Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
725 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
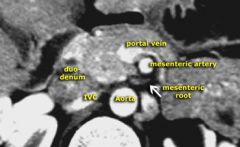
what is distributive shock
|
shock where vasodilation
so drop in SVR - septic shock - anaphal - neurogenic |
|
|
|
Drug treatment
- septic shock (distributive) - anaph (distrib) |
Septic shock: fluids, NE (levafed)
Anap : epi, intub, diphenhyd, steroids neuro : see low BP and low HR, fluids, dopamine or dobutamine |
|
|
|
SIRS
sepsis s shock |
SIRS : meetsSIRS crit (under 50% infected)
Sepsis : SIRS + infected likley severe sepsis: organ dysfx but fluid responsive septic shock: non resp fluids |
|
|
|
cardiogenic shock ?
CO SVR |
low CO
high SVR high wedge cold clammy skin (skin vessels clamp) high JVD If only iso R heart failure just give fluids to inc preload. |
|
|
|
wedge measures
|
nml wedge 6 - 12 mmHg
floats down PArt pulm cap bed pressure L Atrial L Vent end Diastolic OR PRE-LOAD so increases with pump failure |
|
|
|
Cardiac output CO
? nml ? ? how measure ? clinical |
nml 4 - 8 mmHg
CO = SV x HR measure with Swn Ganz thermodilution In MI low SV and low CO, in hemmorr no preload, no SV, no CO. Increase CO: inc contractility, inc HR, inc preload, dec afterload. |
|
|
|
SVR
clinical comparison |
SVR / Body surface area = SVRIndex
nml SVRI 1500 - 2400 SVR vas resist over sys circ aka afterload low in distrib shovk, high in cardiogenic and hypovol shock as vasoconstriction |
|
|
|
shock with
low wedge low CO high SVR |
hypovolemic
|
|
|
|
shock with
high wedge low CO high SVR |
cardiogenic
|
|
|
|
shock with
low / nml wedge high CO low SVR |
distributive shock
|
|
|
|
Pressors
|
NE : strong A2 vasoconst, some B1 HR , ++ SVR +CO, USE sepsis
EPI : strong B1, A1 vasoconst, ++ SVR, Use snaph, Arrest Phenylephrine : A1 vasoconst, Sepsic, neuro, hypo2/2 anesthesia Na nitroprusside : dilates AandV, dec pre and afterload, USE : heart failure with low CO DOPAMINE int dose 5-10 ug/kg/min "Cardiac dose" + DA-R, + heart-R, some A1 to + CO in cardioshock high dose 10-10 ug/kg/min DA, B1, ++ A1 vasocon, ++ SVR to treat cardio or septic shock. dobutamine +B1 B2 to +CO dec SVR to treat cardiogenic shock milnerone: phosph dioester inhib |
|
|
|
ABG vent pulm
ventilation mode to wean / liberate vent |
pressure support often used with IMV
pressure support is set pressure delivered with each breath pt takes (boost) * liberation is taking off vent and may not require weaning first (now not on vents long so lung muscles dont get weak) * taking out ET tube = extubation * removing tracheostomy tube = decannulation |
|
|
|
ABG vent ICU pulm
what is assist control vent ? |
CMV or assist control
* every breath has same volume or pressure, time if pat initiates breath by themselves, they get the full tidal volume given. |
|
|
|
ABG pulm ICU
what is IMV vent |
* spont breathes are allowed between mandatory breaths
* when pt inintiates breath, vent gives pressure support but vol of breath determ by pt effort |
|
|
|
ABG pulm ICU
PEEP - uses - SE |
PEEP/ CPAP
- elevated end expir pressure - keep alveoli open LEVELS : * min 5 mm H2O * ARDS 10-20 cm H2O * COPD 5-10 cm H@) - use CHF, ARDS ** -SE hypotension as decreases PRE-LOAD |
|
|
|
acid base state that keeps patient on a vent ?
|
alkalosis as H+ stimulates resp.
|
|
|
|
AMPLE
|
allegies
meds / mech of injury past med hx / pregnant LAST MEAL EVENTS surrounding mech of injury |
|
|
|
trauma recusiation
amt urine adequete |
adults 0.5 ml/kg/hr ~ 30 ml/hr
child over 1 : 1 ml/kg/hr child under 1 : 2 ml/kg/hr |
|
|
|
head face fracture changes in acute trauma mgt
|
no NGT tube, use OGT tube
|
|
|
|
what is 3 to 1 rule
|
3 crystaloids vol to 1 vol blood loss
|
|
|
|
blood vol in adult ?
|
blood 7 % adult wt
70 kg adult 4.9 L blood Kid 8-9% weight Transfuse: loss half blood volume GIVE FFP when rise PT, PTT to 1.5 nml fibronogen under 100] GIVE PLTS when under 50-17K |
|
|
|
After chest tube for hemothorax
indications for thoracotomy |
1,500 cc drainage from tube at placement
200 ml/hr for 4 hours decomp after intitial stablization ~ 25% hemothorax pts have pneunon also |
|
|
|
sucking chest wound
|
lung collapse on inspiration
init treatment cover with occlusive dressing sealed on 3 sides |
|
|
|
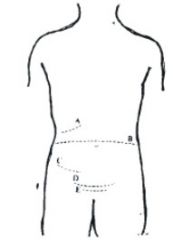
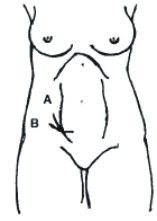
seal belt sign
|
lower ant abdom wall
- perf bladder / bowel - chance fx a lumbar distraction fracture |
|
|
|
blood around umbilicus
|
Cullen sign
peri umbilical bruise hemmor intraperitondeal hemm |
|
|
|
Cullen sign
|
peri umbilical bruise
hemmor intraperitondeal hemm peritoneal viscera: liver, spleen, stomach, sm bowel, sig tranv colon |
|
|
|
grey turners sign
|
flank hemm ( bet ant post axill folds)
retroperitonfeal hemm retroper organs most duod, panc, kidneys, ureters, desc and asc colon , Abd aorta, IVC , renal and splenic vessels |
|
|
|
Kehr sign
|
refer pain left shoulder or neck due to splenic supture
worse in trendelenberg or with LUQ palpation |
|
|
|
FAST looks at what 4 sites
|
morrisons pouch RUQ liver - kidney
splenorenal recess LUQ pouch douglas above rectum for hemopericardium : sub xiphoid and parasternal |
|
|
|
When DPL
|
unstable
sens for hemoperitoneum questionable FAST hollow organ injuries Negatives: 1% risk injury, false postives, no good retroperitoneum Must place foley and decompress stomach first. |
|
|
|
Amer Burn Assoc criteria admid burn center
|
Under 10 yrs or Over 50
2nd 3rd degree > 10% other ages 0ver 20% FT burns over 5 % any age elec incl lightening inhal injury or other trauma too |
|
|
|
fluid lyte requirements in 24 hours
|
per 24 hours you need
Per kg and Per 70 kg person water 35 ml/kg -> 2,100 ml per 70 kg K 1 mEq/kg -> 30 mEq Chl 1.5 mEq/kg -_ 45 mEq Na 1-2 mEq/kg -> 30-60 mEq |
|
|
|
Fluid lyte losses daily
urine sweat resp stool Na and K chl |
Fluid lyte losses daily
urine 25-30 ml/kg/day-> 1,200-1,500 ml sweat 200-400 ml, Has 40 mEq of Na, Cl per liter resp 500-700 ml stool 100 - 200 ml , from colon has mainly potassium 65 mEq liter LYTe losses Na and K 100 mEq Chl 150 mEq Physiol resp hypovolemia : save Na and fluid via renin, aldo, ADH, vasoconst ANGII and symp, low UOP, first tachycardia, then hypotension. |
|
|
|
? third spacing and fluid shifts post op
|
edema or fluid to interstitim
Happens in ileus when fluid leaves bowel post-op. Then day 3 post-op fluid returns intra vascularly and can cause fluid overload. So switch to hypotonic fluid and slow wIV rate. |
|
|
|
surgical cause metabolic acidosis
|
loss bicarb : diarr , ileus, fistula of pancreas or sm bowel so loss of fluid , CA inhibotors
Anion Gap Met Acidosis : SALUD starvation (ketoacids) alcohol lactic acidosis (ischemia, necrotic tissue) Uremia (renal failure) DKA |
|
|
|
surg cause hypochloremic alkalosis
|
NGT suction
loss stomach HCL vomiting |
|
|
|
cause
resp acidosis |
pain
PTX hypovent CNS depress airway obst |
|
|
|
acid/base with NGT suctioning
|
hypochlor hypocalcemic met alkalosis
RX: IVF, Cl/K replacement |
|
|
|
Normal daily secretions
bile gastric pancreas Sm bowel saliva |
Normal daily secretions
bile 1000 ml / 24 hrs gastric 2000 ml pancreas 600 ml Sm bowel 3000 ml saliva 1500 ml almost all secns are reabsorbed REMEMBER BGS (alphabetically) and !L, 2L, 3L |
|
|
|
fluid to replace
gastric NGT suction : duod bile and panc : sm bowel ileostomy : colon diarr : post op p lap : |
fluid to replace
gastric NGT suction : D5 1/2 NS + 20KCL duod bile and panc : LR +/- bicarb sm bowel ileostomy : LR colon diarr : LR +/- bicarnb post op p lap : LR for 24-36 hrs then main |
|
|
|
what lyte causes or worsens ileus
|
* low K
it also worsen dig toxicity it can be caused by low mg also low Na |
|
|
|
# 1 cause post op of low Na
|
fluid overload
|
|
|
|
how treat hyper mg
|
hyper mg is over 2.5
treat ca gluconate IV Sx: resp failure, CNS depression, depressed DTR CAUSES in sx: TPN, renal failure, over IV hydration |
|
|
|
ICU glucose goal
|
80-110
|
|
|
|
Top causes low plts in sx pt post op
|
sepsis
H2 blockers hep massive transf DIC abx spurriius swn ganz Under 20K spont bleed Need over 50K for surgery |
|
|
|
body fluid composition in lytes
hint compare to lyte's conc in plasma |
saliva
Na 10 K 26 Cl 10 HCO3 30 gastric na 60 K 10 cl 130 HCO3 0 ileal (like plasma) Na 140 K 5 Cl 104 Hco3 30 panc (high bicarb) Na 140 K 5 Cl 75 HCO3 115 colon (K ++ higher plasma, and bicar) Na 60 K 30 Cl 40 HCO3 40 |
|
|
|
recus fluid lyte compositions
|
LR
Na 130 K4 Cl 109 HCO3 28 NS Na 154 K 0 Cl 154 HCO3 40 1/2 NS Na 77 K 0 Cl 77 Hco3 0 M/6 lactate Na 167 K0 Cl0 HCO3 167 3% hypertonic saline Na 513 K0 Cl 513 HCO3 0 |
|
|
|
adynamic ileus
|
|
|

aneurysm rupture
|
aneurysm rupture
|
|
|

RUQ pain
vomiting kid |
Appendicolith
|
|
|
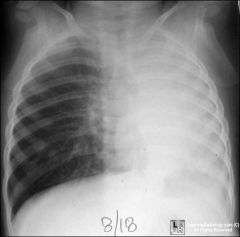
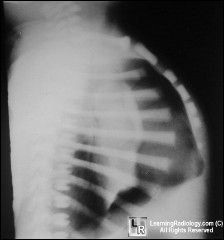
atel L lung due to asthma
|
atel L lung due to asthma
|
|
|

Where ? atel vs PNA
|

Atel LUL
|
|
|

What ?
|
cavitary breast cancer
|
|
|

What ?
|
cecum cancer
|
|
|

What ?
|
esophagus cancer
|
|
|

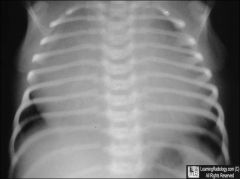
baby
trouble breathing common congen malform |
C CAM
|
|
|

What ?
|
cavitary cancer
|
|
|

|
abscess cavity
|
|
|

|
co arc aorta
figure 3 sign |
|
|

|
Colon polyps
GI |
|
|
What ?
|
diverticula
|
|
|

|
diverticulitis
|
|
|
congenital defect baby
cyanotic |
Ebsteins
|
|
|
problem ?
|
free air under diaph
|
|
|

watery diarrhea that is smelly
gut pain no fever |
giardia
|
|
|

lung Ct
person feels fine |
lung harartoma
|
|
|
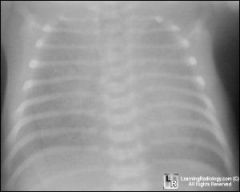
newborn 36 weeks
had to be intubated |
hyaline mmb dz
|
|
|
What is going on ?
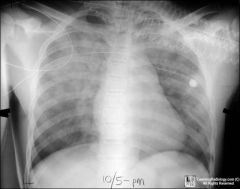
person cant breath post trauma |
hydro pneumo thorax
|
|
|

patient with nephrotic syndrome
gut scan |
hypoalbumenemia
I made up scenario for image |
|
|

name stone
|
jackstone calculus
|
|
|

type of fx
|
jones fx
|
|
|

gut pain
no stool |
localized ileus LUQ
|
|
|

HIV gut pain
|
lymphoma gut
|
|
|

kid
bloody diarrhea |
meckels diverticula
|
|
|

type of fx
|
monteggia fx
|
|
|
|
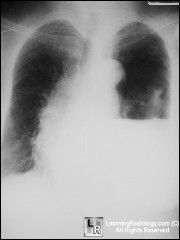
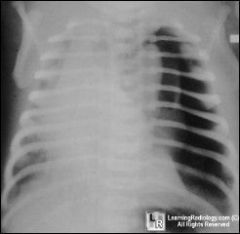
non cardio edema
|
|
|

|
rib osteochrondroma
|
|
|

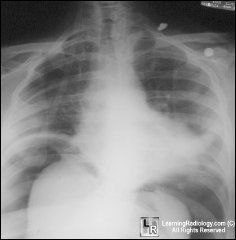
person losing weight
hoarse voice |
pancoast tumor
|
|
|

shot in butt
so do BE |
rectum perf
GI |
|
|

patient post cardiac surgery
SOB |
pericardial effusion
" water bottle sign " |
|
|

what sx do they need ?
|
gall bladder removal as have
porcelain GB and risk cancer |
|
|
What do you need to do ?
|
Tension PTX
Needle to chest |
|
|
What is happening ?
|
Tension PTX
|
|
|

pat with JVD
SOB ascites maybe old guy |
Pulm HTN
|
|
|
chronic lung disease
post surgery on leg fx Now acutely SOB |
lung infarct
|
|
|

had hodkins as a teen
|
radiation fibrosis
|
|
|

problems pooping
|
rectal cancer
|
|
|

|
SBO
sm bowel obst GI |
|
|

gut pain
hands abn tight face skin tight |
scleroderma
|
|
|

50 YO male
small scrape to toe now red and hot |
septic arthritis
|
|
|
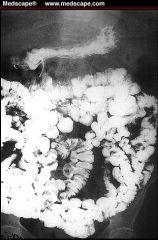
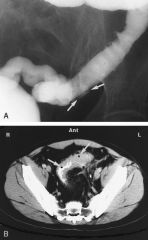
chronic episodes of watery diarr starting as child
skin lesions anemia |
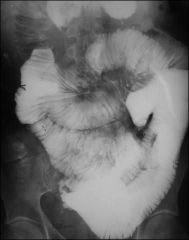
sprue celiac dz
The BEnema shows : spicules edema ulcers biopsy : blunted villa and crypt hyperplasia |
|
|

cough blood
was in jail |

TB
|
|
|
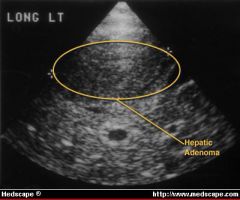
young women, on OCP, RUQ pain.
|

