Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
987 Cards in this Set
- Front
- Back
|
Name the first eight abdominal layers, from most superficial to deepest.
|
skin, superficial fascia, external oblique muscle, internal oblique muscle, transversus abdominis muscle, transversalis fascia, extraperitoneal tissue, peritoneum
|
|
|
True or False: The transversus abdominus muscle runs superficial to the internal oblique muscle.
|
False; the internnal oblique is superficial to the transversus abdominus muscle
|
|
|
What two blood vessels and one nerve run along the spine at the level of the umbilicus?
|
Aorta, Inferior vena Cava (IVC) and sympathetic trunk run together along the spine
|
|
|
True or False: The latissimus dorsi is more superficial than the quadratus lumborum.
|
true
|
|
|
True or False: The transversalis fascia runs superficially to the transversus abdominis muscle.
|
False; the fascia runs deep to the muscle
|
|
|
True or False: The rectus sheath wraps around the outside of the rectus abdominis.
|
true
|
|
|
What is the most superficial muscle group making up the lateral abdominal wall?
|
external abdominal oblique muscle
|
|
|
What is the deepest muscle group making up the lateral abdominal wall?
|
transversus abdominis muscle
|
|
|
What lies between the bilateral rectus abdominis muscles, formed by the rectus sheath?
|
linea alba
|
|
|
Which parts of the duodenum are retroperitoneal?
|
2nd, 3rd and 4th parts of the duodenum
|
|
|
Name two major organs that lie completely in the retroperitoneal space.
|
kidneys and adrenal glands
|
|
|
What part of the pancreas is not found in the retroperitoneal space?
|
the pancreatic tail
|
|
|
True or False: The rectum lies in the retroperitoneal space.
|
true
|
|
|
True or False: The psoas muscles runs in the retroperitoneal space.
|
true
|
|
|
Which two parts of the urinary system are retroperitoneal?
|
kidneys and ureters
|
|
|
Which parts of the colon are found in the retroperitoneal space?
|
ascending (right) and descending (left) colon
|
|
|
What 2 major blood vessels run in the retroperitoneal space?
|
aorta and IVC
|
|
|
In the gastrointestinal tract, the falciform ligament connects which two structures?
|
liver to anterior abdominal wall
|
|
|
In the gastrointestinal tract, the hepatoduodenal ligament connects which two structures?
|
liver and duodenum
|
|
|
In the gastrointestinal tract, the gastrohepatic ligament connects which two structures?
|
the liver and the lesser curvature (superior part) of the stomach
|
|
|
In the gastrointestinal tract, the gastrocolic ligament connects which two structures?
|
the greater curvature of the stomach (inferior part) and the transverse colon
|
|
|
In the gastrointestinal tract, the gastrosplenic ligament connects which two structures?
|
the greater curvature of the stomach and the spleen
|
|
|
In the gastrointestinal tract, the splenorenal ligament connects which two structures?
|
the spleen and the posterior abdominal wall
|
|
|
The _____ ligament connects the liver and the abdominal wall.
|
falciform
|
|
|
The _____ ligament connects the liver and the duodenum.
|
hepatoduodenal
|
|
|
The _____ ligament connects the liver and the lesser curvature of the stomach.
|
gastrohepatic
|
|
|
The _____ ligament connects the transverse colon and the greater curvature of the stomach.
|
gastrocolic
|
|
|
The _____ ligament connects the spleen and the greater curvature of the stomach.
|
gastrosplenic
|
|
|
The _____ ligament connects the spleen and the posterior abdominal wall.
|
splenorenal
|
|
|
The falciform ligament contains what structure?
|
ligamentum teres (derivative of the fetal umbilical vein)
|
|
|
The hepatoduodenal ligament contains what structures?
|
the portal triad (hepatic artery, portal vein, and common bile duct)
|
|
|
The gastrohepatic ligament contains what structures?
|
the gastric arteries (right and left)
|
|
|
The gastrocolic ligament contains what structures?
|
the gastroepiploic arteries (right and left)
|
|
|
The splenorenal ligament contains what structures?
|
splenic artery and vein
|
|
|
The _____ ligament contains the ligamentum teres.
|
falciform
|
|
|
The _____ ligament contains the portal triad (the portal vein, the portal artery, and the common bile duct).
|
hepatoduodenal
|
|
|
The _____ ligament contains the gastric arteries.
|
gastrohepatic
|
|
|
The _____ ligament contains the gastroepiploic arteries.
|
gastrocolic
|
|
|
The _____ ligament contains the splenic artery and the splenic vein.
|
splenorenal
|
|
|
Name the ligament in the gastrointestional tract which is dervived from the fetal umbilical vein.
|
falciform ligament
|
|
|
The portal triad can be compressed through what opening to control bleeding?
|
omental foramen (also known as the epiploic foramen of Winslow)-opening into the lesser sac
|
|
|
What gastrointestinal ligament can be cut to access the lesser sac during surgery?
|
gastroheptic ligament
|
|
|
True or false: The gastrocolic ligament is part of the greater omentum.
|
true
|
|
|
The gastrosplenic ligament separates what two structures?
|
left greater and lesser sacs
|
|
|
the gastrohepatic ligament separates what 2 structures?
|
right greater and lesser sacs
|
|
|
What structure attaches the digestive tract to the abdominal wall?
|
mesentery
|
|
|
Which layer of the muscularis externa is closer to the lumen: the circular layer or the longitudinal layer?
|
the circular layer is the inner layer of muscle within the muscularis externa
|
|
|
What is the innermost layer of the gut wall called?
|
the mucosa
|
|
|
What is the outermost layer of the gut wall called?
|
serosa/adventitia
|
|
|
In the gut wall, the submucosa is found between what two layers?
|
mucosa and muscularis externa
|
|
|
List three components of the gut wall mucosa.
|
epithelium (absorption), lamina propria (support), muscularis mucosa (motility)
|
|
|
What is the primary function of the epithelium of the gut wall mucosa?
|
absorption
|
|
|
What is the primary function of the lamina propria of the gut wall mucosa?
|
support
|
|
|
What is the primary function of the muscularis mucosa of the gut wall mucosa?
|
mucosal motility
|
|
|
What structure is found within the submucosa of the gut wall?
|
the submucosal nerve plexus (Meissner's plexus)
|
|
|
Meissner's plexus controls what three functions of the submucosal gut wall?
|
secretions, blood flow, absorption
|
|
|
What are the two main components of the muscularis externa?
|
inner circular layer and outer longitudinal layer
|
|
|
What lies between the inner circular and outer longitudinal layers of the muscularis externa?
|
Myenteric nerve plexus (Auerbach's plexus)- responsible for GI motility
|
|
|
List the four main layers of the gut wall, starting from the inside and going out.
|
mucosa--> submucosa--> muscularis externa--> serosa/adventitia
|
|
|
True or false: The rate of basal electrical rhythm in the stomach is 9 waves/minute.
|
False; the rate of slow waves in the stomach is 3 waves/min
|
|
|
What is the rate of basal electrical rhythm in the duodenum?
|
12 waves/min
|
|
|
What is the rate of basal electrical rhythm in the ileum?
|
8-9 waves/min
|
|
|
Villi are found in which section of the digestive tract?
|
small intestine (duodenum, jejunum, ileum)
|
|
|
The primary function of the myenteric plexus is to coordinate what function?
|
motility
|
|
|
In what portion of the gut does the myenteric plexus coordinate motility?
|
along the entire gut wall
|
|
|
What is another name for the myenteric nerve plexus?
|
Auerbach's plexus
|
|
|
Do the myenteric and submucosal plexuses contains cell bodies of sympathetic or parasympathetic terminal effector neurons?
|
parasympathetic (remember rest and DIGEST)
|
|
|
The myenteric plexus is located between what two smooth muscle layers?
|
The inner circular layer and the outer longitudinal layer; recall AUerbach's is on the AUtside (more outside than Meissner's plexus)
|
|
|
True or False: The myenteric nerve plexus contains cell bodies of some parasympathetic terminal effector neuons.
|
true
|
|
|
True or False: Absorption in the gut is an example of a process that is regulated by the submucosal nerve plexus.
|
true
|
|
|
True or False: Gut wall motility is an example of a process that is regulated by the submucosal nerve plexus.
|
False; it is regulated by the myenteric nerve plexus (of Auerbach)
|
|
|
True or False: Local secretion is an example of a process that is regulated by the submucosal nerve plexus.
|
true
|
|
|
True or False: Blood flow is an example of a process that is regulated by the submucosal nerve plexus.
|
true
|
|
|
What is another name for the submucosal nerve plexus?
|
Meissner's plexus
|
|
|
The submucosal plexus is located between what two layers?
|
mucosa and inner circular smooth muscle layer of the muscularis externa
|
|
|
The upper one-third of the esophagus is composed of _____ muscle.
|
striated
|
|
|
The lower one-third of the esophagus is composed of ______ muscle.
|
smooth
|
|
|
True or False: The middle one-third of the esophagus is composed only of striated muscle.
|
False; the middle one-third of the esophagus is composed of both smooth and striated muscle
|
|
|
At what spinal level does the celiac trunk branch off the aorta?
|
T12
|
|
|
At what spinal level does the superior mesenteric artery branch off the aorta?
|
T1
|
|
|
At what spinal level does the inferior mesenteric artery branch off the aorta?
|
L3
|
|
|
At what spinal level does the left renal artery branch off the aorta?
|
L1
|
|
|
At what spinal level do the testicular or ovarian arteries branch off the aorta?
|
L2
|
|
|
What spinal level does the aorta bifurcation occur at?
|
L4
|
|
|
What is the parasympathetic innervation for the stomach?
|
vagus nerve (CN X)
|
|
|
What is the parasympathetic innervation for the proximal two-thirds of the transverse colon?
|
vagus nerve (CN X) (midgut)
|
|
|
What is the parasympathetic innervation for the distal one-third of transverse colon and the upper portion of the rectum?
|
pelvic parasympathetic nerve (hindgut)- L3
|
|
|
True or False: The vagus nerve innervates structures at the L3 vertebral level.
|
False; the L3 vertebral level is innervated by the pelvic parasympathetics
|
|
|
True or False: The vagus nerve innervates structures at the L1 vertebral level.
|
true (this corresponds to midgut)
|
|
|
True or False: The vagus nerve innervates structures at the T12/L1 vertebral level.
|
True; this corresponds to foregut
|
|
|
Pelvic parasympathetics innervate the gastrointestinal region supplied by which artery?
|
inferior mesenteric artery (hindgut)
|
|
|
What is the parasympathetic innervation for the liver, gallbladder and pancreas?
|
vagus nerve (CNX)
|
|
|
The splenic flexure of the colon is a watershed area between the bloodflow from which two arteries?
|
superior mesenteric artery and inferior mesenteric artery (midgut and hindgut)
|
|
|
What are the three main arteries that supply the gastrointestinal tract?
|
The celiac trunk, superior mesenteric artery, and inferior mesenteric artery
|
|
|
What are the three embryologic divisions of the gastrointestinal tract?
|
The foregut, midgut, and hindgut
|
|
|
What embryologic division of the gastrointestinal tract is supplied by the celiac trunk?
|
foregut
|
|
|
What artery supplies the midgut?
|
SMA
|
|
|
What embryologic division of the gastrointestinal tract is supplied by the inferior mesenteric artery?
|
hindgut
|
|
|
What are the main gastrointestinal structures derived from the foregut?
|
stomach, liver, gallbladder, pancreas, proximal duodenum up until the ampulla of vater
|
|
|
What main artery supplies the stomach to the proximal duodenum, liver, gallbladder, and pancreas?
|
celiac trunk
|
|
|
What portion of the gastrointestinal tract is derived from the midgut?
|
distal duodenum (from ampulla of vater) through proximal 2/3 of transverse colon
|
|
|
What main artery supplies the midgut?
|
superior mesenteric artery
|
|
|
What portion of the gastrointestinal tract is derived from the hindgut?
|
distal 1/3 of transverse colon to rectum above the pectinate line
|
|
|
What main artery supplies the hindgut?
|
inferior mesenteric artery
|
|
|
The stomach receives its main blood supply from branches of what structure?
|
the celiac trunk
|
|
|
Name the three branches of the celiac trunk.
|
common hepatic artery, splenic artery and left gastric artery (lesser curvature of stomach)
|
|
|
What are the two branches of the proper hepatic artery?
|
left and right hepatic arteries
|
|
|
True or False: The cystic artery is a branch of the hepatic artery proper.
|
False; the cystic artery branches off of the right hepatic artery, a branch of the hepatic artery proper
|
|
|
What are the two branches of the gastroduodenal artery?
|
Superior pancreaticoduodenal and right gastroepiploic arteries
|
|
|
True or False: The right and left gastroepiploic arteries anastamose along the lesser margin of the stomach.
|
False; they anastamose along the greater curvature/margin of the stomach
|
|
|
The short gastric arteries have poor anastomoses if the _____ artery is blocked.
|
splenic
|
|
|
Strong anastomoses exist between what two sets of arteries of the celiac trunk?
|
Left and right gastroepiploics and left and right gastrics
|
|
|
The internal thoracic/mammary (subclavian) can anastamose with the inferior epigastric (external iliac) via what arterial connection?
|
Superior epigastric (internal thoracic)
|
|
|
If the abdominal aorta is blocked, the superior pancreaticoduodenal (celiac trunk) artery can anastamose with what vessel?
|
Inferior pancreaticoduodenal artery (SMA)
|
|
|
If the abdominal aorta is blocked, which artery can anastamose with the left colic artery (IMA)?
|
Middle colic artery (SMA)
|
|
|
The superior rectal artery (IMA) can anastamose with what artery?
|
Middle rectal artery (internal iliac)
|
|
|
True or False: The superior pancreaticoduodenal artery comes off of the superior mesenteric artery to anastomose with the inferior pancreaticoduodenal artery.
|
False; the superior pancreaticoduodenal artery branches off of the celiac trunk to anastomose with the inferior pancreaticoduodenal artery (which branches off of the SMA)
|
|
|
If the abdominal aorta is blocked, there are several anastomoses that will provide collateral flow. Complete this one: _____ _____ (from the subclavian) to the superior epigastric (internal thoracic) to the inferior epigastric (normally fed by the external iliac).
|
internal mammary
|
|
|
If the abdominal aorta is blocked, there are several anastomoses that will provide collateral flow. Complete this one: internal mammary (from the subclavian) to the _____ _____ (internal thoracic) to the inferior epigastric (normally fed by the external iliac).
|
superior epigastric
|
|
|
If the abdominal aorta is blocked, there are several anastomoses that will provide collateral flow. Complete this one: internal mammary (from the subclavian) to the superior epigastric (internal thoracic) to the _____ _____ (normally fed by the external iliac).
|
inferior epigastric
|
|
|
If the abdominal aorta is blocked, there are several anastomoses that will provide collateral flow. Complete this one: _____ _____ (from the celiac trunk) to the inferior pancreaticoduodenal (normally fed by the superior mesenteric artery).
|
superior pancreaticoduodenal
|
|
|
If the abdominal aorta is blocked, there are several anastomoses that will provide collateral flow. Complete this one: superior pancreaticoduodenal (from the celiac trunk) to the _____ _____ (normally fed by the superior mesenteric artery).
|
inferior pancreaticoduodenal
|
|
|
If the abdominal aorta is blocked, there are several anastomoses that will provide collateral flow. Complete this one: _____ _____ (from the inferior mesenteric artery) to the middle rectal (normally fed by the internal iliac).
|
superior rectal
|
|
|
Give three examples of clinical manifestations of portosystemic anastomoses.
|
Esophageal varices, internal hemorrhoids, and caput medusae; (remember: gut, butt and caput
|
|
|
Portosystemic anastomoses from the left gastric vein to the esophageal vein can manifest as what?
|
esophageal varices
|
|
|
A patient with portal hypertension presents with discomfort on defecation and bright red blood per rectum. Physical examination shows prolapsed dilated veins around the anus that are not tender. What is the explanation of these findings?
|
A portosystemic anastomoses between the superior and middle rectal arteries created internal hemorrhoids, which are painless
|
|
|
Portal-systemic anastomoses from the paraumbilical vein to the inferior epigastric and superior episgastric veins can manifest as what?
|
caput medusa at the navel
|
|
|
What condition is a common cause of portal-systemic anastomoses?
|
portal hypertension
|
|
|
Esophageal varices result from anastomoses between the _______ vein and the _______ vein.
|
left gastric; esophageal
|
|
|
Caput medusae results from anastomoses between the ____ vein and ____/_____ veins.
