Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
79 Cards in this Set
- Front
- Back

Basic steps in neurotransmission: sites of drug action
|
1. Uptake of precursors
2. Synthesis of transmitter 3. Uptake/ transport of transmitter into vesicles 4. Degradation of surplus transmitter 5. Depolarization by propagated action potential 6. Influx of Ca in response to depolarization 7. Release of transmitter by exocytosis 8. Diffusion to postsynaptic membrane 9. Interaction with postsynaptic receptors 10. Inactivation of transmitter 11. Reuptake of transmitter or degradation products by nerve terminals 12. Uptake of transmitter by non-neuronal cells 13. Interaction with presynaptic receptors |
|
|
Major neurotransmitters in the body
|
1. Acetylcholine
2. Dopamine 3. GABA (gamma-aminobutyric acid) 4. Glutamate 5. Glycine 6. Norepinephrine 7. Serotonin |
|
|
Acetycholine - role
|
1. Used by the spinal cord neurons to control muscles
2. Used by many neurons in the brain to regulate memory. 3. Excitatory: most instances |
|
|
Dopamine - role
|
Produces feelings of pleasure
Inhibitory usually |
|
|
GABA
|
Major inhibitory neurotransmitter in the brain
|
|
|
Glutamate
|
Most common excitatory neurotransmitter in the brain
|
|
|
Glycine
|
Used mainly by neurons in the spinal cord.
Always inhibitory |
|
|
Norepinephrine
|
Neurotransmitter and a hormone
Peripheral nervous system: part of the fight-flight response Brain: neurotransmitter regulating normal brain processes Excitatory usually, but inhibitory in a few brain areas |
|
|
Serotonin
|
Inhibitory in pain pathways in the spinal cord
|
|
|
Ways that drugs interfere with neurotransmission
|
1. Increasing number of impulses
2. Release NT from vesicles with or without impulses 3. Block reuptake or block receptors 4. Produce more or less NT 5. Prevent vesicles from releasing NT |
|
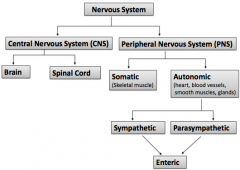
What nervous system does autonomic belong to?
|
Peripheral nervous system (PNS)
|
|
|
What does autonomic control?
|
1. Conveys all the outputs from CNS to rest of the body
- Except the motor innervation to skeletal muscle 1. Heart 2. Blood vessels 3. Smooth muscles 4. Glands 2. Regulates the involuntary function of the body i. Smooth muscle tone - Contraction and relaxation of vascular and visceral smooth muscle ii. The heart rhythm and force iii. All exocrine (skin, salivary, lacrimal) and certain endocrine (renin from kidneys) secretions iv. Energy metabolism (particularly in liver and skeletal muscle) e.g. digesting a meal and maintaining BP |
|
|
What are the two systems that belong to the autonomic?
|
1. Sympathetic
2. Parasympathetic Can not work alone |
|
|
Autonomic nervous system (ANS): Sensory receptors -> sensory neurons -> CNS (Integration) -> Preganglionic autonomic Efferent neurons (motor neurons)
-> ?????????????????? -> Effector organ |
GANGLIA
|
|
|
Autonomic nervous system - Roles
|
1. Maintain homeostasis
2. Most organs receive dual innervaton (some exceptions) 3. In general, opposing actions of the two systems balance one another 4. A rise in parasymp activity is accompanied by a fall in sympathetic activity (some exceptions) |
|
|
Some general rules of ANS neurotransmission - All motor nerve fibers leaving the CNS release ACh -> nicotinic receptors
|
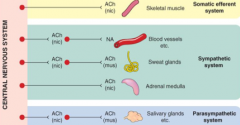
True
|
|
|
Some general rules of ANS neurotransmission - All postganglionic PS fibers release ACh -> muscarinic receptors - T/F?
|
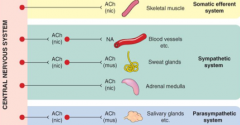
True
|
|
|
Some general rules of ANS neurotransmission - All postganglionic sympathetic fibers release NA -> a & b receptors - T/F?