On ultrasound, hepatic adenoma can be seen as round smooth-surfaced mass, slightly more echogenic than surrounding liver.
Ans image is CT with Figure 1. Computed tomographic scan of abdomen showing large intraparenchymal hematoma in the liver measuring 7.5 X 7.5 X 10 cm. Seen also is large subcapsular hemorrhage with evidence of hemoperitoneum. |
|
|
|
female, RUQ pain
|

CT FNHyperplasia : stellate scar, lobulated intrahepatic lesions with central lucency (scar).
|
|
|
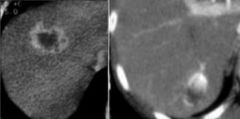
liver mass ?
|
Hemangiomas enhance in BOTH art and venous phases just as bright as aorta.
LEFT: rimenhancement in breast metastasis. RIGHT: nodular discontinuous enhancement in hemangioma. The enhancement of a hemangioma starts peripheral . It is nodular or globular and discontinuous. Rim enhancement is continuous peripheral enhancement and is never hemangioma. Rim enhancement is a feature of malignant lesions, especially metastases. |
|
|
|
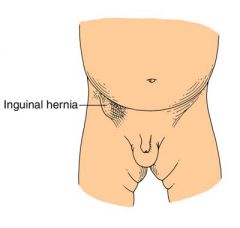
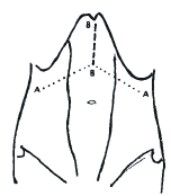
diastasis recti ?
|
DIASTSIS RECTI is not a hernia. Although often confused and at times mis-diagnosed as an epigastric hernia, which it is not, these abdominal wall protrusions occur due to a widened band of non-contractile fascia or tendon normally present between the rectus musles. There is no defect or true hernia present in a normal Diastaasis Recti. Since this fascia does not contract as does normal adjacent muscle, when individuals with DR strain (e.g., do a sit-up), an elongated bulge in the upper abdomen, tappered at each end will appear. This non-tender bulge extends from just below the breast bone, down to the navel. Unlike Epigastric Hernias, a Diastasis Recti is not localized along the linea alba line, but involves the entire space between the breast bone and the navel. They are likened to a narrow foorball in shape. There is no pain associated with this bulge and it is not apparent when standing or walking, but is evident only when straining (sit ups). This is a variant of normal anatomy and Diastasis Recti is not a hernia. Surgery is not indicated for this condition and we disuade ill-advised attempts at surgical correction.
|
|
|
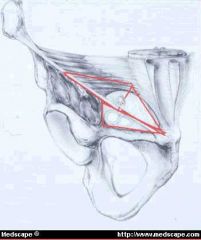
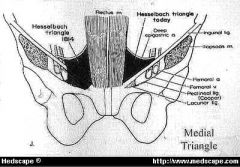
name groin triangles ( 3 )
|
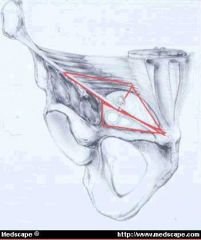
MEDIAL TRIANGLE aka Hesselbach's, Hessert) is bounded by the inguinal ligament, the lateral border of the rectus muscle and the deep epigastric vessels.
LATERAL triangle is bounded by the deep epigastric vessels medially, and by the inguinal ligament laterally to a variable point approximately halfway between the deep inguinal ring and the anterior iliac spine (the lowest point on the inguinal ligament that the internal oblique and tranversus abdominus muscles are fused). The superior boundary is a line connecting that point on the inguinal ligament to the medial reach of the deep epigastric vessels. |
|
|

|
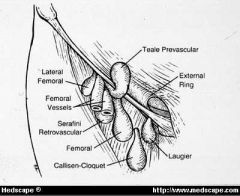
femoral hernia
medial to femoral vessels under inguinal lig Another kind hernia Coopers hernia : thru fem canal and tracking into scrotum and labia majus |
|
|
|
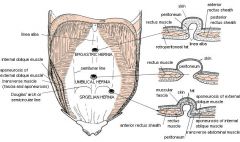
whats spigelian hernia
|
|
|
|
|
|
|
|
|
direct ?
|
|
|
|
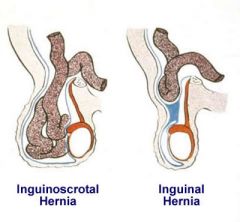
old man hernia
he's a smoker |
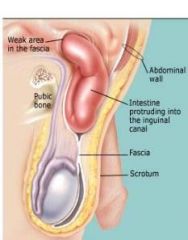
Direct inguinal hernia
men. Rare to strangulate. Does not go into scrotum. Thru transversalis fascia _> post to inguinal canal not in canal. MEDIAL to inf epi vessels. RF: men with chronic cough (smokers), and BPH(strain to pee). |
|
|
|
hasselbach s triangle borders
|
epigastric vessels
inguinal ligament / Pouparts (from int oblique) DIRECT hernia goes thru Hess. Triangle lat border rectus sheath |
|
|
|
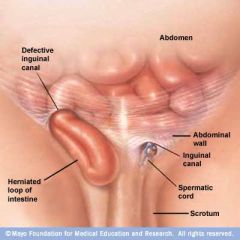
organs in inguinal hernia in boys and girls ?
|
boys sm int
girls ovary/Ftube can see Littre : meckels adrenal rest |
|
|
|
sliding hernia =
pantaloon hernia = |
hernia sac partly made by wall of viscus organ like bladder or stomach
pantaloon = both direct and indirect as starddles inf epigastric vessels |
|
|
|
types lumbar hernia
|
petits rare, inf lumbar triangle
Borders: iliac crest, ext obliq anterioraly, lat dorsi posteriorly grynfelts rare, sup lumbar triangle |
|
|
|
hernia next to an ostomy
|
parastomal hernia
|
|
|
|
richeters hernia
|
only on part of bowel sidewall in hernia sac
|
|
|
|
type diaph hernia
|
morgagni : anterior parasternal
bochdalek : thru post diaph often on left 'de lk' on the left |
|
|
|
hernia with meckels
or appendix |
meckels : littre
rupture appendix : Amyand's |
|
|
|
most common hernia ?
most likley to strangulate ? |
indirect inguinal hernia
5% all men most common in men and women strangulate : femoral > indirect > direct |
|
|
|
indications for lap hernia repair ?
when never use mesh ? |
bilat inguinal
recurring need to resume full activity soon no mesh if infection risk higher |
|
|
|
femoral hernia
who ? how fix ? |
femoral hernia rarest, 5% all
but 85% of these women. MEDIA to inguinal ligament 1/3 incarcerate Repair with McVey using Coopers ligament, mesh plug repair |
|
|
|
women multiparous
recent weight loss Howship Romburg sign : hip flexed, ext rotated and abducted and you feel mass |
obturator hernia, rare
|
|
|
|
omphacele
|
midline
more likley assoc other defects can see malrotation on umbilicus with cord on sac can have liver Rx: Ng decompress, IV abx and IVF, later sx |
|
|
|
gastroschisis
|
no sac
off to side get fluid and lyte abn uncommon to see assoc abn except for intest atresia umbilicus on skin to left of gasro sac |
|
|
|
child umbil hernia ?
|
repair if 2 cm at age 4 to 5
use pants in vest method to close defect in linea alba |
|
|
|
femoral canal borders ?
|
MED " lacunar ligament / Gimbernat
LAT : fem vein ANT : ing ligament Post : Coopers lig / pectineal lig hernia goes thru fem ring |
|
|
|
Patient coming to have sx for indirect hernia needs what pre-op ?
|
rectal exam
COLONOSCOPY !! they may be straining due to colon cancer. |
|
|
|
trauma
rib fractures |
if rib 1 and 2 look for great vessel inj
Rx consv, rest , pain mgt |
|
|
|
PTX
|
tube thoracotomy
if fail to reexpand consider injury to trachebronch tree |
|
|
|
how dx trauma aortic rupture
|
CXR loss of knob**, apical cap, deviated NG tube, HEMOmediastinum.
CT angio TEE Gold is aortagram not CT Angio but most use CT Angio |
|
|
|
blunt cardiac injury presentation ?
|
40% with arrhythmia
45% cardiogenic shock 15% anatomic defects (most die pre-hosp) |
|
|
|
treat bleeding liver
|
first in trauma bleeding liver
pack liver then can try pringle where compress proper hepatic artery between on finger in epipolic foramen/winslow and another anterior to free edge of lesser omentum. |
|
|
|
flail chest treatment
|
first do thoracocentesis to R/O PTX, hemothorax.
Then if no early response early ETT. LAter on can use intercostal blocks for pain. |
|
|
|
emergency airway on person who shot self in face
|
midface injury emergency airway
cricothyROTOMY - needle/percutaneous or surgical Needle thry cricothyroid membrane Using nasal or oral airway can push blood into trachea |
|
|
|
face injury and loss of upgaze ?
muscle |
injury sup rectus muscle or occ inf oblique
|
|
|
|
blunt trauma pericardial tamponade is due to what
|
rupture of myocrdium
or Cor art lacteration |
|
|
|
trauma
becks triad ? |
muffled heart sounds
JVdistension hypotension Signs of pericardial tamponade |
|
|
|
which pentrating chest wounds req abdom exploration
|
below nipples or tip scapula
|
|
|
|
patient
diff blod pressures in blood and feet pulsatile left supraclavicular hematoma left hemotjorax over 500 ml What is gonna happen ? |
imment completion of
traumatic rupture of aorta - falls over 12 feet - head on collision - tbone collision 9% pts have nml CXR GOld is thoracic aortagram TREAT with beta blocker keep systolic under 120 mmHg |
|
|
|
Kehr signs ?
|
pain left shoulder due to diaph irritation from splenic injury
|
|
|
|
Vicryl
|
absorbable
braided loss strength at 2 weeks gone at 4 weeks synthetic |
|
|
|
silk
|
braided
non absorbable |
|
|
|
prolene
|
non absorbable
Used: hernia, vas anast |
|
|
|
monocryl
|
Absorbable
monofilament |
|
|

vert vs hor mattress stirch
|
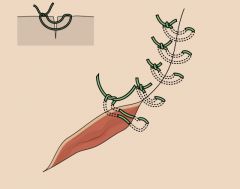
Question showed a horizontal mattress :
hor mattress parallell to wound ABOVE is vert mattress : everts, perp to wound |
|
|
|
Fig. 4. Transverse and transverse-oblique Incisions. A. Kocher incision. B. Transverse Incision. C. Rockey-Davis incision. D. Maylard incision. E. Pfannenstiel incision
|
|
|