|
paraumbilical; superior/inferior epigastric veins
|
|
|
Hemorrhoids result from anastomoses between the ______ vein and _____ and _____ veins.
|
superior rectal; middle rectal and inferior rectal
|
|
|
Portocaval shunt placement between the ______ _____ and ______ _____ veins relieves portal hypertension by shunting blood from the ______ circulation to the ______ circulation.
|
splenic vein; left renal; portal; systemic
|
|
|
The pectinate line is formed where the embyonic _____ derivatives meet the _____ derivatives.
|
hindgut; ectodermal
|
|
|
What type of hemorrhoids occur above the pectinate line?
|
internal hemorrhoids (painless)
|
|
|
Which type of hemorrhoids are not painful?
|
internal hemorrhoids (above the pectinate line)
|
|
|
What type of cancer occurs above the pectinate line in the rectum?
|
adenocarcinoma
|
|
|
Above the pectinate line, there is what type of innervation: visceral or somatic?
|
visceral innervation; thus internal hemorrhoids are NOT painful
|
|
|
Above the pectinate line, the arterial supply comes from what artery?
|
superior rectal artery (a branch of the IMA)
|
|
|
The superior rectal artery is a branch of what artery?
|
inferior mesenteric artery (IMA)
|
|
|
Venous drainage above the pectinate line is from the _____ _____ vein to the _____ _____ vein to the _____ _____.
|
superior rectal; inferior mesenteric; portal vein
|
|
|
What type of hemorrhoids receive visceral innervation?
|
internal hemorrhoids (thus they are NOT painful)
|
|
|
What type of hemorrhoids can occur below the pectinate line?
|
external hemorrhoids (painful)
|
|
|
Which type of hemorrhoids are painful?
|
external hemorrhoids
|
|
|
What type of cancer occurs below the pectinate line?
|
squamous cell carcinoma
|
|
|
Below the pectinate line, there is what type of innervation, somatic or visceral?
|
somatic (thus external hemorrhoids are painful)
|
|
|
Below the pectinate line, the arterial supply is from what artery?
|
inferior rectal artery (branch of the internal pudendal artery which is a branch of the internal iliac artery)
|
|
|
The inferior rectal artery is a branch of what artery?
|
the internal pudendal artery which is a branch of the internal iliac artery
|
|
|
Venous drainage below the pectinate line is from the _____ _____ vein to the _____ _____ vein to the _____ ______ ______.
|
inferior rectal; internal pudendal; internal iliac; Inferior Vena Cava (IVC)
|
|
|
_____ hemorrhoids receive somatic innervation and are therefore _____.
|
external; painful
|
|
|
The apical surface of hepatocytes face what space?
|
bile canaliculi (like lumen side bringing the bile)
|
|
|
The basolateral surface of hepatocytes face what space?
|
sinusoids (blood side facing the toxins to be cleansed in the sinusoids)
|
|
|
The sinusoids of the liver drain into what vessel?
|
the central vein
|
|
|
What fluid drains through the space of Disse?
|
lymph (in the liver)
|
|
|
In the liver, bile flows from zone ___ (centrilobular zone) to zone _____ (periportal zone).
|
3; 1 (from inside to outside)
|
|
|
In the liver, blood flows from zone _____ (periportal zone) to zone _____ (centrilobular zone).
|
1; 3 (outside to inside)
|
|
|
In the liver, hepatocytes secrete bile into the bile _____, which drain into the bile _____ leading to the central hepatic duct.
|
canaliculi; ductules
|
|
|
Zone I of the liver is also known as the _______ zone.
|
periportal (around the portal triad)
|
|
|
True or False: Zone I (periportal zone) of the liver is affected first by viral hepatitis.
|
true (since this is the first area of the liver to see the bugs and viruses from the blood)
|
|
|
Zone III of the liver is also known as what?
|
centrilobular/pericentral (center of the liver lobule)
|
|
|
Which zone of the liver contains the P450 system?
|
Zone 3/ centrilobular zone thus it is most susceptible to drug toxicities
|
|
|
True or False: Zone III (pericentral vein/centrilobular zone) is affected first by viral hepatitis.
|
False; zone I is affected first by viral hepatitis; zone III is affected first by ischemia
|
|
|
True or False: Zone III (pericentral zone/centrilobular zone) is most sensitive to toxic injury.
|
true
|
|
|
Zone III (pericentral zone/centrilobular zone) is the first site affected by ______ (alcoholic/viral) hepatitis.
|
alcoholic
|
|
|
Name two characteristics of the sinusoids of the liver that make them "irregular capillaries."
|
Fenestrated endothelium and lack of a basement membrane
|
|
|
Liver sinusoids are lined with what kind of endothelium?
|
fenestrated
|
|
|
Notably, the sinusoids of the liver are lacking what structure that most capillaries have?
|
basement membrane
|
|
|
The structure of the liver sinusoids allows macromolecules of plasma to have full access to which cells?
|
hepatocytes
|
|
|
En route from the liver sinusoids to the hepatocytes, plasma macromolecules must pass through what space?
|
The perisinusoidal space (the space of Disse)- where the lymphatics of the liver are
|
|
|
A patient presents with right upper quadrant abdominal pain. Further work-up reveals a gallstone obstructing the common bile duct. Which two biliary ducts drain directly into the common bile duct?
|
the cystic duct and the common hepatic duct
|
|
|
Which two biliary ducts drain into the common hepatic duct?
|
right hepatic duct and left hepatic duct
|
|
|
What is the name of the structure formed by the common bile duct and the pancreatic duct as they empty into the duodenum?
|
The ampulla of Vater
|
|
|
What is the name of the sphincter through which bile passes to enter the duodenum?
|
sphincter of Oddi
|
|
|
True or False: The gallbladder drains directly into the cystic duct
|
true-- then the cystic duct drains in the common hepatic duct to form the common bile duct
|
|
|
The ampulla of Vater opens into what part of the small intestine?
|
the second part of the duodenum
|
|
|
What vein is found within the femoral triangle? artery? nerve?
|
femoral vein, femoral artery, femoral nerve
|
|
|
What structure forms the superior border of the femoral triangle?
|
inguinal ligament
|
|
|
What structure forms the lateral border of the femoral triangle?
|
sartorius muscle
|
|
|
What structure forms the medial border of the femoral triangle?
|
adductor longus muscle
|
|
|
What structure is a fascial tube that extends below the inguinal ligament?
|
femoral sheath (contains femoral artery and vein and lymphatics, but NOT the femoral nerve)
|
|
|
What three main structures are contained within the femoral sheath?
|
Femoral artery, femoral vein, and femoral canal (deep inguinal lymph nodes)
|
|
|
What does the femoral canal contain?
|
deep inguinal lymph nodes
|
|
|
What femoral triangle structure lies outside of the femoral sheath?
|
femoral nerve
|
|
|
Going from lateral to medial, list the components that are found within the femoral triangle.
|
femoral Nerve, femoral Artery, femoral Vein, Empty space, Lymphatics (NAVEL) - venous near penis
|
|
|
What is the site of protrusion of an indirect hernia in the inguinal canal?
|
the internal (deep) inguinal ring
|
|
|
Which runs more medially, the medial umbilical ligament or the median umbilical ligament?
|
median umbilical ligament (remnant of the fetal allantois/urachus)
|
|
|
Name the layers that compose the spermatic cord, from the most superficial to the deepest layer.
|
skin, external spermatic fascia, cremaster muscle and fascia, internal spermatic fascia
|
|
|
True or False: The spermatic cord runs through the external (superficial) inguinal ring.
|
True
|
|
|
True or False: The rectus abdominis muscle is deep to the pyramidalis muscle and superficial to the medial and median umbilical ligaments.
|
true
|
|
|
From the most superficial layer to deep, what are the three muscles that cover the internal (deep) inguinal ring?
|
external abdominal oblique, internal abdominal oblique, transversus abdominis
|
|
|
What is it called when abdominal structures enter the thorax?
|
diaphragmatic hernia
|
|
|
When diaphragmatic hernias occur in infants, it is often as a result of the defective development of what membrane?
|
pleuroperitoneal membrane (between the pleura of the lungs and peritoneum of the abdomen)
|
|
|
What two types of hernias are more common among infants?
|
diaphragmatic hernias and indirect inguinal hernias
|
|
|
What is the most common type of diaphragmatic hernia?
|
sliding hiatal hernia
|
|
|
With a hiatal hernia, the _____ herniates upward through the _____ _____ of the diaphragm.
|
Stomach; esophageal hiatus
|
|
|
What is the entrance point of an indirect inguinal hernia into the abdominal wall?
|
internal (deep) inguinal ring
|
|
|
An indirect inguinal hernia exits the abdominal wall through the _____ _____ _____ and then enters the _____.
|
internal inguinal ring; scrotum
|
|
|
What structure do both direct and indirect inguinal hernias pass through?
|
external (superficial) inguinal ring
|
|
|
What structure is useful for spatially differentiating direct inguinal hernias from indirect inguinal hernias?
|
inferior epigastric arteries (The inferior epigastric artery; use MDs don’t LIe: Medial to inferior epigastric artery = Direct hernia and Lateral to inferior epigastric artery = Indirect hernia to recall locations)
|
|
|
An indirect inguinal hernia enters the internal inguinal ring _____ to the inferior epigastric artery.
|
lateral
|
|
|
Indirect hernias occur in infants as a result of the failure of the _____ _____ to close.
|
processus vaginalis
|
|
|
Which type of hernia is much more common among males?
|
indirect inguinal hernia
|
|
|
A direct inguinal hernia protrudes through what?
|
the inguinal (Hesselbach's) triangle
|
|
|
A direct inguinal hernia bulges directly through the abdominal wall _____ to the inferior epigastric artery.
|
medial
|
|
|
True or False: A direct inguinal hernia passes through the internal (deep) inguinal ring.
|
False; it passes through the external (superficial) inguinal ring only
|
|
|
True or False: A direct inguinal hernia passes through the external (superficial) inguinal ring.
|
true
|
|
|
True or False: An indirect inguinal hernia passes through the internal (deep) inguinal ring.
|
true
|
|
|
True or False: An indirect inguinal hernia passes through the external (superficial) inguinal ring.
|
true
|
|
|
Which type of hernia usually occurs among older men?
|
direct inguinal hernia
|
|
|
Hesselbach's triangle is defined by what structure superiorly?
|
inferior epigastric artery
|
|
|
Hesselbach's triangle is defined by what structure medially?
|
The rectus abdominus muscle
|
|
|
Hesselbach's triangle is defined by what structure inferiorly?
|
inguinal ligament
|
|
|
The inguinal ligament is also known as what?
|
Poupart's ligament
|
|
|
Relative to the pubic tubercle, where is a femoral hernia typically located?
|
Below and lateral to the pubic tubercle
|
|
|
Are femoral hernias more common in men or women?
|
women
|
|
|
What type of hernia is most likely to become incarcerated?
|
femoral hernia (bowel may become incarcerated)
|
|
|
What cells produce the hormone gastrin?
|
G cells in the antrum of the stomach
|
|
|
Where within the gastrointestinal tract are G cells located?
|
antrum of the stomach (by the pyloric sphincter)
|
|
|
What hormone causes the following three effects: increased hydrogen secretion, increased growth of the gastric mucosa, and increased gastric motility?
|
gastrin
|
|
|
What physical state of the stomach leads to increased gastrin release?
|
distention
|
|
|
The presence of what substance within the stomach leads to increased gastrin release?
|
Amino acids (or peptides)
|
|
|
The stimulation of what nerve increases gastrin secretion?
|
The vagal nerve
|
|
|
Is gastrin release decreased by acid or base secretion?
|
it is decreased by acid secretion-- feedback inhibition (a pH under 1.5 will inhibit gastrin secretion)
|
|
|
Gastrin release is greatly increased in patients with what syndrome?
|
Zollinger-Ellison syndrome- ectopic gastrinoma leading to increased acid secretion and ulcers
|
|
|
In Zollinger-Ellison syndrome, there is greatly increased secretion of what protein?
|
gastrin
|
|
|
What two amino acids are especially potent stimulators of gastrin release?
|
Tryptophan and phenylalanine
|
|
|
What cells in the gastrointestinal tract make cholecystokinin?
|
I cells (cholecystokInIn)
|
|
|
Where in the gastrointestinal tract are I cells located?
|
The duodenum and the jejunum
|
|
|
What are the 3 main actions of cholecystokinin?
|
delays/decreases gastric emptying, increases pancreatic enzyme secretions, stimulates gallbladder contraction
|
|
|
Do fatty acids increase or decrease the secretion of cholecystokinin by I cells in the duodenum and the jejunum?
|
increase (this is why pain from gallstones can be increased after eating a fatty meal)
|
|
|
Do amino acids increase or decrease the secretion of cholecystokinin by I cells in the duodenum and the jejunum?
|
increase
|
|
|
In cholelithiasis, pain worsens after the ingestion of what type of foods?
|
Fatty foods; due to stimulation of CCK release
|
|
|
Secretin is produced by what cells?
|
S cells of the duodenum
|
|
|
Secretin has what effect on the pancreas?
|
increases HCO3- release from the pancreatic ductular cells
|
|
|
Secretin has what effect on the stomach?
|
decreases gastric acid secretion
|
|
|
Which two substances stimulate secretin release within the duodenum?
|
acid and fatty acids
|
|
|
Secretin secretion is stimulated by acid and/or fatty acids within the lumen of what specific portion of the gastrointestinal tract?
|
duodenum
|
|
|
Secretin-stimulated pancreatic bicarbonate functions to neutralize _____ _____ within the _____.
|
gastric acid; duodenum
|
|
|
Why is it important that secretin-stimulated bicarbonate neutralize gastric acid within the duodenum?
|
so that pancreatic enzymes can function
|
|
|
Secretin _____ (increase/decreases) secretion of bile.
|
increases
|
|
|
Somatostatin is made by what cells? in what two locations in the gastrointestinal tract are they found?
|
D cells; The pancreatic islets and the gastrointestinal mucosa
|
|
|
Does somatostatin lead to increased or decreased pepsinogen secretion? Increased or decreased gastric acid secretion?
|
decreased; decreased
|
|
|
Does somatostatin increase or decrease fluid secretions in the small intestine? pancreatic secretions?
|
decrease; decrease
|
|
|
What effect does somatostatin have on the gallbladder?
|
decreased contractions
|
|
|
What substance, which is secreted by the pancreatic islet cells, decreases the release of insulin and glucagon?
|
somatostatin (thus it can be used in the treatment of a glucagonoma or insulinoma)
|
|
|
The presence of what substance in the gut lumen causes increased somatostatin release?
|
acid
|
|
|
What type of nerve stimulation causes decreased somatostatin release?
|
vagal nerve (because somatostatin turns everything down -- and you don't want to do that when you have a meal coming!)
|
|
|
What inhibitory hormone made by the pancreas has antigrowth hormone effects as well?
|
somatostatin (thus it can be used to treat acromegaly)
|
|
|
Glucose-dependent insulinotropic peptide is made by what cells? Where in the gastrointestinal tract are they found?
|
K cells; duodenum and jejunum
|
|
|
What is the exocrine regulatory effect of glucose-dependent insulinotropic peptide?
|
Glucose-dependent insulinotropic peptide (aka gastric inhibitory peptide) decreases gastric acid secretion - - along with glucagon-like-peptide-- GIP is an incretin that causes insulin release from beta cells in the presence of high glucose
|
|
|
What is the endocrine regulatory effect of glucose-dependent insulinotropic peptide?
|
Glucose-dependent insulinotropic peptide increases insulin release- - along with glucagon-like-peptide = incretins
|
|
|
What effect do fatty acids have on the secretion of glucose-dependent insulinotropic peptide?
|
increases GIP (since GIP decreases gastric acid secretion-- it makes sense that fatty acids stimulate its release--feedback inhibition)
|
|
|
What effect do amino acids have on the secretion of glucose-dependent insulinotropic peptide?
|
Amino acids cause increased secretion
|
|
|
What effect does oral glucose have on the secretion of glucose-dependent insulinotropic peptide (GIP)?
|
increases
|
|
|
Why is an oral glucose load used more rapidly by the body than an equivalent load that is given intravenously?
|
Because oral (but not intravenous) glucose stimulates glucose-dependent insulinotropic peptide and glucagon-like peptide (GIP and GLP = incretins), which stimulates insulin release
|
|
|
Which GI hormone can be used to treat VIPoma and carcinoid tumors?
