Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
|
What are the five systemic diseases in this lecture?
|
Sickle cell nephropathy
Amyloidosis Light chain disease HIV-associated nephropathy Cryoglobulinemia |
|
|
What do many 60% of patients with hgb SS disease (sickle cell) have over 45 years?
What will a small minority (4-12%) develop? |
Microalbuminuria
ESRD |
|
|
What results in polymerization of deoxygenated hemoglobin S and subsequent sickling of erythrocytes?
|
Relative hypoxia (partial pressure of oxygen 10-35 mmHg), acidosis, and hyperosmolarity of inner medulla
|
|

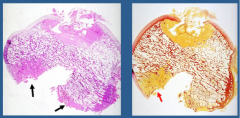
What is shown in each?
|
Injection micrographs:
A = no hemoglobinopathy (visible vasa recta) B = sickle cell trait (cortical vasculature decrease, vasa recta attenuated and distorted) C = sickle cell disease (decrease in cortical vasculature, vasa recta absent) |
|
|
What will you see clinically in sickle cell nephropathy?
|
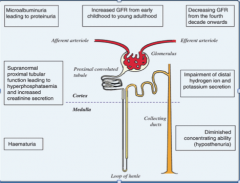
Microalbuminuria --> proteinuria
Hyperphosphatemia and increased creatinine secretion Increased GFR early childhood --> adult, decreasing GFR from fourth decade onward Impairment of distal H+ ion and K+ secretion Diminished concentrating ability (hyposthenuria) |
|
|
What is seen in the earlier stages of sickle cell nephropathy?
Later stages? |
Glomerular hypertrophy, hemosiderin deposits, focal areas of hemorrhage or necrosis
Interstitial inflammation, edema, fibrosis, tubular atrophy, papillary infarcts |
|
|
What is seen in end stage sickle cell nephropathy?
|
Glomerular enlargement and focal segmental glomerulosclerosis
|
|
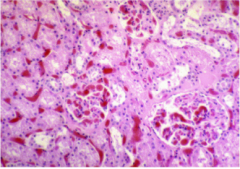
What is shown here? What does sickle cell crisis result from?
|
Sickle cell nephropathy
Glomeruli occluded by sickled red cells Extensive congestion and sickling in peritubular capillaries Sickle cell crisis = sickling in kidney, particularly vasa recta |
|
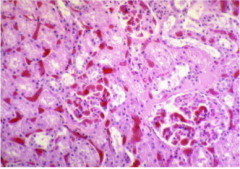
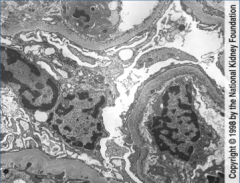
What is shown here?
What will the patient have clinically? |
Sickle cell nephropathy
Glomerulomegaly and mesangial expansion Tubular epithelial hemosiderin accumulation Interstitial fibrosis and vascular stenosis Chronic renal disease and proteinuria |
|
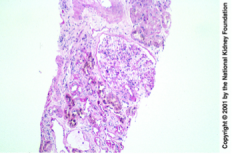
What is shown here?
|

Renal artery thrombosis in sickle cell disease
|
|
|
What is the definition of amyloidosis?
|
Group of chronic diseases characterized by the deposition of abnormal protein in blood vessels and interstitium, eventually leading to organ malfunction.
|
|
|
What is the epidemiology of amyloidosis?
What is the range of severity? |
Uncommon, primarily in late middle-aged and elderly persons, may be primary (most common) or secondary (reactive systemic).
Incidental to fatal |
|
|
Pathogenesis of amyloidosis?
Where is it first deposited? Then where? What does it do there? Result? |
Misfolded proteins (chemically diverse but similar) all folded into beta-pleated sheets
Blood vessel walls --> interstitial --> squeezes cells to death --> organ failure |
|
|
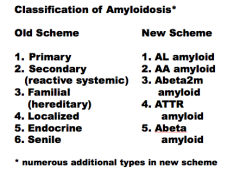
What are the old and new schemes for the classification of amyloidosis?
|
|
|
|
Draw the pathways of amyloid deposition.
|
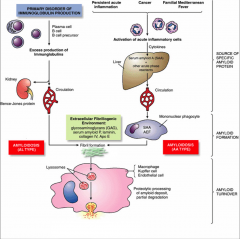
Lymphocyte and plasma cell derived immunoglobin light chains are amyloidogenic in fibrillogenic environment.