|
kocher subcostal for gb open sx
|
|
|
|
The incision may be continued across the midline into a double Kocher incision or roof top approach (Chevron Incision) (Figure 6), which provides excellent access to the upper abdomen particularly in those with a broad costal margin (Chute et al, 1968; Brooks et al, 1999). This is useful in carrying out total gastrectomy, operations for renovascular hypertension, total oesophagectomy, liver transplantation, extensive hepatic resections, and bilateral adrenalectomy etc (Chino & Thomas, 1985; Pinson et al, 1995; Miyazaki et al, 2001).
|
|
|
|
mcburney
1/3 from ant sup il spine to umbilicus for appy |
|
|
|
bassini hernia repair
|
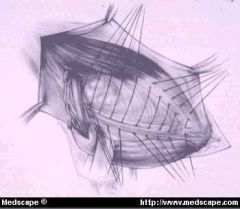
Figure 13. Modified Bassini. The posterior wall is not opened. Sutures placed between the transversus arch aponeurosis and conjoint tendon to the inguinal ligament create tension on the tissues approximated.
Needs relaxing incision. |
|
|
|
lichenstein hernia sx
shouldice canada |
tension free with mesh
shouldice : imbrication uses 4 layers muscles, conjoint to inguinal |
|
|
|
Potassium is over 6.5
|
Why :
alkalosis Rx: Ca Bicarb dialysis insulin and dextrose albuterol lasix kayexolate |
|
|
|
ileus,weak, tetany
N/V paresthesia RF: diuertics, some abx, steroids, alkalosis, diarr, intestinal fistula, NG aspiration, vomit, insulin, amphotericin |
Potassium under 3.5
ECH flat t waves u waves, Rapid Tx, IV KCl IV Max periph 10 mEq hr try treating low mg |
|
|
|
seizure confusion
stpor pulm edema or periph edema tremor paralysis RF innadequete hydration, diuersism Vomit, diarr, tachypnea, TPN |
Hypernatremia Na 135 - 145
TReat D5W 1/4 NS or 1/2 NS slowly hydrate If over do it SEIZUURES not cental pontine myelosis !! |
|
|
|
Treating hypernatremia to fast causes what ?
|
seizures
|
|
|
|
treating hyponatremia too fast causes ?
|
central pontine myelosis
|
|
|
|
seixure coma
N/V ileus lethary confusion weakness |
low Na
Can be hypovol, euvol, hypervol Post op usually vol overload. |
|
|
|
SIADH what about Na level ?
|
SIADH Sodium level is always down here
LOW |
|
|
|
acute treamtent hypercalcemic crisis
what are ecg signs |
1. vol expand with NS
2. diuresis furosimide. ECG short QT, prolong PR |
|
|
|
hypoalbuminemia
- how calculate Ca level in - surg causes |
(measure alb level) x 0.08 then add this to measured Ca level
surg causes : short bowel intest bypass, sepsis, pancreatitis ECG: prolonged QT and ST, TREAT: Ca gluconate IV. |
|
|
|
high blood glucose
low |
high sx cause: DM, infection, TPN, drugs, drawing over site, somat-oma, glucoma
low:liver failure, ad insuff, gastrojejunostomy |
|
|
|
labs to assess O2 delivery
|
* SvO2 : = mixed venous oxy sat which is O2 in blood of RV or pulm art so indirect measure supply and demand.
* lactic acid * ph * base deficit |
|
|
|
frank starling curve
|
CO increases with increasing preload up to a point.
|
|
|
|
In ARDS what do want vent to be
|
LOW TIDAL volume so 6 cc/kg ideal body weight
|
|
|
|
cause CO2 retention
|
hypovent
inc dead space inc CO production (hypermetabolic state) |
|
|
|
bad SE PEEP
|
dec COutput
esp with hypovolemia dec compliance with high PEEP barotrauma fluid retention high ICP |
|
|
|
nml ph and Pco2 values
|
ph 7.35 to 7.45
PCO2 35 - 45 35-45 rule |
|
|
|
liver cyst
high eosinophils cyst may have calcified walls |
NEVER ASPIRATE
hydatid cyst echoncoccus from sheep, cat dog travel usually asympto, incidental finding Rx: albenadole then resect |
|
|
|
liver cyst
anchony fever high WBCs high LFTs guatmalan homosexual veteran alcoholic now living in VA institution W/U what is it ? treat ? |
Amoebic abscess "anchovy paste"
w/u ct or us SEROLOGY Bug is entamoeba from intestine Rx first with Iv metro. Do not drain in OR unless do not resolve or super infected with bacteria |
|
|
|
liver cyst
high WBCs high LFTs #1 cause |
pyogenic
treat IV antibiotics and percutaneous drainage with U/S and CT drainage No OR unless multi and loculated. |
|
|
|
things that are in right lobe
|
cysts congenital many small ones
cysts hyatid from echinococcus cavernous hemangioma right posterior |
|
|
|
how can you tell
liver adenoma from FNH |
USe tc-99 study
And FNH uptakes sulfer |
|
|
|
treatment FNH ?
|
resect only if symptomatic
|
|
|
|
treatment adenoma ?
|
resect all
|
|
|
|
Diverticulitis scan of choice
|
abdom CT
never colonscope or enema |
|
|
|
When to operate diverticulitis
|
Under 40
not better in 72 hours with antibiotics immunocompromised patients 2 or more episodes have electie resection later Complicated diverticulitis : abscess, perf with peritonitis, |
|
|
|
diverticulitis surgery
|
* primary anast if no poop leak
* if pt hemo unstale, hartman, colostomy, close rectal stump. later on re anastmosis * if just local perf with abscess try antibtoics or percut drainage and later surgery |
|
|
|
how work up if fistual from divertic
|
barium enema, ct, sigscope
cystoscope vag exam |
|
|
|
most common gi fistula
|
bowel bladder from diverticulitis
|
|
|
|
surgery nutrition
respitory quotient what can be done to decrease CO2 production/retention in patient on a vent ? |
increase fat decrease carbo calories given.
|
|
|
|
serum markers of nutrition in order of timingq
|
prealbumin t1/2 2-3 days
transf 8-9 days albumin 14-20 days total kymoh count anergy retinol binding ptn 12 hrs |
|
|
|
vit a def ?
chromium |
no vit a : poor wound heal
no chromium : diabetic state |
|
|
|
pt TPN
poor wound healing alopecia dermatitis taste disorder |
zinc def
|
|
|
|
patient on TPN
dry flaky skin alopecia |
fatty acid def
|
|
|
|
state of shock ?
HR 130 RR 31 BP 80/50 confused |
class III
30-40% |
|
|
|
state of shock ?
mild anxiety normal vital signs |
class I hemmorage
under 15% blood loss |
|
|
|
state of shock ?
BP 110/50 HR 105 RR 24 |
class II
15 - 30 % blood loss nml systolic BP decreased pulse pressure tachycardia tachypnea anxiety |
|
|
|
state of shock ?
HR 145 BP 70/50 RR 36 confused lethargic no urine output |
class IV
over 40 % |
|
|
|
dypnea rales
pulsus alternans (pulse increased with greater filling after weak pulse) loud P2 part of S2 gallop hypotension low CO low UOP |
cardiogenic shock
|
|
|
|
post injury thrown from car
hypotension bradycardia |
neurogenic shock
|
|
|
|
bacteria that cause infection in wound in first 24 hours
|
strep
closotridium |
|
|
|
what does abscess look like on CT
|
only post op on day 7, takes that long.
fluid in fibrous rind. gas in fluid collection. |
|
|
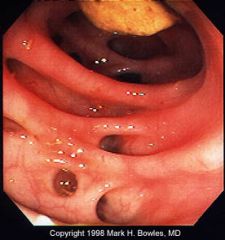
name
|
diverticulosis
thick mural wall grey narrow contrast in lumen black dot is gas in wall which is wall abscess |
|
|
|
steroids
- vit to help healing ? - what stage of healing ? |
vit a helps corticosteroids pts
helps inflammation stage |
|
|
|
how long do you hold ASA
|
10 days
|
|
|
|
spinal anesthesia
where ? SE? |
thecal
SE urine retention hypotentsion (neurogenic shock) |
|
|
|
regional anesthesia
|
spinal afferant from region
like radial nerve block lido bupivocaine/marcaine |
|
|
|
rapid seq anesthesia steps
|
pre ox and short acting induction agent ( prop, midozolam, Na thiopenta)
muscle relax cricoid pressure intubate inhalation anesthetic RApid to dec risk of aspiration ! |
|
|
|
Contraindication to Succ choline
|
burns
NM trauma or paralyzing diseases eye trauma (it inc eye pressure) or increased ICP (it inc K) |
|
|
|
lidocaine
- signs of OD -why add Na bicarb to lido |
- signs toxicity : tinnitus, perioral numb, metal taste, blur vision, muscle twitch, drowsy as large overdose (10 mcg/ml) seizure, coma, respa rrest, LOC, apnea
- bicarb dec burning as lido is acidic Note, it wont work in abscess |
|
|
|
CI nitrous oxide
|
PTX
SBO |
|
|
|
why can you get low BP from morphine ?
SE mepiridine ? How treat low RR from both ? |
histamine
mepiridine SE : like morphine but less phinter spasm, but normepiridine seizure and tachycardia Use naloxine for low RR from both. |
|
|
|
epidural anesthsia
advantage SE |
epidural
Advantage : no dec cough reflex SE: ORTHOSTATIC hypotension dec motor fx, urine retention, remove foley after epidural cath removed or likely urine retention |
|
|

vasc
|
Terminology
Several different terms are used for the chronic symptoms that can occur after a deep vein thrombosis: 1. Venous stasis syndrome 2. Postthrombotic syndrome 3. Venous insufficiency syndrome 4. Postphlebitic syndrome These terms all describe the same symptom complex. What is it? Clots in the deep veins (DVT) lead to an obstruction of blood outflow from the legs or the arms back to the heart. When the body tries to heal from these clots the valves in the veins are often damaged. However, functioning valves are needed to prevent blood from pooling in the legs. Following a DVT the obstruction of the vein and the destruction of valves lead to impaired blood flow from the extremities back to the heart. If a vein is completely blocked, neighboring smaller veins may enlarge to bypass the obstruction. These bypassing veins are called collaterals and can get quite large, particularly in the pelvis and abdomen in patients with thrombosis of the big vein in the abdomen (= inferior vena cava). Such collaterals can sometimes be seen as prominent veins underneath the skin. If good collaterals have formed, symptoms of leg swelling and pain are often not present or are only mild. However, in some patients collaterals do not get all that big and can not carry all the blood needed to drain the legs or arms; this then leads to chronic arm or leg swelling, pressure and pain. Who develops it? Patients who have had a DVT may or may not develop the venous stasis syndrome. Typically, the more extensive the DVT was, the more severe the syndrome will be. However, this is not always so: patients who have had very extensive acute DVTs with severe acute symptoms may recover completely and may not be left with any chronic symptoms. Approximately 60 % of patients will recover from a leg DVT without any residual symptoms. 40 % of patients will have some degree of postthrombotic syndrome, ca. 4 % of patients severe symptoms. The symptoms of postthrombotic syndrome usually occur within the first 6 months, may be up to 2 years after the clot. If a patient has done well for ½ - 2 years after the clot it is highly unlikely that he/she will develop the postthrombotic syndrome. In patients with arm DVT postthrombotic syndrome develops in approximately 15 % of patients. Patients with DVT of larger veins, i.e. those in the shoulder and upper chest area (in medial terms "axillosubclavian DVT") and left-over clot (residual thrombosis) appear to be at particular risk for postthrombotic syndrome, whereas arm clots associated with catheters are at lower risk. Little is known as to who will develop chronic symptoms and who won't. However, it is known, that patients with DVT who wear daily compression stockings (see below) for several month after the acute DVT will develop significantly less venous stasis syndrome. It is, therefore, important to wear individually fitted compression stockings if there is any leg swelling, beginning within days of the diagnosis of the acute DVT. They are typically worn for several months, if not years. Symptoms * chronic leg swelling * chronic (or waxing) pain * diffuse aching * leg heaviness * leg tiredness * leg cramping * dark skin pigmentation (=postthrombotic pigmentation; figure) * hardening of the skin * skin dryness * formation of varicose veins * skin ulcer (stasis ulcer) |
|
|

vasc
Name ? Pt has heart dz, DM, smokes |
venous stasis ulcer
Loc : medial malleolus Assoc : skin changes with statis dermatitis like thick scaly skin, pigementation, Characteristics • Ruddy color base • Surrounding skin is reddened or brown • Shallow depth • Irregular wound margins • Moderate to heavy exudate • Pitting or non-pitting edema • Skin temperature is warm to the touch (normal) • Granulation tissue is present • Infection is not common • Minimal pain (unless infected) • Peripheral pulses are present and palpable • Capillary refill is normal • Usually located near the ankle or lower calf |
|
|

vasc
Pt is a smoker, high fat/chol diet HTN, heart dz, DM, obese, RA |
Chronic art insuff :
- tissue necrosis and / or ulceration - Pulselessness - Painful ulceration bullet - Small, punctate ulcers well circumscribed - Cool or Cold skin - cap refill over 3 secs bullet - shiny, thin, dry skin and Loss of digital and pedal hair Location : top of the foot. smaller arterial vessels is more difficult to address. |
|
|

name mallipati class
|
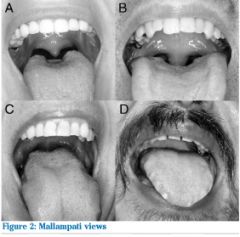
A class I see fauces, ant post pillars, uvual
B class II palate, fauces, base uvual C class III palate, only base of uvula D class IV cant see palate |
|
|
|
Pre-Op finding on cardiac auscultation linked to ischemia, MI, sudden death ?
|
aortic stenosis
thrill over R sternal border cresendo-descc SYSTOLIC 2nd R intercostal space murmur, radiates to carotids L V heave of lift from LV hypertrophy Need CXR, ECG, echo, maybe cath as need operation for new valve. SX: Syncope, angina, dypnea |
|
|
|
CV
Aortic stenosis indicaton for repair |
symptoms
OR valve Xsxn area under 0.75 cm2 and/or gradient over 50 mmHg Note: loud murmur sign of big gradient or big LV |
|
|
|
cv
mech vs non valve |
mech durable but need life anticoag
|
|
|
|
what is + stress test pre-op ?
what is a bad echo ? |
ST depression over 0.2 mV
poor response HR to low BP or stress echo bad : aoric stenosis, or EF under 35% echo sens but not very specific REVERSIBLE defects more concerning |
|
|
|
Risk of MI in non cardiac sx
|
GOldman
High : h or EG evidence infact, angina, or angio CAD, prior CABG Intermed : evidence non heart atheroscledfosis Low no clinical athersclerosis but high RF profile negibible : low Rf profile Numbers: no prior MI 0.1-0.6 Mi in lat 6 months : 4% prior cabg 1.2 |
|
|
|
CHF
CAD valve need endocarditits prohy |
CHF: risk P edema
CAD : 3x risk death, if need CABG first wait 30 days, death in 3 days asympto MI Valve: Aortic stenosis under 1 cm and gradient over 50 mmHg, do echo, maybe new valve first endocarditis : mod risk hypertrophic myppathy, Tet, fake valve |
|
|
|
treat post op urine retention
|
- ensure fluid rescus
- straight cath twice 6 hrs apart, then foley if no pee - can try prazozin or penoxybenzomeine |
|
|
|
stages of guts return to action
|
sm int
stomach colon |
|
|
|
plt needs
how much a bump with one unit ? |
normal over 150 k
unlikley to bleed 100-150k 20-50 possible excess sx bleeding 10-20k spon muscosal and curt bleed under 10 k spont bleed and in GI one plt unit bumpps 5 - 10k |
|
|
|
nutr
labs indicate malnutrition ? inc sx risk ? |
alb under 3
trans under 150 under 80% IBW or over 120% IBW recent change over 10% |
|
|
|
real time to be NPO pre-op
|
To dec risk aspiration with intubation
- solids 6-8 hrs - fluids 2-3 hrs |
|
|
|
when hold warf pre op
|
3 choices :
- avoid 3 days pre, start again POD#2 - admit preop , change to hep and hold few hrs preop - change LMW heparin |
|
|
|
thyroid meds
|
give thyroid replacements on day of sx, ok to hold post-op a day pr 2 as t1/2 7 days.
thyroid antagonist hold on day of sx |
|
|
|
wound healing
what impairs collagen stage |
vit c def
ptn calorie malnut |
|
|
|
classic example of delayed primary closure of surgical wound ?
|
ruptured pus full appendix
- close periotoneumm fasica and give abx - use secondary intention as wound dirty and risk infection HIGh - sub cut tissues not sutured until 3 to 5 days later |
|
|
|
- magic number for wound infection risk
- type of pressure inn OR |
> 10 5 microorgs dose
- postive pressure - sterile parts of body: lower Resp, upper urinary |
|
|
|
sm bowel bugs
normal flora |
strep
enterbacteria bacteriodes very low lactobacilli |
|
|
|
lg bowel bugs
normal flora |
bacteriodes
enterobacter ( ecoli, kleb, salm) s aureus, clost |
|
|
|
lower urinary tract
normal flora |
staph epi
strep diptheriods gram neg rods |
|
|
|
patient
post mastectomy skin flap swelling |
seroma as lymph channels disrupted
aspirate (unless it is in groin) and place drain do inc risk infection as feed bugs |
|
|
|
patient with incisional hernia
abd pain, N, V |
OR ASAP
may strang bowel repair fascia +/- mesh no mesh if infected |
|
|
|
when is tape CI
|
active bleeding
complex surface perimeum tape >> staples > sutures |
|
|
|
calcium and ph
|
acidosis increases ionized fraction
alkalosis, hyperventilation, decreases it |
|
|
|
nutrition
Harris vs Fick for calorie requirements |
Basal Energy expenditure
Harris : estimates BEE Fick catheter equation if have swan ganz: (SaO2-SvO2) xCOxHbx95.18 Males 25 kcal/kg/day females BEE 22 kcal/kg/day KIDS do not use Harris for REE Use kilocal/kg for age using chart of RDA ------- post op : x 1.3 trauma/sepsis/burn x 1.6-2 fever : 12% inc per degree C |
|
|
|
vasc
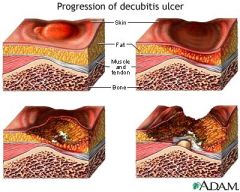
wound STAGES OF decub ulcers |
|
|
|
|
neck injury zones
|
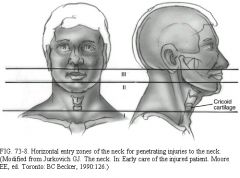
triangles :
anterior and posterior anterior has three zones I : below cricoid III above angle mandible posterior : not much above spin acc nerve, below it subclavian vein, plexus, apices lung treatment: if intubate and no airway: may have laryngtracheal separation and you are in false lumen. So, tracheostomy. CAreful of pneumonhemoPTX at apices lungs. If suspect, and need central line, use femoral or opposite side. Never blind probe neck. Go to OR** zone II with expanding hematoma, and SQ emphy, trachea dev, change voice quality, air bubbles in wound, Subclavian injury: put IVs in legs or opposite arm. |
|
|
|
"sacral sparing"
|
voluntary anal sphinter intact or voluntary toe flex, perianal sensation
sign of incomplete cord injury But sacral reflexes may be preserved in complete transection |
|
|
|
determines ICP ?
What is CPP ? indication to moniter ICP in trauma ? |
- monroe kelly
vol brain vol blood vol CSF - CPP = MAP - ICP - GCS under 9, altered LOC or unconc and muti trauma ir dec consc focal neuro abn |
|
|
|
Use of CN to localize injury in coma ?
|
cornea reflex intact pons
gag intact upper medulla CN6 palsy is often false localizing sign |
|
|
|
how remember which brain bleed is cresect ?
|
sUbdural is cUrved like
cresent |
|
|
|
Rx SAH
|
anti-conv and observe
|
|
|
|
skull fx:
open and closed which need OR |
depressed skull to OR if:
dirty for debriide, severe deform, ipinge brain, open fx, CSF leak If open fx, abx, seiz prophy, surgery |
|
|
|
when to OR for spine fx
|
unstable vertbra
incomplete injury extrinsic compression spine hematoma |
|
|
|
patient post spine surgery
- bilateral loss pain and temp - paraplegia what part of cord ? what happened ? |
Anterior cord syndrome
art adamawitz (enter L1 supply to T4) or compression from FLEXION - pain and temp (Sthal) - paraplegia (CST) still posterior cord so vibr, position |
|
|
|
man stabbed in back
left side paralysis left side loss of virb and position right side loss of pain and temo |
Brown Sequard syndrome
hemisection ipsi motor contra pain temp stab, tumor, |
|
|
|
60 year old man has car crash
whiplash walks ok very weak hand shake |
central cord syndrome
pre-existing canal stenosis like hyperextension weaker in arms > legs hands weaker than biceps |
|
|
|
if steroids are helpful, when
|
non penetrating and within 8 hours
high dose methypred (30mg/kg over 25 min in hour 1) then continuous 5.4 mcg/kg/hr over next 23 hours |
|
|

