Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
126 Cards in this Set
- Front
- Back
|
What are some indications for inducing parturition in:
a. horse b. dog c. cow |
a. twins, high risk mares (lameness, placentitis, anatomic defects, pre-pubic tendon rupture, behavior problems)
b. maternal-fetal disproportion, pregnancies w/ 1 pup, acquired physical inability c. pregnancies prone to prolonged gestation (in vitro produced calves, cloned calves), seasonal calving (Australia) |
|
|
How does the fetus control the onset of parturition?
|
fetus releases ACTH --> glucocorticoids --> placenta produces inc. estrogen --> PGF-2a release from uterine endometrium --> luteolysis, relaxin release from CL, oxytocin relase
inc. estrogen --> expression of oxytocin receptors in uterus relaxin --> relaxation of cervix, widening of birth canal oxytocin --> myometrial contractions |
|
|
What are the stages of parturition?
|
I: preparation of fetus & dam for birth process
II: fetus expelled III: fetal membranes expelled |
|
|
What are the 3 processes that occur during the postpartum period?
|
contraction of myometrial cells
desquamation of endometrial placental surface endometrial repair |
|
|
What are some indications for induction of abortion?
|
misalliance/unwanted pregnancies
improve breeding efficiency: equine twins, mummies improve production efficiency: pregnant feedlot heifers |
|
|
When must maternal recognition of pregnancy occur?
|
before release of PGF-2a & luteolysis
|
|
|
What determines maternal recognition of pregnancy in:
a. cow, doe, ewe b. mare c. sow |
a. trophoblastic protein-1 (OTP-1, BTP-1): interferon like compounds
b. not known: embryo motility present until d. 15-16, then fixates c. at least 2 embryos in each horn, estrogen (from conceptus), re-routing of PGF-2a, PGE? |
|
|
What is the gestation length & for how many days is the CL required in:
a. ewe b. sow c. mare d. cow e. doe f. bitch g. queen |
a. 150 d.; 55-60 d.
b. 115 d.; term c. 320-360 d.; 4-5 mo. d. 270-292 d.; 200-250 d. e. 150 d.; term f. 64-66 d.; near term g. 63-65 d.; 50 d. |
|
|
At what day(s) does maternal recognition of pregnancy occur in:
a. ewe b. sow c. mare d. cow e. doe |
a. 10-12 d.
b. 10-12 d. c. 14-17 d. d. 14-17 d. e. 14-17 d. |
|
|
How many days post-ovulation is the CL responsive to PGF-2a in diestrus in:
a. ewe b. sow c. mare d. cow e. doe f. bitch |
a. 5-14 d.
b. 12-17 d. c. 5-14 d. d. 5-17 d. e. 5-18 d. f. > D5-8 diestrus |
|
|
For how many days post ovulation is the CL responsive to PGF-2a in PREGNANCY in
a. ewe b. sow c. mare d. cow e. doe f. bitch g. queen |
a. 50-60 d.
b. term c. 4-5 mo. d. term e. term f. term g. term |
|
|
What drugs are used for induction of abortion/parturition in the COW:
a. abortion up to 5 mo. b. abortion 5 mo. to term c. parturition (w/in 2 wks of due date) d. elective C-section |
a. PGF-2a
b. PGF-2a + Dex c. PGF-2a + Dex d. PGF-2a &/or Dex 24 hrs before sx to ensure fetal maturation |
|
|
What drugs are used for induction of abortion/parturition in the MARE:
a. abortion up to 40 d. b. abortion 40-100 d. c. abortion > 120 d. d. parturition (> 330 d.) |
a. 1 injection of PGF-2a
b. multiple injections of PGF-2a c. PGE + PGF-2a or oxytocin d. oxytocin -if Ca > 40 mg/dl -do U/S to verify fetal heart beat 1st DEX has no effect in horses up to 120 d., can also do saline uterine infusion to induce abortion |
|
|
What is the recommended procedure in DOGS for:
a. induction of abortion b. induction of parturition |
a.
spay if not a breeding dog else, wait & preg check at 25-30 d. if pregnant, give Dex for 8-12 d., followed by PGF-2a + cabergoline b. rely on diestrus 1 date (whelping after 57 d.) & do elective C-section |
|
|
What is the recommended procedure in CATS for:
a. induction of abortion b. induction of parturition |
a. spay if not a breeding cat
else, preg check if pregnant: PGF-2a > 30 d. (better ~45 d.) &/or cabergoline > 30 d. b. C-section based on rads |
|
|
What is the recommended procedure in DOES for:
a. induction of abortion b. induction of parturition |
a. PGF-2a
b. after day 144: PGF-2a + Dex |
|
|
What is the recommended procedure in EWES for:
a. induction of abortion b. induction of parturition |
a. PGF-2a
b. after day 143: Dex OR Dex + estradiol benzoate |
|
|
What is the recommended procedure in SOWS for:
a. induction of abortion b. induction of parturition |
a. PGF-2a
b. after d. 111: PGF-2a +/- oxytocin |
|
|
In what species is uterine torsion most common?
