Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
96 Cards in this Set
- Front
- Back
|
23 year-old female
Malar rash, proteinuria, joint pain LAD Lymphocytes show functionally defective FAS gene product Effect of this mutation |
Impairs efficacy of CTLs in deleting clones of autoreactive T lymphocytes
AS a result, those self-recognizing T lymphocytes go on to cause considerable damage |
|
|
Ligaments preventing anterior/posterior displacement.
|
Anterior = ACL
Posterior = PCL |
|
|
64 year-old male
Difficulty walking Reports muscle cramps after walking on level ground Cramps subside with rest Decreased sexual performance h/o MI and carotid endarterectomy Diagnosis Pathophys |
Intermittent claudication (muscle pain w/exercise that remits with rest) is almost ALWAYS result of ATHEROSCLEROSIS of larger named arteries.
Obstruciotn of blood flow in arteries results from fixed stenotic atheromatous lesions. Note that atheromas are lipid-filled intimal plaques that bulge into arterial lumen. These stenoses prevent sufficient increase in blood flow to muscles during exercise, resulting in ischemic muscle pain. |
|
|
ADH receptors:
Effects of stimulating each |
V1: Vasoconstriction and inc'd PG release
V2: Located in MEDULLARY portion of CD, allows for enhanced water permeability of principal cells |
|
|
How does the cortical segment of the CD differ from the medullary segment (functionally)?
|
Cortical segment promotes sodium reabsorption via ALDOSTERONE
Medullary segment has V2 receptors and allows reuptake of water |
|
|
22 year-old female
Acute onset abdominal pain, nausea, confusion Several episodes of abdominal pain correlating with alcohol use Urine turns dark upon standing IV dextrose immediately improves symptoms Diagnosis Pathophys Pathophys of treatment |
Patient suffers from acute intermittent porphyria
ALA synthase is rate limiting step of heme production; it is INDUCED by EtOH, barbiturates, hypoxia, griseofulvin (anything inducing P450) A deficiency of HMB synthase (Porphobilinogen-->Uroporphyrinogen) will result in an accumulation of ALA and Porphobilinogen (formed by ALA dehydratase), which are toxic to human tissues. Remember that deficiencies of early steps of heme synthesis cause neuro syx w/o photosensitivity, while derangements in latter steps cause photosensititivy. Exposure of urine to light in pts excreting large amounts of porphyrinogen results in light induced formation of porphyrins and darkening of color of urine. Treatment with high dose glucose will INHIBIT ALA synthase and decrease the amount of ALA and Porphobilinogen made. |
|
|
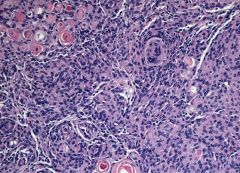
When are Psammoma bodies seen?
|
Papillary Thyroid Cancer
Serous Ovarian Adenocarcinoma Meningiomas MESOthelioma |
|
|
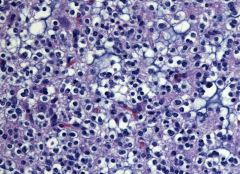
Oligodendroglioma
|
|
|
Psammoma bodies-->meningioma
|
|
|
54 year-old man
Administered unknown drug Develops flushing, diaphoresis, nausea BP 100/70, pulse 55/min Pupils constricted but reactive to light ID Drug Given Under what circumstances would you give this drug? |
Patient received a cholinergic agonist; these drugs increase GI smooth muscle tone to produce nausea, vomiting, abdominal cramps, diarrhea; also decrease heart rate, cardiac conduction and contractility, and may result in bradycardia, hypotension
Bethanechol used to stimulate peristalsis in POSTOPERATIVE ILEUS Also used to treat non-obstructive urinary retention (ATONIC BLADDER) Carbachol and pilocarpine used to lower intraocular pressure in GLAUCOMA |
|
|
Describe the steps ingested cholesterol takes to becoming bile salts.