|
somatostatin (octreotide)
|
|
|
Where is vasoactive intestinal polypeptide secreted within the gastrointestinal tract?
|
Parasympathetic ganglia in sphincters, gallbladder, small intestine
|
|
|
Vasoactive intestinal polypeptide _____ (increases/decreases) intestinal water and electrolyte secretion.
|
increases (thus VIPomas cause massive diarrhea)
|
|
|
Vasoactive intestinal polypeptide _____ (increases/decreases) relaxation of intestinal smooth muscle and sphincters.
|
increases (thus VIPomas cause massive diarrhea)
|
|
|
Distention _____ (increases/decreases) secretion of vasoactive intestinal peptide.
|
increases
|
|
|
Vagal stimulation _____ (increases/decreases) secretion of vasoactive intestinal peptide.
|
increases
|
|
|
Adrenergic input _____ (increases/decreases) secretion of vasoactive intestinal peptide.
|
decreases (since adrenergic= sympathetic)
|
|
|
A patient presents with copious diarrhea due to secretions from a tumor. Where might the tumor be found?
|
The patient likely has a VIPoma, a non-α, non-β islet cell pancreatic tumor that secretes vasoactive intestinal peptide
|
|
|
Which small messenger molecule causes an increase in smooth muscle relaxation in the gut?
|
nitric oxide (may be missing in achalasia)
|
|
|
Achalasia is caused by an increase in lower esophageal sphincter tone. Loss of secretion of what small messenger molecule contributes to this condition?
|
nitric oxide
|
|
|
Name the hormone produced in the small intestine that produces migrating motor complexes.
|
motilin (clears stomach of undigested food)
|
|
|
Motilin secretion is _____ (increased/decreased) while in a fasting state.
|
increased
|
|
|
Intrinsic factor is a product of what cells?
|
gastric parietal cells
|
|
|
_____ _____ is required for the uptake of vitamin B12 within the terminal ileum.
|
intrinsic factor
|
|
|
The autoimmune destruction of parietal cells results in what two conditions?
|
achlorhydria and pernicious anemia (macrocytic (megaloblastic) anemia)- atrophic gastritis
|
|
|
Pernicious anemia is the result of the _____ destruction of _____ cells.
|
autoimmune; parietal
|
|
|
What cells make gastric acid?
|
parietal cells
|
|
|
Does histamine lead to increased or decreased gastric acid production?
|
increases (thus anti-H2 agents like cimetidine and ranitidine are used to treat acid reflux)
|
|
|
Does acetylcholine lead to increased or decreased gastric acid production?
|
increased (parasympathetic = rest and DIGEST-- thus more acid is needed for digestion)
|
|
|
Does gastrin lead to increased or decreased gastric acid production?
|
increased
|
|
|
Does somatostatin lead to increased or decreased gastric acid production?
|
decreased
|
|
|
Does GIP lead to increased or decreased gastric acid production?
|
decreased
|
|
|
Does prostaglandin lead to increased or decreased gastric acid production?
|
decreased (thus prostaglandin inhibitors like NSAIDs can cause increase risk of ulcers-- prostaglandins are protective of the gastric mucosa)
|
|
|
Does secretin lead to increased or decreased gastric acid production?
|
decreased (since it is trying to make the duodenal environment less acidic for pancreatic enzymes to work)-- it also causes bicarbonate secretion from pancreas
|
|
|
A tumor causes continuous high levels of acid secretion and ulcers. Name the tumor and its product.
|
gastrinoma which produces gastrin which causes release of gastric acid from parietal cells in the stomach
|
|
|
What cells make pepsin?
|
chief cells
|
|
|
What is the action of pepsin?
|
initial protein digestion before pancreatic enzymes reach food in duodenum
|
|
|
At what pH range does pepsin function optimally?
|
acidic
|
|
|
Does the presence of acid increase or decrease the production of pepsin by chief cells in the stomach?
|
increase since H+ cleaves pepsinogen to pepsin
|
|
|
What cells found within the stomach and duodenum secrete bicarbonate?
|
Mucosal cells and Brunner's glands (proximal duodenum) produce bicarbonate
|
|
|
Bicarbonate secretion within the gastrointestinal tract is increased by what substance?
|
secretin
|
|
|
HCl and intrinsic factor are released by _____ cells in the _____ of the stomach.
|
parietal; body
|
|
|
_____ is produced by chief cells in the _____ of the stomach.
|
pepsinogen; body
|
|
|
Name three different types of secretory cells found in the duodenum.
|
K cells (Glucose-dependent insulinotrophic peptide = gastric inhibitor peptide), I cells (cholecystokinin), S cells (secretin)
|
|
|
What drug can block vagal stimulation of parietal cells?
|
atropine (since it is anti-parasympathetic/anti-cholinergic)
|
|
|
Atropine blocks what transmitter in the vagal stimulation of parietal cells.
|
ACh (anti-cholinergic)
|
|
|
True or false: Atropine blocks vagal stimulation of G cells.
|
False; vagal stimulation of G cells is unaffected by atropine as GRP is the neurotransmitter in these neurons and not acetylcholine
|
|
|
What are the sources of salivary secretion? which is most serous? which is most mucinous?
|
submandibular, parotid, submaxillary and submanidibular
parotid is most serous (Serous towards the Sides) sublingual is most mucinous (Mucinous in the Middle) |
|
|
what is the function of alpha-amylase (ptylain) in saliva?
|
begins starch digestion prior to reaching the stomach where it is inactivated by gastric acid
|
|
|
what is the function of bicarbonate in saliva?
|
it neutralizes oral bacterial acids and maintains dental health
|
|
|
what are the functions of mucins (glycoproteins) in saliva?
|
lubricates food
|
|
|
what nerve runs through the parotid gland and can injured during surgery?
|
facial nerve
|
|
|
Is salivary secretion mediated by sympathetic innervation, parasympathetic innervation, or both?
|
both
sympathetic- T1-T3- superior cervical ganglion parasympathetic- via facial and glossopharyngeal nerves |
|
|
low flow rate of saliva is (hypotonic/isotonic), allowing for more time to absorb Na+ and Cl-, while high flow rate is (hypotonic/isotonic), allowing for less time to absorb Na+ and Cl-?
|
hypotonic; isotonic
|
|
|
The proton pump of parietal cells can be found on which side of the cell?
|
the luminal side (but is not always on the surface--thus must take PPI before meals)
|
|
|
The proton pump of the parietal cells pumps _____ cations into the cell and sends _____ out of the cell and into the lumen.
|
K+, H+
|
|
|
What common class of drugs inhibit the parietal cell's proton pump? Give an example of one.
|
proton pump inhibitors (e.g. omeprazole)
|
|
|
True or False: Histamine receptors are found on parietal cells.
|
true H2 receptors are found on parietal cells
|
|
|
True or False: Acetylcholine receptors are found on parietal cells.
|
true (stimulate gastric acid release)
|
|
|
True or False: Prostaglandin receptors are found on parietal cells.
|
true (inhibit gastric acid release)
|
|
|
What specific type of acetylcholine receptors are found on parietal cells?
|
M3
|
|
|
Drug names with what suffix antagonize the H2 receptor in parietal cells?
|
-tidine (e.g. cimetidine, ranitidine, famotidine)
|
|
|
What class of drugs antagonize parietal cells' muscarinic acetylcholine receptors?
|
anti-cholinergics (e.g. atropine)
|
|
|
True or False: There are clinically useful inhibitors for the gastrin receptors on the parietal cells.
|
false; there are gastrin receptors but they are not clinically useful as gastrin's main action is through ECL release of histamine-2
|
|
|
Parietal cells use which enzyme to convert water and carbon dioxide into hydrogen and bicarbonate ions?
|
carbonic anhydrase
|
|
|
Is the mucus secreted by Brunner's glands acidic, alkaline, or neutral?
|
alkaline
|
|
|
Drug names with what suffix antagonize the H2 receptor in parietal cells?
|
-tidine (e.g. cimetidine, ranitidine, famotidine)
|
|
|
What class of drugs antagonize parietal cells' muscarinic acetylcholine receptors?
|
anti-cholinergics (e.g. atropine)
|
|
|
True or False: There are clinically useful inhibitors for the gastrin receptors on the parietal cells.
|
false; there are gastrin receptors but they are not clinically useful as gastrin's main action is through ECL release of histamine-2
|
|
|
Parietal cells use which enzyme to convert water and carbon dioxide into hydrogen and bicarbonate ions?
|
carbonic anhydrase
|
|
|
Is the mucus secreted by Brunner's glands acidic, alkaline, or neutral?
|
alkaline
|
|
|
What common class of drugs inhibit the parietal cell's proton pump? Give an example of one.
|
proton pump inhibitors (e.g. omeprazole)
|
|
|
True or False: Histamine receptors are found on parietal cells.
|
true H2 receptors are found on parietal cells
|
|
|
True or False: Acetylcholine receptors are found on parietal cells.
|
true (stimulate gastric acid release)
|
|
|
True or False: Prostaglandin receptors are found on parietal cells.
|
true (inhibit gastric acid release)
|
|
|
What specific type of acetylcholine receptors are found on parietal cells?
|
M3
|
|
|
What is the function of Brunner's gland secretions?
|
To neutralize acid contents entering the duodenum from the stomach
|
|
|
Brunner's glands are located in what portion of the gastrointestinal tract?
|
submucosa of the duodenum- they are the only submucosal glands of the GI tract!
|
|
|
Brunner's glands are located in what layer of the gastrointestinal tract?
|
submucosa -they are the only submucosal glands of the GI tract!
|
|
|
What disease involves hypertrophy of Brunner's glands?
|
peptic ulcer disease
|
|
|
Which pancreatic enzyme functions to digest starch? Is it secreted in an active or inactive form?
|
alpha-amylase; active form
|
|
|
Lipase, phospholipase A, and colipase function primarily in what process?
|
fat digestion
|
|
|
Trypsin, chymotrypsin, elastase, and carboxypeptidases all function in what process?
|
protein digestion
|
|
|
True or False: Trypsin and chymotrypsin are pancreatic proteases.
|
true
|
|
|
True or False: Elastase and Carboxypeptidases are pancreatic proteases.
|
true
|
|
|
The pancreatic proteases are secreted as what?
|
proenzymes (aka zymogens)
|
|
|
What enzyme converts trypsinogen to trypsin?
|
Enterokinase/enteropeptidase (brush border enzyme in the duodenum)
|
|
|
Where is enterokinase (a protein that activates trypsin) located?
|
In the duodenal brush border
|
|
|
After being converted to its active form, trypsin then does what?
|
It activates the other proenzymes (and more trypsinogen- positive feedback loop)
|
|
|
In addition to enterokinase, what other enzyme can convert trypsinogen to the active form of trypsin?
|
trypsin - positive feedback loop\
|
|
|
What are the three basic enzyme groups that digest carbohydrates?
|
Salivary amylase, pancreatic amylase, and oligosaccharide hydrolases (on intestinal brush border)
|
|
|
What enzyme starts the process of carbohydrate digestion? which bonds does it hydrolyze?
|
Salivary amylase; alpha 1,4 linkages
|
|
|
When salivary amylase hydrolyzes α-1,4 linkages, it yields maltose, maltotriose, and a-limit dextrans which are what type of carbohydrate molecules?
|
dissacharides
|
|
|
Pancreatic amylase is at its highest concentration in what area of the gastrointestinal tract?
|
The duodenal lumen
|
|
|
Pancreatic amylase hydrolyzes starch to what two substances?
|
Oligosaccharides and disaccharides
|
|
|
Where are oligosaccharide hydrolases found?
|
At the brush border of the intestine (rate limiting step in carbohydrate digestion)
|
|
|
Which enzyme controls the rate-limiting step in carbohydrate digestion?
|
Oligosaccharide hydrolases on the intestinal brush border
|
|
|
What are the products of the reactions catalyzed by oligosaccharide hydrolases?
|
monosaccharides (glucose, galactose and fructose)
|
|
|
True or False: Only monosaccharides are absorbed by enterocytes.
|
True; this includes glucose, galactose, and fructose
|
|
|
Glucose and galactose are taken up by what transporter in the gastrointestinal tract?
|
Sodium-glucose linked transporter 1 (sodium dependent)- SGLT-1 thus sodium and glucose should be given together for most efficient glucose absorption in treatment of dehydration
|
|
|
Sodium-glucose linked transporter 1 (a sodium-dependent transporter) absorbs what monosaccharides in the gastrointestinal tract?
|
glucose and galactose
|
|
|
Fructose is taken up by what transporter in the gastrointestinal tract?
|
Glucose transporter 5 (GLUT-5)
|
|
|
All monosaccharides are transported from the enterocytes to the blood by what transporter?
|
Glucose transporter 2 (GLUT-2)
|
|
|
True or False: Sucrose can be directly absorbed by the gastrointestinal tract without being further broken down.
|
False; sucrose is a disaccharide, and only monbosaccharides (glucose, galactose, fructose) are absorbed directly by enterocytes (sucrose = glucose + fructose)
|
|
|
Where is iron absorbed in the gastrointestinal tract?
|
duodenum (FAB to remember iron, folate, B12 sites of absorption and length stores in the body)--iron must be absorbed as a divalent cation
|
|
|
Where is folate absorbed in the gastrointestinal tract?
|
jejunum (FAB to remember iron, folate, B12 sites of absorption and length stores in the body)
|
|
|
Where is vitamin B12 absorbed in the gastrointestinal tract?
|
terminal ileum (FAB)
|
|
|
Along with vitamin B12, what else is absorbed in the ileum?
|
bile acids
|
|
|
What are the six components of bile?
|
Bile salts, phospholipids, cholesterol, bilirubin, water, and ions
|
|
|
What is the only means of cholesterol excretion from the body?
|
via bile
|
|
|
True or False: Bile salts are water-insoluble.
|
False; bile salts are water-soluble because they are conjugated to glycine or taurine
|
|
|
Bile salts are _____ _____ that have been conjugated to amino acids.
|
bile acids
|
|
|
Bilirubin is a breakdown product made during _____ metabolism.
|
heme
|
|
|
Bilirubin is actively taken up by what cell type?
|
hepatocytes
|
|
|
What is the essential structural difference between direct and indirect bilirubin?
|
Direct bilirubin is conjugated; indirect bilirubin is not
|
|
|
Direct bilirubin is conjugated with what?
|
glucoronic acid
|
|
|
What type of bilirubin is water soluble, direct or indirect?
|
direct
|
|
|
What is jaundice?
|
Yellow skin and sclerae due to elevated levels of bilirubin
|
|
|
Indirect bilirubin is free bilirubin that is complexed with what substance in plasma?
|
albumin
|
|
|
Unconjugated bilirubin travels through the circulation bound to _____. This complex can be measured as _____ _____.
|
Albumin; indirect bilirubin
|
|
|
Albumin carries unconjugated, water-insoluble bilirubin through the circulation to the _____ for excretion.
|
liver
|
|
|
The liver excretes what form of bilirubin into the bile?
|
conjugated/direct bilirubin
|
|
|
The conjugated bilirubin that gets excreted into the bile by the liver can be measured as _____ _____.
|
direct bilirubin
|
|
|
The form of bilirubin that gets excreted renally is called _____.
|
urobilirubin
|
|
|
Within the colon, conjugated bilirubin gets converted to _____ by _____.
|
urobilinogen; bacteria
|
|
|
The bacterial conversion of conjugated bilirubin to urobilinogen occurs primarily in the _____.
|
colon
|
|
|
The form of bilirubin that gets excreted in the feces is called _____.
|
sterocobilin (which gived feces its characteristic color)
|
|
|
From the gut, urobilinogen that does not get excreted fecally enters the _____ _____, which takes it back to the _____.
|
enterohepatic circulation; liver
|
|
|
Salivary gland tumors are generally _____ (benign/malignant).
|
benign
|
|
|
Where is the most common location for a salivary gland tumor?
|
parotid gland
|
|
|
A patient presents with a painless, movable mass in a salivary gland. The mass is removed and found to be benign. It later recurs. What type of tumor is it?
|
pleomorphic adenoma- most common salivary gland tumor, painless, moveable mass, benign with high rate of recurrence)
|
|
|
Name the benign tumor composed of heterotopic salivary gland tissue trapped in a lymph node, surrounded by lymphatic tissue.
|
Warthin's tumor
|
|
|
What is the most common malignant salivary gland tumor?
|
mucoepidermoid carcinoma
|
|
|
Achalasia results from the failure of what process to occur?