|
bovine
|
|
|
Why is uterine torsion less common in mares than cow?
|
less common in mare d/t dorsally attached broad ligaments
bovine uterus attached laterally compared to equine |
|
|
What causes uterine torsion?
|
may be predisposed by any condition that permits ↑ mobility of uterus
-gravid horn enlarges & is supported by rumen, SI, & abdominal wall -non-gravid horn much smaller & creates unbalanced suspension -↑ incidence in cattle housed in stanchions or tie-stall barns for long periods -↑ incidence in conditions resulting in ↓ amt. of uterine fluid -may be precipitated by a sudden movement: fall or slip, butted by another cow, etc. |
|
|
What are clinical signs of uterine torsion?
|
vary from normal to extreme colic: ↑ w/ degree of torsion
in mare & multipara species, signs of abdominal pain are 1st indication of torsion if torsion occurs during parturition: -cow may stand w/ tail elevated -strain w/o fetal membranes or extremities appearing at vulvar opening -have ↑ HR, RR, & rarely ↑ rectal temp. |
|
|
How is uterine torsion diagnosed?
|
based on vaginal & rectal exam
in mares, cows, & ewes, torsion usually extends posterior to cervix & involves vagina rectal exam: preferred diagnostic method b/c of possibility of torsion being cranial to cervix & not palpable per vagina • R torsion: R broad ligament pulled downward & ventral to vagina or uterine body & L broad ligament stretched over top of vagina or uterine body • L torsion: L broad ligament pulled downward & ventral to vagina or uterine body & R broad ligament stretched over top of vagina or uterine body • amt. of torsion on broad ligament helps indicate degree of torsion: as ligament seems more taut --> ↑ degree of torsion • fetus may be hard to palpate: dorso-pubic position (upside down) may indicate 180° torsion vaginal exam findings • vaginal walls may be spirally twisted --> stenosis of vagina • folds spiraling in clockwise direction indicate R uterine torsion • folds spiraling in counterclockwise direction indicate L uterine torsion |
|
|
What is the tx for uterine torsion in cows for:
a. 180-270 degree torsions b. torsions < 180 degrees |
a. place dam in lateral recumbency & roll dam around fetus in direction of torsion
-if R torsion, place dam on R side -after rolling, do rectal exam: may have to roll more than once laparotomy to correct torsion -administer oxytocin to dilate cervix & attempt to deliver fetus per vagina -if unsuccessful, finish C-section thru incision b. if cervix is partially dilated: apply detorsion rod if cervix is undilated -roll & administer oxytocin -if unsuccessful, perform C-section |
|
|
What is the tx for uterine torsion in:
a. mares, ewes, does b. dogs & cats |
a. rolling of dam
b. C-section, OVH if affected horn is ischemic |
|
|
What circumstances lead to fetal mummification?
|
maintenance of dead fetus by:
-presence of another normal viable fetus (pigs, dogs, cats, horses) -persistence of CL of pregnancy assoc. w/ mummified fetus (cows, goats) -maintenance d/t P4 secretion |
|
|
What are some causes of fetal mummification in cows & when during pregnancy does it usually occur?
|
genetic factors
torsion of umbilical cord infectious diseases that don’t cause much inflammation: Campylobacter fetus, BVD usually occurs in 4th, 5th, or 6th months of pregnancy |
|
|
What are some rectal exam findings assoc. w/ fetal mummification in cows?
|
-thick uterus w/ no cotyledons
-no membrane slip -palpable mass in uterus -no fremitus in middle uterine a.: palpable movement of blood -CL present on ovary |
|
|
How often are the left & right horns affected in uterine torsion in dairy cows?
|
59% of torsions are to LEFT, 41% to RIGHT
-torsion to LEFT assoc. w/ R horn pregnancy, torsion to RIGHT assoc. w/ L horn pregnancy -gravid horn rolls toward & over non-gravid horn |
|
|
What is the tx for fetal mummification in cows?
|
PGF-2α IM
-should expel fetus in 48-72 hrs -may pass to vagina & stop: manually remove w/ lubrication -cow will stand w/ tail head elevated, strain, may start to have bad odor -may need to repeat PGF-2α in 96 hrs: 90-95% deliver after 2 treatments C-section (~5%) |
|
|
What is the occurrence of fetal mummification in:
a. horse b. goat & sheep c. pig d. dog & cat |
a. rare
b. affects single fetuses or 1 or both of twins: assoc. w/ infections causing fetal deaths & abortions c. fetuses that die b'twn 40-90 d. maintained & expelled at parturition: common w/ some viral diseases d. occurs w/ some viral diseases |
|
|
What is the pathogenesis of fetal maceration?