Patient fell of ladder onto their head
OR anvil fell on head name fx ? stable or not ? |
burst fx or jefferson fx
C1 fx of both sides of ring unstable from axial loading |
|
|

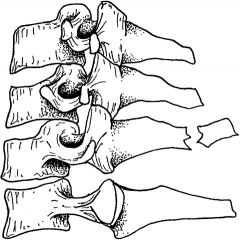
hyperextension injury
|
hangman fracture
C2 (hangman C2, jefferson president so #1) more stable meaning rarely spinal cord injury but treat all as unstable The hangman´s fracture is located in the pedicles of C2, with C2 displacing anteriorly on C3 (Fig. 264-15). The fracture is caused by an extension mechanism and is seen in judicial hangings. Suicidal hangings do not usually cause the extreme hyperextension seen in judicial hangings and do not cause a hangman´s fracture. The same fracture is seen in motor vehicle and diving accidents where sudden hyperextension forces are applied in deceleration. Owing to the large diameter of the spinal canal at the level of C2, even displacement of C2 on C3 may not cause neurologic injury, and these patients may be neurologically intact. This injury is unstable and mandates immediate consultation. |
|
|

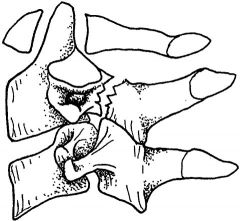
look at C2
|
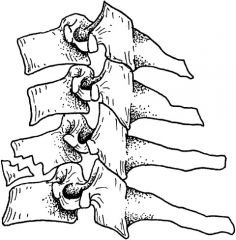
teardrop flexion fx
ant inf vert body chips off like teardrop assoc with tear of post lig so often neuro injury too |
|
|
|
man shoveling snow, heard crunch in shoulder
|
An avulsion of the spinous process of the lower cervical vertebrae, classically C7, is known as a clay-shoveler´s fracture (Fig. 264-7). Intense flexion against contracted posterior erector spinal muscles causes avulsion of the spinous process. An isolated clay shoveler´s fracture is mechanically stable. Conservative treatment with ice, analgesia, rest, and early referral is indicated
|
|
|

Man fell
back pain bruise on lower abdom wall |
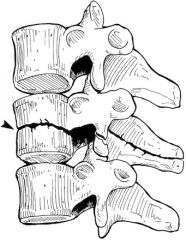
chance fx = distraction of posterior part of vertebra usually lower lumbar, below cord, L1 or L2 (is some ant compression but minor vs post compression)
Originally most often caused by seat belts as hyperflexion injuries , now thorax crush or hyperflex. · Seat belt injuries usually involve the lower thoracic and upper to mid lumbar spine (L1 and L2 most commonly) · Chance fractures are hyperflexion injuries in which there is distraction of the posterior elements and impaction of the anterior components of the spine o Compression component from hyperflexion is usually minor compared to distraction componento SIGN : BACK PAIN, SEAT BELT BRUISE ANT ABDOM WALL *** NEED ADB CT !!!! rare is spine cord transection. o Up to 50% serious blunt injury to internal organs : primarily the pancreas, duodenum and mesentery 0 children may not fx but intestinal and urinary bladder injuries o fx is below cord end but can hit nerves so bowel and bladder signs o die from gut injury |
|
|
|
rectal exam, feel step off
|
coggeal fx, r/o rectal bleed
rx donut |
|
|
|
trauma
how dx pericardial tamponade |
GOLD : direct see via
subxiphoid window sm midline if see injury, do median sternotomy. Cut sac ant and parallel to phrenic N, stuff hole with foley baloon, use 3-0 non absorb sutures, Keys: tamponade relief, vol expland, correct adidosis, perfuse heart, avoid hypothermia chamber injury : LV 40% = RV then RA 24% LA tiny, 3% Also: fast |
|
|
|
diaphragm holes ?
spine levels needed for diaph function ? |
"I 8 10 ECGs at 12"
I = I (IVC) @ 8th vertebra ECG = esophagus at 10th vert A is aorta, azygous, thoracic duct at 12th vert T8 IVC T9 esoph, vagus, T12 aorta, thoracic duct, azygos vein C3 thru 5 keeps you alive |
|
|
|
peritoneal or retro ?
liver |
peritoneal
|
|
|
|
peritoneal or retro ?
spleen |
peritoneal
|
|
|
|
peritoneal or retro ?
duod |
duod :
1-3rd parts retro 4th intra |
|
|
|
peritoneal or retro ?
kidney |
kidney ureter
retro |
|
|
|
peritoneal or retro ?
asc colon |
retro
|
|
|
|
peritoneal or retro ?
trans colon |
peritoneal
|
|
|
|
peritoneal or retro ?
desc colon |
retro
|
|
|
|
peritoneal or retro ?
sigmoid colon |
peritoneal
|
|
|
|
peritoneal or retro ?
sm bowel |
peritoneal
|
|
|
|
peritoneal or retro ?
stomach |
peritoneal
|
|
|
|
peritoneal or retro ?
pancreas |
retro
|
|
|
|
peritoneal or retro ?
aorta |
retro
|
|
|
|
peritoneal or retro ?
IVC |
retro
|
|
|
|
peritoneal or retro ?
renal vessels |
retro
|
|
|
|
peritoneal or retro ?
splanic vessels |
retro
|
|
|
|
peritoneal or retro ?
iliac vessels |
NEITHER !
pelvic like urethra, bladder prosate ovary uterus |
|
|
|
peritoneal or retro ?
rectum |
neither
pelvic |
|
|
|
pt post trauma
neuro intact peritonitis and guarding what do they need ? |
trauma lap now.
no other w/u |
|
|
|
trauma
waht does CT miss |
diaph
colon panc injury |
|
|
|
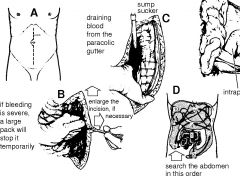
critieria ex lap
|
stomach bleeding
periotoneal irritation dipah injury free air in gut bladder rupture rectal perf confirmed with sig scope transabdom misslepath ------ + DPL,abd trauma hemo unstable evisceration, Ct see injury you can fix in OR, remove impaled thing |
|
|
|
trauma thor
reasonable w/o dipah injury |
cxr (at first nml in half)
upper GI barium enema U s CT MRI CAreful with NGT as esoph gets kinked. |
|
|
|
liver injury
-who might escape OR |
standard is OR
May try non-OR (~half): -very few pentrating stab stable after CT/DPL - try blunt more often - clearly grade and see injury with CRT as grade III or less (hematoma subcapsular, hema parencyma under 75% or under 3 lobes, no vena cava or major hep vein injury, no avulsion - no peritoneal signs - no other inj needing lap - no need blood tx Mgt: serial hct Q4-6hrs ReCt 2-3 days |
|
|
|
Pt post liver lac
Scenario A : upper gi bleed RUQ pain + fecal occult blood jauncide Scenario B: draining bile over 50 mls/day for over 14 days |
A. hemobilia (1%)
try angioembolize B. bile fisula, 7-10%, closes on own with drainage C. also see hyperpyrexia for 3-5 days self lim |
|
|
|
kid with 9th rib fx
left neck/shoulder hurts when you push LUQ Name w/u modality What degree means go to OR ? |
spleen fx
CT great, prescise If unstable, U/S for hemoperitoneum No good: DPL, laparoscopy Therapy: angio embolize if stable hint of may of failing nonOR mgt: . blush on CT Grade III goes to OR : subcap hematomam over 50% area, or parenchyma over 5cm or expanding parenchymal hematoma, or lac over 3 cm or lac into vessels or HILAR injury or devascularized spleen. remove spleen if : "pulverized" shock, otherwise repair/antomic resect. Give pneumo vax day discharge. |
|
|
|
trauma to stomach , sm bowel , and perf
type of wound ? Diagnosis ? |
- wound clean-contam in stomach, gut not dirty until term ileum really
- Dx: Exam for peritonitis DPL or laparoscopy free air on CXR ! note it is CXR Bad choices : CT false-neg OR : stab pylorus : pyloroplasty, stab body fix it. Sm Bowel: most 1 anast, unless nasty then try 2nd look delay anast |
|
|
|
Kid 4 yr old
signs like SBO gets CT/upper GI with water sol con |
See duod bruise
which in kids assoc abuse Rx: NGT decom TPN reeval upper GI 1 week |
|
|
|
man 24 yr
shot in lg bowel bleeding ALOT Rx ? What is lac to rectum ? anus ? |
OR ASAP, skip CT but may show free air, may miss specific injury.
If small perf try repair or small resxn with 1repair CI to ANASt with hemmorage as #1 cause death exsang from other injurys or MOFS or sepsis. Most rectal injury extra peritoneal, + bladder Dx: DRE, RIGID proctoscope (in OR) mandtory of path of knife or bullet thru pelvis Rx: diverting proximal loop colostomy +/- distal limb closure and repair of perf, end col muscus fisuta. Can close colostomy in 3-4 mnths. Anus injury : do sigmoid colostomy |
|
|
|
what can bleed if panc gets shot ?
|
behind pancreas is :
IVC, aorta, L kidney, renal vein, splanic vein, spleinc Art, SMA,, SMV lateral : spleen medial : duod |
|
|
|
pancreas ducts anat
|
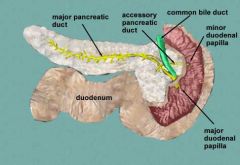
Major duct joins CBD at ampulla where sphincer Oddi is. Then they dump to duod at ampulla Vater.
minpr duct is higher up. |
|
|
|
panc trauma
labs : Dx when take out pancreas ? |
- amylase
- dx: CT : LESSER sac fluid, fluid spleic vein and panc body, retro bleed ERCP, if stable or to eval mised injuries Sx: Whipple or remove panc when duod or panc head devitalized. with distal transxn: take out distal panc, tie ducts. with prox transxn hard, try ext drain and stenting. |
|
|
|
trauma with flank pain and hematuria
OR fluid responsive, distended abd, hypotensive, dec pulses LE, fluid on FAST, missles on KUB |
renal art injury
OR contained hematoma vas injury MGT vascular injuries: recus, prep ct chin to thigh warm, srtop bleeding, if tamponaded get prox and distal control before opening hematoma. if active hemm, get active contrl Comps: vasoenteric fisula |
|
|
|
renal injury
|
contusion : capsule intact, can have hematoma, IVP nml, CT can have edema or micro-leak contrast to renal parencyma; admit hx, no OR
lacL if minor and only cortex watch clolosely, renal fracture/shattered kidney : OR ASAP. kidney rips off. |
|
|
|
airway for 10 year old
face shattered |
NEEDLE cricothyroidomy
a cricothy surgically CI in under 13 yolds recall |
|
|
|
minor extra per bladder rupture
|
foley drain and observe
if intraperio or large need OR closure |
|
|
|
seat belt sign :
3 injuries (one is gut) |
sm bowel L2
pancreas |
|
|
|
blood in pelvis fx is A or V ?
|
90% venous
|
|
|
|
duod injury
|
Duod injury : Dx with upper GI watersoluble con, CT MISSES so does DPL. 1-2nd part of duod more likley fatal
Sx: 1. Most 1 repair, try omentun patch, gastric diversion. 2. pyloric exclusion : close duod injury, staple off pylorus, gastrojejunostomy |
|
|
|
stable parasternal GSW
|
CXR
FAST, chest tube, +/- Or for subxiph window |
|
|
|
in kids, a lab for abd injury
|
ALT ASt
|
|
|
|
Rx myoglobinuria
|
HAM
hydrate IVf Alkalinize urine with IV bicarb mannitol diuresis |
|
|
|
change in fluids burn pts after 24 hrs
|
colloid, D5W and 5% alb : need free water and have cap leak.
also in first 24 hrs never give glu |
|
|
|
What closes ductus arteriosus and what opens it ?
|
closes it : indomethacin
Keeps patent : prostaglandin In fetus desat blood goes thru it. |
|
|
|
arterial switch vs Rastelli ?
|
transpostion of great arteries
egg heart marked pulm congestion on cxr TGA with VSD -> arterial switch before 2 wks old TGA with VSD plus LV outflow obst -> palliative systemic pulm shunt, then Rastelli (aorta reroute internally over VSD, then PA attached to Rv externally) TGA with septium: balloon septosomy of f ovale, then arterial switch. |
|
|
|
surgery for tet of fallot
|
If ratio pulm art to aorta 1:3 one step
ratio under 1:3 2 step: palliative enlarge stenotic outflow (blalock-taussig anast subclav to PA, wateston aortic-pulm anast, potts) THEN corrective procedure. |
|
|
|
balloon dilation for ?
|
pulm stenosis
|
|
|
|
tricuspid atresia sx ?
|
newborn emergency palliation enlg ASD/fovale or systmeic-pulm shunt
Then bidirectional Glenn then Fontan (cavopulm shunt) |
|
|
|
PDA
what drug ? when sx ? |
PDA
indomethacin to close it OR when : premie severe resp insiff refractory indo and then double ligate ductus watchful for L recurr laryngeal, larger kids get a coil in it. infants get more risk endocarditits, pulm HTN |
|
|
|
when OR for VSD
|
most close on own
patch if * CHF not controlled with meds * VSD not closed by 9 mnths old and pulm pressure 2/3 of systemic pressure * if pulm and systemic flow is ovr 2:1 after 4 yrs old Outcome : 1/3 regress pulm vasc resist, 1.3 same, 1/2 gradual dec |
|
|
|
eisenmenger rx
|
only can try heart lung tx
|
|
|
|
heart sx that can result in paralysis
|
co-arc sx as cross clamp aorta
goal to keep occlusion under 20 min distal aortic pressure over 50 mmHg |
|
|
|
norwood sx ?
|
hypoplastic left heart
1. attach PA to arotic arch, resex atrial septum to mix blood 2. later take down shunt, connect atrial to PA via Glenn or fontan. |
|
|
|
neonatal GFR and urine
|
GFR half that of adults
50 ml/min/m2 vs adult 100 urine conc 600 mOsm vs 1200 adults |
|
|
|
nutrition
stress sx hormones do what ? |
hypermetabolism
muscle breakdown faster than normal more gluconeogenesis |
|
|
|
nutrition
where do you see muscle wasting in PE |
interossues fingers
quads temporalis also PE: check lungs PNA, GI look for BS and periotonitis post op |
|
|
|
nutrition
What is total energy expediture ? |
TEE =
1. basal metabolic rate 2. phy activity ~ 10%, more vairable pt in health 3. diet induced thermogenesis (still goes in when TPN ! biochemical) |
|
|
|
nutrition
BMR depends on ? |
health
awake fasting body size BODY composition - lean body mass ** - fat mass - free fat mass ** So not body wt is predictor. Danger is when obese person loses body wt in illness people don't feed as fast as 'dont look thin'. but person losing fat and LEAN body mass. |
|
|
|
nutrition
starving vs stress ptn needs |
stress:
inc ptn needs more muscle ptn breakdown more aa oxid more ACR synth Strav dec ptn needs as metab adapts (slower) dec gluconeogenesis more ketone oxidation ptn go to liver where deamin and then glu to brain for use. |
|
|
|
nutrition
where does nitrogen from ptn get elim ? |
urine
urea |
|
|
|
nutrition
carb use in stress vs starvation |
stress:
inc gluconeogensis inc INSULIN resistance inc plasma glu inc energy needs starvation: less gluconeogensis less energy needs (adapting) |
|
|
|
nutrition
nitrogen balence |
order 24 hr urine
1 g ptn intake has 0.16 g nitrogen So if 40 g ptn in diet 40 g x 0.16 g nitrogen - urine nitrogen - 3g = * For TPN use -3g as adjustment factor. can be a little bit neg, like 0.13ish as in crit ill not going to be + or zero exactly. |
|
|
|
acute abd davis lecture
pain poorly localized diffuse assoc autonomic signs like: -hypotension - sweat - N/V -abd wall spasm TYPE of PAIN TYPE of CAUSE / ORGAN |
visceral pain
- organ with visceral peritonem cover So capsule of organ stretching, distension - chem irritation (gastric or panc enz) - ischemia - stretch of hollow viscus (so NOT liver) |
|
|
|
acute abd davis lecture
Pain sharp , well localized |
somatic
arises near site pathology - abd wall - par peritoneum - root mesentary - dipahragm via ff spinal nerves |
|
|
|
acute abd davis lecture
referred pain teste |
kidney stone
pyelo |
|
|
|
acute abd davis lecture
referred pain supraclavicular fossa / clav region |
dipahrgm
esp left with spleen when push LUQ |
|
|
|
acute abd davis lecture
referred pain scapula |
gallstone
aneurysm (back) |
|
|
|
acute abd davis lecture
referred pain back |
pancreas
abd aneurysm |
|
|
|
acute abd davis lecture
colicky pain ? |
comes and goes
from obst hollow viscus organ as peristalsis waves |
|
|
|
acute abd davis lecture
ulcer pain |
burning pentrating
sharp knife like perf ulcer |
|
|
|
acute abd davis lecture
cyst pain |
mid cycle mittleschmertz / graafian follicle
onset of menses : ruptured corpus luteum cyst |
|
|
|
acute abd davis lecture
peritonitis pt position |
knees and hip flexed
|
|
|
|
acute abd davis lecture
tenderness types rigidity ? |
direct : over inflam local or stretched capsule
rebound : from peritnoeal inflamm crepitis : soft tiss infection (anar) , air leaving pleural space Invol rigidity = from spasm of abd wall muscle, can be uni or bi, +/- tenderness |
|
|
|
acute abd davis lecture
percussion - hyperresonance - tenderness |
- bowel gas OR free air
- tender : infla local or general , distended capsule |
|
|
|
bowel sounds ranges
|
Description
1. Bowel Sounds Normal bowel sounds occur approx. every 5-10 seconds and have a high-pitched sound. If after 2 minutes no bowel sounds are heard, the statement “absent bowel sounds” may be made and suggest a paralytic ileus that is due to diffuse peritoneal irritation. Also borborygmi associated with hyperperistalsis which is common in early acute intestinal obstruction. "hypoactive" is under 3-4 a minute |
|
|
|
succussion splash ?
|
A succussion splash may be detected in a distended abdomen as a result of the presence of gas and fluid in an obstructed organ. The examiner applies the stethoscope over the patient’s abdomen while shaking the patient from side to side. The presence of sloshing sound generally indicates distention of the stomach or colon.
|
|
|
liver span
|
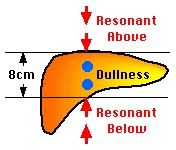
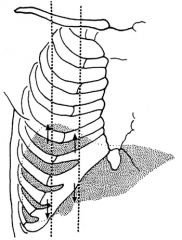
liver span
In the right midclavicular line, liver dullness should be 6 to 12 cm. In the midsternal line liver dullness should be 4 to 8 cm. Bates pg 366 Anonymous The liver span should be 6-12 cm. in the MCL. The liver span should be 4-8 cm in the midsternal line. - Will decreased when there is free air in the abdomen, as from a perforated hollow viscus -The span of liver dullness is increased when the liver is enlarged. Cirrhosis, hepatitis, venous congestion,malignancy. The span of liver dullness is decreased when the liver is small. It may also be decreased when free air is present below the diaphragm as from a perforated hollow viscus.. The span is usually greater in men and in tall people. - A more common cause of overestimating liver size (false-positive measurement) is some form of chronic obstructive lung disease. This makes percussion of the upper border of the liver difficult. Obesity can cause problems in both percussion and palpation. Distention of the colon may obscure the lower liver dullness. This may result in understanding the size of the liver (false-negative measurement). |
|
|
|
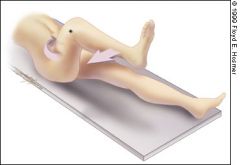
psoas sign ?
|

