia, steam inhalations, warmth applied to anterior neck |
|
|
What causes epiglottitis? |
Haemophillus influenzae B |
|
|
How does epiglottitis present? |
Initially with a URTI which rapidly progresses--> airway obstruction |
|
|
What are the differences between adult and child presentations of epiglottitis? |
Children: URTI - child is unwell, febrile, toxic. May drool and have difficulty swallowing. Altered or muffled cry Adults: Severe sore throat disproportionate to oropharyngeal appearance. Voice is muffled or altered. Usually no cough |
|
|
Management of epiglottitis |
Do not examine the mouth Do not perform Xray Do not lie patient down Get expert help early to intubate - give nebulised adrenaline I.V. antibiotics - ceftriaxone and penicillin Steroids Visual diagnosis with nasopharyngeal intubation Blood culture Notifiable disease |
|
|
What infection causes diffuse inflammation of the airways not just of the supra glottis? |
Croup |
|
|
How might the cough sound of a child with croup? |
Brassy like a dog's bark |
|
|
What causes croup? |
95% are viral e.g. parainfluenza |
|
|
How can severe croup be managed? |
Antibiotics, humidified oxygen and nebulised adrenaline, steroids. |
|

|
Laryngeal papilloma |
|
|
What is the main malignant condition of the upper airway? |
Squamous cell carcinoma |
|
|
What might cause recurrent laryngeal nerve palsy? |
Thyroid surgery causing damage to the recurrent laryngeal nerve. |
|
|
How might an acute upper airway obstruction be managed? |
Endotracial intubation Cricothyroidotomy Tracheostomy |
|
|
Give 5 indications for a tracheostomy |
1. In an acute situation to bypass a laryngeal obstruction 2. Following surgery of the head and neck to prevent breathing difficultlies secondary to swelling 3. In cases where long term intubation is required. Long term intubation causes scarring of the larynx 4. To prevent overspill of secretions in to the lungs e.g. in diseases where swallowing and coughing is impaired 5. To allow air entry in to the lungs following a laryngectomy |
|
|
What are the 2 types of tracheostomy? |
End tracheostomy Side tracheostomy |
|
|
Describe some early risks of a tracheostomy |
Surgical emphysema Pneumothorax Tube displacement Blocked tube |
|
|
Describe some late risks of tracheostomy |
Tracheocutaneous fistula failed closure Tracheo-oesophageal fistula Tracheal stenosis |
|
|
Define sleep apnoea |
30 or more episodes of cessation of breathing each with a minimum duration of 10seconds occurring over a duration of 7 hours sleep |
|
|
What are the long term complications of obstructive sleep apnoea? |
Pulmonary hypertension and right ventricular strain --> cor pulmonale |
|
|
What is central sleep apnoea? |
Where the central respiratory drive is at fault --> cessation of breathing |
|
|
Define what is meant by mild OSAHS |
5-14 events per hour |
|
|
What is meant by severe OSAHS |
> 30 events per hour |
|
|
Symptoms of obstructive sleep apnoea hypoponoea syndrome (OSAHS) |
Daytime sleepiness - restless sleep Witnessed apnoeas Impaire concentration Snoring Unrefreshed sleep Nocturia Choking episodes during sleep Reduced libido |
|
|
What factors increase obstructive sleep related breathing disorders? |
Age - increases up to 6th and 7th decade Sex - M:F = 2-5:1 increases in women after menopause Obesity Obstructive upper airway abnormality - e.g. craniofacial abnormalities, adenotonsiller hypertrophy, turbinate hypertrophy, nasal polyposis Social habits - smoking and alcohol Other risk factors - genetics, hypothyroidism, acromegaly, drugs causing central depression e.g. opiatesT |
|
|
Treatment of sleep related breathing disorders |
Continuous positive airway pressure (CPAP) Establish and treat possible underlying cause - localise the airway obstruction Behavioural changes - in simple snoring may allow partner to fall asleep first, earplugs Weight loss Smoking and alcohol reduction Intra-oral appliance - enlarge pharyngeal airway Drugs Surgery - upper airway or nasal Tracheostomy Uvulopalatopharyngoplasty Laser assisted uvulopalatoplasty Radiofrequency Maxillofacial surgery |