When do gallstones occur? |
Free cholesterol-->cholic and chenodeoxycholic acids (Bile acids)
Bile acids conjugated to either glycine or taurine-->bile salts -->Secreted into bile canaliculi Phosphotidylcholine helps cholesterol become more soluble as well Circumstances for developing gallstones: -High cholesterol -Low bile acids -High phosphatidylcholine |
|
|
Key laboratory findings of DKA (relevant to pH).
|
DKA is assocd w/high anion gap metabolic acidosis accompanied by a compensatory RESPIRATORY alkalosis (will blow off CO2-)
pH = acidic Serum bicarb = LOW PaCO2 = low |
|
|
What is the most common pituitary adenoma?
|
Prolactinoma
|
|
|
Why do patients with CREST syndrome develop esophageal dysphagia?
What will be seen on barium esophagram? |
Systemic sclerosis results in excessive tissue fibrosis (hallmark of systemic sclerosis)
Esophageal dysmotility is result of atrophy and fibrous replacement of esophageal muscles. Esophageal body and LES become ATONIC and DILATED, resulting in severe reflux. Barium esophagrum will display dilated esophagus and absent peristalsis. |
|
|
Which viruses comprise the picornaviridae family?
Which are acid labile? Acid stable? |
Enteroviruses:
-Coxsackie A -Echovirus -Poliovirus -Hepatitis A virus All of the above are acid STABLE, because they are ingested and need to survive the acidic environment of the stomach. The only acid-labile of the group is RHINOVIRUS, which is inactivated by stomach acid. |
|
|
What drug must be given in combination with cisplatin?
Why? |
Cisplatin formes ROS that can cause severe nephrotoxicity.
Need to give AMIFOSTINE--a thiol-based cytoprotective free-radical scavenger used to decrease nephrotoxicity assocd w/platinum-containing agens. |
|
|
Green vs Rust-Colored Sputum:
Causes |
Green = myeloperoxidase (granules of neutrophils) in bacterial infections
Rust = blood; due to hemolysis in alveolar infection (extravasation of blood) |
|
|
Toxic Shock Syndrome:
Pathophys |
Staph aureus produces TSST-1 which acts as superantigen
ACtivates large number of helper T cells which release IL-2, and macs which release IL-1 and TNF These interleukins cause capillary leakage, circulatory collapse, hypotn, shock, fever, skin findings, and multiorgan failure |
|
|
List the 4 MAOIs.
Which is selective? |
Phenelzine
Tranylcypromine Isocarboxazid Selegiline (selective MAO-B inhibitor) |
|
|
75 year-old male
Calcification of aortic valve Cause of calcification? |
Calcification is a hallmark of cell injury and death, it occurs in ALL necrotic tissues, including fat necrosis.
Damaged cardiac valves and atheromatous plaques are calcified bc of cell death. |
|
|
43 year-old female
Presents with reduced energy, fatigue, hypocrhomic microcytic anemia Treated with iron supplementation Several weeks later, peripheral smear demonstrates enlarged RBCs that appear blue on Wright-Giemsa stain Why? |
Inc'd BM erythropoiesis results in accelerated release of immature RBCs (reticulocytes) into bloodstream.
Reticulocytes contain BLUISH cytoplasm and reticular precipitates of residual RIBOSOMAL RNA which stain blue on Wright-Giemsa stain. |
|
|
Where do H. pylori colonize?
Effects? Site of ulceration? |
H. pylori live in the mucus layer overlying the epithelium of gastric antrum and fundus
Use mucus and urease to protect themselves from stomach acid. H. pylori associated gastritis leads to a decrease in number of SMS-producing antral cells. SMS normally inhibits gastrin release; high gastrin levels cause inc'd local release of histamine, which stimulates gastric parietal cells to secrete inc'd levels of acid. Low pH gastric fluid enters duodenum and if not neutralized causes duodenal ulceration. |
|
|
Most chemical carcinogens enter the body in an inactive state (pro-carcinogens), how do they become activated?