|
Relaxation of the lower esophageal sphincter
|
|
|
In patients with achalasia, the lower esophageal sphincter cannot relax as a result of the loss of what source of innervation?
|
The myenteric (Auerbach's) plexus- between circular and longitudinal smooth muscle layers
|
|
|
Achalasia causes the progressive development of what symptom due to high LES opening pressure and uncoordinated peristalsis?
|
dysphagia-difficulty swallowing
|
|
|
In patients with achalasia, what test yields a classic diagnostic image?
|
barium swallow shows "bird's beak" or "rat's tail" appearance
|
|
|
In patients with achalasia, barium swallow imaging shows a _____ esophagus with an area of distal _____.
|
dilated; stenosis
|
|
|
Secondary achalasia can result from what disease?
|
Chagas' disease
|
|
|
Achalasia is associated with an increased risk of what malignancy?
|
esophageal cancer
|
|
|
What is the name of the sphincter separating the esophagus from the stomach?
|
lower esophageal sphincter
|
|
|
Scleroderma (CREST syndrome) is associated with esophageal dysmotility involving _____ (high/low) pressure _____ (proximal/distal) to the lower esophageal sphincter.
|
low; proximal
|
|
|
A patient comes to the clinic complaining of heartburn after meals and regurgitation of food upon lying down. What esophageal condition does he likely have?
|
Gastroesophageal reflux disease (GERD)
|
|
|
An alcoholic is brought into the emergency department vomiting copious amounts of blood. The condition this patient likely has causes painless bleeding from what vessels?
|
Submucosal veins in the lower 1/3 of the esophagus, forming varices
|
|
|
True or False: Mallory-Weiss syndrome causes painless mucosal lacerations at the gastroesophageal junction due to severe vomiting.
|
false; the lacerations are PAINFUL and lead to hematemesis
|
|
|
A bulimic patient is brought into the emergency department vomiting blood and complaining of significant epigastric pain. What condition does this patient likely have?
|
Mallory-Weiss syndrome
|
|
|
An alcoholic patient is brought into the emergency department vomiting blood and complaining of significant epigastric pain. What condition does this patient likely have?
|
Mallory-Weiss syndrome
|
|
|
True or False: Boerhaave syndrome causes transmural esophageal rupture due to violent retching.
|
true, remember "Been-Heaving Syndrome"
|
|
|
Ingestion of what compound classically causes esophageal strictures?
|
lye (alkaline corrosive, NaOH)
|
|
|
Esophagitis is commonly associated with what three etiologies?
|
infection (CMV, HSV-1, and Candida albicans), reflux, or chemical ingestion
|
|
|
Which three infectious agents can cause esophagitis?
|
CMV, Herpes Simplex V-1, Candida albicans
|
|
|
Plummer-Vinson syndrome has a triad of what symptoms?
|
1. dysphagia due to esophageal webs--> predispose to esophageal cancer
2. glossitis 3. iron deficiency anemia |
|
|
The dysphagia component of Plummer-Vinson syndrome is caused by what pathology of the esophagus?
|
esophageal webs
|
|
|
A patient is having difficulty swallowing. He has a swollen, tender tongue that appears smooth. Laboratory tests reveal iron deficiency anemia. What is the most likely diagnosis?
|
Plummer-Vinson syndrome
|
|
|
Is Barrett's esophagus an example of glandular dysplasia, hyperplasia, neoplasia, or metaplasia?
|
metaplasia
|
|
|
Barrett's esophagus is an example of what type of metaplasia?
|
Glandular (columnar epithelial) metaplasia; replaces non-keratinized stratified squamous epithelium
|
|
|
What causes Barrett's esophagus?
|
chronic acid reflux
|
|
|
Barrett's esophagus can predispose to the development of what disease?
|
adenocarcinoma of the esophagus (remember BARRett’s = Becomes Adenocarcinoma, Results from Reflux)
|
|
|
The junction between the esophagus and stomach is called the _____ junction.
|
Squamocolumnar; also known as the SCJ or the Z line
|
|
|
What are two behavioral risk factors for esophageal cancer?
|
drinking alcohol and smoking cigarettes
|
|
|
What are the eight risk factors for esophageal cancer?
|
Alcohol/Achalasia, Barrett's esophagus, Cigarette smoking, Diverticuli (Zenker's), Esophagitis/Esophageal webs, Familial history
|
|
|
In the United States, which type of esophageal cancer is most common?
|
Squamous cell carcinoma and adenocarcinoma of the esophagus have a roughly equal incidence
|
|
|
Worldwide, which type of esophageal cancer is most common?
|
squamous cell carcinoma
|
|
|
Squamous cell carcinoma is most common in which section(s) of the esophagus?
|
upper 1/3 and middle 1/3 of esophagus
|
|
|
Adenocarcinoma is most common in which section(s) of the esophagus?
|
lower 1/3
|
|
|
What symptoms are often associated with malabsorption syndromes?
|
diarrhea, steatorrhea, weight loss, and weakness
|
|
|
Give five etiologies of malabsorption syndromes.
|
Celiac sprue, tropical sprue, Whipple's disease, disaccharidase deficiency, and pancreatic insufficiency
|
|
|
Etiologically, celiac sprue is best grouped within what category of diseases?
|
autoimmune diseases
|
|
|
Patients with celiac sprue develop autoantibodies to what substance?
|
Gluten (gliadin) in wheat and other grains
|
|
|
Celiac sprue primarily affects what part of the bowel?
|
proximal small bowel
|
|
|
Tropical sprue can be treated with what kind of drugs?
|
antibiotics (it is caused by an infectious disease)
|
|
|
Which section(s) of the gastrointestinal tract can be affected by tropical sprue?
|
the entire small bowel
|
|
|
What causes Whipple's disease?
|
Tropheryma whippelii
|
|
|
In Whipple's disease, what cell type is in the intestinal lamina propria and the mesenteric nodes?
|
PAS positive macrophages
|
|
|
The classic macrophages seen in Whipple's disease stain positive with what stain?
|
Periodic acid-Schiff stain (PAS)
(for glucose) |
|
|
The classic macrophages seen in Whipple's disease can be found in what two locations?
|
the intestinal lamina propria and mesenteric nodes
|
|
|
A patient presents with malabsorption, soreness in the joints, confusion and chest pain. The diagnosis is Whipple's disease. Is the patient most likely male or female?
|
male (older men are most often affected)
|
|
|
The most common disaccharidase deficiency involves what disaccharidase?
|
lactase (poor Jeff)
|
|
|
Are the villi in lactase deficiency normal or abnormal in appearance?
|
normal
|
|
|
What type of diarrhea is associated with disaccharidase deficiency?
|
osmotic-- the lactose is not absorbed and acts to pull water into the pooh
|
|
|
True or false: Self-limited lactase deficiency can occur following bowel damage from viral diarrhea.
|
true; lactase is located at the tips of intestinal villi, making it vulnerable to damage
|
|
|
What are three common causes of pancreatic insufficiency?
|
cystic fibrosis, chronic pancreatitis, obstructing cancer
|
|
|
Pancreatic insufficiency causes the malabsorption of what macronutrient(s)?
|
fats-- including fat soluble vitamins D, A, K, and E
|
|
|
Pancreatic insufficiency causes the malabsorption of what vitamins?
|
Vitamins A, D, E, and K
|
|
|
Define celiac sprue.
|
An autoimmune-mediated intolerance of gliadin (wheat) that leads to steatorrhea and blunted villi
|
|
|
True or False: Celiac sprue is more common among people of African descent.
|
False; it is most common among people of Northern European descent
|
|
|
What region of the gastrointestinal tract is most affected by celiac sprue?
|
the jejunum
|
|
|
True or False: Celiac sprue is associated with dermatitis herpetiformis.
|
true
|
|
|
True or False: Celiac sprue is associated with malignancy.
|
True- it can be associated with T-cell lymphoma (possibly due to cellular changes from chronic inflammation--lymphocytes in the lamina propria)
|
|
|
Celiac sprue is associated with what type of malignancy?
|
T-cell lymphomas
|
|
|
What are two histological findings for celiac sprue?
|
Blunting of villi and the presence of lymphocytes in the lamina propria
|
|
|
What serum test is used to screen for celiac sprue?
|
Serum levels of tissue transglutaminases
(or antibodies to gliadin) |
|
|
True or False: Decreased mucosal absorption seen in celiac sprue primarily affects the duodenum.
|
false; it primarily affects the jejunum
|
|
|
_____ (Acute/chronic) gastritis is erosive, whereas _____ (acute/chronic) gastritis is nonerosive.
|
Acute; chronic
|
|
|
What are the two types of chronic gastritis?
|
Type A (autoimmune gastritis in fundus and/or body of stomach) and Type B (associated with H. pylori- in antrum-distal stomach)
|
|
|
Which specific type of gastritis is said to be fundal?
|
Type A chronic gastritis- autoimmune
|
|
|
Which specific type of gastritis is said to be antral?
|
Type B chronic gastritis- h. pylori
|
|
|
List six causes of acute gastritis.
|
Nonsteroidal anti-inflammatory drugs, alcohol, stress, uricemia, burns, and brain injury
|
|
|
What is the name for the acute gastritis that occurs in patients with severe burns?
|
Curling's ulcer; remember Burned by the Curling iron
|
|
|
Cushing's ulcer refers to the situation in which _____ _____ leads to acute gastritis.
|
brain injury; remember Always Cushion the brain
|
|
|
Etiologically, type A (fundal) gastritis is best grouped within what category of diseases?
|
Autoimmune diseases
|
|
|
In type A (fundal) gastritis, there are autoantibodies to what?
|
gastric parietal cells-- pernicious anemia (lack of B12) and achlorhydria (lack of H+)
|
|
|
Type A (fundal) gastritis is characterized by what two pathologic states?
|
Pernicious anemia and achlorhydria; remember AB pairing—pernicious Anemia affects gastric body
|
|
|
what causes type B (antral) gastritis?
|
Helicobacter pylori infection
|
|
|
True or False: Acute gastritis carries an increased risk of gastric carcinoma.
|
False; chronic gastritis increases the risk of MALT lymphoma (type B-h. pylori)
|
|
|
By what mechanism do NSAIDs cause acute gastritis?
|
A decrease in PGE2 causes a decrease in gastric mucosa production
|
|
|
By what mechanism do severe burns cause acute gastritis?
|
Curling's ulcers cause a decrease in plasma volume, leading to a sloughing of gastric mucosa
|
|
|
By what mechanism does brain injury cause acute gastritis?
|
Cushing's ulcers causes an increase in vagal stimulation, causing increased ACh, in turn leading to increased H+ production (acid production)
|
|
|
True or False: Ménétrier's disease involves gastric atrophy with protein loss, parietal cell atrophy and decreased mucous cells.
|
False; it involves gastric HYPERTROPHY with protein loss, parietal cell atrophy, and INCREASED mucous cells
|
|
|
True or False: Ménétrier's disease is precancerous.
|
true
|
|
|
Ménétrier's disease involves gastric hypertrophy with _____ cell atrophy and increased _____ cells
|
parietal; mucous
|
|
|
A patient undergoes endoscopy, which reveals a thickened gastric lining. Gastric biopsy reveals increased mucous cells and parietal cell atrophy. What condition does this patient likely have?
|
Ménétrier's disease
|
|
|
Stomach cancer is almost always what type of carcinoma?
|
adenocarcinoma
|
|
|
In patients with stomach cancer, what three processes occur early and aggressively and thus worsen the prognosis?
|
Local spread, spread to the lymph nodes, and metastasis to the liver
|
|
|
What organ is often the first to be affected by the metastases of stomach cancer?
|
liver
|
|
|
Stomach cancer is associated with what dietary exposure?
|
Nitrosamines (from smoked foods)
|
|
|
What two conditions of the stomach are associated with gastric cancer?
|
Achlorhydria and chronic gastritis
|
|
|
What is the term for stomach cancer that tends to show a diffusely thickened, rigid appearance?
|
Linitis plastica; seen as a "leather bottle" appearance of the stomach
|
|
|
Where is a Virchow's node found, and what is it?
|
left supraclavicular node- metastasis from gastric carcinoma
|
|
|
Krukenberg's tumor is located where?
|
bilateral ovarian cancer from metastasis from gastric carcinoma
|
|
|
What physical finding of the skin is associated with adenocarcinoma of the stomach?
|
Acanthosis nigricans
|
|
|
What are two key histologic findings in Krukenberg's tumor?
|
abundant mucous and signet rings
|
|
|
What blood type is commonly associated with stomach cancer?
|
type A (I am going down)
|
|
|
Peptic ulcer disease affects what two regions of the gastrointestinal tract?
|
The stomach (gastric ulcers) and the duodenum (duodenal ulcers)
|
|
|
What is it called when stomach cancer metastasizes to the subcutaneous periumbilical region?
|
Sister Mary Joseph's nodule
|
|
|
Is the pain of gastric ulcers exacerbated, relieved, or unaffected by food intake?
|
Exacerbated (Gastric = pain Greater with meals)
|
|
|
Gastric ulcers may lead to what constitutional symptom?
|
weight loss
|
|
|
Are gastric or duodenal ulcers more closely tied to H. pylori infection?
|
duodenal ulcers (almost 100% are due to H. pylori, while about 70% of gastric ulcers are)
|
|
|
What is the second most common cause of gastric ulcers, after Helicobacter pylori?
|
Chronic use of nonsteroidal anti-inflammatory drugs
|
|
|
What type of ulcers are caused by decreased mucosal protection from gastric acid?
|
gastric ulcers
|
|
|
Is the pain of duodenal ulcers exacerbated, relieved, or unaffected by food intake?
|
relieved--> weight gain (Duodenal ulcers- pain Decreases with meal)
|
|
|
Duodenal ulcers may lead to what constitutional symptom?
|
weight gain; due to symptom relief with consumption of food
|
|
|
What type of ulcers are caused by increased gastric acid secretion or decreased mucosal protection?
|
duodenal ulcers
|
|
|
Patients with duodenal ulcers tend to have hypertrophy of _____ _____.
|
brunner's glands-- bicarb secreting submucosa glands of the duodenum
|
|
|
A patient complaining of stomach pain is found to have a lesion with irregular, raised margins. Is this finding indicative of an ulcer or a malignancy?
|
malignancy (peptic ulcers have clean margins and have a "punched-out" appearance)
|
|
|
List four common complications of peptic ulcers.
|
bleeding, perforation, obstruction, penetration into pancreas (not intrinsically pre-cancerous)
|
|
|
True or False: Peptic ulcers are intrinsically precancerous.
|
False; ulcers are not intrinsically precancerous
|
|
|
Do gastric ulcers more often occur in older or younger patients?
|
older
|
|
|
Recurrent duodenal ulcers due to increased gastric acid secretions and increased gastrin levels described which syndrome?
|
Zollinger-Ellison syndrome- gastrinoma
|
|
|
Inflammatory bowel disease includes what two conditions?
|
Crohn's disease and ulcerative colitis
|
|
|
What is a possible etiology of Crohn's disease?
|
Postinfectious
|
|
|
What general category of diseases is thought to include a possible cause of ulcerative colitis?
|
Autoimmune diseases
|
|
|
What type of inflammatory bowel disease may involve any portion of the gastrointestinal tract?
|
crohn's disease
|
|
|
What type of inflammatory bowel disease always shows rectal involvement?
|
ulcerative colitis
|
|
|
What type of inflammatory bowel disease tends to show continuous lesions?
|
ulcerative colitis
|
|
|
What type of inflammatory bowel disease tends to show skip lesions?
|
crohn's disease
|
|
|
The lesions of Crohn's disease tend to be found throughout the _____ as well as in the _____ _____.
|
Colon; terminal ileum
|
|
|
What type of inflammatory bowel disease tends to spare the rectum?
|
crohn's disease
|
|
|
What gastrointestinal disease tends to demonstrate cobblestone mucosa and creeping fat?
|
crohn's disease
|
|
|
What gastrointestinal disease tends to show friable mucosal pseudopolyps with freely hanging mesentery?
|
ulcerative colitis
|
|
|
What happens to the bowel wall in patients with Crohn's disease?
|
it thickens-- transmural inflammation
|
|
|
The bowel wall thickening of Crohn's disease can cause what sign on barium swallow x-ray?
|
"String sign"-- affected areas with strictures
|
|
|
What gastrointestinal disease can cause linear ulcers, fissures, and fistulas?
|
crohn's disease
|
|
|
What gastrointestinal disease shows noncaseating granulomas and lymphoid aggregates on microscopy?