|
|
What are the vegetative symptoms of vertigo? |
Nausea Vomiting Diarrhoea and pallor |
|
|
How might the duration of a vertigo attack help with diagnosis? |
Positional vertigo - seconds to minutes Labyrinthitis - mins to hours |
|
|
How might you examine a patient complaining of vertigo? |
Otoscopy Nystagmus - direction and degree Cranial nerve examination Past pointing Romburg Dix Hallpike - BPPV
|
|
|
What would a positive Romburg sign indicate in a patient with vertigo? |
Vestibular deficit |
|
|
What causes BPPV |
Debris / otochonia in the semicircular canals |
|
|
How can you manage BPPV? |
Epley manouvre |
|
|
In BPPV what will show in the dix hallpike manoeuvre? |
Dizziness and downwards (geotropic) rotational nystagmus Nystagmus will be latent and will fatigue Patient's dizziness or nystagmus will stop after 30secs or so |
|
|
How might cholesteatoma cause vertigo? |
Sac erosion of the labyrinth |
|
|
Why must long term vestibular sedatives be avoided? |
Can cause parkinsonism like symptoms and delay central compensation --> prolonged vestibular rehab. Vestibular sedatives usually settles vertigo within couple of days in labyrinthine causes. If vertigo has not settled and nystagmus is present this suggests a central lesion |
|
|
Describe the typical presentation of vestibular neuronitis |
Acute severe attack of isolated vertigo with nystagmus and often vomiting but WITHOUT loss of hearing. Caused by viral infections affecting the labyrinth or vestibular nerve BPPV may follow. |
|
|
What are the differentials of vestibular neuronitis? |
Demyelination or vascular lesions in the brain stem but these often are accompanied by other abnormalities |
|
|
Management of vestibular neuronitis |
Vestibular sedatives e.g. cinnarizine and possibly steroids |
|
|
How would you manage labyrinthitis |
Vestibular rehab therapy with balance exercises. Prochlorpromazine, cinnarizine. |
|
|
Describe the typical symptoms of sudden vestibular failure |
Prostration, nausea and vomiting. No auditory features. |
|
|
What is presbystasis? |
Disequilibrium caused by ageing with no known aetiology. = diagnosis of exclusion, must rule out other pathology |
|
|
What is a vestibular migraine? |
A migraine with symptoms associated with inner ear balance and mechanisms. Vertigo can occur in the absence of headache. |
|
|
How can you treat vestibular migraines? |
Pitozifen Amytriptyline Propanolol |
|
|
What are the differentials of a patient presenting with "dizziness"? |
Vertigo - false sense of motion or spinning Disequilibrium - off balance or wobbly Presyncope - feeling of losing consciousness Lightheadedness - Vague symptoms, possibly feeling disconnected from the environment |
|
|
What might cause disequlibrium? |
Parkinson's disease (observe patient's gait or coordination) or diabetic neuropathy |
|
|
Name some causes of light headedness? |
Psychiatric - depression, anxiety, hyperventilation syndrome |
|
|
How might you manage othostatic hypotension causing pre syncope? |
Alpha agonists, mineralocorticoids, lifestyle changes |
|
|
Swaying to the left on a Romburg test would indicate what? |
Vestibular dysfunction on the left side |
|
|
What is spontaneous jerk nystagmus a sign of? |
Vestibular disease
|
|
|
What signs of jerk nystagmus indicate a central cause within the brain? |
Nystagmus persisting for more than a few weeks A change in direction of the beat with time or following a change in gaze direction Beating in directions other than horizontally Different jerks in 2 eyes |
|
|
How would you manage vestibular neuritis |
Vestibular sedatives and steroids |
|
|
Where does the eustachian tube open? |
into the nasopharynx |
|
|
What are the 3 divisions of the pharynx? |
Nasopharynx Oropharynx Hypopharynx |
|
|
How is the hypopharnx divided? |
2 lateral recesses: the piriform fossa Posterior pharyngeal wall Postcricoid space |
|
|
What is the function of the hypopharynx? |
