Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
62 Cards in this Set
- Front
- Back
|
Where are nicotinic receptors found?
What drugs block these receptors? |
Neuromuscular jn (skeletal muscle)
And postganglionic neurons of symp/psymp Curare drugs--ex: tubocurarine |
|
|
52 year-old woman
Episodic loss of urine Can't make it to the bathroom before urinating on self Detrusor instability Diagnosis Treatment |
Urge incontinence (overactive bladder) due to uninhibited bladder contractions (detrusor instability)
Treat with antimuscarinic drug targeting M3 receptors. Ex: oxybutynin Be careful bc these drugs may cause confusion in the elderly (antimusc AEs) |
|
|
20 year-old woman
Small, underdeveloped ovaries Ovaries consist of connective tissue with no follicles present |
Streak ovaries (Turner's)
|
|
|
HLA Class I vs II Serotypes (examples)
|
HLA Class I: HLA B27
HLA Class II: DR, DP, DQ |
|
|
What disorders comprise the seronegative spondylopathies?
Which HLA class predisposes patients to developing them? |
Seronegative spondylopathies include:
Reactive Arthritis (Reiter syndrome) Ankylosing spondylitis Psoriatic arthritis Arthritis associated with bowel disease Individuals expressing HLA B28 are at inc'd risk of seronegative spondyloarthropathies. |
|
|
S-100 Tumors
|
Schwannomas
Melanomas (both melanocytes and Schwann cells are derived from NCC) |
|
|
Which cranial nerves can develop Schwannomas?
Which can't? Why not? |
All cranial nerves except CN II can develop schwannomas because they are covered by Schwann cells (and thus are considered PNS).
CN II is covered by oligodendrocytes and cannot develop a schwannoma. Note: the most common site of intracranial schwannomas is the cerebellopontine angle at CN VIII (acoustic neuromas). |
|
|
43 year-old male
Advanced HIV Develops impaired vision Diagnosis |
CMV-induced retinitis
|
|
|
This anti-viral is associated with nephropathy and neurotoxicity (delirium/tremor).
|
Acyclivor
|
|
|
This anti-viral is associated with severe neturopenia.
|
Ganciclovir
|
|
|
This anti-viral is associated with renal wasting leading to low Mg2+ and decreased release of PTH leading to low Ca2+.
|
Foscarnet
|
|
|
This anti-viral causes fat redistribution, hyperglycemia, and hypertriglyceridemia.
|
Protease inhibitors
|
|
|
Define myocardial stunning.
|
Brief ischemic episodes (<30 mins) followed by reperfusion allows for full recovery--usually over hours to days.
|
|
|
Define myocardial hibernation.
|
Repetitive ischemia of cardiac myocytes or persistent hypoperfusion results in chronic but reversible loss of contractile function, referred to as hibernation.
Reversed by resvascularization with CABG or balloon angioplasty. Time course of function recovery is variable, occurring within hours to months. |
|
|
Define ventricular remodeling.
|
Chronic changes in mass, volume, shape, myocyte composition of heart, to compensate for INCREASED hemodynamic load.
|
|
|
32 year-old female
Persistent diarrhea Tea-colored, odorless stool No response to dietary modification, even despite 2 day fast Total lack of gastric acid secretion in stomach Diagnosis Pathophys Treatment |
VIPoma: pancreatic islet cell tumor that causes excess VIP secretion resulting in WDHA (Watery Diarrhea, Hypokalemia, Achlorhydria) syndrome.
Does this because VIP inhibits H+ secretion and stimulates pancreatic HCO3 and Cl- secretion. Tx: Octreotide to decrease production of all GI hormones (VIP included) |
|
|
46 year-old female
Right-sided flank plain s/p surgery for cervical cancer Palpable mass deep in RUQ Diagnosis Pathophys |
Hydronephrosis--ureters are at risk of injury during pelvic surgeries
Hysterectomies especially risky bc ureters course posterior to uterine arteries, which are ligated in this procedure. Ligating the ureters would allow the kidneys to continue developing urine, but urine would get backed up (causing hydronephrosis). |
|
|
65 year-old smoker
Dyspnea, cough CXR demonstrates mass in RUL Elevated serum calcium Bone Scan negative Diagnosis Pathophys |
Squamous cell carcinoma producing PTHrP (PTH related protein)--acts similarly to PTH although degree of hypercalcemia is higher with PTHrP produciton than in primary hypereparathyroidism.