|
occurs in all species & at any stage of gestation
differs from mummification in that uterine contents become contaminated -may follow fetal death w/ partial cervical dilation w/o fetus being expelled -open cervix --> uterine contamination (superb media for bacterial growth) |
|
|
fetal maceration: bovine
a. clinical signs b. rectal exam findings |
a. straining, fetid vulvar d/c, fever, anorexia, dec. milk production
b. distended, swollen fetus, gas crepitation in uterus |
|
|
fetal maceration: bovine
a. tx b. px |
a. if cervix is dilated, fetus can be removed by forced extraction (use plenty of lubrication)
if cervix is closed, can try prostaglandins: less successful than w/ mummies -if not successful: C-section -always check for presence of a 2nd fetus b. poor for cow to reproduce again -tx not always successful -extensive endometrial damage d/t bacteria |
|
|
fetal maceration: equine
a. dx b. tx c. px |
a. rectal or vaginal exam
b. remove fetus by manually dilating cervix c. poor for future reproduction d/t extensive endometrial damage |
|
|
fetal maceration: dogs & cats
a. dx b. tx |
a. abdominal palpation & rads (halo of gas around fetus), possible vulvar d/c
b. OVH |
|
|
What species are most affected by hydrops conditions?
|
cattle, sheep, goats
most fetuses are dead |
|
|
What is the pathogenesis of hydrops allantois?
|
90% of dropsical cases
usually assoc. w/ dz of uterus -causes functional changes in allantois chorion --> overproduction of allantoic fluid -removal of fluid --> refilling in a matter of hours |
|
|
What is the difference in abdominal enlargement pattern w/ hydrops allantois vs. hydrops amnion?
|
hydrops allantois: rapid abdominal enlargement (may be non-ambulatory)
- usually occurs late in gestation -uterus is swollen & turgid: hard to palpate fetus or placentomes hydrops amnion: slowly developing abdominal enlargement -flaccid uterus: fetus & placentomes may or may not be palpable -pear shaped abdomen |
|
|
What is the prognosis for hydrops allantois?
|
very poor for survival: systemic shock, high incidence of retained placenta & metritis post-delivery
|
|
|
What is the pathogenesis of hydrops amnion?
|
assoc. w/ genetic or congenitally defective fetus: can’t swallow amniotic fluid
|
|
|
What is the tx for hydrops conditions?
|
salvage slaughter recommended
-genetic implications of hydrops amnion -poor px & uterine damage or dz in allantois induce parturition or C-section: invariably have retained placenta (poor px) |
|
|
Twinning is only considered pathological in what species?
|
horse
accounts for 20-30% of all equine abortions |
|
|
What are some methods to prevent twin conceptions in horses?
|
management of double ovulations: must have transrectal U/S
-breed mare w/o regard to # of anticipated ovulations -give hCG or GnRH to cause synchronous ovulations -determine length of interval b’twn ovulations correction of twin embryos: use of U/S -during mobility phase (days 11-17) -wait until embryos are separated & pinch one -may require frequent U/S 5-15 min. apart -after fixation (after day 17 up to ~ day 27-28) -if fixed bilaterally: rupture 1 vesicle -if fixed unilaterally: allow natural reduction to occur (50% by day 20, 90% by day 40) -transvaginal aspiration: days 30-40 (~50% success rate) abortion of both conceptuses: PGs, uterine infusion, crushing of both vesicles, nutritional limitations to cause mare to resorb 1 fetus |
|
|
What are some causes of prolonged gestation in
a. pigs b. sheep c. cows d. iatrogenic |
a. iodine deficiency, genetic basis (inbred lines)
b. consumption of Veraturum californicum (not common) c. genetics: Holsteins, Ayrshires, Guersneys -never produces normal calves d. decapitation of fetus, prolonged administration of progesterone (mostly horses), vitamin A deficiency (esp. in pigs) |
|
|
What is the pathogenesis of fetal emphysema?
|
assoc. w/ prolonged dystocia (> 24 hrs) in almost all species
-fetus dies at or near parturition & organisms from vagina invade uterus & fetus --> emphysema -rarely, may occur in face of closed cervix in cases of septic metritis |
|
|
What is the tx for fetal emphysema?
|
traction w/ adequate lubrication if fetus in proper presentation, position, & posture
fetotomy C-section -food animals: often a salvage procedure -litter bearing species: OVH |
|
|
What are some advantages of artificial insemination?
|
control of animal dz: eliminate coitus, can test sires for dz, can add ABs to semen
↑ use of an outstanding sire incompatibilities are overcome eliminates danger & undesirability of maintaining a male on premises |
|
|
What are some disadvantages of AI?