|
Crohn's disease; remember for Crohn's, think of a fat GRANny and an old crone skipping down a cobblestone road away from the wreck (rectal sparing)
|
|
|
True or False: Ulcerative colitis shows granulomas on microscopy.
|
False; microscopy shows crypt abscesses and ulcers, but no granulomas
|
|
|
What type of abscesses are seen microscopically in patients with ulcerative colitis?
|
crypt absesses
|
|
|
Is perianal disease a complication of Crohn's disease, ulcerative colitis, or both?
|
Crohn's disease
|
|
|
Is malabsorption a complication of Crohn's disease, ulcerative colitis, or both?
|
Crohn's disease
|
|
|
Is toxic megacolon a complication of Crohn's disease, ulcerative colitis, or both?
|
Ulcerative colitis
|
|
|
Is colorectal carcinoma more commonly a complication of Crohn's disease or ulcerative colitis?
|
Ulcerative colitis
|
|
|
Are strictures a complication of Crohn's disease, ulcerative colitis, or both?
|
Crohn's disease
|
|
|
What are the extraintestinal manifestations of Crohn's disease?
|
ankylosing spondylitis, erythema nodosum (often on shins), uveitis, migratory polyarthritis, immunologic disorders
|
|
|
What are the extraintestinal manifestations of ulcerative colitis?
|
pyoderma gangrenosum and primary sclerosing cholangitis (PSC)
|
|
|
The mucosal and submucosal inflammation with friable mucosal pseudopolyps and freely hanging mesentery of ulcerative colitis can cause what appearance on imaging?
|
lead pipe appearance due to loss of haustra
|
|
|
Name the three current treatments most commonly used for ulcerative colitis.
|
Sulfasalazine, infliximab, colectomy
|
|
|
Name the two treatments most commonly used for Crohn's disease?
|
Corticosteroids and infliximab
|
|
|
A patient presents with recurrent abdominal pain that improves with defecation. She complains about changes in her stool frequency and appearance. What is the most likely diagnosis? Are there any structural abnormalities?
|
Irritable bowel syndrome; no- may have alternating diarrhea and constipation or one or the other, pathophy is multifaceted. Treat the symptoms.
|
|
|
What age groups are affected by appendicitis?
|
all ages
|
|
|
What is the most common indication for emergent abdominal surgery in children?
|
appendicitis
|
|
|
Where does the pain of appendicitis typically start?
|
periumbilical (starts as vague and crampy pain)
|
|
|
The initial pain of appendicitis often migrates to what spot?
|
McBurney's point (1/3 the distance from the iliac crest to the umbilicus)
|
|
|
In addition to pain, what two other symptoms are typical of appendicitis?
|
fever and nausea
|
|
|
What potentially disastrous complication can occur with appendicitis?
|
perforation--> peritonitis thus the emergent need for surgery
|
|
|
In the elderly, what important condition must be included in the differential diagnosis of acute abdominal pain in addition to appendicitis?
|
diverticulitis
|
|
|
A young woman presents to the emergency room with diffuse periumbilical pain and nausea. Other than appendicitis, what condition should be ruled out?
|
ectopic pregnancy
|
|
|
What test easily distinguishes an ectopic pregnancy from appendicitis?
|
beta-Human Chorionic Gonadotropin (pregnancy test)
|
|
|
A _____ is a blind pouch that leads off of the alimentary tract.
|
diverticulum
|
|
|
True or False: Diverticula communicate with the lumen of the gut.
|
true
|
|
|
What layers does a "true" diverticulum consist of?
|
all three 3 layers-- mucosa, submucosa, muscularis mucosa
|
|
|
what layers does a "false"/ "pseudo" diverticulum consist of?
|
only 2-- mucosa and submucosa (no outpouching of muscularis mucosa/externa)
|
|
|
"False" diverticula most commonly occur where _____ _____ perforate the _____ _____.
|
vasa recta; muscularis externa
|
|
|
List the four organs in which diverticula commonly occur.
|
esophagus, stomach, duodenum and colon
|
|
|
Are most diverticula congenital or acquired?
|
acquired
|
|
|
Are most diverticula "true" or "false?"
|
"False" diverticula
|
|
|
Diverticula are most often found in what segment of the gastrointestinal tract?
|
sigmoid colon
|
|
|
Diverticulosis is defined by the presence of what?
|
Many diverticula
|
|
|
What percentage of patients who are >60 years old have diverticulosis?
|
50% (so it is common)
|
|
|
What is the etiology of diverticulosis?
|
Increased intraluminal pressure combined with focal weakness of the colonic wall (lower fiber diet is associated)
|
|
|
Diverticulosis is associated with what types of diets?
|
low fiber diets
|
|
|
True or False: Patients with diverticulosis usually have symptoms.
|
False; these patients are most often asymptomatic
|
|
|
List two symptoms that can be associated with diverticulosis.
|
painLESS diverticular bleeding (bright red blood per rectum) and vague abdominal discomfort
|
|
|
What is the definition of diverticulitis?
|
Inflammation of the diverticula
|
|
|
Diverticulitis classically causes pain in what region of the abdomen?
|
left lower quadrant
|
|
|
List the four most common complications that may be caused by diverticulitis.
|
perforation, peritonitis, abscess formation and bowel stenosis
|
|
|
What complication of diverticulitis can lead to pneumaturia?
|
colovesical fistula (fistula between bowel and bladder)
|
|
|
What medication can be used to treat diverticulitis?
|
antibiotics
|
|
|
Define Zenker's diverticulum.
|
A herniation of mucosal tissue at the junction of the pharynx and the esophagus
|
|
|
Is Zenker's diverticulum a true or a false diverticulum?
|
false
|
|
|
True or False: Halitosis is a presenting symptom of a Zenker's diverticulum.
|
true (bad breath)
|
|
|
True or False: Dysphagia is a presenting symptom of a Zenker's diverticulum.
|
true-- food gets stuck in the diverticulum-- stink and dysphagia
|
|
|
Meckel's diverticulum represents a persistence of the _____ _____ .
|
vitelline duct or yolk stalk
|
|
|
Meckel's diverticulum can sometimes contain ectopic _____ mucosa and/or _____ tissue.
|
gastric; pancreatic tissue
|
|
|
If a Meckel's diverticulum contains _____ _____, then it can ectopically secrete _____.
|
gastric mucosa; acid
|
|
|
What is the most common congenital anomaly of the gastrointestinal tract?
|
meckel's diverticulum
|
|
|
List four pathologic conditions that can be caused by a Meckel's diverticulum.
|
bleeding, volvulus, intussusception, obstruction
|
|
|
Where do the complications of a Meckel's diverticulum tend to occur within the gastrointestinal tract?
|
Near the terminal ileum
|
|
|
True or False: A Meckel's diverticulum is the same thing as an omphalomesenteric cyst.
|
False; an omphalomesenteric cyst is a cystic dilation of vitelline duct
|
|
|
A(n) _____ _____ is a cystic dilation of the vitelline duct.
|
omphalomesenteric cyst
|
|
|
About what size is a typical Meckel's diverticulum?
|
2 inches long
|
|
|
Where are Meckel's diverticuli typically located?
|
within 2 feet of the ileocecal valve
|
|
|
In about what percentage of the population can Meckel's diverticula be found?
|
2%
|
|
|
When in life do Meckel's diverticula typically present?
|
typically before age 2
|
|
|
What is intussusception?
|
The "telescoping" of one bowel segment into a distal segment
|
|
|
What is a serious complication of intussusception?
|
Compromised blood supply leading to infarction (abdominal emergency in early childhood)
|
|
|
If intussusception occurs in adults, it is often caused by what?
|
intraluminal mass
|
|
|
Is intussusception found more commonly in adults or infants?
|
infants
|
|
|
What is volvulus?
|
The twisting of a portion of bowel around its mesentery
|
|
|
True or False: Volvulus can lead to bowel obstruction.
|
true
|
|
|
True or False: Volvulus can lead to colorectal cancer.
|
False; however, it can lead to obstruction and infarction
|
|
|
Volvulus may occur at the _____ _____, where there is redundant mesentery.
|
sigmoid colon (and cecum)
|
|
|
Is Hirschsprung's disease congenital or acquired?
|
congenital
|
|
|
What is enlarged in patients with Hirschsprung's disease?
|
The colon
|
|
|
In patients with Hirschsprung's disease, what is noted on intestinal biopsy?
|
lack of enteric nerve plexus (Meissner's and Auerbachs)--failure of migration of neural crest cells
|
|
|
In patients with Hirschsprung's disease, does the aganglionic segment lack Auerbach's plexus, Meissner's plexus, or both?
|
both
|
|
|
Hirschsprung's disease results from the failure of what process?
|
neural crest cell migration
|
|
|
How does Hirschsprung's disease typically present?
|
with chronic constipation early in life
|
|
|
In patients with Hirschsprung's disease, where is the dilated segment of the colon relative to the aganglionic segment?
|
the dilated segment is proximal to the aganglionic segment
|
|
|
In patients with Hirschsprung's disease, which segment of the colon is constricted?
|
the aganglionic segment
|
|
|
There is an increased risk of Hirschsprung's disease among people with what condition?
|
Individuals with Down syndrome
|
|
|
A newborn boy has been vomiting bilious stomach contents and his abdomen has become progressively distended. What condition is likely in this newborn?
|
duodenal atresia
|
|
|
Duodenal atresia is associated with what sign on imaging?
|
"double bubble" sign (dilated distal stomach and duodenum)
|
|
|
Duodenal atresia is due to the failure of _____ of small bowel during development.
|
recanalization
|
|
|
Duodenal atresia is associated with what chromosomal abnormality?
|
down syndrome
|
|
|
What two intestinal disorders are associated with Down syndrome?
|
Hirshprung's disease and duodenal atresia
|
|
|
In the disease _____ _____, a meconium plug can obstruct the intestines, preventing stool passage. This intestinal disorder is known as _____ ______.
|
cystic fibrosis; meconium ileus
|
|
|
Why are premature neonates more prone to develop necrotizing enterocolitis?
|
Because they have decreased immunity
|
|
|
True or False: Necrotizing enterocolitis affects only the colon.
|
False; the colon is usually involved, but this condition can involve the entire gastrointestinal tract
|
|
|
What intestinal layer is initially affected by necrotizing enterocolitis?
|
Intestinal mucosa
|
|
|
What is the most-feared complication necrotizing enterocolitis?
|
Perforation (peritonitis)
|
|
|
Ischemic colitis typically affects _____ (neonates/children/adults/the elderly).
|
the elderly (vascular risk factors!)
|
|
|
Where does ischemic colitis commonly occur?
|
splenic flexure (watershed zone) and distal colon
|
|
|
True or false: Adhesions can cause well-demarcated necrotic zones in the bowel.
|
true
|
|
|
Adhesions cause _____ (acute/chronic) bowel obstruction, commonly from a recent surgery.
|
acute
|
|
|
True or False: Adhesions leading to acute bowel obstruction are commonly seen in patients who have had abdominal surgery.
|
true
|
|
|
What test can confirm a diagnosis of angiodysplasia?
|
angiography
|
|
|
In what three locations is angiodysplasia typically found in the gastrointestinal tract?
|
terminal ileum, cecum, and ascending colon
|
|
|
Describe the blood vessels seen in angiodysplasia.
|
Tortuous and dilated (like esophageal varices)- prone to bleeding
|
|
|
Angiodysplasia causes what symptom?
|
bleeding
|
|
|
Is angiodysplasia more common in a younger population or in the elderly?
|
elderly
|
|
|
Approximately ____% of colonic polyps are benign hyperplastic hamartomas.
|
90%
|
|
|
The more villous the colonic polyp, the _____ (more/less) likely it is to be malignant.
|
More; remember VILLOUS = VILLainOUS. This is because the normal colon does not have villi-- if it is becoming more villous it is a sign that there is more dysplasia/metaplasia
|
|
|
Where in the colon are polyps most commonly found?
|
rectum and sigmoid colon
|
|
|
Adenomatous colon polyps are precancerous lesions. What are three factors that increase their risk of being malignant?
|
1. increased size
2. villous histology (long finger-like projections) 3. increased epithelial dysplasia |
|
|
What is juvenille polyposis syndrome?
|
having multiple polyps in the GI tract-- increased risk of developing adenocarcinoma
|
|
|
juvenille polyps are usually sporadic lesions in children <5 years old. Where are most of these polyps located?
|
80% in the rectum- If it is a single polyp there is no malignant potential
|
|
|
What inheritance pattern does Peutz-Jegher syndrome have?
|
Autosomal Dominant
|
|
|
What autosomal dominant congenital syndrome features multiple non-malignant hamartomas throughout the GI tract, along with hyperpigmented macules on the mouth, lips, hands and genitalia?
|
Peutz-Jegher's syndrome
|
|
|
What is the ranking of colorectal cancer among the most common cancers?
|
3rd most common and 3rd most deadly!
|
|
|
What category of chronic diseases are important risk factors for colorectal cancer?
|
Chronic inflammatory bowel diseases
|
|
|
Which form of inflammatory bowel disease is most associated with colorectal cancer?
|
Ulcerative colitis
|
|
|
What is a common presentation of a left sided colon cancer?
|
obstruction
|
|
|
Most colorectal cancers are sporadic rather than familial. Sporadic colorectal cancer can be due to _____ instability (85% of cases) or _____ instability (15% cases).
|
chromosomal; microsatellite
|
|
|
What is a common presentation of a right sided colon cancer?
|
bleeding (Left obstructs, Right bleeds)
|
|
|
List two familial conditions that are important risk factors for colorectal cancer.
|
Familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer (lynch syndrome)
|
|
|
What are the most important risk factors for colorectal cancer?
|
Nonmalignant neoplasms (that is why we remove all polyps!), inflammatory bowel disease, diet, tobacco use, familial syndromes, gene deletions, increased age, personal history of colon cancer, and family history of colon cancer, streptococcus bovis bacteris, large villous adenomas, juvenille polyposis syndrome, Peutz-Jegher syndrome
|
|
|
What syndrome is a benign polyposis syndrome with increased risk of colorectal cancer and visceral malignancies?
|
Peutz-Jeghers syndrome
|
|
|
At what age is screening for colorectal cancer typically initiated?
|
50 years old
|
|
|
What two tests play the most important role in current colorectal cancer screening practices?
|
Stool occult blood testing and colonoscopy
|
|
|
What appearance does colorectal cancer classically present with on barium swallow x-ray?
|
"apple core" lesion
|
|
|
What is a nonspecific tumor marker for colorectal cancer?
|
CEA (carcinoembryonic antigen)
|
|
|
True or False: Familial adenomatous polyposis is inherited in an autosomal dominant fashion.
|
True; afflicted individuals inherit one faulty copy of the gene and lose the other through an acquired mutation; this is the "two-hit" hypothesis
|
|
|
Familial adenomatous polyposis involves mutation of the ____ gene on chromosome ____.
|
APC; 5q
|
|
|
Colonoscopy of a patient with familial adenomatous polyposis reveals thousands of _____.
|
polyps (a carpet of polyps)--> 100% chance of getting CRC-- need to do colectomy :(
|
|
|
True or false: Familial adenomatous polyposis follows the two-hit hypothesis of malignancy.
|
true
|
|
|
True or false: Familial adenomatous polyposis is pancolonic but never involves the rectum.
|
False; it is pancolonic but always also involves the rectum
|
|
|
Gardner's syndrome includes familial adenomatous polyposis along with ____ and ____ ____ tumors and _____ hyperplasia
|
Osseous; soft tissue; retinal
|
|
|
What type of brain malignancy is associated with Turcot's syndrome?
|
glioma and medulloblastoma; remember TURcot = TURban (CNS tumor)
|
|
|
Hereditary nonpolyposis colon cancer, or Lynch syndrome, involves mutations of DNA ____ ____ genes.
|
mismatch repair
|
|
|
True or False: 80% of cases of heriditary nonpolyposis colon cancer progress to colorectal cancer.
|
true
|
|
|
True or False: Heriditary nonpolyposis colon cancer rarely involves the proximal colon.
|
False; the proximal colon is always involved
|
|
|
A patient has hyperpigmented mouth, lips, hands, and genitalia. The patient's recent colonoscopy revealed hamartomatous polyps throughout the colon. What syndrome does this patient likely have?
|
Peutz-Jegher's syndrome
|
|
|
True or False: Peutz-Jeghers syndrome is benign and not associated with an increased risk of colorectal cancer.