Name the specific enzyme. |
Microsomal monooxygenase--the enzyme otherwise known as cytochrome p450.
|
|
|
Increased WBC
Peripheral smear shows immature cells (bands, metamyelocytes, myelocytes) Very few blasts Leukocyte alkaline phosphatase is low Diagnosis |
CML
|
|
|
Increased white blood cell count
Peripheral smear shows many immature cells (bands, metamyelocytes) Very few blasts Leukocyte alkaline phosphatase is elevated |
Leukemoid reaction--over-exuberant WBC response resulting from bacterial infeciton, malignancy
Neutrophil alkaline phosphatase levels will be normal OR elevated |
|
|
Increased white blood cell count
Mostly myeloblasts (>20%) |
AML
|
|
|
Increased white blood cell count
Mostly mature lymphoid cells Normal myeloid cell count |
CLL
|
|
|
t(9;22)
|
CML--Philadelphia Chromosome
|
|
|
63 year-old man
New-onset dyspnea, wheezing Facial flushing, diarrhea CT scan shows mass lesions in right live lobe and appendix Diagnosis Treatment |
Patient has carcinoid syndrome (production of 5HT)
Treat with octreotide to inhibit secretion of many hormones |
|
|
What is the effect of hyperventilation on cerebral blood flow?
|
Decreases cerebral blood flow due to lower CO2
|
|
|
Which bugs are catalase positive and pose a threat to patients with CGD?
|
Remember: pts with CGD have deficient NADPH and have very little H2O2 to work with.
Bugs are: Staph aureus (duh) Pseudomonas Aspergillus Nocardia Serratia |
|
|
Protamine is the antidote for ______.
|
Heparin
|
|
|
Aminocaproic acid is the antidote for __________.
|
Streptokinase
tPA |
|
|
12 year-old male
Ataxia Episodic erythematous and pruritic skin lesions Loose Stools Loss of neutral aromatic amino acids in urine (tryptophan) Diagnosis Treatment |
Patient has Hartnup disease (mostly asyx) but results in tryptophan wasting
Tryptophan is needed to form NIACIN--patient is presenting with syx of niacin deficiency. Give niacin! |
|
|
Non-amphetamine stimulant used in narcolepsy
|
Modafinil
|
|
|
Etanercept:
MOA Use Precautions |
Etanercept is a TNF-alpha inhibitor used to treat moderate to severe RA (esp when have failed MTX tx)
Can cause reactivation of Tb; need to have PPD before starting treatment. |
|
|
First-line treatment for high triglycerides.
|
Fibrates
|
|
|
Grows in bile AND 6.5% NaCl
VS Grows in bile but NOT 6.5% NaCl: Identify bug Associated procedures |
Grows in bile and salty water: Enterococci, E. faecium (acquired after GU procedure)
Don't grow in salty water: Strep bovis (colonic malignancy) |
|
|
Sensation between big toe and second toe.
|
Deep peroneal
|
|
|
Anti-fungals that:
Act on cell wall (glucans) Act on cell membrane (2 MOAs) Act on DNA/RNA synthesis |
Cell wall: Caspofungin; inhibit glucan synthesis
Cell membrane: Ampho B and Nystatin (both bind ergosterol); Azole (INHIBIT SYNTHESIS of ergosterol) DNA and RNA synth: Flucytosine (pyrimidine) |
|
|
Exudate vs Transudate
|
Exudate: extravasation of plasma water and plasma proteins (seen in inflammatory states)
Transudate: ultrafiltrate of plasma caused by hemodynamic changes |
|
|
Tb drug resulting in optic neuritis.
|
Ethambutol
|
|
|
Which thyroid cancer:
spindle-cells elevated serum calcitonin |
Medullary
|
|
|
Caucasian newborn
Develops abdominal distention Begins vomiting bilious fluid soon after birth Abdomen shows air fluid levels and dilatation of small bowel Laparotomy reveals inspissated green fecal mass obstructing lumen of distal ileum Diagnosis What is patient likely to die of? |
Green mass suggests distal ileum has been obstructed by dehydrated meconium.
Cystic fibrosis is most common case of meconium ileus (leads to isotonic dehydration of lumen contents) Patient likely to die of pneumonia. |
|
|
How does a strawberry hemangioma change over time?
|
First increases in size and then regresses
|
|
|
22 year-old female
Recurrent abdominal pain and anxiety Symptoms improve following IV administration of heme preparation What enzyme was inhibited? What other substance inhibits this? |
ALA synthase!