|
selections of males must be strictly adhered to
easier for inbreeding to occur dz may still be spread if untested males are used trained personnel required: inseminators, heat detectors proper facilities required |
|
|
What semen collection methods are used for AI in
a. pigs b. most other species |
a. warmed thermos
b. artificial vagina |
|
|
What are some principles related to preservation of semen?
|
all must be extended
every time you process semen, you ↓ viability (esp. in dog & horse) consider any agent to be spermicidal, even air storage containers for frozen semen: straws, ampules, pellets, microencapsulation |
|
|
In what species must semen be filtered to remove large gel fraction?
|
pig, horse
|
|
|
timing of AI: cow
a. timing of insemination b. method of depositing semen c. site of semen deposition d. length of estrus |
a. 12-18 hr. after onset of estrus
b. rectovaginal c. intrauterine d. 12-18 hrs |
|
|
timing of AI: sheep
a. timing of insemination b. method of depositing semen c. site of semen deposition d. length of estrus |
a. 15 hrs after onset of estrus
b. vaginally via speculum c. intracervical d. 30 hrs |
|
|
timing of AI: pig
a. timing of insemination b. method of depositing semen c. site of semen deposition d. length of estrus |
a. 30 hrs after onset of estrus
b. vaginally via bent catheter c. intracervical d. 48 hrs |
|
|
timing of AI: horse
a. timing of insemination b. method of depositing semen c. site of semen deposition d. length of estrus |
a. 48 hrs prior to end of estrus (most breed EOD after onset of estrus)
b. vaginocervical c. intrauterine d. 7 d. |
|
|
timing of AI: cat
a. timing of insemination b. method of depositing semen c. site of semen deposition d. length of estrus |
a. when showing behavioral estrus
b. vaginal c. anterior vagina d. 2-3 wks if not mated (induced ovulators) |
|
|
timing of AI: dog
a. timing of insemination b. method of depositing semen c. site of semen deposition d. length of estrus |
a. 2-3 d. after 1st estral smear
b. vaginal c. anterior vagina d. 7-9 d. |
|
|
What are some hereditary causes of dystocia?
|
abnormality of genital tract, twinning, ↑ fetal head size (ex. hydrocephalus), prolonged gestation: usually have large fetus, ankylosed joints (ex. perosomus elumbis), mummified fetus, double muscling (cattle)
|
|
|
What are some nutritional/management causes of dystocia?
|
↓ pelvic size
fat in pelvic cavity uterine inertia: d/t lack of exercise during pregnancy --> lack of muscle tone close confinement: lack of exercise |
|
|
What are some traumatic/infectious causes of dystocia?
|
abdominal wall damage, uterine torsion, pelvic fx (small animals)
infection: not very common -can cause: uterine inertia, incomplete cervical dilation, fetal death, loss of caruncles (ruminants) |
|
|
What are some causes of uterine inertia --> dystocia?
|
-lack of exercise
-over-stretching of uterus -older animals (dogs, ewes, does): failure of oxytocin release |
|
|
What is meant by the presentation of the fetus?
|
relationship of spinal axis of fetus to that of the dam: longitudinal (99.9%) or transverse
portion of fetus that is approaching or entering pelvic cavity or birth canal: anterior or posterior if longitudinal, dorsal or ventral if transverse |
|
|
What is meant by the position of the fetus?
|
in longitudinal presentation: relationship of dorsum of fetus to quadrants of maternal pelvis
-dorsosacral, R or L dorsoilial, dorsopubic in transverse presentation: relationship of head of fetus to quadrants of maternal pelvis -L or R cephalo-ilial |
|
|
What is meant by the posture of the fetus?
|
relationship of fetal extremities to body of fetus
-extremities may be flexed, extended, or retained: describe joint closest to pelvis -R or L side -above or beneath fetus |
|
|
What is the normal presentation, position, & posture of a normal unipara?
|
-anterior longitudinal presentation
-dorsosacral position -head, neck, & forelimbs extended |
|
|
What is the approach to dystocia correction?
|
-hx: how long has dam been in labor?, how much intervention has gone on before vet arrived?
-exam -PE -rectal: clean out, check for uterine torsion, determine which horn is pregnant -vaginal -discuss px w/ owner -place dam in desired location -anesthesia |
|
|
What obstetrical procedures are used in dystocia correction
|
mutation: return of fetus to normal presentation, position, & posture by:
-repulsion: pushing fetus out of maternal pelvis into abdominal cavity -rotation: turning fetus on its long axis to bring it into dorsosacral position -version: rotation of fetus on its transverse axis -extension of neck & limbs -repulsion of proximal limb -lateral rotation of mid-limb -traction of distal limb |
|
|
What is forced extraction of fetus & what are some indications for its use?