This phenomenon is known as humoral hypercalcemia of malignancy. |
|
|
Where does the majority of free water reabsoprtion in the nephron occur REGARDLESS OF HYDRATION STATUS?
|
Proximal tubule (absorbs more than 60% of fluid filtered!)
|
|
|
22 year-old male
Episodic burning neuropathy in extremities Non-blanching macules between umbilicus and knees Diagnosis Pathophys Disease sequelae |
Fabry disease due to inherited deficiency of ALPHA-GALACTOSIDASE A
In patients with this deficiency there is an accumulaiton of CERAMIDE TRIHEXOSIDE in tissues. Without enzyme replacement tx, progressive renal insufficiency will lead to RENAL FAILURE and death. Note: presentation-- -acroparesthesia (episodic, debilitating, burning neuropathic pain in extremities) -angiokeratomas: punctuate, dark red, non-blanching macules and papules that occur between umbilicus and knees |
|
|
PaO2 Normal
SaO2 Decreased Oxygen content Low Diagnosis |
CO poisoning (CO competes with O2 and thus decreases perent saturation of Hgb)
O2 content - both dissolved and O2 attached to Hgb so much be decreased if PO2 is normal |
|
|
PaO2 Normal
SaO2 Normal O2 Content Decreased Diagnosis |
Anemia (low Hgb)--can be due to chronic blood loss
|
|
|
PaO2 Normal
SaO2 Normal O2 Content Increased Diagnosis |
Polycythemia (high Hgb)
|
|
|
Equation for resistance.
|
R = nL/(r^4)
Where n = viscosity of blood L = length of vessel r = radius of vessel |
|
|
Protein in signal transduction contains several alpha-helical regions consisting of valine, alanine, isoleucine.
Function of protein? |
Non-polar, hydrophobic amino acids such as valine, alanine, isoleucine, methionine, and phenylalanine are generally located interiorly on globular proteins, where they're shielded from direct contact with water.
Thus these proteins act to form the portion of a receptor that spans the phospholipid bilayer ('transmembrane domain') |
|
|
S. pneumoniae:
Virulence factor |
Capsular polysaccharide that inhibits phagocytosis by macrophages and polymorphonuclear leukocytes
|
|
|
What are the 5 general characteristics of DNA viruses?
Exceptions? |
All DNA viruses:
1. Are HHAPPPPy viruses: Hepadna, Herpes, Adeno, Pox, Parvo, Papilloma, Polyoma 2. Are double stranded EXCEPT parvo (single-stranded) 3. are linear--EXCEPT paiplloma, polyoma (circular, supercoiled); EXCEPT hepadna (circular, incomplete) 4. Are icosahedral (EXCEPT pox--complex) 5. Replicate in nucleus--EXCEPT pos (carries own DNA-dependent RNA polymerase) |
|
|
Where do DNA viruses replicated?
|
All replicate in nucleus (except poxvirus)
|
|
|
What are the characteristics of RNA viruses?
Exceptions? |
All RNA viruses are ssRNA, except Reovirus and Rotavirus (dsRNA)
Positive-stranded: I went to a RETRO (retrovirus) TOGA (togavirus) party, where I drank FLAVored (flavivirus) CORONA (coronavirus) and ate HIPPY (hepevirus) CALIFORNIA (calicivirus) PICKLES (picornavirus) |
|
|
Where do RNA viruses replicate?
|
All replicate in cytoplasm (except influenza and retrovirus)
|
|
|
Which viruses are naked (nonenveloped)?
|
Naked CPRR and a PAPP smear
Calicivirus Picornavirus Reovirus Rhinovirus Parvovirus Adenovirus Papilloma Polyoma |
|
|
Where do enveloped viruses acquire their envelopes?
|
From plasma membrane, except herpesvirus (nuclear membrane)
|
|
|
Which DNA viruses are enveloped?
|
Herpesviruses (HSV, VZV, CMV, EBV)
HBV Smallpox |
|
|
Which DNA viruses are nucleocapsid viruses?
|
Adenovirus
Papillomavirus Parvovirus |
|
|
Which RNA viruses are enveloped?
|
Influenza
Parainfluenza RSV Measles, Mumps, Rubella Rabies HIV |
|
|
Which RNA viruses are nucleocapsid viruses?
|
Enteroviruses (polio, coxsackie, echo, HAV)
Rhinovirus Reovirus (rotavirus) |
|
|
What characteristics must a naked RNA virus have to act directly as mRNA using the host's intracellular machinery for translation?
|
Must be single-stranded and positive sense.