It only makes sense that lots of heme inhibits heme synthesis!!! Glucose does this too. |
|
|
44 year-old
HIV positive Pains in arms, legs Irregular, unequal pupils that respons to light, but do not constrict on accommodation Positive Romberg Deep tendon reflexes absent Diagnosis Type of organism (family) |
This is neurosyphilis, a spirochete
Areflexia and positive Romberg indicate tabes dorsalis (dorsal columns, dorsal roots)--loss os positional sense (hence cannot maintain balance with closed eyes, a positive Romberg) INvolvement of dorsal sensory roots leads to loss of pain sensation and areflexia Accommodating but non-reactive pupils are Argyll Robertson pupils |
|
|
Major causes of aortic stenosis.
|
Calcification (bicuspid aortic valve)
Rheumatic heart disease |
|
|
Sputum culture grows budding yeast that forms germ tubes at 37ºC.
Organism? |
Candida albicans--a part of normal flora (not an abnormal finding)
|
|
|
57 year-old female
Fever, chills, RUQ pain Fluid-filled cavity in right lobe of liver What is the likely organism and how did it get there? |
Likely staph aureus via hematogenous route (seeding from another site)
|
|
|
What connection between cardiac chambers is considered a variant of normal in an adult patient?
|
Patent foramen ovale--usually remains functionally closed, but any abnormality increasing RA pressure above LA pressure can produce R to L shunt.
|
|
|
Prussian blue stain:
When does something turn blue? What would this indicate if it's found in alveolar cells? |
Prussian blue stain detects intracellular iron. Iron will turn blue.
When there is increased intravascular pressures in pulmonary capillary bed, iron-containing proteins and erythrocytes are extravasated into alveoli, phag'd by macs, and converted to hemosiderin. Finding macs with hemosiderin (iron) in the alveoli indicates chronic left-sided heart failure (build up of pressure for lungs). |
|
|
34 year-old male
Brother died of liver cirrhosis Serum ferritin of 1800 µg/L What does the ferritin tell you? What is the mutation involved here? |
Ferritin = stored iron
Patient has hereditary hemochromatosis due to a mutation to the HFE gene (HLA-H). This patient will have abnormally elevated intestinal absorption. |
|
|
IgG4 antibodies to phospholipase A receptor (PLA2R)--a transmembrane protein abundant on podocytes
Diagnosis |
Membranous nephropathy--HUGE PROTEIN LOSS
|
|
|
73 year-old male
Epigastric pain that starts 30-40 minutes after meals Doesn't respond to antacids PMH significant for HTN, HLD, CABG GI endoscopy normal What's the cause? |
Generalized atherosclerosis
Involvement of intestinal arteries (bowels have diminished blood supply), pronounced after meals Often caused by atherosclerotic narrowing of the celiac trunk, SMA, and IMA Weight loss is COMMON (many pts avoid pain a/w eating) |
|
|
Babinski sign indicated damage to UMN/LMN.
|
UMN
|
|

How did this happen (basic cell processes)?
|
This shows a cystic cavity surrounded by gliosis--macroscopic appearance of an OLD CEREBRAL INFARCT (LIQUEFACTIVE NECROSIS)
Release of lysosomal enzymes from ischemic neurons results in degradation of tissue in ischemic region. Phagocytic cells migrate, remove necrotic tissue leaving a cavity, astrocytes proliferate around necrotic area with formation of a scar (Gliosis). Complete digestion of necrotic tissue w/formation of a cavity = liquefactive necrosis. |
|
|
Scrotal vs Testicular Lymph Drainage
Provide alternative names |
Lymph from scrotum-->inguinal LNs
Lymph from testes-->para-aortic AKA RETROPERITONEAL nodes |
|
|
Lung is opacified
Trachea is deviated What would cause deviation of the trachea and in which directions (relative to opaque lung)? |
Trachea deviates toward opacified lung in setting of volume loss (atelectasis)
Away from opacified lung in setting of large pleural effusion |
|
|
65 year-old smoker
CXR shows complete opacification of right lung Tracheal deviation to right |
Because this pt is a smoker, he likely has a lesion in the RIGHT MAINSTEM BRONCHUS
This prevents ventilation of right lung and results in alveolar collapse Which is why trachea shifts to right |
|
|
Why do macrosomic babies experience transient hypoglycemia?