|
False; Peutz-Jeghers syndrome is benign but is associated with an increased risk for colorectal cancer as well as other visceral malignancies
|
|
|
What malignancies are patients with Peutz-Jeghers syndrome at risk of developing?
|
colon and other visceral malignancies (breast, pancreas, stomach, ovary)
|
|
|
chromosomal instability that leads to colon cancer involves what gene(s)?
|
APC/Beta-catenin (A Popular Cause)--85% of all CRC
|
|
|
microsatellite instability involves mutations in what type of genes?
|
DNA mismatch repair genes
|
|
|
Carcinoid tumors are malignancies of which type of cell?
|
Carcinoid tumors are derived from endocrine cells
|
|
|
What percentage of small bowel tumors are carcinoids?
|
50%
|
|
|
What is the most common site of a carcinoid tumor?
|
small intestine
|
|
|
The production of what leads to the classic presentation of carcinoid syndrome (ie, wheezing, flushing, diarrhea)?
|
5-HT (serotonin)
|
|
|
True or False: Wheezing is a classic presenting symptom of carcinoid tumors.
|
true
|
|
|
True or False: Constipation is a classic presenting symptom of carcinoid tumors.
|
False; carcinoid classically presents with wheezing, right-sided heart murmurs, diarrhea, flushing
|
|
|
What finding is seen on electron microscopy in carcinoid tumors?
|
Dense core bodies; these are secretory vesicles
|
|
|
Does cirrhosis tend to be focal or diffuse within the liver?
|
diffuse
|
|
|
In cirrhosis, what pathological process occurs diffusely throughout the liver?
|
fibrosis (regenerative nodules and fibrous bands)
|
|
|
In the cirrhotic liver, diffuse fibrosis destroys the normal liver _____, and there is _____ regeneration.
|
architecture; nodular
|
|
|
Cirrhosis is sometimes further characterized as being either _____ or _____.
|
macronodular; micronodular
|
|
|
Are the nodules of macronodular cirrhosis uniform or varied in size?
|
varied (Drugs and bugs can do various things)
|
|
|
Micronodular cirrhosis is often the result of what category of liver damage?
|
metabolic (alcohol, hemachromatosis, wilson's disease)
|
|
|
Macronodular cirrhosis is usually the result of significant liver injury leading to _____ _____.
|
hepatic necrosis
|
|
|
Give two examples of disease processes that typically lead to macronodular cirrhosis.
|
Postinfectious hepatitis and drug-induced hepatitis (drugs and bugs)
|
|
|
Which form of cirrhosis is most associated with an increased risk of hepatocellular carcinoma: micronodular or macronodular?
|
Macronodular
|
|
|
In cirrhosis, a _____ _____ may relieve portal hypertension.
|
portocaval shunt
|
|
|
A surgical portacaval shunt allows blood to flow between the _____ _____ and the _____ _____ _____.
|
splenic vein; left renal vein
|
|
|
An effect of portal hypertension within the esophagus includes the formation of _____.
|
esophageal varices
|
|
|
In patients with cirrhosis and portal hypertension, melena may be the result of bleeding from either _____ _____ or _____ _____.
|
esophageal varices; peptic ulcer
|
|
|
The rupture of esophageal varices may result in which two different forms of gastrointestinal bleeding?
|
hematemesis or melena
|
|
|
What is a manifestation of portal hypertension within the spleen?
|
splenomegaly (back up through the splenic vein)
|
|
|
What is a manifestation of portal hypertension that can be visualized on the abdominal wall?
|
Caput medusae
|
|
|
When portal hypertension results in a collection of intraperitoneal fluid, it is called _____.
|
Ascites
|
|
|
What are manifestations of portal hypertension that are found within the rectum?
|
internal hemorrhoids-- painless
|
|
|
What condition may be noted on the eye examination of patients with cirhosis as a result of the effects of liver cell failure?
|
scleral icterus
|
|
|
The foul-smelling breath of patients with cirrhosis is referred to as what?
|
Fetor hepaticus (smells like a corpse)
|
|
|
Visible dilated capillary proliferation within the skin secondary to the effects of cirrhosis is called what?
|
spider nevi
|
|
|
What breast abnormality may be noted in male patients with cirrhosis as a result of liver cell failure?
|
gynecomastia
|
|
|
What change in genitalia may occur in patients with cirrhosis as a result of liver cell failure?
|
testicular atrophy
|
|
|
What is the name for the coarse ‘flapping’ tremor of the hands that may occur in patients with cirrhosis?
|
asterixis
|
|
|
List two hematologic abnormalities that may result from liver cell failure in patients with cirrhosis?
|
bleeding tendency and anemia
|
|
|
Why do patients with cirrhosis have an increased tendency to bleed?
|
Liver cell failure leads to the decreased production of prothrombin and clotting factors
|
|
|
What physical finding may be noted in the ankles of patients with cirrhosis as a result of liver cell failure?
|
edema
|
|
|
Are the peptic ulcers of cirrhosis considered to be an effect of portal hypertension or an effect of liver cell failure?
|
an effect of portal hypertension
|
|
|
Are the ascites of cirrhosis considered to be an effect of portal hypertension or an effect of liver cell failure?
|
an effect of portal hypertension
|
|
|
Is the coma of cirrhosis considered to be an effect of portal hypertension or an effect of liver cell failure?
|
An effect of liver cell failure
|
|
|
Is the scleral icterus of cirrhosis considered to be an effect of portal hypertension or an effect of liver cell failure?
|
An effect of liver cell failure
|
|
|
Are the spider nevi of cirrhosis considered to be an effect of portal hypertension or an effect of liver cell failure?
|
An effect of liver cell failure
|
|
|
Is the gynecomastia of cirrhosis considered to be an effect of portal hypertension or an effect of liver cell failure?
|
An effect of liver cell failure
|
|
|
Is the anemia of cirrhosis considered to be an effect of portal hypertension or an effect of liver cell failure?
|
An effect of liver cell failure
|
|
|
Is the ankle edema of cirrhosis considered to be an effect of portal hypertension or an effect of liver cell failure?
|
An effect of liver cell failure (not making sufficient albumin to maintain oncotic pressure--keeping fluids in the capillaries)
|
|
|
What two gastrointestinal enzymes are markers of injury to hepatocytes?
|
Alanine aminotransferase and aspartate aminotransferase (the aminotransferases)
|
|
|
Which aminotransferase is the strongest marker of viral hepatitis?
|
alanine transaminase (ALT> AST)
|
|
|
Which aminotransferase is the strongest marker of alcoholic hepatitis?
|
Aspartate transaminase (AST > ALT by 2:1 or more)
|
|
|
Which gastrointestinal enzyme is a marker of myocardial infarction?
|
aspartate transaminase (AST)
|
|
|
Which liver enzyme is elevated with heavy alcohol consumption?
|
gamma glutamyl transpeptidase (GGT)
|
|
|
What enzyme is a marker of obstructive liver disease?
|
alkaline phosphatase (also elevated when there is enhanced bone resorption- Paget's or multiple myeloma)
|
|
|
What enzyme may be elevated in a patient with hepatocellular carcinoma?
|
alkaline phosphatase (obstruction of the bile flow)
|
|
|
Alkaline phosphatase is a marker of _____ _____ as well as of obstructive liver disease.
|
bone disease (enhanced bone resorption that can be seen in paget's disease and multiple myeloma)
|
|
|
Which two gastrointestinal enzymes are used as markers for acute pancreatitis?
|
amylase and lipase (released from the pancreas)
|
|
|
Which gastrointestinal enzyme is a marker for mumps infection?
|
amylase
|
|
|
Which enzyme is a marker for Wilson's disease?
|
decreased ceruloplasmin (we measure the free form and when there is a lot of copper as in wilson's disease then it gets bound by the ceruloplasmin, decreasing the levels of this enzyme)
|
|
|
Which enzyme marker is elevated in bile duct disease?
|
alkaline phosphatase
|
|
|
What condition is a rare and often fatal childhood hepatoencephalopathy?
|
Reye's syndrome
|
|
|
What liver pathology is associated with Reye's syndrome?
|
Microvesicular fatty changes
|
|
|
What metabolic disturbance is often found in children with Reye's syndrome?
|
hypoglycemia
|
|
|
In addition to fatty liver and hypoglycemia, what other finding is classically associated with Reye's syndrome?
|
coma
|
|
|
What type of infections are associated with Reye's syndrome?
|
viral infections
|
|
|
List two specific viral infections that are especially associated with Reye's syndrome.
|
varicella zoster virus (VZV) and influenza B
|
|
|
Exposure to what type of drugs is associated with Reye's syndrome?
|
salicylates (aspirin)
|
|
|
As a result of Reye's syndrome, what drug is no longer recommended for children?
|
aspirin
|
|
|
Because aspirin is associated with Reye's syndrome in children, what drug is instead recommended for this age group?
|
acetaminophen (tylenol)
|
|
|
True or False: In hepatic steatosis, macrovesicular fatty changes reverse with alcohol cessation.
|
true
|
|
|
Hepatic steatosis is a _____ (short-term/long-term) liver change with moderate alcohol intake.
|
short term
|
|
|
True or False: In alcoholic hepatitis, hepatocytes are often apoptotic.
|
False; hepatocytes become swollen and necrotic, and Mallory bodies (intracytoplasmic inclusions) are often present
|
|
|
True or False: In alcoholic hepatitis, hepatocytes are often swollen.
|
true
|
|
|
True or False: In alcoholic hepatitis, hepatocytes are often necrotic.
|
true
|
|
|
In alcoholic hepatitis, the liver is often infiltrated by what cell type?
|
neutrophils
|
|
|
In alcoholic hepatitis, what is the general ratio of AST to ALT?
|
AST > ALT (ratio usually > 1.5); (remember: You're toASTed with alcoholic hepatitis)
|
|
|
______ _____ are intracytoplasmic eosinophilic inclusions that are often seen in alcoholic hepatitis.
|
mallory bodies
|
|
|
In alcoholic cirrhosis, sclerosis may be noted around the central vein in zone _____ on liver histology.
|
zone III
|
|
|
In alcoholic hepatitis, which is typically elevated more: aspartate aminotransferase or alanine aminotransferase?
|
aspartate aminotransferase
|
|
|
In viral hepatitis, which is typically elevated more: aspartate aminotransferase levels or alanine aminotransferase levels?
|
alanine aminotransferase
|
|
|
True or False: Alcoholic cirrhosis is an irreversible form of liver disease.
|
true
|
|
|
In alcoholic cirrhosis, the micronodular, irregular shrunken liver is described as having a ______ appearance
|
"Hobnail"
|
|
|
True or False: In alcoholic cirrhosis, sclerosis is seen around the central vein (zone III).
|
true
|
|
|
True or False: Hepatic steatosis seen with alcohol ingestion is associated with manifestations of chronic liver disease such as jaundice and hypoalbuminemia.
|
False; alcoholic cirrhosis is associated with manifestations of chronic liver disease
|
|
|
What is the most common primary malignant tumor of the liver in adults?
|
hepatocellular carcinoma
|
|
|
What two infectious diseases are associated with an increased incidence of hepatocellular carcinoma?
|
hepatitis B and hepatitis C
|
|
|
Excessive exposure to what two types of substances is associated with an increased incidence of hepatocellular carcinoma?
|
Alcohol (alcoholic cirrhosis) and carcinogens such as aflatoxin B1 (in peanuts)
|
|
|
List the diseases that are associated with an increased incidence of hepatocellular carcinoma.
|
hemachromatosis, Wilson's disease, alpha-1-antitrypsin disease, alcoholic cirrhosis, hep B and C, aflatoxins (peanuts)
|
|
|
What are typical signs and symptoms of hepatocellular carcinoma?
|
Tender hepatomegaly, hypoglycemia, ascites, and/or polycythemia
|
|
|
True or False: Hepatocellular carcinoma commonly disseminates hematogenously (as opposed to via the lymphatics).
|
true
|
|
|
What laboratory finding is sometimes used as a marker for hepatocellular carcinoma?
|
alpha fetoprotein (aFP)
|
|
|
True or False: Hepatocellular carcinoma may lead to Budd-Chiari syndrome.
|
true (Budd Chiari syndrome = thrombosis of IVC
|
|
|
True or False: Renal cell carcinoma may lead to Budd-Chiari syndrome.
|
false
|
|
|
What causes nutmeg liver?
|
It is caused by backup of blood into the liver
|
|
|
What are the two common causes of nutmeg liver?
|
Right-sided heart failure and Budd-Chiari syndrome
|
|
|
If nutmeg liver is persistent, centrilobular congestion and necrosis can result in what pathological condition of the liver?
|
Cirrhosis; known as cardiac cirrhosis if secondary to heart failure
|
|
|
In Budd-Chiari syndrome, there is occlusion of the _____ _____ _____ or of the _____ veins.
|
inferior vena cava; hepatic
|
|
|
In Budd-Chiari syndrome, venous occlusion results in hepatic _____ and eventual _____.
|
congestion;necrosis
|
|
|
What liver region becomes congested and necrotic in Budd-Chiari syndrome?
|
the centrilobular region (corresponding to zone 3)
|
|
|
In Budd-Chiari syndrome, centrilobular congestion and necrosis lead to what disease?
|
congestive liver disease
|
|
|
How does the congestive liver disease characteristic of Budd-Chiari syndrome manifest?
|
As hepatomegaly, ascites, abdominal pain, and eventually liver failure
|
|
|
Name three conditions associated with Budd-Chiari syndrome?
|
hepatocellular carcinoma, pregnancy, polycythemia vera
|
|
|
True or False: Polycythemia vera is associated with Budd-Chiari syndrome.
|
true
|
|
|
True or False: Wilson's disease is associated with Budd-Chiari syndrome.
|
False; but Budd-Chiari syndrome is associated with polycythemia vera, pregnancy, and hepatocellular carcinoma
|
|
|
α1-Antitrypsin deficiency leads to the accumulation of misfolded proteins where?
|
In the endoplasmic reticulum of hepatocytes
|
|
|
Patients with α1-antitrypsin deficiency have _____ (increased/decreased) elastic tissue in the lungs.
|
decreased
|
|
|
Decreased elastic tissue in the lungs of patients with α1-antitrypsin deficiency causes what medical condition in these people?
|
panacinar emphysema
|
|
|
What is the inheritance pattern seen in α1-antitrypsin deficiency?
|
co-dominant (when both alleles contribute to the genetic phenotype--e.g. ABO blood types)
|
|
|
α1>-Antitrypsin deficiency can be diagnosed histologically by seeing what in liver biopsy samples?
|
PAS positive globules
|
|
|
What is physiological neonatal jaundice?
|
at birth, due to immature UDP glucoronyl transferase (UGT) there is a build up of unconjugated bilirubin (unconjugated hyperbilirubinemia) --> jaundice/kernicterus
|
|
|
what is the treatment for physiologic neonatal jaundice? how does it work?
|
phototherapy- it converts unconjugated bilirubin to a water soluble form that can be excreted in the urine.
|
|
|
Normally, liver cells convert _____ bilirubin into _____ bilirubin.
|
unconjugated (indirect); conjugated (direct)
|
|
|
What is another name for unconjugated bilirubin?
|
indirect bilirubin
|
|
|
What is another name for conjugated bilirubin?
|
direct bilirubin
|
|
|
What organ performs the function of converting unconjugated bilirubin into conjugated bilirubin?
|
the liver
|
|
|
What form of bilirubin is water soluble?
|
direct/conjugated bilirubin
|
|
|
What form of bilirubin can be excreted into the urine?
|
direct/conjugated bilirubin
|
|
|
What form of bilirubin can be excreted into the bile?
|
direct/conjugated bilirubin
|
|
|
After being excreted into bile by the liver, direct bilirubin is then converted by _____ _____ into _____.
|
gut bacteria; urobilinogen
|
|
|
In addition to the bacterial conversion of bilirubin, how else is urobilinogen formed?
|
directly from heme metabolism
|
|
|
Is the hyperbilirubinemia of hepatocellular jaundice conjugated, unconjugated, or both?
|
both
|
|
|
Is the hyperbilirubinemia of obstructive jaundice conjugated, unconjugated, or both?
|
conjugated (extrahepatic obstruction)
|
|
|
Is the hyperbilirubinemia of hemolytic jaundice conjugated, unconjugated, or both?
|
unconjugated
|
|
|
Describe the level of urine bilirubin in the case of hepatocellular jaundice.
|
increased (some of the bilirubin in conjugated)
|
|
|
Describe the level of urine bilirubin in the case of obstructive jaundice.
|
increased
|
|
|
Describe the level of urine bilirubin in the case of hemolytic jaundice.