can also bring leg straight up Key is bring hip posterior.
FIGURE 1A. The psoas sign. Pain on passive extension of the right thigh. Patient lies on left side. Examiner extends patient's right thigh while applying counter resistance to the right hip (asterisk). |
|
|
what is this ?
|
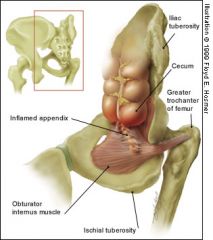
The obturator sign.
Pain on passive internal rotation of the flexed thigh. Examiner moves lower leg laterally while applying resistance to the lateral side of the knee (asterisk) resulting in internal rotation of the femur. |
|
|
|
Diastasis recti ?
|
Diastasis recti- separation of the rectus abdomenus muscle, contents bulge from to form a midline ridge. Repeated pregnancies, obesity, and chronic lung disease predispose to it. No clinical consequences.
|
|
|
|
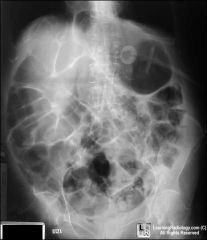
acute abd cope
abdom pain and constipation inc distention little to no vomiting |
lg bowel obstruction
Do plain film before OR, rule out renal failure as uremia causes giant abd distention and vomit |
|
|
|
acute abd cope
male infant screams draws up legs looks pale and ill gets better later on happens again |
intussecption
rectal exam : blood or mucus rectal air enema |
|
|
|
acute abd cope
severe abd pain collapse ridgid wall |
visceral perf
usually stomach or duod -often stomach ulcer erode - can be gb perf or stercoral ulcer colon or rare app rupture |
|
|
|
acute abd cope
severe abd pain collapse ridgid wall then ridgid board like abdomen hr or 2 later pt looks and feels better bit still ridig wall later inc HR, vomit, more distension |
perf gastric ulcer
pain by shoulder has peritonitis can see air under diaph |
|
|
|
acute abd cope
severe RUQ pain / tender and risgid |
acute cholecystitis
leaking duod ulcer (exclude chest with CXR) |
|
|
|
acute abd cope
severe LUQ pain / tender and ridgid |
pancretitis
perf gastric ulcer jej diverticulitis spont spleen rupture leak spelic A acute perinephritis |
|
|
|
acute abd cope
LLQ |
app
leak duod ulcer acutepanc regional illeitis infl ileocecal glands infl meckels cholecystitis w/ low gb biliray pancreatitis left iliac low left kidney left pyelitis or left pleurisy |
|
|
|
acute abd cope
RLQ |
diverticulitis
pericolitis around colon cancer pelvic peritonitis spreading up crohn's colitis |
|
|
|
acute abd cope
Barium usage obstructions |
sm int PARTIAL obst
- xray first to r/o total obst, can miss partial, ok to give meal w/barium when symtoms, won't turn partial to full Lg intestine - NEVER barium as can complete a block Colon obst Barium ENEMA |
|
|
|
acute abd cope
w/u renal system uretala colic |
* serious injury pt, think renal injury
- do IVPyelogram to confirm one good kidney before take out injured one * plain film to show stone -> (if no stone shown ~15%) TRY U/S -> then IVP * suspect uretal stone from acute pyenephrosis-> IVP |
|
|
|
acute abd cope
tell acute panc from acute cholecystitis in crit ill |
radio scans
tc uptake by liver and goes to GB in panc see uptake by GB usually |
|
|
|
acute abd cope
pt central epigastric pain and A. LUQ pain left side plural effusion B. right side pleural effusion |
Pleural effusion seen with sub-diaph
inflamm processes , uni or bi A. pancreatitis B. perf ulcer Do not tap unless want to test for amylase as unsure if from panc |
|
|
|
acute abd cope
role of u/s in appendicitis appy |
Graded compression u/s
less sensitive 85% specificity 92% - a thick wall appendix confirms ( over 6mm noncompressible appendix) but abscense does not rule out - useful in questionable case to r/o tubal, female gyne |
|
|
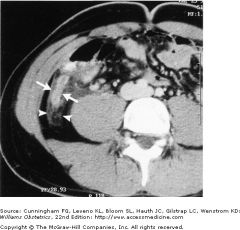
RLQ pain
25 yo |
appendix
+ CT for appy : Use contrast thicken wall over 6 mm dilation of lumen periappendiceal streaking (density in perimesentary fat) see arrows under 15% have fecolith xray only 30% obst czed by fecolith overall CT with con : sens 95-98% and spec 83-90% appy |
|
|
|
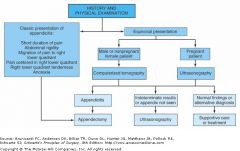
treatment
algo appy |
|
|
|
|
acute abd cope
best modalities for w/u Choices : XRAY, Barium/GI, US, CT Appy : Perf : Panc : DiverticITIS : CholecystITIS : abscess : intest Obst : intest inflam : int ischemia : aor aneu : aor rupture : renal colic : gyne : - rupture follicle - ectopic - TuboOvAb |
best modalities for w/u
Choices : XRAY, Barium/GI, US, CT Appy : CT -> US Perf : XR GI > CT Panc : CT > US > XR GI DiverticITIS : CT > GI CholecystITIS : HIDA US > CT > XR abscess : CT > US intest Obst : GI XR > CT intest inflam : GI > CT > XR int ischemia : CT ok aor aneu : CT US aor rupture : CT > US renal colic : IVP > rest same gyne : US > CT - rupture follicle US - ectopic US >> CT - TuboOvAb US > CT Page 60 |
|
|
|
Order of exam in abdomen
|
inspect
ausculate palapte percuss |
|
|
|
hernia exam in inguinal canal
which kind of hernia touches where on finger |