|
Neonates of diabetic moms exposed to high maternal glucose levels in utero
Develop compensatory insulin hypersecretion (results in macrosomia) and can cause hypoglycemia NOTE THAT MATERNAL INSULIN DOES NOT CROSS PLACENTA |
|
|
Which vasodilators are specific to coronary vessels?
|
Adenosine
Dipyridamole |
|
|
What metabolic (pH status) abnormality can be better elucidated by measuring urinary Chloride?
Why? |
Metabolic alkalosis
If losing hydrogen ions form vomiting/nasogastric suction-->serum Cl- decreases and leads to decrease in urinary Cl- If due to thiazides or loop diuretics-->inc'd renal loss of Na, followed by excretion of Cl- Reabsorption of HCO3 maintains electrical neutrality |
|

What is this most likely to be?
|
Metastases to liver (multifocal) from another primary site (breast, lung, colon)
NOT hepatocellular carcinoma (that would be in someone with HBV or HCV) |
|
|
What type of diverticula (true/false) is due to pulsion?
|
Pulsion = straining (like BM)
Will form FALSE diverticulum (mucosa and submucosa only) |
|
|
What is the effect of a chronic arteriovenous shunt on cardiac output?
Why? |
Inc'd cardiact output because of inc'd sympathetic stimulation to heart, dec'd total peripheral resistance, inc'd venous return
|
|
|
What is the effect of phenylephrine infusion on cardiac output?
|
Increases sympathetic tone-->vasoconstriction, inc'd total peripheral resistance
Thus a decrease in cardiac output with no change in blood volumes or venous return |
|
|
Euchromatin vs Heterochromatin:
Which is methylated? |
Heterochromatin is methylated (low transcriptional activity)
|
|
|
Effect of histone acetylation on transcriptional activity.
|
Histone acetylation forms euchromatin with high transcriptional activity
|
|
|
Why should chest expansion be monitored in a patient with ankylosing spondylitis?
|
Inflammation of costovertabral and costosternal junctions leading to pain which can limit ches wall expansion-->hypoventilation
Other things to watch at for are uveitis, and ascending aortitis |
|
|
Describe the ion changes (concentrations) that digoxin causes in cardiac myocytes.
|
Digoxin inhibits Na-K-ATPase
This increases intracellular sodium Decreasing gradient that drives Na-Ca transporter, which leads to inc'd calcium in the cell The greater the concentration of calcium in the cell, the greater the contraction will be Remember that contraction occurs when sodium and calcium enters the cell, and potassium exits |
|
|
Organism that is gram positive and bile soluble.
|
Strep pneumo
|
|
|
Oseltamivir:
MOA (not protease inhibit) Effects on virus it acts on |
Neuraminidase inhibitor useful in treatment of influenza A and B
Neuraminidase is req'd for release of virus from infected cells and spread via respiratory tract This drug causes newly synthesized virions to adhere to host cell surface and form viral aggregates (thereby reducing spread of virus) |
|
|
Acyclovir vs Ganciclovir:
Uses |
Acyclovir is used for herpes
Ganciclovir is used for CMV (esp CMV retinitis) |
|
|
What is the most likely outcome for a patient with HCV?
|
Stable chronic hepatitis (followed closely by chronic hepatitis progressing to cirrhosis)
|
|
|
23 year-pld male
Returned from trip abroad White spots over suntanned skin KOH prep shows spaghetti and meatball appearance |
This is tinea versivolor aka pityriasis versicolor
Caused by Malassezia FURFUR |
|
|
Anti-viral causing neutropenia
|
Ganciclovir
|
|
|
Anti-viral causing bone marrow suppression
|
Zidovudine (anemia, granulocytopenia)
|
|
|
How exactly does HbS result in sickling?
|
Valine (neutral) in place of glutamic acid promotes hydrophobic interaction among hemoglobin molecules and results in polymerization of HbS molecules and RBC distortion
|
|
|
In healthy individuals, PaCO2 is the major stimulator of respiration (via central chemoreceptors).