Chronic inflammatory disease --> synthesis of acute phase reactants by liver (SAA) --> SAA in presence of AEF released by macrophages and in fibrillogenic environment forms amyloid. Macrophages degrade amyloid --> involved in amyloid deposition and turnover. |
|
|
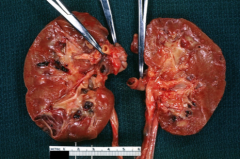
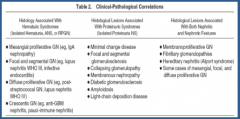
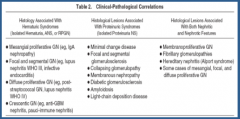
What does advanced renal disease result in?
What will happen to size of kidney? What may predominate? What can tubular and interstitial deposits lead to? |
Nonproliferative, noninflammatory glomerulopathy
Increase Vascular involvement Tubular atrophy and interstitial fibrosis |
|
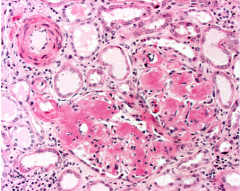
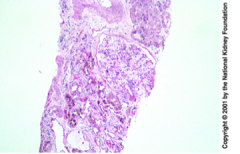
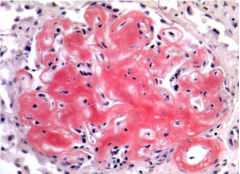
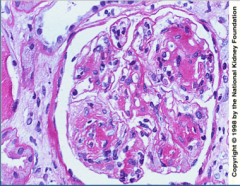
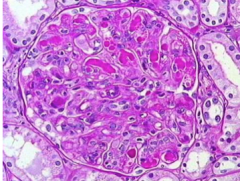
What is shown here? Describe.
|
Amyloid kidney
Amorphous hyaline and eosinophilic |
|
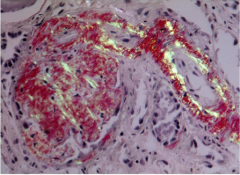
What is shown here? Stain type?
|
Amyloid kidney:
Congo red stain |
|
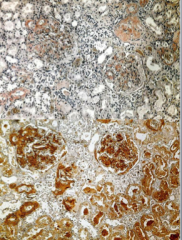
What is shown here? Test?
|
Congo red stain under polarized light = apple green birefringence.
|
|
Can you tell what type of amyloid it is with congo red stain?
What is an immunoperoxidase stain used for (above)? Problems? |
Never
Amyloid A Plagued with false positives and false negatives so becoming uncommon to send off for molecular testing. |
|
|
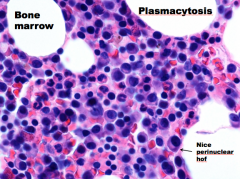
What is the most common amyloid type?
What does it consist of? What is it called in urine? 15% of patients with what disease have this? Most patients will just have what? |
Amyloid L (primary)
Immunoglobin light chains Bence-Jones proteins Multiple myeloma Monoclonal gammopathy |
|
|
Median age of diagnosis of amyloid L?
Symptoms? Kidney changes? |
64 years
Weakness, weight loss, nephrotic syndrome, peripheral neuropathy, autonomic neuropathy Renal insufficiency w/ enlarged kidneys. |
|
|
Are AL patients usually hypertensive?
What other illnesses will you see associated? |
No
Restrictive cardiomyopathy, sick sinus syndrome, myocardial infarction, gastrointestinal dysmotility, malabsorption, hemorrhage or obstruction, bleeding diathesis. |
|
What will most patients with AL eventually develop?