|
It is absent (acholuria)
|
|
|
Describe the level of urine urobilinogen in the case of hepatocellular jaundice.
|
It is normal or low
|
|
|
Describe the level of urine urobilinogen in the case of obstructive jaundice.
|
it is decreased because you're not getting the bile (containing the bilirubin into the gut to be converted to urobilinogen)
|
|
|
Describe the level of urine urobilinogen in the case of hemolytic jaundice.
|
increased
|
|
|
In what condition is the activity of UDP-glucuronyl mildly decreased?
|
Gilbert's syndrome
|
|
|
What are the potential complications of Gilbert's syndrome?
|
Gilbert's syndrome has no clinical consequences
(maybe some mild jaundice when stressed or sick) |
|
|
In addition to jaundice, what other symptoms are associated with Gilbert's syndrome?
|
There are none; Gilbert's syndrome is essentially asymptomatic
|
|
|
Is the bilirubin level high, low, or normal in patients with Gilbert's syndrome?
|
high
|
|
|
Which levels are elevated in Gilbert's syndrome: conjugated bilirubin, unconjugated bilirubin, or both?
|
unconjugated
|
|
|
True or False: Gilbert's syndrome is associated with hemolysis.
|
False; however, it causes an unconjugated hyperbilirubinemia
|
|
|
In patients with Gilbert's syndrome, episodes of jaundice are associated with _____.
|
stress
|
|
|
In what condition is the activity of UDP-glucuronyl transferase absent?
|
Crigler-Najjar syndrome type I
|
|
|
When in life does Crigler-Najjar syndrome type I typically present?
|
early in life with jaundice, scleral icterus and kernicterus (bilirubin deposition in the brain)- death usually occurs in childhood
|
|
|
List three findings that are associated with Crigler-Najjar syndrome type I.
|
jaundice, kernicterus (bilirubin deposition in the brain) and high unconjugated bilirubin
|
|
|
Are bilirubin levels elevated, depressed, or normal in patients with Crigler-Najjar syndrome type I?
|
elevated
|
|
|
Which levels are elevated in patients with Crigler-Najjar syndrome type I: conjugated bilirubin, unconjugated bilirubin, or both?
|
unconjugated- liver is completely lacking UDP-glucoronyl transferase
|
|
|
What is kernicterus?
|
bilirubin deposition in the brain
|
|
|
What treatments are used for Crigler-Najjar syndrome type I?
|
phototherapy and plasmapheresis-- but affected children die very young (within the first few years of life)
|
|
|
Which is more severe: Crigler-Najjar syndrome type I or type II?
|
Crigler-Najjar syndrome type I
|
|
|
Crigler-Najjar syndrome type II responds to what treatment?
|
phenobarbital-- induces the liver to produce more UDP-glucoronyl transferase to conjugate more bilirubin
|
|
|
Are bilirubin levels elevated, depressed, or normal in patients with Dubin-Johnson syndrome?
|
elevated
|
|
|
Which levels are elevated in patients with Dubin-Johnson syndrome: conjugated bilirubin, unconjugated bilirubin, or both?
|
conjugated bilirubin
|
|
|
What process is defective in patients with Dubin-Johnson syndrome?
|
The liver excretion of bilirubin
|
|
|
What liver finding is characteristic of Dubin-Johnson syndrome?
|
the liver appears grossly black
|
|
|
Is Dubin-Johnson syndrome considered a severe, moderate, or benign disease?
|
benign
|
|
|
What disease is similar to Dubin-Johnson syndrome but does not involve the finding of a grossly black liver?
|
Rotor's syndrome
|
|
|
In what two ways is Rotor's syndrome different from Dubin-Johnson syndrome?
|
Rotor's syndrome is milder and does not cause the liver to turn black
|
|
|
Unconjugated bilirubin is formed from _____ by Kupffer cells and other parts of the mononuclear phagocyte system.
|
heme breakdown
|
|
|
What cells found within the liver are part of the mononuclear phagocyte system and therefore aid in the conversion of heme to unconjugated bilirubin?
|
Kupffer cells
|
|
|
True or False: The bilirubin that enters hepatocytes is water soluble.
|
False; the bilirubin that enters hepatocytes is water-insoluble
(unconjugated) |
|
|
True or False: The bilirubin that exits hepatocytes is water-soluble.
|
true
|
|
|
The water-soluble (conjugated) bilirubin compound that exits hepatocytes is called bilirubin _____.
|
glucuronide
|
|
|
What enzyme within the hepatocyte converts bilirubin to its water-soluble form?
|
UDP-glucuronyl transferase
|
|
|
Name the hereditary hyperbilirubinemia which results from a problem with bilirubin uptake causing an unconjugated bilirubinemia.
|
Gilbert's syndrome
|
|
|
Name the hereditary hyperbilirubinemia which results from a problem with bilirubin conjugation causing an unconjugated bilirubinemia.
|
Crigler-Najjar syndrome (And Gilbert syndrome)
|
|
|
Name the hereditary hyperbilirubinemia which results from a problem with excretion of conjugated bilirubin causing a conjugated bilirubinemia.
|
Dubin Johnson syndrome and Rotor syndrome
|
|
|
What process is inadequate in patients with Wilson's disease?
|
Hepatic copper excretion
|
|
|
In Wilson's disease, there is a failure of _____ to enter the circulation as ceruloplasmin.
|
copper
|
|
|
What five organs are especially prone to accumulate copper in patients with Wilson's disease?
|
brain (esp basal ganglia), liver, kidneys, corneas, joints,
|
|
|
Wilson's disease is also known as what?
|
hepatolenticular degeneration (degenration of the liver and brain)
|
|
|
Wilson's disease is characterized by what tremor?
|
asterixis (flapping of hand when wrist is extended-- like a bird flapping its wings)-- often sign that the liver is not metabolizing things as it should (eg ammonia--> urea)
|
|
|
Which region of the brain is particularly vulnerable to degeneration in patients with Wilson's disease?
|
the basal ganglia (thus producing parkinsonian like effects)
|
|
|
In Wilson's disease, basal ganglia degeneration results in what type of symptoms?
|
parkinsonian
|
|
|
What is the classic laboratory finding in patients with Wilson's disease?
|
decreased plasma ceruloplasmin
|
|
|
What process occurs in the liver of patients with Wilson's disease?
|
cirrhosis
|
|
|
In which region of the eye are deposits classically seen in patients with Wilson's disease?
|
cornea (leading to Kayser-Fleisher rings)
|
|
|
What cancer is associated with Wilson's disease?
|
hepatocellular carcinoma
|
|
|
What movement disorder is associated with Wilson's disease?
|
chorea purposeless jerky movements-- dancelike
|
|
|
What cognitive disorder is associated with Wilson's disease?
|
dementia
|
|
|
With what medication are patients with Wilson's disease treated?
|
penicillamine - chelator that binds copper and allows it to be excreted in the urine
|
|
|
With what pattern of inheritance is Wilson's disease passed?
|
autosomal recessive
|
|
|
What specific type of anemia is associated with Wilson's disease?
|
hemolytic anemia
|
|
|
What are the common findings of Wilson's disease?
|
remember ABCD to recall the common findings: Asterixis, Basal ganglia degeneration, Ceruloplasmin [decreased], Cirrhosis, Corneal deposits, Copper accumulation, Carcinoma (hepatocellular), Choreiform movements, and Dementia
|
|
|
Hemosiderin is composed of which element?
|
Iron (Fe2+)
|
|
|
What is the name of the disease caused by hemosiderosis (the deposition of hemosiderin)?
|
hemachromatosis
|
|
|
Hemochromatosis classically affects what three organs?
|
liver, heart, and pancreas
|
|
|
Hemochromatosis classically causes what liver finding?
|
micronodular cirrhosis
|
|
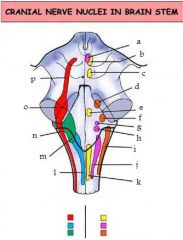
Hemochromatosis is known to induce what skin process?
|
hyperpigmentation (bronze color-->"bronze diabetes"
|
|
|
Hemochromatosis often results in what cardiac disease?
|
congestive heart failure (CHF)- can be dilated or restrictive cardiomyopathy
|
|
|
Hemochromatosis is associated with an increased risk of what cancer?
|
hepatocellular carcinoma
|
|
|
With what pattern of inheritance is primary hemochromatosis passed?
|
autosomal recessive (same as wilson's disease)
|
|
|
True or False: It is possible to develop hemochromatosis without being genetically predisposed to the disease.
|
True (secondary hemochromatosis); due to recurrent blood transfusions as in the case beta thalassemia major
|
|
|
What is the most common cause of secondary hemochromatosis?
|
chronic transfusion therapy as in the case of beta thalassemia major
|
|
|
What are the ferritin levels like in hemachromatosis?
|
high ferritin levels (lots of stored iron)
|
|
|
Do patients with hemochromatosis have high, low, or normal iron levels?
|
high
|
|
|
Do patients with hemochromatosis have high, low, or normal total iron binding capacity?
|
low TIBC- because there is high transferin saturation and thus few remaining binding sites
|
|
|
Do patients with hemochromatosis have high, low, or normal transferrin saturation?
|
high transferrin saturation--carrying around all the iron
|
|
|
What two treatments are often used for hemochromatosis?
|
phlebotomy and deferoxamine chelation
|
|
|
A patient with untreated hemochromatosis sets off metal detectors at the airport while going through security. At least how much total body iron does this patient likely have?
|
50g or more
|
|
|
What is the classic triad of symptoms seen in patients with hemochromatosis?
|
micronodular cirrhosis, diabetes mellitus, and skin hyper pigmentation-- known as "Bronze diabetes"
|
|
|
A patient presents to your office with increasing shortness of breath. He appears to be tan but denies any exposure to the sun. His blood work demonstrates elevated iron and ferritin levels. What does the patient have?
|
hemachromatosis-- heart failure and "bronze" diabetes, so-called secondary to the skin pigmentation seen in this disease
|
|
|
True or false: Hemochromatosis is associated with HLA-A3.
|
true
|
|
|
Is primary sclerosing cholangitis intrahepatic, extrahepatic, or both?
|
both intra and extrahepatic
|
|
|
Primary sclerosing cholangitis involves inflammation and fibrosis of the _____ _____.
|
bile ducts
|
|
|
In primary sclerosing cholangitis, the inflammation and fibrosis of the bile ducts leads to alternating _____ and _____, which are often noted as "beading" on endoscopic retrograde cholangiopancreatography (ERCP).
|
strictures; dilations
|
|
|
What disease is associated with primary sclerosing cholangitis?
|
ulcerative colitis (inflammatory bowel disease)
|
|
|
Primary sclerosing cholangitis can lead to what secondary disease?
|
secondary biliary cirrhosis
|
|
|
(true or false) Patients with primary sclerosing cholangitis have an elevated serum alkaline phosphatase.
|
true
|
|
|
Is primary biliary cirrhosis intrahepatic, extrahepatic, or both?
|
intrahepatic
|
|
|
Is primary biliary cirrhosis an infectious, autoimmune, malignant or degenerative phenomenon?
|
autoimmune
|
|
|
List the symptoms of primary biliary cirrhosis.
|
severe jaundice, steatorrhea, pruritis, and xanthomas (hypercholesterolemia)
|
|
|
What two laboratory findings are classically associated with primary biliary cirrhosis?
|
increased alkaline phosphatase and anti-mitochondrial antibodies
|
|
|
Primary biliary cirrhosis is commonly associated with what two autoimmune disorders?
|
CREST syndrome, scleroderma, and rheumatoid arthritis
|
|
|
What causes secondary biliary cirrhosis?
|
Extrahepatic biliary obstruction
|
|
|
In secondary biliary cirrhosis, extrahepatic biliary obstruction causes _____ (increased/decreased) pressure in the intrahepatic ducts.
|
increased
|
|
|
In secondary biliary cirrhosis, increased pressure in the intrahepatic ducts leads to what?
|
hepatic injury and fibrosis
|
|
|
Secondary biliary cirrhosis is often complicated by what infectious process?
|
ascending cholangitis - inflammation/bacterial infection of the bile duct
|
|
|
In secondary biliary cirrhosis, what causes ascending cholangitis to occur?
|
bacterial infection
|
|
|
In addition to ascending cholangitis, other complications of secondary biliary cirrhosis include bile _____ and bile _____.
|
stasis; lakes
|
|
|
Secondary biliary cirrhosis is characterized by increases in what laboratory parameters?
|
increased alkaline phosphatase, increased conjugated bilirubin, increased cholesterol
|
|
|
Which levels are elevated in patients with secondary biliary cirrhosis: conjugated bilirubin, unconjugated bilirubin, or both?
|
conjugated bilirubin since the obstruction is extrahepatic
|
|
|
Disproportionately high amounts of _____ and/or _____ tend to favor the formation of gallstones.
|
Cholesterol; bilirubin
|
|
|
Gallstones form when solubilizing _____ _____ and _____ are overwhelmed by increased bilirubin and/or cholesterol.
|
Bile acid; lecithin
|
|
|
List the two types of gallstones.
|
Cholesterol stones and pigment stones
|
|
|
Are most cholesterol stones radiolucent or radiopaque?
|
radiolucent-- although 10-20% of cholesterol stones may be radiopaque due to calcification
|
|
|
About what percent of cholesterol stones are radiopaque?
|
10-20%
|
|
|
Why are some cholesterol stones radiopaque?
|
calcification
|
|
|
True or False: Crohn's disease is commonly associated with cholesterol stone formation.
|
true; due to inability of the terminal ileum to reabsorb bile acids-- cannot solubilize cholesterol
|
|
|
True or False: Estrogen exposure is associated with cholesterol stone formation.
|
true-- thus being a fertile female is a risk factor
|
|
|
True or False: The use of clofibrate is associated with cholesterol stone formation.
|
true
|
|
|
True or False: The use of proton pump inhibitors is associated with cholesterol stone formation.
|
False; but the use of clofibrates is associated with cholesterol stone formation
|
|
|
Cholesterol gallstone formation is associated with taking which two medications?
|
clofibrate and estrogen supplements
|
|
|
List the risk factors associated with formation of cholesterol stones.
|
obesity, crohn's disease, cystic fibrosis, advanced age, clofibrate, estrogens, multiparity (multiple childbirths), rapid weight loss, native american origin
|
|
|
What percentage of gallstones are cholesterol stones?
|
80%
|
|
|
Are pigment stones radiolucent or radiopaque?
|
radiopaque
|
|
|
What type of infections are associated with pigment stone formation?
|
biliary infections
|
|
|
In addition to biliary infections, what two other medical conditions are associated with pigment stone formation?
|
chronic hemolysis and alcoholic cirrhosis
|
|
|
What age group is at increased risk for the formation of pigment stones?
|
elderly
|
|
|
Gallstones are best diagnosed by what radiologic modality?
|
ultrasound
|
|
|
Symptomatic gallstones are treated with _____.
|
cholecystectomy
|
|
|
Gallstones can cause what four major complications?
|
ascending cholangitis, acute pancreatitis, bile stasis, cholecystitis
|
|
|
Define biliary colic.
|
Pain caused by gallstones interfering with bile flow, causing bile duct contraction
|
|
|
In what population of patients may biliary colic be absent in the setting of choledocholithiasis
|
diabetics-- neuropathy reduces sensation-- cannot feel pain
|
|
|
Gallstones can cause fistulas between what two organs?
|
the gallbaldder and the small intestine-- gallstone ileus potentially (often at the ileocecal valve)
|
|
|
In what instance would a radiologist see air in the biliary tree on imaging?
|
Air in the biliary tree on imaging would be seen if a gallstone has formed a fistula and obstructed the ileocecal valve
|
|
|
Name the "4 F's" associated with increased risk of developing gallstones.
|
Fat, Female, Fertile and Forty
|
|
|
Name the components of Charcot"s triad of symptoms of cholangitis.
|
Jaundice, fever, and right upper quadrant pain
|
|
|
A patient presents complaining of abdominal pain. On deep palpation of the abdomen, she appears to hold her breath. Name this finding.
|
the patient has a positive Murphy's sign- having the patient inhale brings the inflammed gall bladder closer to your hand causing pain-- so the patient stops inhaling
|
|
|
Cholecystitis is the _____ of the gallbladder due to _____ or ____ or rarely _____.
|
inflammation; gallstones; infection (e.g. CMV), rarely ischemia
|
|
|
Name two infectious agents that can cause cholecystitis.