|
: withdrawal of fetus from dam thru birth canal by application of outside force or traction
indications: uterine inertia, following corrective mutation, relatively large fetus, to cause cervical dilation, posterior presentations, pathological obstructions, to avoid fetotomy or C-section, in combo w/ fetotomy |
|
|
What is the proper chain placement & procedure for forced extraction of fetus?
|
chain placement
-2 loops: above AND below fetlock -through mouth: NOT around mandible -around neck: dead fetus only 3 point traction when possible direction of extractive force -begin dorsal & posterior -after head is at vulva, change to ventral & posterior -alternate traction on limbs & head -rotate fetus 30º R or L before fetal pelvis enters maternal pelvis |
|
|
What is fetotomy & what are some advantages & disadvantages, & indications ?
|
reduction of fetal size by division or removal of certain parts (most commonly done in cattle)
indications: dead fetus, rel. or absolutely oversized fetus, fetal monsters, incomplete cervical dilation (+): reduces fetal size, avoids C-section, minimal assistance necessary, may ↓ trauma to dam, assoc. w/ less infertility that C-section, less aftercare & shorter recovery time than w/ C-section, can be monetarily rewarding (-): lacerations of birth canal, time consuming, hard work, may causes lacerations to operator |
|
|
What are the 5 reflexes assessed to determine fetal viability?
|
1. depress fetal globes --> globes move or eyelids flutter
2. insert finger into mouth --> suckling response 3. insert finger into anus --> anus contracts (may take 30-45 s.) 4. pinch skin --> withdrawal reflex 5. flex a limb maximally --> withdrawal reflex #5 disapperas 1st, #1 disappears last |
|
|
What are some indications for C-section w/ dystocia?
|
fetotomy impossible d/t small birth canal, incomplete cervical dilation, relatively or absolutely large fetus, fetal giants, uterine torsion, hypoplastic genital tract, hydrops conditions (salvage slaughter recommended), vaginal or vulvar stenosis, fetal mummification (rarely have to do: < 5%), uterine inertia (litter bearing species)
|
|
|
What is pelvic splitting & when is it indicated?
|
gives 2-3” more space: makes delivery of large fetuses easier
only done on 1st calf heifers < 27 m of age usually restricted to beef cows on pasture: cow unstable after procedure & needs to be on soft ground requires epidural use pelvic chisel & maintain chisel on symphysis of pubis |
|
|
What is the most common cause of dystocia in cows & how is it treated?
|
fetal oversize (may be relative or absolute)
most can treated w/ forced extraction may require fetotomy more difficult in posterior presentation |
|
|
What are some postural defects in cattle in
a. anterior presentation b. posterior presentation |
a. carpal flexion, partial elbow flexion, shoulder flexion, lateral deviation of head & neck, ventral displacement of head
b. hock flexion, bilateral hip flexion (TRUE BREECH): cannot turn, must deliver in posterior presentation |
|
|
What are some fetal monsters in cows & how is related dystocia usually treated?
|
-shistosomus reflexus: acute angulation of spinal column & incomplete closure of abdominal wall
-often present 4 limbs anteriorally -partial fetotomy: only need 1 cut -perosomus elumbis: malformation of lumbar vertebrae -hydrocephalus |
|
|
What is the most common cause of dystocia in horses & how is it treated?
|
lateral deviation of head +/- neck
-d/t longer relative length of equine neck & explosive (rapid) nature of birth process in mare -correct by same procedures as in cows, but more difficult d/t length of neck |
|
|
What are some causes of dystocia in sheep & goats & how can they be treated?
|
fetal oversize: common cause of dystocia in ewes or does carrying single fetus
-usually remedied by forced extraction uterine inertia: common in ewe d/t hypocalcemia or pregnancy toxemia postural defects in anterior presentation -easily manipulated & extracted if labor is not protracted -same as in cattle & corrected similarly postural defects in posterior presentation -hip flexion -hock flexion: common w/ twins correction -can deliver anteriorally or posteriorally -C-section relatively easy |
|
|
What are some causes of dystocia in pigs & how can they be treated?
|
fetus may be delivered in any longitudinal presentation, posture, & position
dystocias usually relieved by traction w/ hand, snare, or obstetrical forceps uterine inertia: common w/ prolonged labor |
|
|
What are some causes of dystocia in dogs & cats & how can they be treated?