What patients with multiple myeloma are more likely to develop AL? What factors modify the chances of a patient developing amyloidosis? |
Plasma cell dyscrasias, B-cell lymphomas, or multiple myeloma
Those with I chains Amino acid sequence, macrophage activity, and extracellular environment |
|
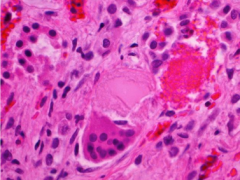
What is shown here? Where do they precipitate and what do they form?
|
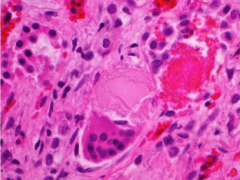
Bence Jones proteins
Precipitate in urine or in tubules Tubular epithelial cells can coalesce into a syncytium around them |
|
|
What is the treatment for amyloidosis--AL?
What about for patients less than 50 years old? What is the median survival time? |
Low dose oral melphalan and dexamethasone
High dose melphalan with autologous cell transplant in patients < 50 years i age 10 months |
|
|
What is reactive systemic (amyloid A) secondary to?
What diseases? What does it consist of? What is acute phase reactant produced by? In response to what? |
Secondary to chronic inflammatory diseases (rheumatoid arthritis, inflammatory bowel disease, or anklyosing spondylitis
Serum A amyloid protein (acute phase reactant produced by liver in response to Il-1 and Il-6) |
|
|
What is main target in AA?
Another common target? How diagnosed? Follows what? |
Kidney
GI tract Renal biopsy Serum AA levels |
|
|
Treatment for AA?
Mechanism? |
Eprodisate
Limits deposition of AA fibrils by interfering with their interaction with tissue glycosaminoglycans Slows renal decline (but not risk of death) |
|
|
What is death from AA usually from?
|
Infection or dialysis related complication
|
|
|
What does amlyoid beta2m occur with?
What does it consist of? Where does it deposit? |
Long term hemodialysis
Beta-2-microglobulin (small molecule, component of MHC class I, normally some in serum) which is not efficiently filtered trough dialysis membrane Synovium, joints, and tendon sheaths |
|

What is shown here? What does it result in?
|
A b2m
Deposition in bone --> destructive arthropathy |
|
What is shown here?
How do the deposits appear? |
Ab2m deposits in a joint
Homogenous pink or yellow Destroying and replacing bone and cartilage |
|
|
What are the two types of amyloid ATTR?
What does it consist of? Where does it form? 4% of what population have a mutated transthyretin? Clinical presentation? |
Senile or familial
Transthyretin Seniele = heart (and pulmonary blood vessels) African Americans Heart failure or arrhythmia |
|
|
What is transthyretin?
|
Serum protein that binds and transports thyroxine and retinol
|
|
|
What is light chain deposition disease?
Will congo red be positive? Does it have fibrillar organization? What does it involve precipitation of and without what? What is it usually associated with? |
Nonamyloid monoclonal Ig deposition disease (MIDD)
Congo red negative No Precipitation of immunoglobulin chain w/o elongation seen in amyloid Multiple myeloma and other lymphoproliferative disease |
|
|
What clinical stuff will you see in light chain deposition disease?
Severity of proteinuria? What syndrome? Renal function? Enlargements? Heart problems? Other random stuff? |
Proteinuria and renal failure
Non-nephrotic range proteinuria w/ tubulointerstitial syndrome Rapidly declining renal function Cardiomegaly, hepatomegaly, conduction disturbances Peripheral neuropathy, GI distrubances, pulmonary nodules, arthropathy, sicca syndrome |
|
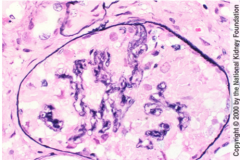
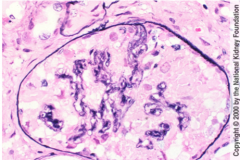
What is shown here?
What does it strongly resemble? |
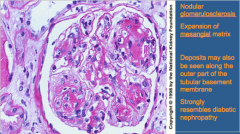
Nodular glomerulosclerosis = characteristic appearance of light chain deposition disease
Diabetic nephropathy |
|
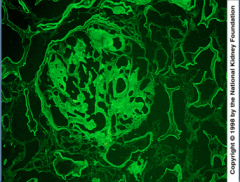
What is shown here?