What is the exception? |
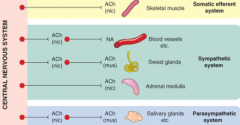
True
Except sweat glands - ACh->muscarinic receptors |
|
|
Parasympathetic
1. Origin 2. Innervation 3. Autonomic ganglia 4. Length of fibers 5. Ratio of preganglionic to postganglionic fibers 6. Response 7. Chemical transmitter at autonomic ganglia 8. Chemical transmitter at the postganglionic nerve ending |
1. Craniosacral
2. Cardiac muscle, smooth muscle, glands, viscera 3. Near or within the wall of the effector 4. Preganglionic (lomg) Postganglionic (short) 5. Branching of minimal 6. Discrete 7. ACh 8. ACh |
|
|
Sympathetic
1. Origin 2. Innervation 3. Autonomic ganglia 4. Length of fibers 5. Ratio of preganglionic to postganglionic fibers 6. Response 7. Chemical transmitter at autonomic ganglia 8. Chemical transmitter at the postganglionic nerve ending |
1. Thoracolumbar
2. Cardiac muscle, smooth muscle, glands, viscera 3. Near the CNS 4. Preganglionic (short) Postganglionic (long) 5. High degree of nerve branching 6. Diffuse 7. ACh 8. NA (most cases) Adrenaline and NA (adrenal medulla) ACh (sweat glands) |
|
|
Most organs receive dual innervation, what the the exceptions - Only sympathetic?
|
1. Sweat glands
2. Salivary glands 3. Adrenal medulla 4. Kidney 5. Pilomotor muscles |
|
|
Most organs receive dual innervation, what the the exceptions - Only parasympathetic?
|
1. Most blood vessels
2. Ciliary muscle of the eye 3. Bronchial smooth muscle |
|
|
Cholinergic transmission - What is it?
|
???
|
|
|
fgdhd
|
gfjjjhfg
|
|
|
Parasympathetic nervous system
|
1. REST & Digest: Conserves energy and restores body resources
2. Dec HR 2. Inc GIT activity 3. Inc digestive enzyme secretion 4. -> Inc Digestion abd Absorption |
|
|
Sympathetic nervous system
|
1. Fight or Flight: Dominates during stress and emergency situations
2. Inc HR and BP 3. Inc blood sugar conc 4. Inc blood flow to skeletal and cardiac muscles 5. Dec blood flow to skin and internal organs 6. Mobilizes energy stores 7. Dilates pupil and bronchioles |
|
|
fjjhg
|
gjkk
|
|
|
Cholinergic transmission - What chemical transmitter has both muscarinic and nicotinic effects?
|
ACh
|
|
|
Muscarinic effects
|
Closely resembles PS stimulation
|
|
|
Nicotinic effects
|
1. Stim of all autonomic ganglia
2. Stim of voluntary muscle 3. Adrenaline secretion from adrenal medulla |
|
|
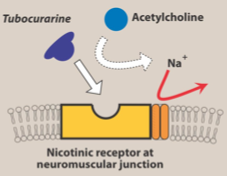
Nicotinic ACh receptors -
1. What are they? 2. What activates and blocks? 3. What types? |
1. Ligand gated ion channel - rosette like pentameric structure -> rapid inflow of cations -> depolarization -> AP
2. Selectively activated by nicotine and blocked by tubocurarine or hexamethonium 3. NM type: Muscle type - stim by PTMA and blocked by tubocurarine NN type: Ganglion type - stim by DMPP and blocked by hexamethonium |
|
|
Nicotinic ACh receptors - Types
1. Location 2. Mechanism of signal transduction 3. Functional response |
NM type - Muscle type
1. Skeletal muscle NMJ, mainly postsynaptic 2. Excitatory; increase cation permeability (Na, K) 3. Skeletal muscle contraction |
|
|
Nicotinic ACh receptors - Types
1. Location 2. Mechanism of signal transduction 3. Functional response |
NN type - Ganglion type
1. Autonomic ganglia, mainly postsynaptic 2. Excitatory, increase cation permeability (NA, K) 3. Secretion of catecholamines Excitation of postganglionic neurons |
|
|
Muscarinic receptors -
1. What are they? 2. Types |
1. G-protein coupled receptors
2. M1-M5 - M1, M3, M5 -> Gq protein -> Activation of PLC -> IP3/DAG -> Inc Ca & PKC - M2, M4 -> Gi protein -> Inhibition of AC -> Dec cAMP -> Dec. Ca conductance |
|
|
ACh receptors - Muscarinic - Types
|
M1: Neuronal
M2: Cardiac M3: Glandular |
|
|
Muscarinic agonists
1. What effects? 2. What are they? 3. Structure 4. Name a few |
1. Parasympathomimetic drugs
2. A quaternary ammonium group 3. An ester group: susceptible for hydrolysis by cholinesterase 4. ACh Carbachol Methacholine Bethanechol Muscarine Pilocarpine Oxotremorine |
|
|
Muscarinic agonists - Pharmalogical effects
|
1. Cardiovascular
- Blood vessels - DIlate - Heart rate - Slow - BP -Dec. 2. GIT - Tone - Inc. - Motility - Inc. - Sphincters - Relaxed 3. Glands - Inc. salivary, lacrimal, intestinal and sweat secretion 4. Eye - Pupil constricts and dec. accommodation |
|
|
Muscarinic agonists - Major clinical use
|
1. Glaucoma and to reverse the effects of mydriatics
- ACh, Pilocarpine, Carbachol 2. Xerostomia - 5-10mg pilocarpine -> Inc. parotid, subman and sublingual secretions - Max flow rates in 30 min, return to baseline in about 3 hrs - 3 times daily - Salivatory stimulatory effects depends on residual salivary gland function - No sig effects on BP, HR, or cardiac function at these doses - Sweating (common), chills, nausea, and dizziness also reported - Cevimeline more selective for M1&M2 (fewer adverse effects) - Oral fluid, saliva substitutes |
|
|
Muscarinic agonists - Adverse effects
|
DUMBELS
1. DIarrhea 2. Urination 3. Miosis 4. Bronchoconstriction 5. Excitaion 6. Lacrimation 7. Salivation |
|
|
Slide 36
|
jghg
|
|
|
What products results from hydrolysis of ACh?