|
fetus may be delivered in any longitudinal presentation, posture, & position
fetal oversize: problem in small litters (≤ 3) digital exam -can correct postural defects of head in medium & large breeds -stroking of vaginal vault (feathering) should cause reflex release of oxytocin --> contraction -if no contraction: uterine inertia forceps can be used to grasp fetus indiscriminate use of oxytocin can cause uterine rupture before administering: -perform digital pelvic exam -abd. rads to check for pup lodged in pelvis |
|
|
What are the cytologic findings assoc. w/ canine
a. proestrus b. estrus |
a. -non-cornified cells: parabasal & small intermediate
-cornified cells: superficial & large intermediate -bacteria, RBCs b. -should have at least 95% cornification (metaplasia): pyknotic nuclei, angular shape, abundant cytoplasm -“clear background”: variable & should not be used solely to estimate fertile period |
|
|
What are the cytologic findings assoc. w/ canine
a. diestrus b. anestrus c. pyometra |
a. -1st day: sudden appearance of ~50% parabasal cells, accompanied by WBCs & bacteria, +/- RBCs
-late diestrus: foam cells: parabasal cells w/ vacuoles -no WBCs b. -parabasal cells: large stippled nucleus w/ little cytoplasm -foam cells -no WBCs c. parabasal cells w/ WBCs & bacteria: can look like early diestrus, but P4 may be low (≤ 2 ng/ml) --> luteolysis |
|
|
After how many hours are fetal membranes considered retained in:
a. cow b. horse c. dog |
a. > 8 hr. after fetus expelled
b. > 3 hr. c. 0.5-1 hr. after last fetus delivered |
|
|
What factors predispose to retained fetal membranes?
|
herds infected w/ certain infectious diseases (ex. Brucellosis in cows)
twins: cows, mares induced parturition: 50-60% will have retain fetal mems females w/ previous hx of retained fetal mems |
|
|
RFM: toxic syndrome in cows
a. signs b. tx c. prevention |
accompanied by severe metritis (less common than non-toxic)
a. varies from slight depression to extreme life-threatening situation -pyrexia, anorexia, severe depression, ketosis, enlarged fluid-filled uterus, rotten odor, +/- placenta at vulvar opening or in vaginal canal (may be able to palpate per rectum) b.-systemic ABs: penicillin -NSAIDs (Banamine) +/- antihistamines - +/- uterine lavage w/ ABs: avoid tx of uterus until systemic signs improve -monitor temp, feed consumption, milk production c. -don’t manually remove retained fetal mems: cut off at vulvar lips, +/- AB infusion of uterus -prevent retained fetal mems: adequate dietary Selenium, clean calving environment |
|
|
RFM: non-toxic syndrome in cows
a. signs b. tx c. prevention |
a. few if any signs: slight depression, strong odor +/- retained fetal mems protruding from vulvar lips
b. -leave placenta alone -ABs if systemic signs develop (penicillin, tetracycline) -examine post-partum & tx if necessary (15-30 d.): uterine infusions?, re-examine prior to breeding -prostaglandins?: cause uterus to contract down (no proven benefit) c. don't manually remove RFM adequate dietary selenium, clean calving environment |
|
|
RFM: horse
a. predisposing factors b. signs if retained < 8 hrs. c. signs if retained > 8 hrs. |
a. delayed uterine involution: induced parturition, C section, obstetrical procedures, prolonged delivery
b. retained < 8 hrs: restlessness, irritation at placenta hanging from vulva, slight signs of colic c. retained > 8 hrs: may develop metritis-laminitis-toxemia syndrome (semi-emergency) -depression, anorexia, pyrexia, colic, fluid distended uterus, ↑ digital pulses, +/- foot pain -placenta may not be present at vulvar lips: small piece can cause clinical signs |
|
|
What is the tx for retained fetal membranes in horse?
|
removal of fetal mems
-oxytocin: IV bolus -oxytocin: IV drip (probably most effective, but may be hard to administer) -uterine lavage: not used much -povidone iodine solution infusion -manual removal NOT recommended: extreme risk of hemorrhage & infection -after removal, placenta should be examined to make sure all of it has been expelled if > 8 hrs -ABs: penicillin -NSAIDs: phenylbutazone -metritis syndrome may require repeated uterine lavages: not used much -laminitis prevention |
|
|
RFM: pig
a. signs b. tx c. prevention |
usually occurs after dystocia or prolonged labor
a. anorexia, depression, purulent vaginal d/c b. hard to tx: oxytocin, parental ABs, intrauterine infusions? c. attention at farrowing, oxytocin to speed delivery? |
|
|
RFM: dog & cat
a. predisposing factors b. signs c. tx d. prevention |
a. seen most commonly in toy breeds in which dystocia or prolonged labor occurs
b. acute metritis: dark green vulvar d/c 12 hrs. after parturition, toxemia, pyrexia, anorexia, tachycardia c. placental removal -feathering: digital manipulation of vaginal vault -sponge forceps to twist membranes: BE CAREFUL! parenteral ABs: ampicillin, amoxicillin AB uterine infusion: hard to get into uterus shock tx: fluids d. may prevent by giving oxytocin 2-3x after whelping in toy breeds -careful: risk or uterine rupture (do rads 1st to make sure no more stuck fetuses!) |
|
|
What factors are assoc. w/ RFM in sheep & goats?
|
Brucella infections
occ. seen in older ewes, does |
|
|
In what species is uterine prolapse most common?