To channel food from the oropharynx to the oesophagus and act as a resonance chamber for voice. |
|
|
Name 3 functions of the larynx |
To protect the distal airway Production of voice Glottis closure during lifting and straining to support the diaphragm |
|
|
What are the key features that indicate a malignant cause of hoarseness? |
S- Smoking, stridor C- Constant/persistent hoarseness, coughing up blood A- acute onset not associated with an URTI, alcohol L- loss of weight D- Dyspnoea, Dysphagia
Must ask about referred pain - otalgia |
|
|
Describe the MDT approach to common voice problems |
Voice therapy: Vocal hygiene advice, lubrication, hydration and avoidance of irritants. Technical advice e.g. posture Medical therapy: Antibiotics, antifungals, antireflux, dietary advice and botox injections Surgical therapy: |
|
|
When might someone receive botox injections? |
Spasmodic dysphonia |
|
|
What symptoms indicate the possibility of laryngeal carcinoma? |
Hoarseness lasting >6weeks. Stridor. Referred otalgia. Dysphagia. Lymphadenopathy. |
|
|
What signs indicate a laryngeal carcinoma? |
Raised, thickened irregular mass with leukoplakia and redness. Narrowing of airway +/- vocal cord fixation Cervical lymphadenopathy |
|
|
How would you treat laryngeal carcinoma? |
Radiotherapy with partial or total excision. |
|
|
What are the symptoms of recurrent laryngeal nerve palsy? |
Weak voice that tires with prolonged use Perilaryngeal discomfort Choking with fluids Higher pitched voice Diplophonia Weak cough |
|
|
Which side is more commonly affected by recurrent laryngeal nerve palsy? |
Left side as it has a longer course |
|
|
How would you investigate? |
CXR - exclude mediastinal mass CT scan of skull base and mid thorax - check lesions along path of nerve Barium swallow if oesophageal lesion or aspiration suspected |
|
|
What are the treatments available for vocal cord palsy? |
Await spontaneous recovery Voice therapy to encourage compensation Surgery: Vocal cord medialisation |
|
|
What are the symptoms of recurrent laryngeal nerve palsy? |
Weak voice that tires on use Perilaryngeal discomfort Choking with fluids Higher pitched voice Diplophonia - 2 toned voice Weak cough |
|
|
What is the primary cause of muscle tension imbalance (MTI)? |
Excessive tension on the laryngeal muscles |
|
|
What causes MTI? |
Stress, depression, poor posture, poor vocal hygiene - talking for long periods over background noise, shouting required for job, eating late at night, not drinking enough fluids, drinking too much caffeine |
|
|
What is the secondary cause of MTI aka dyspnonia? |
Excessive tension required to overcome a deficiency in the boise producing mechanism e.g. poor resp function, defect in folds, nasal blockage affecting resonance. |
|
|
What are the signs and symptoms of MTI (dysphonia) |
Variable huskiness of voice - worsens with use Deeper or higher voice than expected Unstable voice Perilaryngeal soreness Dry/uncomfortable throat Cough usually normal Vocal fold movement abnormal |
|
|
What abnormal vocal cord movements would you expect to see in MTI (dysphonia) |
Anteroposterior constriction Extreme sphincteric closure --> vocal folds disappear from view beneath vocal cords |
|
|
How can you treat MTI (dysphonia) |
Vocal hygeine and lifestyle advice Voice therapy Adress underlying cause |
|
|
What causes vocal polyps? |
Shouting when suffering from GORD or cold |
|
|
What symptoms may a patient get with vocal polyps? |
Husky voice, may be deeper Voice cuts out during speaking |
|
|
What are the non infectious causes of vocal cord lesions? |
Silent reflux Allergy |
|
|
What 4 subgroups can vocal fold changes be categorised in to? |
Increase in vocal fold mass --> lower pitch voice e.g. Reinke's oedema Poor closure of folds --> breathy, weak voice e.g. recurrent laryngeal nerve palsy Increase in stiffness of fold --> poor vibration with rough, harsh voice Lesion on the free edge of the fold --> irregular voice with pitch breaks e.g. nodules, cysts, HPV |