Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
76 Cards in this Set
- Front
- Back
|
What cytokine made by macrophages in inflammation elicits production of acute phase reactants by the liver?
|
IL-6
|
|
|
negative APR:
APR: |
Albumin, prealbumin, RBP, transferrin
C3, MBP, CRP, a-1-at, a2mg, ceruloplasmin, fibrinogen, F8, haptoglobin, SAA, fibronectin... |
|
|
What is the fastest migrating protein on SPEP?
|
Prealbumin = transthyretin
Rarely seen as such small quantities |
|
|
What is the amyloid precursor protein in senile cardiac amyloidosis?
|
prealbumin
|
|
|
half life of albumin? prealbumin?
|
alb: 17d
prealb: 2d |
|
|
Name 2 causes of truly elevated prealbumin
fake elevation? |
chronic alcohol; corticosteroid therapy
falsely elevated in heparin therapy: alters beta-lipoprotein (LDL) such that it migrates in the prealbumin range |
|
|
hallmark of CSF-PEP?
|
sharp prealbumin band. crosses BBB & is actively secreted.
also: double transferrin peak (beta region). BBB transports transferrin but modifies some to Tau protein |
|
|
What migrates to the prealbumin region?
|
prealbumin / transthyretin
RBP (retinol binding protein - Vit A) |
|
|
what regions INCREASE in inflammation?
decrease? |
a1 : a1at (and orosomucoid = a1-acid-gp)
a2: haptoglobin, ceruloplasmin gamma1: gamma globulins gamma2: CRP decreased: albumin, prealbumin, transferrin (beta1) |
|
|
the greatest decreases in serum albumin are seen in?
|
protein-losing conditions (nephrotic syndrome)
|
|
|
classic pattern in nephrosis
|
low albumin
high a2 (a2macroglobulin) low gamma globulin |
|
normal spep.
where is the "origin" located? Which is the anode & which is the cathode? |
origin in located in the gamma region
the anode is on the left, it is + charged, and most proteins are - charged the cathode is on the right and is - charged, gamma globulins are weakly negative so they don't move far from the application site |
|
|
What is the most common defect in HyperIgM Syndrome?
|
defect in a Th2 cell protein (CD40 ligand). The disorder causes immunodeficiencies, including a higher than normal susceptibility to various types of infections.
Can't class switch! |
|
|
What are the 2 most obvious bands that are present in PLASMA but not SERUM?
|
Prothrombin (alpha 1 region)
Fibrinogen (Beta-gamma region)(can misinterpret as an M protein) (Ethanol can precipitate this out in vitro!) |
|
|
beta-gamma bridging is the hallmark of?
|
cirrhosis
|
|
|
Features of tubular proteinura UPEP?
glomerular? |
Tubular - weak albumin band, strong a1, b. impaired tubular reabsorption
glom - Strong albumin band, strong a1, b. Very large and very small proteins are conserved in the kidney |
|
|
Type I cryoglobulins
|
monoclonal. myeloma or waldenstroms
|
|
|
Type 2 cryo
|
monoclonal IgM (RF activity - anti-IgG)
AND polyclonal IgG most common |
|
|
Type 3 cryo
|
mixture 2 polyclonal
|
|
|
#1 cause of mixed cryoglobulinemia (types 2 & 3)
|
HCV
|
|
|
clinical sx of cryoglobulinemia?
Most common renal finding? |
PURPURA (leukocytoclastic vasculitis)
arthralgia HSG LAD anemia sensorineural deficits glomerulonephritis MPGN2 |
|
|
what cardiac marker rises the most compared to normal, following an MI?
What cardiac marker stays elevated the longest following an MI? |
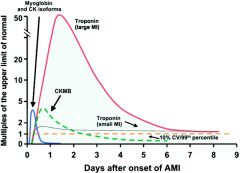
Troponins. 50x normal levels. Most assays measure cardiac troponin I, though there's not much difference with T.