How does this change in those with COPD? |
In prolonged hypercapnia (smokers for example), high PaCO2 ceases to stimulate respiratory drive.
Respiration is instead stimulated by hypoxia (low PaCO2) sensed by peripheral chemoreceptors. |
|
|
Needle-shaped, negatively birefringent crystals
What is their chemical composition? |
Monosodium urate (not uric acid!!!)
|
|
|
Describe the path of CSF beginning with lateral ventricles.
|
LV
Intraventricular foramen of Monro Third Ventricle Cerebral Aqueduct Fourth Ventricle Foramen of Magendie/Luschka Subarachnoid Space |
|
|
What slows the late onset of hemochromatosis in women?
|
MENSTRUATION
MENSTRUATION MENSTRUATION |
|
|
Hypoglycemia after prolonged fasting
Low ketone levels What process is failing to occur? RLS of this process? |
Impaired beta-oxidation of FAs
Acyl-CoA dehydrogenase catalyzes the first step in beta-oxidation |
|
|
What is avascular necrosis (of bone) and when does it occur?
|
Impaired blood supply to segment of bone
Femoral head is most common location Occurs most commonly due to SICKLE CELL, steroid tx, SLE, EtOH Presents with acute onset hip pain exacerbated by weight bearing No swelling, erythema, temp change |
|
|
First-line treatment of essential tremor.
|
Propanolol
|
|
|
Murmurs that diminish on squatting
|
HCM
MVP |
|
|
__________ degeneration can result in mitral valve prolapse.
|
Myxomatous (Connective Tissue) changes can result in mitral valve prolapse--thought to stretch valve leaflets
|
|
|
Which bacteria are able to undergo transformation?
What is transformation? |
SHiN bacteria can transform:
It involves uptake of chromosomal fragments from media--allows non-virulent, non-capsule forming strains to acquire genetic material that codes for capsule and thus gain virulence |
|
|
Which bacteria are able to undergo conjugation?
What is conjugation? |
Conjugation is pilus-mediated transfer of DNA
Occurs in most bacteria, but first described in E. coli |
|
|
Via what 'exchange mechanism' are bacterial able to acquire genes for virulence and antibiotic resistance?
|
Transduction--whereby a bacteriophage (Virus) transfers DNA from one bacterium to another.
|
|
|
Rhomboid crystals with weak positive birefringence
Extracted from knee |
THis is calcium PYROPHOSPHATE
Not calcium oxalate; calcium oxalate occurs in renal calculi |
|
|
Amyloid deposition isolated to a single organ doesn't necessarily form from beta-amyloid protein.
Name the precursors to amyloid formation for: Cardiac Atria Thyroid Pancreatic Islets Cerebrum/Cerebral vessels Pituitary Gland |
Cardiac atria: ANP
Thyroid gland: Calcitonin Pancreatic islets: islet amyloid protein (amylin) Cerebrum/cerebral blood vessels: beta-amyloid protein Pituitary gland: Prolactin |
|
|
Bluish neoplasm under nail bed:
Differential |
Glomangioma (tumor of glombus body--responsible for shunting blood away from skin surfaces in cold temperatures to prevent heat loss)
Melanoma (function of pigmentation) |
|
|
Recent-onset oliguria
Elevated serum creatinine Intranasal ulcer failing to heal Sinusitis, hemoptysis Diagnosis |
This is Wegener's granulomatosis (with polyangitis)
Disease is associated with C-ANCAs (antibodies targeting neutrophils!) |
|
|
21 year-old male
recurrent kidney stones Sodium cyanide added to urine following sodium nitroprusside and urine turns red-purple What is going on in this patient? |
Sodium cyanide-nitroprusside test detects cystine's sulfhydryl groups
He is peeing out cysteine (aminoaciduria)--results in recurrent stone formation from a young age |