|
cow, sheep
emergency in all species: shock, infectious or trauma to exposed mucosa, hemorrhage d/t uterine a. trauma |
|
|
What are some predisposing factors for uterine prolapse & when do most occur?
|
long mesometrial attachments, violent or strong tenesmus, atonic uterus (hypocalcemia), retain fetal mems
occurs most often immediately after parturition or up to several hours later |
|
|
What are some characteristics of uterine prolapse occurrence in cows?
|
high incidence in 1st calf heifers: may be d/t prolonged labor & prolonged postpartum recumbency
higher incidence in stanchioned or stable dairy cattle: d/t elevated front quarters ↑ incidence after dystocia, esp. those in which abnormal force was used to extract calf OR if fetus is not well lubricated ↑ incidence in dairy cattle affected w/ milk fever (hypocalcemia) |
|
|
What is the tx for uterine prolapse in cows?
|
PE, light epidural, wash uterus, remove placenta, remove uterine edema (sulfa-urea powder or powdered sucrose), elevate uterus, replace cervix 1st, then uterine body, then horn
oxytocin injection: contraction of tract to prevent recurrence, vulvar suture, systemic ABs |
|
|
uterine prolapse: sheep
a. signalment b. signs c. tx |
a. older (5-7 yo) over-conditioned ewes
b. same as cow: usually recumbent, exposed uterine mucosa (dirty), enlarged & edematous uterus -usually only gravid horn prolapses c. similar to cow (easier), recurrence more frequent: may recommend salvage |
|
|
What is the tx for uterine prolapse in the horse?
|
tranquilize & sedate
cleanse w/ povidone iodine sol’n epidural if needed reduce as in cow oxytocin after replacing uterus: may cause colic ABs for 3-5 d.: intrauterine, systemic may cross-tie mare to keep her standing early on exercise to ↓ edema |
|
|
What is the tx for uterine prolapse in pigs?
|
true emergency: will self-mutilate uterus, become shocky rapidly
replace via L flank laparotomy: replace 1 horn at a time follow up w/ vulva suturing & oxytocin administration severe uterine damage may indicate hysterectomy |
|
|
What is the tx for uterine prolapse in dogs &cats?
|
one horn may prolapse while other horn remains gravid
prone to self-mutilation may be reduced by external manipulation if edema & necrosis not severe else, laparotomy + external & internal manipulation if replacement not possible: OVH |
|
|
subinvolution of uterus
a. species affected b. time when occurs c. pathogenesis |
a. dog
b. 3 d. to 3 wks postpartum c. occurs when post-parturient uterine contraction is incomplete & placental fluids & debris retained in uterus: uterine inertia, muscle fatigue -incubation of uterine materials --> protein breakdown & formation of materials that when absorbed & excreted via milk caused dz in pups -usually involves both horns |
|
|
subinvolution of uterus
a. signs in pups b. signs in mom c. dx |
a. restlessness, crying, bloating
b. normal physical appearance w/ reddish-brown vulvar d/c c. abnormal involution detected by abdominal palpation or U/S -uterus 2x normal size: may find 1 horn or segment enlarged -consistency depends on amt. of fluid present |
|
|
subinvolution of uterus
a. tx b. prevention |
a. remove pups fro 24-36 hrs: no longer
ergonovine PO for 7-10 d.: causes uterine contractions w/o need for estrogenic priming -can also use oxytocin systemic ABs for 7-10 d.: Ampicillin, Amoxicillin, or Cephalexin b. high quality, balanced nutrition during gestation, ↑ plane of nutrition 10 d. prior to whelping adequate exercise, esp. during last month of gestation |
|
|
subinvolution of placental sites
a. species affected b. time when occurs c. pathogenesis |
a. dog
b. 3-12 wks. post-partum c. exact etiology unknown: trophoblastic cells in placental sites persist & preclude normal involution |
|
|
subinvolution of placental sites
a. signs in pups b. signs in mom c. dx d. tx |
a. normal
b. serosanguineous vulvar d/c w/ blood clots; may see periodic spotting for 12-15 wks postpartum, otherwise normal c. hx & PE, confirm w/ vaginal smear -abdominal palpation: multiple firm, spheroid enlargements along length of uterus, little to no fluid -syncytial trophoblast like cells (multi-nucleated, vacuolated) may be found on vaginal smear: 30-40% of time d. if eating & acting normal: no therapy needed -d/c usually gone by 12th to 13th wk postpartum may treat w/ medroxyprogesterone acetate: hemorrhage stops in 24-48 hrs but starts again once tx stops |
|
|
What are some causes of uterine rupture?
|
occurs spontaneously or 2° to: abortion, dystocia, emphysematous fetuses, chronic peritonitis w/ uterine adhesions (esp. mare), uterine torsion, hydrops, trauma, oxytocin administration
|
|
|
What is the tx for uterine rupture?