|
Cytomegalovirus and Cryptococcus
|
|
|
A patient with suspected cholecystitis has elevated alkaline phosphatase levels. What hepatobiliary structure is likely involved?
|
Bile duct (ascending cholangitis)
|
|
|
Acute pancreatitis is caused by the activation of _____ _____ causing autodigestion of the pancreas.
|
pancreatic enzymes
|
|
|
In acute pancreatitis, the activation of pancreatic enzymes causes what harmful process to occur?
|
autodigestion
|
|
|
What biliary tract disease is a cause of acute pancreatitis?
|
gallstones (most common cause in females-- alcohol is most common cause in men)
|
|
|
What infectious disease is a cause of acute pancreatitis?
|
mumps
|
|
|
_____ stings can cause acute pancreatitis.
|
scorpion
|
|
|
What are two metabolic abnormalities that can cause acute pancreatitis?
|
hypercalcemia and hyperlipidemia
|
|
|
List three substances that can cause acute pancreatitis.
|
alcohol (EtOH), steroids, drugs (e.g. sulfa drugs)
|
|
|
List the causes of acute pancreatitis.
|
IGETSMASHED- Idiopathic, Gallstones, Ethanol, Trauma, Steroids, Mumps, Autoimmune, Scorpion Stings, Hypercalemia/Hyperlipidemia,ERCP (iatrogenic), Drugs (e.g. sulfa drugs)
|
|
|
True or False: Sulfa-containing drugs can cause acute pancreatitis.
|
true
|
|
|
Acute pancreatitis often presents with _____ pain that radiates to the _____.
|
epigastric; back
|
|
|
In addition to abdominal pain, acute pancreatitis also often presents clinically with what two symptoms?
|
anorexia and nausea
|
|
|
What two laboratory findings are classically diagnostic of acute pancreatitis?
|
increased amylase and lipase (lipase is more specific)
|
|
|
Which has higher specificity for acute pancreatitis: amylase or lipase?
|
lipase
|
|
|
Acute pancreatitis can lead to what hematologic complication?
|
D.I.C. -- disseminated intravascular coagulation (and fibrinolysis)-- decreased platelet count- increased aPTT and PT,
|
|
|
Acute pancreatitis can lead to what pulmonary complication?
|
Acute Respiratory Distress Syndrome
|
|
|
What electrolyte abnormality can occur as a complication of acute pancreatitis?
|
hypocalcemia-- due to calcium soap deposits--fat necrosis
|
|
|
Chronic calcifying pancreatitis is strongly associated with what condition?
|
alcoholism
|
|
|
What is the mechanism causing hypocalcemia in acute pancreatitis?
|
Ca2+ collects in pancreatic calcium soap deposits, causing hypocalcemia
|
|
|
What is the mechanism of acute respiratory distress syndrome (ARDS) in acute pancreatitis?
|
Pancreatic enzymes act on lung tissue, causing ARDS
|
|
|
True or False: Acute pancreatitis can cause diffuse fat necrosis.
|
true
|
|
|
Chronic pancreatitis leading to pancreatic insufficiency results in what constellation of symptoms?
|
steatorrhea, fat soluble vitamin (D, A, K, E) deficiency, diabetes mellitus
|
|
|
What is the average survival of a person newly diagnosed with pancreatitic adenocarcinoma?
|
6 months or less
|
|
|
At presentation, pancreatic adenocarcinoma has usually already undergone what malignant process?
|
metastasis
|
|
|
Pancreatic adenocarcinoma is more common in what region of the pancreas?
|
head of the pancreas-- leading to obstruction of bile flow--> jaundice
|
|
|
When pancreatic adenocarcinoma occurs in the head of the pancreas, it often causes what process to occur?
|
obstructive jaundice
|
|
|
Pancreatic adenocarcinoma often presents with _____ pain that radiates to the _____.
|
abdominal; back
|
|
|
True or False: Pancreatic adenocarcinoma often presents with inguinal lymphadenopathy.
|
False; presentation typically includes abdominal pain that radiates to the back, weight loss, migratory thrombophlebitis, and obstructive jaundice
|
|
|
True or False: Pancreatic adenocarcinoma often presents with weight loss.
|
true- from both malabsorption and anorexia
|
|
|
What organ can become palpable in the abdomen of patients with pancreatic adenocarcinoma?
|
palpable gall bladder
|
|
|
In patients with pancreatic adenocarcinoma, a palpable gallbladder is often noted in patients who present with what other finding?
|
obstructive jaundice (Courvoisier's sign)
|
|
|
When a palpable gallbladder along with painless obstructive jaundice is noted in patients with pancreatic adenocarcinoma, it is called what?
|
Courvoisier's sign
|
|
|
In addition to abdominal pain, weight loss, obstructive jaundice, and a palpable gallbladder, pancreatic adenocarcinoma also often presents with what?
|
migratory thrombophlebitis (redness and tenderness on palpation of the extremities)
|
|
|
When migratory thrombophlebitis is noted in patients with pancreatic adenocarcinoma, it is called what?
|
Trousseau's syndrome
|
|
|
What two ethnic groups have an increased risk of pancreatic cancer? Male or female?
|
Jewish and African American, males
|
|
|
Name two tumor markers associated with pancreatic cancer.
|
CEA (carcinoembryonic antigen) and CA-19-9
|
|
|
True or False: Pancreatic cancer has a strong association with alcohol abuse.
|
False; pancreatic cancer has been linked to cigarette smoking
|
|
|
Proton pump inhibitors work on pumps that exchange which two ions?
|
Hydrogen and potassium
|
|
|
H2-blockers work on which stomach cell type?
|
parietal cells which secrete H+ (and intrinsic factor)
|
|
|
Muscarinic antagonists work on which two cell types in the stomach?
|
ECL cells (with M1 receptors) and parietal cells (with M3 receptors)
|
|
|
What do antacids do in the lumen of the stomach fundus?
|
Antacids are basic substances that buffer stomach acid
|
|
|
Where do misoprostol, sulcralfate, and bismuth work in the lumen of the stomach fundus?
|
These drugs have a protective effect on the mucosa underlying ulcers
|
|
|
Give at least three examples of H2-blockers.
|
Cimetidine, ranitidine, famotidine, and nizatidine; remember Take H2 blockers before you DINE
|
|
|
What substance is the endogenous agonist of the H2-receptor?
|
Histamine
|
|
|
Is the blockade provided by H2-blockers reversible or irreversible?
|
reversible
|
|
|
By blocking histamine H2-receptors, H2-blockers decrease _____ _____ secretion by parietal cells.
|
Hydrogen ion
|
|
|
List three clinical uses of H2-blockers.
|
Peptic ulcer, gastritis, mild esophageal reflux
|
|
|
Which H2-blocker has important toxicities that are not seen with other H2-blockers?
|
cimetidine
|
|
|
Cimetidine is a potent _____ of P450.
|
inhibitor-- which can lead to toxic levels of other drugs accumulating
|
|
|
Does cimetidine have a proandrogenic or antiandrogenic effect?
|
antiandrogenic-- gynecomastia, decreased libido, impotence, increased prolactin release)
|
|
|
One toxicity of cimetidine is that it can decrease the renal excretion of what?
|
creatinine (ranitidine can do this as well Cimetidine and Ranitidine decrease CReatinine clearance)
|
|
|
Which two H2 blockers can decrease the renal excretion of creatinine?
|
Cimetidine and Ranitidine (decrease CReatinine clearance)
|
|
|
Name the antiandrogenic effects of cimetidine.
|
increased prolactin release, gynecomastia, decreased libido, impotence
|
|
|
By what mechanism does cimetidine cause confusion, dizziness and headaches?
|
it can cross the blood brain barrier
|
|
|
True or False: Cimetidine is safe during pregnancy because it does not cross the placenta.
|
False; cimetidine is NOT safe in pregnancy as it DOES cross the placenta
|
|
|
Give at least two examples of proton pump inhibitors.
|
omeprazole, lansoprazole
|
|
|
Proton pump inhibitors work by inhibiting _____ _____ _____ in stomach parietal cells.
|
Hydrogen potassium ATPase
|
|
|
True or False: Treating diarrhea is one of the principal clinical uses of proton pump inhibitors.
|
False; clinical uses include peptic ulcers, gastritis, esophageal reflux, and Zollinger-Ellison syndrome
|
|
|
What are PPIs used to treat?
|
peptic ulcers, gastritis, esophageal reflux, and Zollinger-Ellison syndrome
|
|
|
Give an example of a drug that functions in a way that is similar to sucralfate.
|
bismuth
|
|
|
Bismuth and sucralfate work by binding where?
|
To the ulcer base
|
|
|
By binding to the base of an ulcer, bismuth and sucralfate provide what?
|
physical protection
|
|
|
In addition to providing physical protection, bismuth and sucralfate work by allowing _____ secretion to reestablish the pH gradient in the _____ layer.
|
HCO3-; mucus
|
|
|
True or False: Treating traveler's diarrhea is one of the principal clinical uses of bismuth and sucralfate.
|
true
|
|
|
What is triple therapy used for?
|
Helicobacter pylori infection- which can lead to ulcer formation
|
|
|
What are the three components of triple therapy?
|
Metronidazole, Amoxacillin (or tetracyclin), bismuth (also can use PPIs)
Please MAke Tummy Better |
|
|
True or False: A PPI can also be used when treating an ulcer caused by H. pylori.
|
True; (remember: Please MAke Tummy Better to recall possible drugs used to treat H. pylori: PPI, metronidazole, amoxicillin, tetracycline, bismuth
|
|
|
Misoprostol is a _____ ____ analogue.
|
prostaglandin E1
|
|
|
Misoprostol functions by increasing the production and secretion of the _____ _____ _____ and decreasing the production of _____.
|
gastric mucous barrier, acid
|
|
|
Misoprostol is used clinically for the prevention of what?
|
Peptic ulcers induced by nonsteroidal anti-inflammatory drugs
|
|
|
Why is misoprostol used in neonates with congenital heart defects?
|
it maintains a Patent Ductus Arteriosus (shunt between pulmonary arteries and aortic trunk) -- necessary in patients with cyanotic congenital heart defects (e.g. tetrology) Remember Misoprostol Maintains
|
|
|
What is misoprostol used for (other than the treatment of gastrointestinal and cardiovascular conditions)?
|
to induce labor
|
|
|
Within what population is misoprostol contraindicated?
|
Women of childbearing potential
as it is an abortifacient |
|
|
In addition to being an abortifacient, what other toxicity does misoprostol have?
|
diarrhea
|
|
|
List two muscarinic antagonists that are used to treat peptic ulcers.
|
Pirenzepine and propantheline
|
|
|
Muscarinic antagonists block what receptors on enterochromaffin-like cells?
|
M1 receptors
|
|
|
By blocking the M1 receptors on enterochromaffin-like cells, muscarinic antagonists achieve what effect?
|
Decreased histamine secretion
|
|
|
Muscarinic antagonists block what receptors on parietal cells?
|
M3 receptors
|
|
|
Muscarinic antagonists block the M3 receptors on what cells?
|
parietal cells
|
|
|
By blocking the M3 receptors on parietal cells, muscarinic antagonists achieve what effect?
|
Decreased hydrogen secretion
|
|
|
What are the muscarinic antagonists pirenzepine and propantheline used for clinically?
|
Peptic ulcers (rarely used)
|
|
|
Name three major side effects caused by muscarinic antagonists.
|
tachycardia (since they inhibit parasympathetics), dry mouth (anticholinergic) and difficulty focusing the eyes
|
|
|
What effects can antacids have on the efficacy of other drugs?
|
Interference with absorption, bioavailability, and urinary excretion
|
|
|
What are two methods whereby antacid use can affect the absorption, bioavailability, or urinary excretion of other drugs?
|
By altering gastric and urinary pH and by delaying gastric emptying
|
|
|
List three compounds that are commonly used as antacids.
|
Aluminum hydroxide, magnesium hydroxide, and calcium carbonate
|
|
|
The overuse of the antacid aluminum hydroxide can cause what toxicities?
|
constipation and hypophosphatemia, hypokalemia, proximal muscle weakness, osteodystrophy, and seizures
|
|
|
Diarrhea, hyporeflexia, hypotension, cardiac arrest and hypokalemia are side effects of which antacid?
|
magnesium hydroxide (remember Mg = Must go to the bathroom)
|
|
|
Overuse of the antacid calcium carbonate can cause what three toxicities?
|
hypercalcemia, rebound acid increase (oh no tums can make things worse!), and hypokalemia
|
|
|
All antacids can cause _____ if they are overused.
|
hypokalemia
|
|
|
The antacid calcium carbonate can ____ and decrease the effectiveness of other drugs like tetracycline.
|
chelate
|
|
|
A patient who heavily self-medicates her gastroesophageal reflux disease complains of dizziness and diarrhea. Which antacid is she most likely overusing?
|
magnesium hydroxide
|
|
|
A patient has a witnessed first seizure. Afterward he complains of recent constipation and proximal muscle weakness. What medication is he most likely overusing to treat his gastroesophageal reflux disease?
|
aluminum hydroxide (remember a minimum amount of feces)
|
|
|
A patient who heavily self-medicates her gastroesophageal reflux disease experiences cardiac arrest and is resuscitated. What antacid is she likely overusing?
|
magnesium hydroxide
|
|
|
A patient is found to have hypophosphatemia and osetodystrophy. What medication is he most likely overusing to treat his gastroesophageal reflux disease?
|
aluminum hydroxide
|
|
|
A patient becomes hypotensive and hyporeflexive. She mentions that she has gastroesophageal reflux disease. Which antacid is she most likely overusing?
|
magnesium hydroxide
|
|
|
What is the mechanism of action of infliximab?
|
It is a monoclonal antibody to tumor necrosis factor-α
|
|
|
Infliximab works because it is a monoclonal antibody to tumor necrosis factor α, which is a _____ cytokine.
|
proinflammatory
|
|
|
List two diseases that are treated with infliximab.
|
crohn's disease and rheumatoid arthritis
|
|
|
A toxicity of infliximab is that it can cause what within the respiratory tract?
|
infection (including reactivation of latent TB)
|
|
|
Infliximab can cause what toxicity within the cardiovascular system?
|
hypotension
|
|
|
In addition to respiratory infection and hypotension, what is another toxicity of infliximab?
|
fever
|
|
|
Sulfasalazine is a combination of what two drugs?
|
Sulfapyridine (antibacterial) and 5-aminosalicylic acid (like mesalamine-anti-inflammatory)
|
|
|
Which of the following is an antibiotic, sulfapyridine or mesalamine?
|
Sulfapyridine
|
|
|
Which of the following is an anti-inflammatory agent, sulfapyridine or mesalamine?
|
mesalamine (5-aminosalicylic acid)
|
|
|
What activates sulfasalazine after it is taken orally?
|
colonic bacteria
|
|
|
Sulfasalazine is used to treat what two diseases?
|
crohn's disease and ulcerative colitis
|
|
|
What is the main reproductive adverse effect of sulfasalazine?
|
reversible oligospermia
|
|
|
What is the main constitutional toxicity associated with sulfasalazine use?
|
malaise
|
|
|
In addition to malaise and oligospermia, what are two other toxicities of sulfasalazine?
|
nausea and sulfonamide toxicity
|
|
|
Ondansetron is an antagonist of what receptor type?
|
5-HT3 (serotonin)
|
|
|
Ondansetron is used to control vomiting in which two situations?
|
After an operation and for patients getting cancer chemotherapy; remember you will not vomit with ONDANSetron, so you can go ON DANCing
|
|
|
What are two toxicities of ondansetron?
|
constipation and headaches
|
|
|
What is the mechanism of metoclopramide?
|
it is a D2 receptor antagonist
|
|
|
With what drugs does metoclopramide interact?
|
Digoxin and diabetic agents
|
|
|
Metoclopramide is contraindicated in patients with what serious gastrointestinal disorder?
|
Small bowel obstruction, because it is prokinetic and thus will worsen the discomfort of these patients
|
|
|
On what parts of the gastrointestinal tract does metoclopramide act?
|
The lower esophageal sphincter (it increases tone and contractility), the stomach, and the small bowel (increases motility); it has no effect on the colon
|
|
|
Does metoclopramide affect the colon?
|
No; it affects the lower esophageal sphincter, the stomach, and the small bowel
|
|
|
What are the clinical uses of metoclopramide?
|
Diabetic gastroparesis and postsurgical gastroparesis
|
|
|
True or false: Metoclopramide can cause restlessness, drowsiness, fatigue, depression, nausea, and diarrhea.
|
true
|