Troponins. Up to 10 days. |
|
|
What conditions can show a "flipped" LDH ratio, where LDH1 > LDH2?
|
Hemolysis, AMI, renal infarct
..since LDH1 is found in RBCs, heart, and kidney |
|
|
What is LDH-6 and what does it mean in terms of prognosis?
|
LDH6 is not a true isoenzyme of LDH but a mimic that is seen predominantly in alcohol use and indicates hepatic vascular insufficiency in the setting of shock
BAD px |
|
|
What is macro-CK-2?
|
aka mitochondrial CK
a normal variant of CK that is found in mitochondria, however its presence is a BAD finding and is usually seen in advanced disseminated malignancies |
|
|
What is macro-CK-1?
|
An Ig-CK complex that is not cleared readily from the circulation and persists. Autoimmune. Can lead to a chronically elevated CK level, but has no other clinical significance.
|
|
|
AST:ALT in EtOH?
viral hepatitis? |
>2
<1 |
|
|
what is the Regan isoenzyme?
|
form of placental alkaline phosphatase seen in 5% pts with carcinoma
|
|
|
What is the affect of heparin on ALT & AST?
Renal failure? |
Heparin can INCREASE these
Renal failure DECREASES them (cause is unknown) |
|
|
acid phosphatase found most in?
|
RBCs, prostate, bone
|
|
|
How to tell RBC acid phosphatase from others?
|
RBC is RESISTANT to tartrate (=TRAP, same as hairy cell leuk)
|
|
|
What blood groups have higher NONFASTING alkaline phosphatase?
|
Lewis + group B & O
|
|
|
What form of bilirubin is found in the urine?
What form is responsive to phototherapy? |
Urine only has CONJUGATED
UNconjugated responds to phototherapy |
|
|
autoimmune hepatitis shows polyclonal increase in what globulins?
primary biliary cirrhosis? |
ai: IgG
PBC: IgM |
|
|
Causes of UNconjugated hyperbili?
|
Crigler Najar
Gilbert Bowel obstruction Hemolysis Physiologic jaundice, breast milk jaundice |
|
|
Causes of conjugated hyperbili?
|
Dubin Johnson
Rotor Biliary obstruction Sepsis neonatal hepatitis TPN |
|
|
When to worry about neonatal jaundice:
Threshold for exchange transfusion? |
- 1st 24h of life
- continuing to rise after 1 week - Total bili > 12, conj>2, or increase of >5 in one day exchange transfusion when bili >20 |
|
|
Persistently elevated serum amylase concerning for?
What is the most common cause of a normal amylase in the setting of acute pancreatitis? |
pseudocyst
hypertriglyceridemia (TG inhibit the amylase assay) |
|
|
# isoenzymes of amylase & what are they
|
6
first 3 are salivary on electrophoresis last 3 are pancreatic salivary is inhibited by wheat germ lectin (triticum vulgaris amylase is cleared by the kidneys |
|
|
how do amylase, CEA, CA19-9 vary among pancreatic cysts?
|
pseudocyst has elevated amylase
CEA is elevated in mucinous (mucinous cystadenoma has only CEA elevated, IPMN has all 3 elevated) serous and solid-pseudopapillary have decreased all 3 |
|
|
what is delta-bilirubin?
|
conjugated bili covalently linked to albumin, cannot be readily excreted. thus conjugated bili measurements may persist after treatment
|
|
|
palpable purpura (leukocytoclastic vasculitis)
arthralgia HSG anemia sensorineural deficits glomerulonephritis (most commonly?) |
cryoglobulinemia
MPGN2 |
|
|
Rapid correction of hyponatremia can lead to?
Slow correction? |
CPM
cerebral edema |
|
|
Normal BUN:Cr ratio?
|
10:1
Increased: poor renal perfusion (BUN reabsorbed) Decreased: rare: liver disease, poor intake |
|
|
What 4 hormones share the same alpha subunit?
|
hcg
TSH FSH LH |
|
|
When does hcg peak?
|
end of first trimester
|
|
|
increased hcg & inhibin
decreased AFP & uE |
Trisomy 21
|
|
|
decreased AFP, uE, hcg
|
Trisomy 18
|
|
|
increased AFP only
|
neural tube defect
|
|
|
notable drugs eliminated by zero-order kinetics (most drugs are eliminated by first-order = proportional to drug concentration)
|
EtOH
ASA phenytoin |
|
|
what two toxins will give an osmol gap on the commonly used platform of freezing point depression, but not with the less commonly used vapor pressure osmometry?
|
Ethanol & methanol
|
|
|
Metabolites of methanol? source?