CANNOT BE double-stranded or negative sense. |
|
5 year-old male
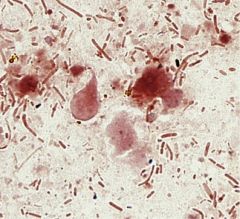
Recurrent diarrhea that does not respond to short-term antibiotics Stool sample below Diagnosis Pathophys |
Giardia lamblia causes injury to duodenal and jejunal mucosa by adhering to intestinal brush border and releasing molecules that induce a mucosal inflammatory response.
Secretory IgA, which impairs adherence, is a major component of adaptive immunity against G. lamblia infection. Patients deficiency in IgA antibodies against Giardia antigens are prone to chronic giardiasis. |
|

57 year-old died in car on way to ER 30 minutes after onset of chest pain
ho HTN, DM, HLD Cross-section of LAD shown Diagnosis Pathophys |
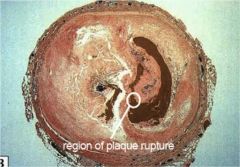
Sudden Cardiac Death:
Ruptured plaque with superimposed thrombus. Resulted in cardiac arrest within 1 hr of precipitating event. Ischemia produces electrical instability in heart and generates LETHAL ARRHYTHMIA (V FIB) Note: extensive MI may result in ventricular dysfunction, however, death due to heart failure caused by MI does not occur suddenly. Ventricular failures is most common cause of death due to MI during in-hospital phase. |
|
|
50 year-old female
h/o radical mastectomy Persistent right arm swelling Increased risk of developing _________. |
Persistent lymphedema (with chronic dilation of lymphatic channels) predisposes patients to develop LYMPHANGIOSARCOMA (rare malignant neoplasm of endothelial lining of lymphatic channels)
Typical scenario would be appearance of lymphangiosarcoma approximately 10 years following radical mastectomy for breast cancer |
|
|
31 year-old male
Farm worker Itchy rash on chest Annular and scaling plaque KOH prep shows branching septate hyphae Diagnosis Treatment Treatment MOA |
Patient presenting with symptoms of tinea corporis (annular scaling plaque w/well-demarcated, raised erythematous borders/central clearing)
Terbinafine used for tx of dermatophytosis. MOA: Inhibits synthesis of ergosterol by INHIBITING SQUALENE EXPOSIDASE |
|
|
This anti-fungal binds to ergosterol.
|
Amphotericin B
Nystatin |
|
|
IV anesthetic agent used in patient undergoing minor surgical repair.
30 minutes after administration, patient is alert and responsive. How did he recover so quickly? |
Accumulation of thiopental and other related lipid soluble barbiturates in brain followed by rapid redistribution into skeletal muscles and adipose tissue (within 5-10 min).
Awakening occurs because plasma level rapidly declines due to REDISTRIBUTION of drug to OTHER TISSUES throughout body (lean tissue). This rapid brain clearance leads to recovery from anesthesia. |
|
|
35 year-old male
RIght knee pain and swelling Cultures of joint aspirate reveal no bacteria Diarrheal illness 2 weeks ago Diagnosis |
Reactive arthritis
|
|
|
A reaction in which A is converted to B has a standard free energy change Gº = +430 cal/mol. This reaction is catalyzed by enzyme X.
A solution containing 1 mol/L of A and 1 mol/L of B is allowed to sit with enzyme B. What will happen? |
Since deltaGº is positive, products are of higher energy state than substrates.
So if add an enzyme, will form more of substrates. |
|
|
Which anticholinesterase can penetrate the CNS?
|
Physostigmine
(others, i.e., neostigmine and edrophonium, can't!) |
|
|
67 year-old male
Alcoholism Leg edema, rash Cognitive changes Multiple vitamin deficiencies Diagnosis Pathophys |
Pellagra due to niacin deficiency: dermatitis, diarrhea, dementia
Dermatitis usually b/l and symmetric on sun-exposed areas of body, consisting of roughened, thickened, scaly skin Diarrhea due to columnar epithelium atrophy of GI tract Dementatia due to neuronal degeneration of brain/SC |
|
|
Niacin:
Sources in diet Physiologic role |
Can either be ingested as vitamin or synthesized from tryptophan
Niacin is an essential component of NAD and NADP (accepts electrons and donates hydrogen ions!) Note: populations that consume corn (where niacin is bound and unabsorbable) often have pellagra |
|
|
Tissue plasminogen activator vs Streptokinae:
MOA (similarities and differences) Uses Contraindications |
Both are thrombolytics and increase clot lysis by increasing formation of plasmin from plasminogen
tPA is fibrin specific streptokinase is non-firbin specific (in theory, fibrin-specific fibrinolytics assocd w/less systemic activation) Use: Acute MI Contraindicated in hemorrhagic stroke, ischemic stroke within one year, active internal bleeding, BP >180/110, suspected dissecting aneurysm |
|
|
28 year-old woman
RLQ pain, vaginal bleeding Menstrual period 7 weeks ago h/o pelvic inflammatory disease BP 80/40, pulse 130 Pale, clammy Diagnosis Histologic findings |
Patient likely presenting with ruptured ectopic pregnancy secondary to PID.