- your finger tip points lateral / to side and lateral to external ring ring
- indirect hernia : touches fingertip in inguinal canal - direct : touches side of examiner finger as not in canal but bulging anterior to canal |
|
|
|
radiology
pat can't stand but want to see if air fluid level , what to do ? |
left lat decub
lay 20 min (so stomach DOWN ) - air stomach : ok - air sm int : adult abn and obst (baby ok) - colon : shld habe no gas colon, rectum |
|
|
|
choledocholithiasis Rx
|
ERCP spincterotomy
if fails, Sx |
|
|
|
bact cholangitis
|
try iv abx , bil drainage , treat cause
|
|
|
|
biliary tumors
|
relieve mech obst
ERCP and stent percut stent by rad sx |
|
|
|
featuers of #1 GB cancer
|
cholangiocarcinoma
adenoca of intra bile ducts assoc stones spreads vascular NO link to HBV or cirrhosis |
|
|
|
cancer of extra hep bile ducts
|
rare in US
#1 far east realt flukes also of ampulla vater always adenocarc present progessive relent obstructive jaundice |
|
|
|
CI to HIDA
|
sig jaundice
|
|
|
|
When use PTC and what it stands for ?
|
percutaneus transhepatic chlangiogram
when can't do ERCP and want to try non-sx mgt |
|
|
|
what does panc make that eats it up ?
|
Inactive as eat panc
tyypsinogen + by enterokinase in duod and then turns on others chymotryp proelastase procarbozypepe prophospholipase A Active enz : don't autodigest panc lipase amylase (panc no strach or fat) |
|
|
|
Dx chronic panc
|
US : sensitive
CT : more sensitive duct dilate, Calcify ERCP more sens as dz advanced, show ducts MOST sensitive endoscope u/s PET scan tells chr panc from panc cancer alcoholics have Ca in 20-50% can go away with abstain |
|
|
|
Surg tx chr panc
|
nerve block thorascopic
decomp - whipple, puestow autoislet tx and total panc-ectomy endotherapy ERCP stents |
|
|
|
nutrition
comps enteral |
aspiration
refeeding bowel obst |
|
|
|
when use TPN ?
CI ? |
panc
crohn IBS post op abd sx fistula short bowel syndrome CI life expect under 3 mnths MOFS sepsis use TPN only 3 days (gut works) |
|
|
|
blood to apapendix
|
SMA to ileocolic to appedicular
|
|
|
|
appy
fold of treves |
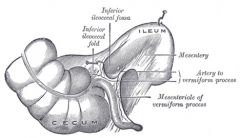
= inferior ileocecal fold
bloodless fold of treves |
|
|
|
how big is too big for appy ?
causes of obst ? |
- nml size 6 to 9 cm
- obst #1 lymphoid tissue (young adults), 30% fecolith, barium, ascarids |
|
|
|
Appy
order of symptoms |
!! key is abd pain before vomit !!
unlike gastro |
|
|
|
High Likilihood ratio appy
Low LR appy |
High LR
#1 RLQ pain ridgidity periumb -> RLQ pain pain before vomit psoas Low LR fever, rebound, Negative LR : unikley to be appy no RLQ had sim pain before |
|
|
|
appy
vs mesenteric adenitis |
mes ad
concurrent or prior URI so nonGI symptoms |
|
|
|
Rx
appy perf |
peritoneal washout
Iv abx leave skin open, reclose ~ 5 days close fascia only |
|
|
|
appy
pregnant |
use us not ct
#1 sx emer in preg 1st tri fetal mort 3-8% up to 30% with perf RX: surg and risk premat labor 10-15% |
|
|
|
appy elderly
|
late present as dont show peritoneal signs as soon
perf high 1/2 delay high WBC |
|
|
|
AIDS pts or on chemo
looks like appy |
think neutropenic colitis
OR CMV bowel perf |
|
|
|
appy
#1 tumor and cause Rx |
carcinoids are 2/3 primary tumors
under 2 cm : remove appy over 2 cm : right hemicolectomy |
|
|
|
branchial cleft vs thyroglossal cyst
which arches ? sx must remove what ? |
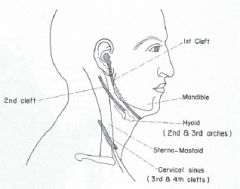
thyroglossal must remove middle of hyoid bone.
most common is cleft 2 thyroglossal cyst can move with swallowing but doesn't have to don't probe brachial arch cysts or can lead to infection |
|
|

what is it ?
Rx ? |
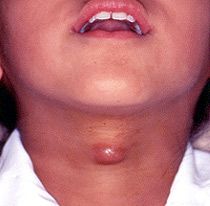
cystic hygroma
remove early or get sclerotic |
|
|
what is it ?
Rx ? |
thyroglossal cyst
|
|
|
|
man 20 year old
pain periumbil and RLQ that is intermittent and colicky slightly high WBC temo 98 DX case files |
Not appy
as pain INTERMITTENT and colicky |
|
|
|
What modality of w/u ?
Female sex active pain RLQ WBC 12K fever 100 case files A. Urine clean, exam right adnexal tenderness B. Urine + WBCs, + RBCs |
A. likley pelvic so use u/s
B. likley not pelvic, (pyelo) so try Ct To be SURE PID vs appy need laparoscopy |
|
|
|
appy
appendicitis CT shows abscess case files |
Interval appendectomy
for appendicitis comp w. abscess or phlegomon 1. 1st treat broad abx 2. CT guide drainage, resolve infection 3. sev weeks later take out app |
|
|
|
never use clinical obesrvcation if see any of what
case files |
limited use of
localized pain , fever, of high WBC already maybe use in early appy w/o local signs as CT less good in early appy |
|
|
|
burr holes ?
|
Rapid decline in consciousness
inc BP and low HR try CT first ! that guides whatever neurosurg does - never do blind ED craniotomy before CT - can consider ventriculostomy / burr hole to release hematoma. If you don't have a CT you can put 6 holes in "woodpecker method" |
|
|
|
in blunt trauma what does CT pick up and miss ?
case files |
CT good for solid organs
poor at retroperitoneal poor hollow viscus organs |
|
|
|
man 60 yr
h/o polyps removed now gross positive hemeoccult hgb 8.7 chronic w/u ? case files |
1. transfuse
2. needs EGD and colonoscopy likely colon |
|
|
|
what is a abdominoperineal resection ?
|
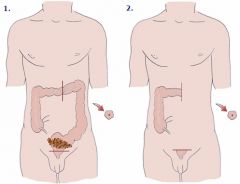
APR
For anal cancer that is low lying - remove rectum and anal canal and sphinter - leaves a permenent colostomy (on left) |
|
|
|
diverticulitis
- small absces - lger - not better in 72 hours - are better in 72 hours - OR ASAP case files |
- - small mesenteric abscess can heal w/ abx
- lger pelvic abscesses need CT drainage - not better in 72 hrs go to OR - are better in 72 hrs may beed to return for elective sx - OR ASAP if perf and peritoneal signs, hemounstable and so resetion and Hartmanss if no contamination can be orimary anastamosis |
|
|
|
repair divertucilar fistula
case files |
- resect sigmoid colon that is part of fisula
- excise fistulous tract - repair/resect other organ |
|
|
|
what is a hartmann ?
|
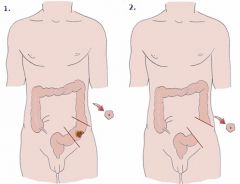
HArtmann
2 stage surgery for emergent sx for diverticlitis first make colostomy then later take it down |
|
|
|
fascial defect or incisional hernia at midline laparotomy site
when ? who ? treatment ? case files |
When ? 3 weeks post op
RF : over 70 Yr, DM, malnutr, perioperative pulm dz Treatment : 1. Eval for sepsis or evisc so do WBC 2. local wound care 3. later on elective repair of fascial defect / incisional hernia that will occur Who needs OR asap : pts risk eviscerate, high WBC and fever, enterocutaneous fistula, uncontrolled sepsis Who not to operate on if can help it : stable dehis, no bowel out, nasty abd you don't want to open |
|
|
|
incisional hernia ?
repair ? |
- can present 5 yrs post op
- avoid repair when occur as high wound infeciton rate and recurr rate so use mesh |
|
|
|
5 days pot op patient has 40 ml serosanguinous fluid from midline lap wound
- what to do ? |
open wound and eval fascia
infected wounds have up to 20% rate of incisional hernia / defect |
|
|
|
biliary colic vs acute cholecystitis vs cholecdocholitiasis
|
b colic : intermittent , nml liver enz
acute cholecystitits : high WBC, stays painful, mild rise non specific liver enz choledocholithisias : dilated common bile duct on U/S of over 5 mm and high liver enz gallstone pancrease: if amylase and lipase high |
|
|
|
biliary colic vs acute cholecystitis vs cholecdocholitiasis
|
b colic : intermittent , nml liver enz
acute cholecystitits : high WBC, stays painful, mild rise non specific liver enz choledocholithisias : dilated common bile duct on U/S of over 5 mm and high liver enz gallstone pancrease: if amylase and lipase high |
|
|
|
gallstone pancreatitis treatment
|
- bowel rest and IV hydration
- during same hospitalization but after calm down (no jaundice) lap cholecystetomy as long as uncomp gallstone panc |
|
|
|
man presents with sudden painful groin mass
what to do ? |
sudden painful mass suggests incarceration
so OR before strangulates Before OR - IVF and fix lytes and try to reduce it |
|
|
|
- 80 year old women in nursing home lost several pounds over last mnths
- 3 days not eating, vomiting, this AM confused and very ill - abd benign no scars, mass on medial thigh Dx |
Obturator hernia
XRay will show dilated small bowel Rx : FIRST recus and hydrate (altermed mental) Then to OT urgent repair |
|
|
|
FNH what has good spec and sens ?
|
Angiography
|
|
|
|
liver tumors seen well on MRI ?
|
On MRI
- high spec and sens for mets adeno and hemangioma - low FNH unless see central scar, low hepato carcinoma, adenoma |
|
|
|
liver tumor seen well on CT ?
|
hemangioma
mets |
|
|
|
angio is good for which liver tumors ?
|
gold standards for hemangioma
and high for mets |
|
|
|
lap u/s good for which liver tumors ?
|
gold standard for hepato carcinoma
when combo w. lap biopsy good for adenoma and met adenocarc |
|
|
|
biopsy which liver tumors ?
|
mandatory got hepato carcinoma and mets adeno
helpful adenoma , rarely helpful in FNH (do angio) CI hemangioma |
|
|
|
name 2 kinds pulm sequestration and treatment ?
|
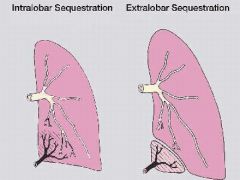
Intralobar :
presents with infection, has no pleura cover, CXR mass or air/fluid level veins drain via pulm veins Rx lobectomy Extra-lobar pleural covering assoc diaph hernia incidental finding CXR venus via pulm vein or azygous vein DX MRI Must do aortigram? or somesthing to prove no vessels draining below dipah which can cause exsanguination if cut |
|
|
|
ruptured omphacele vs gastroschisis
|
omphacele has intact umb cord at leve of abd wall
|
|
|
|
lab bili findings indicating biliary atresia
|
direct bili over 2 mg/dL
direct bili over 10% of bili of total bili |
|
|
|
4 month old infant jaundice direct bili 3 mg/dL
|
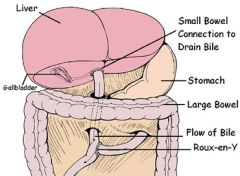
correctible type : blind ending dialtion of c hep duct Use anast with Roux-en-Y loop jejeumum
non-correctable use : Kasai hepato portoenterostomy post op tx prophy abx, phenobarb , liver transplantation Kasai : A surgery performed on an infant with Biliary Atresia to allow bile to flow from the liver. In a Kasai the damaged ducts are removed and replaced with some of the infant’s own intestine. The small intestine is divided (Roux-en-Y) and a section is brought up to the liver. This connection may be inside or outside of the liver. The Kasai procedure is also called a hepatoportoenterostomy. |
|
|
|
kid with volvulus
CI barium enerma |
No enemia if periotontits, perf , profound shock
Rx volvulus : treat dehyd NG to decompress hydrostatic decompression barium enema air enema |
|
|
|
meckels repair ?
|
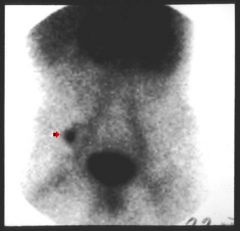
diver tic resection and transverse closure of enterostomy
|
|
|
|
GI bleed lecture
NG aspirate finding neg blood pos bile What next ? If this test neg, what next ? |
on test rules out U GI bleed
-> Do EGD If neg -> Tagged RBC scan ! (not colonoscopy as only see poo and blood) If pos -> Angio to localize |
|
|
|
GI bleed lecture
How fast a bleed needed to see with Tagged RBC scan and angio ? |
Tagged scan : 0.1 cc/min
very sens but not specific to an area Angio L 1 cc/min nad localizes to an area. Still do tagged RBC first and only if tagged pos go to angio. |
|
|
|
GI bleed lecture
NG aspirate neg blood neg bile |
can't rule out U gi bleed
|
|
|
|
GI bleed lecture
+ blood + bile |
U GI bleed
Diff : PUD gastric or duod (since bile) dilauefoy mall weiss |
|
|
|
GI bleed lecture
when might you go to OR without localizing lesion in GI bleed ? incision ? |
hemo unstable (BP under 70) despite cont'd transfusion
NG negative so know its lower 4-5 units/24 hrs 8-10units/48 hrs incision : lap Sx : total abdominal colectomy Risk as 15% bleeds from sm int can try seriel enterotomy (peek holes in sm bowel) TEst answer: no 1 anast as that is slow and concerns about unpreped bowel and healing esp if left colon But 85% stop bleeding on own |
|
|
|
GI bleed lecture
can angio be therapeutic ? |
Can use vasopressin to close vessel
Risk colon ischemia as no alot collateral vessels |
|
|
|
GI bleed lecture
First tag scan negative Pt in ICU for moniter BP drops now What to do ? |
Re RBC tag scan.
Do not have to re-dye load as tagged cells last 24 hours. |
|
|
|
notes fluids kagen
drug that causes hyperkalemia |
pen G
|
|
|
|
Treatment for hyperkalemia
|
Glucose-insulin-bicarb :
- 50 cc D50 - 10-25 u reg insulin - 1 amp NaHCO3 Ca gluconate 10% 50-100cc Kayexalate 5-10 gm po QID dialysis |
|
|
|
Treatment hypercalcemia
|
NS and furosemide
mithramycin chelating agents steroids |
|
|
|
treatment hypocalceima
|
ca chloride
ca gluconate lecture notes |
|
|
|
treatment metabolic alkalosis
|
ch replacement
potassium replacement 0.1 N HCL or ammonium chloride lecture notes |
|
|
|
treatment resp acidosis
|
mech ventilation
lecture notes |
|
|
|
treatment resp alklosis
|
pain mgt
vent support CPAP/PEEP search for sepsis lecture notes |
|
|
|
Treatment
small cell lung cancer |
chemo (has fast mitotic rate) hafe regress
VS non-small cell only 5% regress with chemo No sx - central |
|
|
|
Lung CA
central |
Sentral
Small cell Squamous |
|
|
|
lung ca
plain film size ? |
size ? 0.8 to 1 CM diameter most malig nodules
Good features : Bad features : |
|
|
|
chronic cough
dyspnea syncope headache bloody nose worse with leaning forward and upin AM awakening |
Superior vena cava syndrome blocks venous return
|
|
|
|
hyponatremia
chronic cough smoker |
SIADH
low serum osmol but no edema due to AVP ectopic release |
|
|
|
treatment lung CA
nonsmall cell |
30-50% shrink with radiation
chemo doesn't work Sx if under stage IIIA |
|
|
|
Types of tumor trachea and bronchi
- benign - malig potential bluprints , old version |
BENIGN
sq papillamoatosis HPV 6 11 angioma fibroma leioma chrondma MALIG POTENTIAL br carcinoids (10% malig) adenoid cystic carcinoma mucoepidermoid |
|
|
|
lung ca nodules
- nodule that is stable for 2 yrs - nodule new in last 2 months - and clubbed fingers |
- nodule that is stable for 2 yrs -> needs no further eval
- nodule new in last 2 months -> unlikley to be malignant - SPnodule with hypertrophic osteoarthy : 75% chance carcinoma |
|
|
|
lung ca nodules
no bony mets no bulky contra lat mediastonal LN |
plain film first, may be enough
|
|
|
|
lung ca nodules
when CT |
CT should inc liver and adrenal
better mediastinal LNs |
|
|
|
lung ca nodules or CA
when do bronch ? When do TBNA ? |
Sentral masses
- small cell - squamous Options : direct visualize and biopsy lesions , TBNA (transbronchial needle aspirate), washings TBNA best for staging mediastinal LNs |
|
|
|
lung ca nodules or CA
When do trans thoracic needle biopsy ? TNB When thoracocenesis ? |
Diagnosis :
Chest CT with needle biospy bronchoscopy plus/minus transtracheal biopsy (note with transtrachel needle biopsy can't see node as needle it, rely on CT scan from before of where it is. Endoscope better but only at a few centers. ) Excisional biopsy open vs thorascopic diagnostic but risks PTX. Can be therapeitic for small lesions, sol mets, prim cancer if cant have more major sx TNB ? -peripheral nodules - Most CT guided -sensitivty 70-100% thorcocentesis -TOC pulm effusion and suspect malignancy |
|
|
|
lung ca nodules or CA
single nodule under 3 cm intra parenchymal opacity wel marginated |
= def of solitary pulmonary nodule
Most benign - granuloma, haramtoma, intrapulm lymoh nodes Some malig - bronchogenic carcinoma RF malignant : - over 1 cm and even more if over 4 cm - indistinct margins (corona radiata) - document growth on FU plain film - pt older - male Smoker over 50 YRs over 50% malig VS 5-10% malig overall. |
|
|
|
lung ca nodules or CA
small cell staging |
70% met at dx
2 stages limited : one radiation portal VS extensive : the rest |
|
|
|
lung ca nodules or CA
non-small cell staging |
Work up to determine if sx possible
Chest CT (incl liver and adrenal for mets) If malig pleural eff CI sx TNM staging system |
|
|
|
lung ca nodules or CA
recall lung areas where CA more often ? |
Right > left
upper > lower |
|
|
|
lung ca nodules or CA
recall Sites of extra thoracic mets |
1. bone (vert bone pain)
2. liver 3. adrenal 4. kidney |
|
|
|
paraneo syndromes can also get with lung CA not just gut cancer ?
|
acanthosis nigracans
thrombophlebitis Also paraneo cushing SIADH Eat Lam cerbellar ataxia hypertrophic osteoarthy |
|
|
|
tests to workup tumor or lung mass
recall |
- sputum cytology (diagnostic in 5-20%)
needle biopsy w. CT or floror guidance broncho with brushings, biopsy or both w or without mediastinoscope, scalene node biopsy, or open lung biopsy. |
|
|
|
lung CA
T3 and T4 stage ? Adam online |
In T3, a tumor of any size has directly invaded any of the following:
* Chest wall * Diaphragm * Membrane covering organs and structures in the chest * Outer wall of the membrane around the heart (pericardium) In addition, one or more of the following conditions are present: * The tumor is in the main airway, less than 2 cm away from the carina, but is not in the trachea (windpipe). * The tumor is associated with a collapsed lung or swelling that blocks the entire lung. In T4, the tumor has invaded any of the following: * Area between the lungs (mediastinum) * Heart * Great vessels (the blood vessels that carry blood from the heart) * Carina, trachea, or esophagus * Main portion of the spine In addition, one or both of the following occurs: * Separate tumors are present in the same lobe * The tumor is accompanied by an increased amount of fluid between the pleural membrane and the lung. |
|
|
|
lung CA and on biopsy :
- Only a few layers of cancer cells are detected within one local area. - The cancer has not grown through to the top lining in the lung |
Stage 0 or Carcinoma in Situ
Stage 0 or carcinoma in situ (Tis, N0, M0) are noninvasive cancers. Only a few layers of cancer cells are detected within one local area. The cancer has not grown through to the top lining in the lung and can be surgically removed. There is a high risk for development of a second tumor, however. Treatment Options: * Surgery, often a limited procedure, where only part of a lobe is removed from the lung. * In patients who cannot be treated surgically, consider photodynamic therapy, cryotherapy, or brachytherapy. Adam online |
|
|
|
lung CA treatments
|
Treatment Options.
* Combination of two- or three-drug chemotherapies that include platinum-based drugs and newer drugs; * Bevacizumab (Avastin) may be used for patients with non-squamous lung cancer, no spread to the brain, and who are not coughing up blood. * External-beam radiation for symptom relief * Paclitaxel, gemcitabine, or docetaxol are all additional drug options * If metastasized cancer involves only one or two areas in the brain, it may respond to surgery followed by radiation to the brain. |
|
|
|
lung CA sx :
|
# Mainstay lobestomy for central lesions
# for primary cancer that is re sectable and no CI, do node dissections. The surgical removal of an entire lobe or parts of a lung is the primary treatment for eligible patients in the early stages of cancer. Recurrence is high after surgery, although the new tumor is often operable. # Some patients with stage IIIA cancer may also benefit from surgery. The intent at this stage is to extend survival time, rather than cure the disease. Wedge Resection or Segmentectomy. Wedge resection and segmentectomy remove only a small part of the lung. They preserve almost normal breathing function after the operation. Lobectomy. Removal of one of the lobes of the lung is called lobectomy. The patient must have enough lung function to undergo this procedure. The patient has a 3 - 5% after this operation, with older patients having the highest risk. Pneumonectomy. Pneumonectomy removes the entire lung. The patient has a 5 - 8% risk of death after this procedure. The oldest patients have the greatest risk, and they almost always have a recurrence. Stage 1 and small, and old try VATS |
|
|
|
pt too sick or for sx and early stage and adequte lung function
|
try radiation.
also palliative rad |
|
|
|
features sq lung CA ?
|
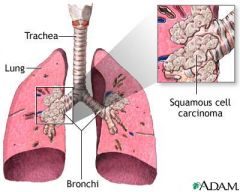
Squamous
central in HILUS so Pancoast slow growth and late mets assoc smoking |
|
|
|
adenocarc
lung CA features ? |
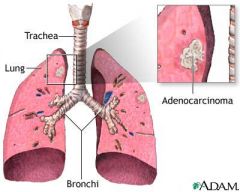
adeno
peripheral rapid spread hematog and nodal spread assoc lung scarring |
|
|
|
small cell lung CA feautres ?
|
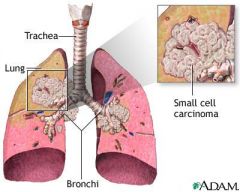
Small cell
Sentral highly malig non operable usually |
|
|
|
LARGE CELL lung CA features ?
|
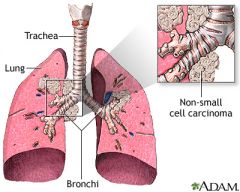
large cell lung CA a subtype of non-small cell
usually peripheal very malig |
|
|
|
lung Ca
diff between IIIa and III b and why it matters ? |
For NON SMALL cell
III a operate/resect if early IIIA, chemo +/- radio., 5yr surv ~ 20% 1. tumor in chest wall, diah, or mediasrinal pleura or pericardial sac AND + nodes in lung or ipsi hilum and NO mets T3N1M0 2. LN mets ipsi mediastinal or subcarinal nodes, NO Mets and NO mediastinal tumor invasion T1-T3N2 M0 III b no operate but chemo and radiation (XRT) |
|
|
|
When chemo for lung CA
|
induction chemo BEFORE sx for NON small cell CA inc survival
|
|
|
|
lung CA
isolated brain mets ? |
sx resect
|
|
|
|
CI to sx for lung CA
recall |
Sup vena cava syndrome
supra clav LN mets , scalene node mets , mets in other organs trachea carina involved small cell cancer PFTs show FEV1 under 1 (as to remove lung must be over 1 to start as must be over 800 cc after sx to do well) cardiac cripple or prior MI |
|
|
|
Post op FEV1 goal
|
Post op FEDV1 over 800 cc
so pre op must be over 2 for pneumonectomy If FEV1 under 2, try VQ scan |
|
|
|
wheezing
atelectasis bronchoscope shows round red-yellow mass protrudeing into brochial lumen |
carcinoid tumor
slow growing comnfused with asthma Rx: lobeectomy with LN dissection OR sleeve dissection of proximal (cut out bad ring of bronchus and anast ends) good prog if nodes negative |
|
|
|
Esophagus
why does it leak after anastomosis ? What nerbe runs here ? |
no serosa , like distal rectum
nerve here is VAGUS |
|
|
|
esophagus thru what level in diaphragm
|
esophagus thru T10
T8 IVC T10 esophagus T12 aorta |
|
|
|
name wrist bones ?
proximal row and distal row ? |