|
formate & formaldehyde
windshield washer fluid |
|
|
Metabolites of ethylene glycol? source?
clues in lab? |
oxalate & glycolate
antifreeze calcium oxalate crystals! |
|
|
What 2 alcohols do not cause acidosis but do produce an OSMOL gap?
|
Ethanol
Isopropanol |
|
|
Treatment of methanol or ethylene glycol OD?
|
Ethanol! competitively inhibits the enzyme alcohol dehydrogenase, which is responsible for producing the toxic metabolites of these drugs
|
|
|
abdominal pain and bilateral wrist drop
|
long-term lead poisoning
|
|
|
How does Fe deficiency perpetuate Pb toxicity (2 ways)?
|
1. Can't make heme molecules so protoporphyrins are increased (precursor)
2. Increased GI uptake of Fe also increased uptake of Pb |
|
|
Elevated free erythrocyte protoporphyrin (FEP) and zinc-protoporphyrin (ZPP) are elevated in what 2 conditions?
|
lead poisoning
iron deficiency |
|
|
What levels of CO are seen in smokers?
Severe symptoms with lethargy, LOC? |
2-6%
20-50% |
|
|
Time from ingestion for full acetaminophen absorption?
antidote? |
4 hours
N-acetylcysteine (promotes metabolism via conjugation and decreased production of toxic NAPQI) |
|
|
Why do alcoholics have a higher risk of hepatic injury from acetaminophen toxicity?
what zone of the liver shows acetaminophen toxicity? |
Alcohol induces the P450 system in the liver, wchih increases the amount of acetaminophen metabolized to NAPQI
Zone 3 (centrilobular) |
|
|
Bitter almond odor in breath
|
Cyanide toxicity
|
|
|
Clues to cyanide toxicity
mechanism? |
almond breath
cherry red skin severe anion gap metabolic acidosis (LACTATE) inhalation of smoke (insulation) or pesticide increased THIOCYANATE (metabolite) CN binds cytochrome a3 and leads to decreased oxygen-dependent metabolism |
|
|
treatment of CN tox
|
nitrites (form met-hgb) and sodium thiosulfate (forms thiocyanate, harmless compound eliminated by kidneys)
|
|
|
Earliest signs of ASA OD?
|
tinnitus & dizziness
|
|
|
Mortality in aspirin OD is best correlated with the ___-hr plasma salicylate concentration, with values >___mg/dL having a high fatality rate
|
6
130 |
|
|
what are the crazy stages of metabolic / respiratory / acidosis / alkalosis in ASA toxicity?
|
1. Respiratory alkalosis, 3-8h post ingestion, from direct stimulation of respiratory center
2. Compensatory metabolic acidosis, 12-24h, where patients usually present 3. Increased anion gap metabolic acidosis, through metabolic effects such as Krebs cycle inhibition 4. respiratory acidosis from CNS depression |
|
|
Ingested arsenic is largely excreted in the ____ with most of the remainder distributed into ____, _____, and ____.
|
urine
skin, nails, and hair |
|
|
Sx arsenic toxicity
|
vomiting, bloody diarrhea, abdominal pain
cytopenias with basophilic stippling peripheral neuropathy, nephropathy, skin hyperpigmentation and hyperkeratosis |
|
|
2 characteristic syndromes with weird names associated with chronic mercury toxicity
|
1. Acrodynia / Feer syndrome
-autonomic manifestatsions and desquamative erythematous rash palms & soles. - increased urinary catecholamines ~ pheo! 2. Erethism - CNS d/o with personality changes, irritability, fine motor disturbances |
|
|
name 2 toxins that are best screened for with 24-hour urine levels
|
arsenic & elemental mercury
|
|
|
what drug, when taken with digoxin, enhances its toxicity?
|
quinidine
|
|
|
best test of quinidine toxicity
|
EKG (prolonged QT interval, torsades de pointes)
|
|
|
digoxin t 1/2
|
36h
|
|
|
warfarin dosing in a patient with mutations in:
VKORC1 CYP2C9 |
VKORC1: confers warfarin resistance & requires INCREASED dose
CYP2C9: Leads to DECREASED warfarin metabolism, and increased serum levels, so DECREASED dosage is needed |
|
|
Tangier disease
|
AR
Absent Apo-A1, no HDL |