Endometrial biopsy would reveal DECIDUAL (GESTATIONAL) changes in endometrium but no chorionic villi. |
|
|
Colon cancer:
Right vs Left Sided Presentation |
Right-sided cancer (ascending colon) tends to present with syx of iron deficiency anemia and systemic syx
Patients with left-sided colon cancer manifest as partial intestinal obstruction. |
|
|
Classic appearance of PSGN on microscopy.
|
LUMPY BUMPY HUMPS
LUMPY BUMPY HUMPS LUMPY BUMPY HUMPS |
|
|
Lumpy bumpy appearance of mesnaium:
Contents |
Granular deposits of IgG, IgM, C3 (immune complexes)
|
|
|
What drugs cause fat distribution from extremities to the trunk?
|
Glucocorticoids
HAART therapy (highly active antiretroviral tx) due to HIV-1 protease inhibitors Fat also depsoits to thorax, posterior neck (BUFFALO HUMP), and supraclavicular region |
|
|
How exactly dow TZDs decrease insulin resistance?
|
Bind PPAR-gamma to increase transcription of ADIPONECTIN (adiponectin levels are low in DM II) which affects glucose/lipid metabolism.
|
|
|
7 year-old boy
Colicky abdominal pain with bloody stools Urine appeared red Palpable skin lesions on buttocks Diagnosis Pathophys Other symptoms |
Henoch-Schönlein Purpura!!
Small vessel vasculitis in children Usually occurs few weeks after illness Antigen from infection likely produces IgA ab's and IgA-containing immune complexes deposit on vessel walls, inducing inflammatory reaction. Syx: GI: vasculitis within GI tract-->GI bleeds Kidney: identical to Berger disease-->IgA nephropathy; CRESCENT formation Skin: palpable purpura Joints: ARTHRALGIAS, esp. ankle and knee joints |
|
|
10 year-old male
Exertional dyspnea, fatigability Toe cyanosis, clubbing No finger abnormalities Diagnosis |
Differential cyanosis--cyanosis of lower extremities but not of upper body; it's the result of reduced arterial oxygen saturation in distal aorta
Most likely cause of R to L shunting of blood flow would be PATENT DUCTUS ARTERIOSUS (not VSD!!!) PDAs act similarly to VSDs; initially begin as LtoR and aren't a problem, until later in life when they're RtoL. Note: if this presentation were in an ADULT, it would likely be AORTIC COARCTATION |
|
|
What physiologic conditions would minimize the infective dose of V. cholerae?
|
Anything decreasing acidity of stomach (cholera likes alkaline media): Achlorhydria, food ingestion, antacid ingetion
|
|
|
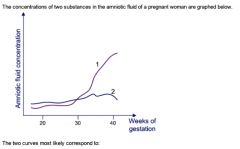
Curve 1 is phosphatidylcholine, aka LECITHIN (know both of these!!!)
Curve 2 is sphingomyelin (derp) |
|
|
How do the following organs response to minimal change disease?
Kidneys Liver |
Due to loss of protein, there's a dorp in colloid osmotic pressure in the blood; as a result fluid moves into the interstitial tissue and edema occurs.
Kidneys detect drop in fluid levels and release renin; this causes sodium and fluid retention, thus exacerbating the edema. Liver cannot compensate for amount of albumin loss so begins synthesizing as many proteins (doesn't matter what kind) as it can--VLDL, TG, cholesterol, lipoproteins, etc. |
|
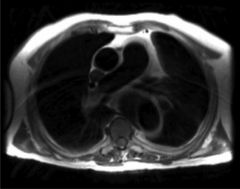
Diagnosis
Pathophys Risk factors |
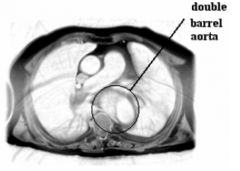
"Double barrel aorta"--this apparent second cavity is really an intramural hematoma.
Aortic dissections give rise to hematomas as more nad more blood creeps behind medial wall. Intimal tear thought to be primary event. Single most important risk factor for dev't of intimal tears leading to aortic dissections is HYPERTENSION. |
|
|
What vascular risks does smoking pose?
|
ATHEROSCLEROSIS-->aneursym
Not dissection! |