Some scaphoid
Lovers lunate Try triquetrum Positions pisiform That Trapezium Also the areticular disk between pisiform, ulnar bone and lunate which makes meniscus of wrist. They trapezoid Cant Capitate Handle hamate |
|
|
|
muscles that extend wrist ?
|
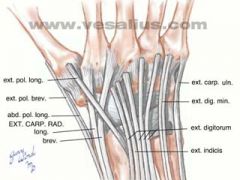
WRIST EXTENSORS
On posterior of wrist / dorsal side RADIAL NERVE and all extrinsic muscles meaning attach to forearm not to within hand. * Extensor Carpi Radialis Longus * Extensor Carpi Radialis Brevis FLEXOR GROUP * Flexor Carpi Radialis * Palmaris Longus * Flexor Carpi Ulnaris ROTATORS OF THE WRIST * Pronator Teres * Pronator Quadratus * Supinator |
|
|
|
what is dequer wrist tenosynovitis ?
|
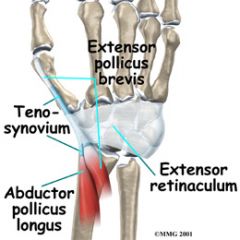
de Quervain's tenosynovitis affects two thumb tendons. These tendons are called the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB).
tendons run along radius Sx : pain above thumb in wrist diff : intersection syndrome , more medial |
|
|
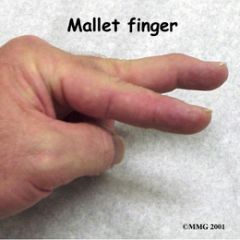
name problem ?
hand |
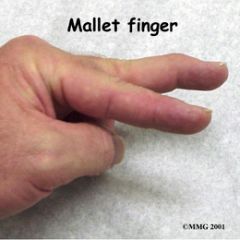
ext tendon along top of finger rips off DIP
Rx splint for 6 weeks or else cant straighten finger out (under side of finger is flexor tendon ) |
|
|

name problem ?
hand |
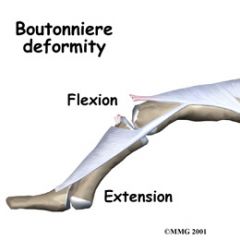
tear in central slip of extensor hood
|
|
|
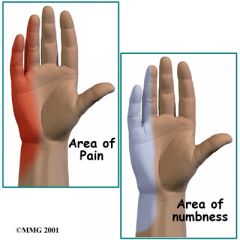
chronic onset
|
Cubital Tunnel Syndrome
ulnar nerve where it crosses the inside edge of the elbow. ( very similar to the pain that comes from hitting your funny bone). It supplies feeling to the little finger and half the ring finger. It works the muscle that pulls the thumb into the palm of the hand, and it controls the small muscles (intrinsics) of the hand. Causes N actually stretches several millimeters when the elbow is bent. Sometimes the nerve will shift or even snap over the bony medial epicondyle. Over time, this can cause irritation. pulling levers, reaching, or lifting. Constant direct pressure on the elbow over time may also lead to cubital tunnel syndrome. The nerve can be irritated from leaning on the elbow while you sit at a desk or from using the elbow rest during a long drive or while running machinery. OR The ulnar nerve can also be damaged from a blow to the cubital tunnel IN MEDIAL ELBOW |
|
|
|
hand nerve radial sensory ?
|

radial nerve enters between superfic and deep extensor muscles in back of hand.
supplies extensors |
|
|
|
hand nerve ulnar ?
|

ulnar :
passes between pisiform and hook of hamate and tunnel of guyon supplies Flex carpi ulnaris and 1/2 F dig profundus |
|
|
|
hand nerve median ?
|

enters carpal tunnel
to flexor muscles |
|
|
|
hypothenar muscle ?
nerve ? hand |
hypothenar muscles are opposite hand
Ulnar nerve - abductor digiti minimi - flex digiti minimi - opponoms digiti minimi |
|
|
|
hand injurys needing OR vs ER repair ?
|
extensor : more ER
flexor : more OR |
|
|
|
flexor tendon of hand injury zones ?
|
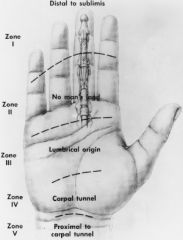
TENDON INJURIES
Flexor Tendons The most common cause of flexor tendon injury is a laceration. Flexor tendon lacerations can be subtle; however, the careful examiner will identify these injuries. A classification system for flexor tendon injuries has been developed based on location, treatment considerations, and prognosis. ZONE I Extends from the insertion of FDS to the profundus tendon. Patients with these injuries lose flexion at the DIP. Retrieval of the proximal tendon is often difficult. ZONE II Involves the portion of the digital canal occupied by both FDS and FDP. The close proximity of these tendons makes it essential for exact repair with minimal operative trauma. This region is often referred to as “no man´s land” because of the frequent poor outcomes prior to the 1960s when improved repair techniques were developed. Lacerations in this zone are common, and partial lacerations are more common then complete. ZONE III Extends from the distal edge of the carpal tunnel to the proximal edge of the flexor sheath. The lumbrical muscles originate from FDP in this region. Outcomes are generally favorable. ZONE IV Involves the carpal tunnel and related structures. The area must be explored carefully because so many vital structures go through the carpal tunnel. Isolated injuries are the exception. ZONE V Involves injuries to tendons proximal to the carpal tunnel. Injuries here tend to be severe and often involve multiple tendons as well as the median or ulnar nerve. It is essential to search for all major structures. A hand surgeon should repair flexor tendon lacerations. Primary repair should occur within 12 h. Secondary repair can occur up to 4 weeks after the injury. Another type of flexor tendon injury is the avulsion of FDP from its insertion in the distal phalanx. This can occur from a grasping motion against high-speed resistance. The patient will be unable to flex the distal phalanx. Prognosis depends on the size of the bony fragment, the length of time from injury to repair, and the blood supply to the tendon. |
|
|
|
hand intrinsic muscle ?
|
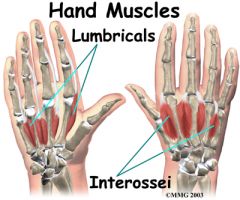
Median nerve :
- dorsal interossei : abduct finger - palmer interosseu : adduct finger lumbricals flex MCP and extend PIP, DIP use Median and Ulnar nerve Ulnar for palmaris brevis for hand grip |
|
|
|
hand tests ?
- bend thumb tip ? flex pol longus - bring thumb to side and back ? ext poll brevis and abd poll brevis - raise thumb only while rest of hand is flat ? ext poll longus |
hand tests ?
- bend thumb tip ? flex pol longus - bring thumb to side and back ? ext poll brevis and abd poll brevis - make fist with little finger extended alone ? ext digiti minimi Radial , extrnsic muscle (Extrensors) |
|
|
|
hand tests ?
- flex and ext a fist at wrist ? ext carpi radialis longus and brevis - make fist with little finger extended alone ? ext digiti minimi |
hand tests ?
- flex and ext a fist at wrist ? ext carpi radialis longus and brevis - make fist with little finger extended alone ? ext digiti minimi Extensors are Radial |
|
|