What is characteristic of this disease? What are the two possibilities? |

Light chain disease -- IF
Glomerular capillary loop, mesangial staining, and LINEAR tubular staining Either kappa or lambda light chain paraprotein (KAPPA MOST COMMONLY) |
|
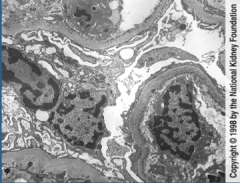
What is shown here?
|
Light chain disease:
Endothelial cell side deposition of material likened to silt...like Mud Island (Nichols) |
|
|
When you have an increased suspicion of light chain disease?
What is the key to diagnosis? When is renal and patient survival better? |
Nephrotic syndrome or rapidly progressive tubulointerstitial nephritis, cardiac diastolic dysfunction, and presence of monoclonal immunoglobin in the urine or serum
Renal biopsy Pure MIDD without cast nephropathy |
|
|
What are the two viral-associate kidney diseases?
|
HIV-associated nephropathy
Cyroglobulinemia |
|
|
What patient population is much more susceptible to HIV-associated nephropathy?
Clinical findings? |
African Americans
Progressive azotemia, significant proteinuria, and minimal peripheral edema in patients with advanced HIV disease |
|
|
What is HIV associated nephropathy classically a form of?
What will you see? What does it result from? |
Focal segmental glomerulosclerosis
Prominent microcystic tubular dilation and interstitial inflammation and fibrosis Podocyte dedifferentiation and proliferation Direct infection by HIV-1 and expression of viral genes Nef and Vpr in renal epithelial cells in genetically susceptible host |
|
|
What may causes susceptibility of African Americans to HIV associated nephropathy?
Why? |
APOL1
G1 and G2 APOL1 mutations = resistance to Tryopanosoma brucei rhodesience (African sleeping sickness) infection as the inhibitor cannot bind to the variant protein. |
|
What is shown here? What is this due to?
|
|
|
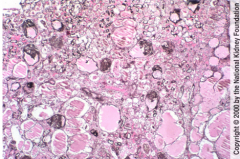
What is shown here?
What is the most common lesion in HIV infection-related renal disease? |
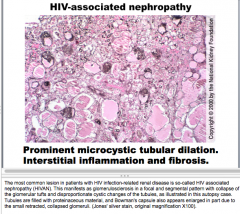
Prominent microcytic tubular dilation.
Interstitial inflammation and fibrosis. Tubules filled with proteinacious material HIVAN (HIV associated nephropathy) |
|
|
What is cyroglobulinema? Clinical findings?
|
Palpable purpura, anthralgia, asthenia accompanied by organ involvement (nephropathy and neuropathy) and elevated serum RF, Ig capable of binding to IgG
|
|
|
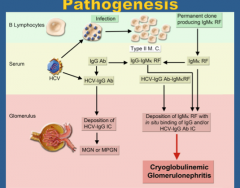
What is mixed cryogrobulinemia associated with?
What type of disorder is it? |
Hepatitis C (90% cases)
B-cell lymphoproliferative disorder -- > deposition of immune complexes containing rheumatoid factor (RF), IgG, HCV RNA, and complement on endothelial surfaces, eliciting vascular inflammation |
|
|
True or false.
Patients with mixed cryoglobulinemia syndrome may be referred to different specialties according to prevalent symptoms. |
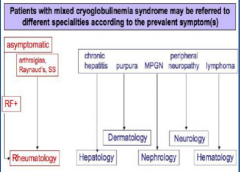
True
|
|
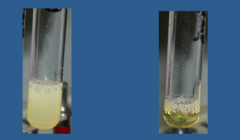
Which is positive, which is negative? Temperature?
|
Left = positive
Right = negative Temp = 4 degrees Celsius |
|
What is shown here?
What can it have in capillary lumens? |
Cryoglobulinemic glomerulonephritis: membranoproliferative pattern
Can have pseudo-thrombi in capillary lumens |
|
|
What is the pathogenesis of cyroglobulin glomerulonephritis?
|
|
|
Summary of lecture?
|
Summary of lecture?
|
|
|
|
|
|
|
|
|
|