|
1. Choline
2. Acetate |
|
|
Give one example of drug that acts as cholinesterase blockers?
|
1. Reversible
- Edrophonium - Neostigmine - Physostigmine - Pyridostigmine - Donepezil - Rivastigmine - Galantamine 2. Irreversible - Ecothiophate |
|
|
Mechanisms of reversible vs irreversible AChE inhibitors
|
Slide38
|
|
|
Anticholinesterases - Edrophonium
|
1. Quaternary alcohol
2. REversible binding by electrostatic forces and hydrogen bonds to the active site 3. Prevent access to ACh 4. No covalent bond involved, therefore enzyme-inhibito complex is short-lived (2-10mins) |
|
|
Anticholinesterases - Neostigmine and Physostigmine
|
1. Carbamate esters
2. Covalent bonds 3. Longer time to be hydrolyzed (30min-6hrs) |
|
|
Anticholinesterases- Organophohsphates
|
1. Irreversible AChE inhibitor - Ecothiophate
2. Phosphorylates the active site: binds covalently via its phosphate group to serine-OH group at the active site -> loss of alkyl group (aging) -> impossible for enzyme reactivators (PAM) to break the bond between the remaining drug and the enzyme -> Permanently inactivates the enzyme -> Restoration requires synthesis of new enzyme molecules |
|
|
AChE: Pharmacological effects-CNS
|
- Excitation -> convulsions (low dose)
- Depression - unconsciousness - respiratory failure (high dose) |
|
|
AChE: Pharmacological effects - Effect of autonomic cholinergic synapses
|
1. Inc salivary, lacrimal, bronchial, GIT secretions
2. Inc peristaltic activity 3. Bronchoconstriction 4. Bradycardia, hypotension 5. Miosis 6. Dec. intraocular pressure |
|
|
AChE: Pharmacological effects - Effect on NMJ
|
1. Inc strength of contraction
2. Fibrilation of muscle fiber 3. High does -> depolarise NM blockade 4. Reversal of tubocurarine effect 5. Improved transmission in myasthenia gravis |
|
|
AChE: Pharmacological effects - Demyelination of nerves
|
Weakness and sensory loss
|
|
|
AChE: Pharmacological effects - Cholinesterase activators
What is the name? What does it do? |
1. Pralidoxime (PAM)
2. Reactivates ChE once blocked by organophosphates |
|
|
Muscaricnic agonists - Clinical uses
|
1. Glaucoma (pilocarpine and physostigmine)
2. Postoperative ileus - congenital megacolon 3. Postoperative urinary retention - neurogenic bladder 4. Reflux oesophagitis 5. To reverse the actions of non depolarizing NMJ blockers 6. Myasthenia Gravis 7. Alzheimer's disease 8. Atropine poisoning |
|
|
Organophosphate poisoning
1. Signs and symptoms 2. What to do |
1. Signs and symptoms
- Salivation - Sweating - Bronshoconstriction - Vomiting - Diarrhoea - Depolarizing NMJ blockade 2. What to do - Maintain vital signs - Decontaminate - High dose atropine |
|
|
Muscarinic antagonists
1. Another name 2. What are they? 3. Structure 4. Names |
1. Parasympatholytic drugs
2. Competitive antagonists 3. Usually contain ester and basic group in the same relationship as ACh 4. Atropine - Scopolamine - Ipratropium - Tropicamide - Cyclopentolate - Pirenzepine - Darifenacin |
|
|
Muscarinic antagonists - Pharmacological effects
|
1. Inhibition of secretions
2. Effects on heart rate 3. Effects on eye 4. Effects on GIT 5. Effects on other smooth muscles 6. Effects on CNS |
|
|
Muscarinic antagonists - Pharmacological effects -
|
hjgkhg
|
|
|
Muscarinic antagonists - Pharmacological effects
|
hfhkf
|
|
|
Muscarinic antagonists - Pharmacological effects
|
hfhg
|
|
|
Muscarinic antagonists - Pharmacological effects
|
hgkkh
|
|
|
Muscarinic antagonists - Pharmacological effects
|
hghgj
|
|
|
Muscarinic antagonists - Pharmacological effects
|
hjgk
|
|
|
Muscarinic antagonists - Atropine
|
1. In opthalmology, to produce mydriasis and cycloplegia prior to refraction
2. To treat spastic disorders of GI and lower urinary tract 3. To treat organophosphate poisoning 4. To suppress respiratory secretions prior to surgery |