|
C-section
OVH: cat, dog, sow, small ruminants (usually a salvage procedure in food animals) tx for peritonitis: systemic ABs, NSAIDs may lead to uterine adhesions --> fertility problems, birthing problems monitor horse for laminitis |
|
|
What is the recommended protocol for pregnancy diagnosis in horses?
|
12-16 d: rectal palpation & transrectal U/S
14 d: twin detection & intervention 25 d: heart beat detection mid/late gestation: recheck using transabdominal U/S &/or estrone sulfate assay to check for fetal viability |
|
|
What are the 4 positive signs of pregnancy in cows found via rectal palpation?
|
fetal membrane slip (> 30 d): chorioallantois slips thru fingers
amniotic vesicle (28-60 d): spherical, turgid placentomes (> 75 d) fetus (> 65 d) |
|
|
What is the recommended protocol for pregnancy diagnosis in the cow?
|
rectal palpation > 35 d. post-breeding OR
U/S at 24-27 d. OR BioPRYN (bovine pregnancy specific protein B): > 30 d. |
|
|
What is the recommended protocol for pregnancy diagnosis in sheep & goats?
|
U/S: transrectal if < 35 d., transabdominal if > 35 d.
|
|
|
What is the recommended protocol for pregnancy diagnosis in the pig?
|
teasing w/ boar
U/S: 25-32 d. |
|
|
What is the recommended protocol for pregnancy diagnosis in dogs & cats?
|
20-30 d.: abdominal palpation, U/S
radiography: bitch: > 45 d., queen > 40 d. relaxin (> 30 d.): bitch |
|
|
When can abdominal palpation be used to dx pregnancy in dogs & cats?
|
embryonic vesicles: multiple 1-4 cm swellings in uterus
bitch: 3-4 wks queen: 18-22 d. (easier to palpate) hard to isolate after 30 d.: confluence |
|
|
timing AI: goat
a. timing of insemination b. method of depositing semen c. site of semen deposition d. length of estrus |
a. 12-24 hrs. after onset of estrus (double breeding 12 hrs apart may improve conception rates)
b. vaginally via speculum c. deep cervical d. 18-36 hrs |
|
|
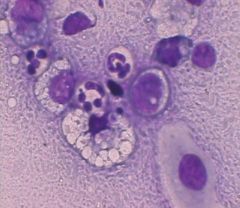
pyometra
|
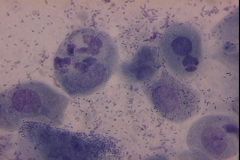
What is the pathologic condition in this canine vaginal smear?
|
|
|
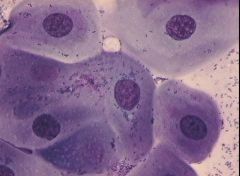
proestrus
parabasal, small intermediate, large intermediate, superficial, RBCs |
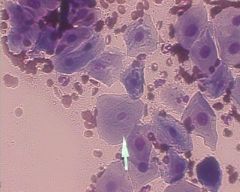
What stage of estrous cycle is present in this dog & what types of cells are present?
|
|
|
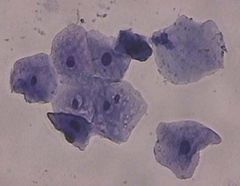
anestrus
parabasal cells |
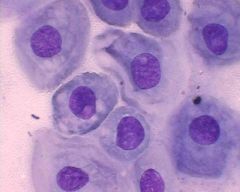
What phase of the canine estrous cycle is shown here & what is the predominant cell type?
|
|
|
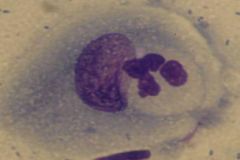
foam cells
late diestrus, anestrus |
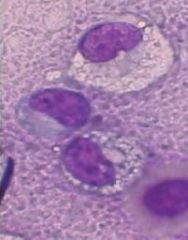
What type of cell is shown & with what parts of the canine estrous cycle are they related?
|
|
|
estrus
|

What phase of the canine estrous cycle is shown here?
|
|
|
estrus
|
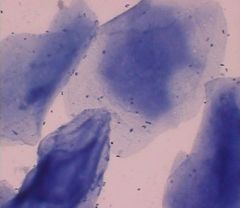
What phase of the canine estrous cycle is shown here?
|
|
|
early diestrus
WBC, bacteria |
What phase of the canine estrous cycle is shown here & what cell type is present?
|
|
|
diestrus day 2
|
What phase of the canine estrous cycle is shown here?
|
|
|
diestrus day 1
|

What phase of the canine estrous cycle is shown here?
|
|
|
estrus
|
What phase of the canine estrous cycle is shown here?
|
|
|
chronic vaginitis
|
What pathologic condition is demonstrated on this canine vaginal smear?
|