|
|
Muscarinic antagonists - Scopolamine
|
1. In obstetrics, with morphine to produce amnesia and sedation
2. To prevent motion sickness |
|
|
Muscarinic antagonists - Ipratropium
|
Tx of asthma
|
|
|
Muscarinic antagonists - Pirenzipine
|
Peptic ulcer
|
|
|
Muscarinic antagonists - Darifenacin
|
Urinary incontinence
|
|
|
Muscarinic antagonists - Tropicamide/Cyclopentolate
|
Ophthalmology use, short acting than atropine
|
|
|
Adverse effects of muscarinic antagonists
|
1. Blurred vision
2. Confusion 3. Mydriasis 4. Constipation 5. Urinary retention |
|
|
Cholinergic blocking agents - Dental practice
|
1. Do not overhead dental light into eyes (Photophobia)
2. Monitor heart rate and qualities before tx 3. Make sure the walkway is unobstructed (blurred vision) 4. Examine oral cavity for caries, candidiasis, periodontal 5. Oral health education - Chronic dry mouth: Home F products on a daily basis - Xylitol gum - stim saliva for anti-caries effect |
|
|
Neuromuscular junction (NMJ) blockers
1. What do they do? 2. Structure 3. Used clinically |
1. Block the cholinergic transmission between motor nerve endings and nicotinic receptors on the neuromuscular endplate of skeletal muscle.
2. Structural analogues of ACh - Act either as antagonists -> non-depolarizing type - Or agonist -> depolarizing type at receptors on the endplate of the NMJ. 3. During surgery for complete muscle relaxation, without using higher doses of anaesthesia |
|
|
Classification of muscle relaxants according to mechanism of action
|
1. Depolarizing: Succinylcholine
2. Nondepolarizing: - Pancuronium - Atracurium - Cisatracurium - Doxacurium - Vecuronium - Pipecurium - Mivacurium - Rocuronium |
|
|
Muscle relaxants: Non depolarizing agents
|
1. Also called competitive or stabilizing agents
2. Compete with ACh at the NMJ 3. Blocks the effects of ACh -> muscle paralysis and flaccidity 4. Can be counteracted clinically by AntiChE drugs 5. Initial muscle weakness quickly changes to flaccid paralysis |
|
|
Muscle relaxants: Non depolarizing agents
|
1. First muslces affected are those innervated by cranial nerves (eyes, face and neck)
2. Followed by Limb, Abdomen, Trunk, Intercostals and diaphragm 3. Recovery usually in reverse order |
|
|
Muscle relaxants : Can non depolarizing agents affect mental status or pain?
|
NO because they do not cross BBB
|
|
|
Muscle relaxants: Use of non depolarizing agents
|
Intermediate and prolonged muscle relaxatoin
1. Facilitated intubation 2. Muscle relaxation for surgery 3. Continued mechanical ventilation 4. Prevent additional injury (penetrating globe injuries) |
|
|
Muscle relaxants: Depolarizing agents - Suxamethomium/Succinylcholine - Biphasic effect
|
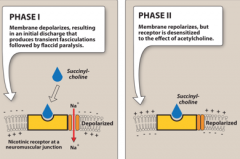
1. Phase1:
- Acts like ACh and depolarizes the synaptic membranes of the mucle - Not deactivated by AChase - Causes muscle fasiculations, followed by muscle paralysis and flaccidity 2. Phase 2: Not seen except in high concentrations - Causes receptor site blockade and continued paralysis |
|
|
Muscle relaxants - Succinylcholine
|
1. Only clinically available agent
2. Bisfunctional agonist - two cholines esterified to a central dicarboxylic acid. 3. Resistant to AChE, but susceptible to plasma ChE 4. Binds to nicotinic receptors in skeletal muscle - Initial spasm: due to maintained depolarisation at end-plate since the drugs act as agonists - Paralysis: due to inactivation of voltage-sensitve Na channels by over-depolarisation |
|
|
Muscle relaxants - Succinylcholine - Uses
|
Rapid endotracheal intubation during the induction of anaestheis
Electroconvulsive shock tx |
|
|
Muscle relaxants - Succinylcholine - Adverse effects
|
1. Malignant hyperthermia
2. Apnoea 3. Hyperkalemia |