name injury ?
|
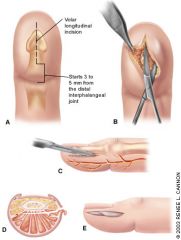
Felon :
tense in fingertip pad unlike whitlow where painful but soft pad. Pad has fibrous septae so little room so gets tight and swollen. Bugs : S. aureus, streptococci First-generation cephalosporin or anti-staphylococcal penicillin Incision and drainage should be performed if infection is well established. Oral antibiotic therapy usually is adequate. Because the septa attach to the periosteum of the distal phalanx, spread of infection to the underlying bone can result in osteomyelitis.16 |
|
|
|
Rx paronchyia ?
|
7 days abx soaks, retract skin nail margin
If more extensive, unroll skin at base of nail and lat and ID at area of most pus and drain under dig block. |
|
|
|
breast CA
findings on prior breast biopsies assoc with breast CA ? |
aty hyperplasia
LCIS |
|
|
|
breast CA
and hormone meds ? |
combo HRT over 4 yrs
estrogen over 5 yrs OCP slight inc and stops once stop OCP |
|
|
|
breast CA
percent biopsies showing CA ? |
20%
|
|
|
|
breast CA
sens and spec mamm ? |
mamm
Screening : 80-95% sens IF so with breast exam Also high specificity Vs diagnostic if done with symptoms |
|
|
|
breast CA
sens and spec ultrasound ? |
US used only diagnostically NOT for screening
poor sens good spec solid vs cyst homo vs not 1st tool for young women |
|
|
|
breast CA
sens and spec MRI ? |
diagnostic use
high sens over 95% low spec as sees lots of masses useful in breast dense on mammogram can use gadolin contrast |
|
|
|
breast CA
options palable mass ? |
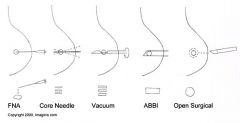
FNA : give no tissue arch just cytology, at best 94% accurate sens for CA. ** 10% FALSE neg rate so can't r/o CA
Percut core biopsy 96% sens CA excisional biospy 100% sens CA incisional biospy Dx adv dz and inititate Rx |
|
|
|
breast CA
options non palp mass |
need imaging
stereotaxic core biopsy (mammogram guide) 96% sense CA U/S guided core biospy 90-95% sens CA needle localized excisional biospy (sx after needle placed mamm) 98% sens CA |
|
|
|
breast CA
screening recs ACS |
BSE monthly age 20
clinical breast exam per 3 yrs age 20-39, annually age 40 mamm age 40 yearly |
|
|
|
breast CA
what has Ca++ on mammo ? |
fibrocystic change
ductal hyperplasia insitu carcinoma invasive carcinoma |
|
|
|
breast CA nodes ?
|
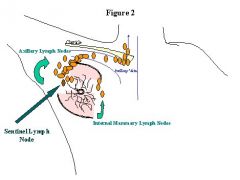
on clinical exam palpate :
supraclavicular infraclavicular thyroid involved in adv cases axillary |
|
|
|
breast CA
Mammogram views ? |
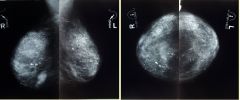
Left
MLO medial lateral oblique CC cranio caudal : top of muscle, and between breast and muscle should be lucent |
|
|
|
breast CA
breast CA ultrasound breast findings |

cysts should be in same place as tissue and often oblong in that plane
no echos in them (be homgen) |
|
|
|
breast CA
month after box falls of women skin or nipple retraction oil cyst in wall of breast |
fat necrosis
Rx follow by PE |
|
|
|
breast CA
women 35 well circum tumor mobile mass |
women younger / Middle aged
more cellular vs fibroadenoma RX: Wide local excision (recur locally) If recur or large may need mastectomy. Do not need LN removal even if malig cystosarc phyloide as don't met by lymph |
|
|
|
breast CA
what is LCIS ? |
marker for inc risk Breast CA
not itself pre malig bilat and multicentric Rx no sx |
|
|
|
breast CA
What is DCIS ? |
usually defined as mammogram changes, sometimes comedo mass
if any signs invasion managed as such RX: - lumpectomy and total br radiation post op - total mastectomy |
|
|
|
breast CA
extended beyond BM Rx ? |
= invasive carcinoma
remove breast plus mgt axillary LN mgt |
|
|
|
breast CA
stages I and II |
- lumpect axill LN dissection and total breast irrad post op
- mod rad mastect and rad sometimes and chemo sometimes |
|
|
|
who is poor candidate for lump and breast irradiation ?
|
small breat / lg tumor
tumor over 4 cm carcinoma behind nipple multicentric DCIS or invasice extensive ductal carcin in situ compliance scleriderma / SLE |
|
|
|
breast CA
read skin or peau d'orange |
stage III B or C
inflamm carcinoma Rx chemo PRE - op = neoadjevant AND modified rad mast (total mast and axill LN mgt) then radiation afdter chemo as lots of local recurrence |
|
|
|
breast CA
axillary lymph nodes ? DAngers of dissecton ? |
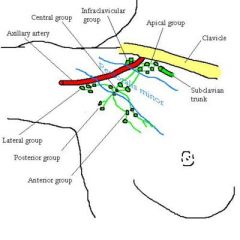
The surgical classification is used in axillary dissection for breast cancer.
CA spreads level 1 to 2 to 3 and 3 is worse. - based on relationship to pec minor. Level 1 nodes : lateral or side of pec minor (lateral, anterior and posterior nodes) Level 2 consists of those nodes under pec minor : central nodes and some of the apical nodes. Level 3 (medial to medial border of pec minir nad under clavicle) consists of those nodes beyond the superior border of pectoralis minor. ROTTER's nodes : between pec major and minor. Axill and int mamm LN drain also. It includes the remaining apical nodes and infraclavicular nodes. Dangers of dissection : damage axillary A and nerbe seroma, lymphedema, rest shoulder mvt from scar contraction |
|
|
|
breast CA
mets ? |
via venous plexus Batson's
to spine |
|
|
|
breast CA
anatomy nerve veins |
long thoracic nerve is posterior -> serr ant -> wing scapula
mediaL pectoral N is really lateral to lat pect N as named based on brachial plexus -> pec maj and minor -> weak of these muscles intercostobrachial N : anesh inner arm skin thoracodorsal N -> lat dorsi -> cant push up from sitting axill vein is superior and is most of vein drainage Art : - lat thoracic A and thoraco dorsal A to Axill A - int mamm A perf and intercostal A |
|
|
|
breast CA
Cse 42 yr old mass persists for 3 mnths undiagnosed FNA non- diagnostic what to do ? |
FNA false neg 10% !! cant r/o cancer
Oberving not option if over 30. Algo: Over 30 : U/S or FNA. - fluid non bloody and mass resolves serial fu screening per guidelines - mass persists/no fluid -> mammo or get tissue via FNA or needle biospy ----- dx made then treat ---- non diagnostic : get more tissue with excisional bx then treat and f/u |
|
|
|
breast CA
Case 20 yr firm mass well circum non tender |
fibroadenoma til proven other
RF AA, smoker Dx FNA and can observeif under 3 Cm if FNA non dx, pt over 30 or symptoms MUST excise mass |
|
|
|
breast Ca
what is mondot's dx ? |
thrombophlebitis of lat thor or thoracoepi vein
RF trauma, sx, infection Sx: pain axilla or upper breast and on PE feel a tender cord Dx US gives clear dx Tx ASA, wam compress, resolves 2-6 wks if persist can try sx |
|
|
|
breast CA
you needle aspirate cyst and fluid is ____ what do you do ? |
- green or cloudy and single dom cyst ok to discard
- bloody sent to cytology |
|
|
|
peds sx
hirshsprung |
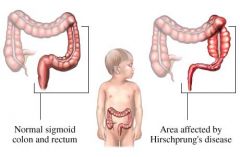
|
|
|
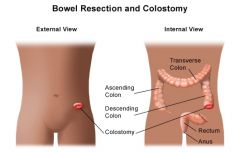
peds sx
hirshsprung |

|
|
|
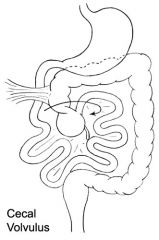
gi sx
name condition |
cecal volvulus
|
|
|
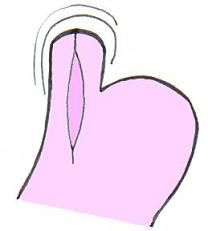
what sx is this for ?
gi sx |
achalasia
|
|
|
|
gi sx
stomach what is antrectomy ? |
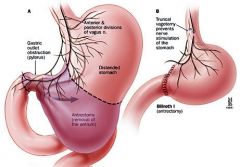
see pic
|
|
|
name sx and what it is for ?
gi sx |
APR
?? |
|
|
|
gi sx
what is an ivor lewis ? |

|
|
|
|
gi sx
peds sx what is kasai ? |
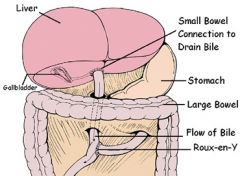
i think for biliary atresia
|
|
|
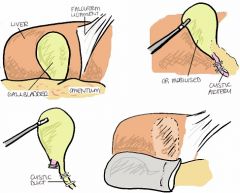
gi gb sx
describe lap chol and who can get one ? |
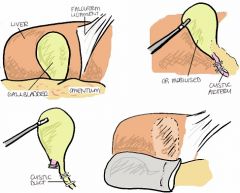
|
|
|
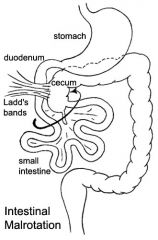
what is this ?
s sx ? |
malrotation
sx emergency |
|
|
gi sx
what is this test and what does it show ? |
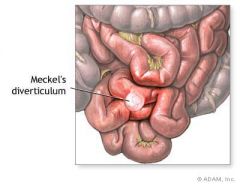
meckels scan
sx to take out not just meckels but also part of intestine near it as that is part that bleeds due to acid eating it. |
|
|
|
gi sx
panc anat of panc |

|
|
|
|
peds sx
lung pulm seq name 2 types |
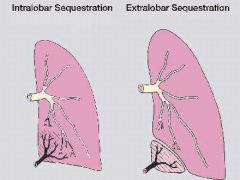
|
|
|
|
peds sx
how repair TEF ? |
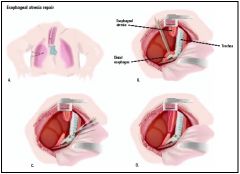
|
|
|
|
gi sx
types of stomas ? |
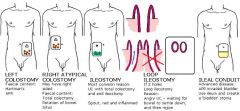
|
|
|
|
gi sx
panc descrive whipple |
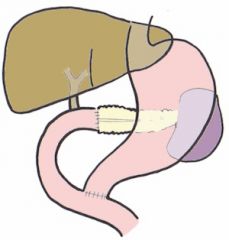
|
|
|

esoph
gi name disorder pic is pre and post procedure |
esoph atresia
Achalasia of the esophagus. Left: Moderately advanced achalasia. Note dilated body of esophagus and smoothly tapered lower portion. Right: Widely patent cardioesophageal region following cardiomyotomy (Heller procedure). (Reproduced, with permission, from Way LW [editor]: Current Surgical Diagnosis & Treatment, 10th ed. Originally published by Appleton & Lange. Copyright © 1994 by The McGraw-Hill Companies, Inc.) |
|
|
|
esoph
gi treatment for achalasia |
Surgical Myotomy
A modified Heller cardiomyotomy of the LES and cardia results in good to excellent symptomatic improvement in over 85% of patients. Because gastroesophageal reflux may develop in up to 20% of patients after myotomy, most surgeons also perform an antireflux procedure (fundoplication). Myotomy is now performed with a laparoscopic approach and is preferred to the open surgical approach. The low morbidity of laparoscopic surgery has led some experts to recommend it for initial treatment. In experienced hands, however, the initial efficacies of pneumatic dilation and laparoscopic myotomy are nearly equivalent. |
|
|
|
abg pulm icu
what O2 sat does the following equal : 30 mmHg ? 40 mmHg 60 mmHg |
30 mm Hg ~ 60% O2 sat
40 ~ 75% O2 sat 60 mm Hg ` 90% SaO2 2 Once PaO2 exceeds 70mmHg further increases do not necc increase O2 delivery. |
|
|
|
abg pulm icu
What is base excess ? |
non resp part of ABG
incl RBC buffering nm is -2 to +2 |
|
|
|
abg pulm icu
If the PH is decreased by 0.8 : what should happen to others for a balenced deficit ? Calculate what PaCO2 should be for a pt with PH of : 7.40 |
For 0.8 change in Ph
pa CO2 changes 10 mmHg 0.8 PH -> 10 in CO2 [ this is using HCO3 / PCO2] Ph 7.40 -> PaCO2 40 Ph 7.32 -> PaCO2 50 7.48 -> CO2 30 |
|
|
|
abg pulm icu
low ph : acidosis high PaCO2 : retaining CO2 nl BE and HCO3 |
uncompensated
resp acidosis as BE and bicarb nml like NM dz or lung dz or resp center depression Rx treat cause, mech vent, buffers |
|
|
|
abg pulm icu
nml ph high paCO2 high BE and HCO3 |
comp resp acidosis
like NM dz or lung dz or resp center depression Rx treat cause, mech vent, buffers |
|
|
|
ABG icu pulm
high ph low pa CO2 nl BE and bicarb |
uncomp resp alk
Cx: resp center stim , iatrogenic Rx: treat cause |
|
|
|
ABG icu pulm
nml ph low pa CO2 low BE and bicarb |
comp resp alk
Cx: resp center stim , iatrogenic Rx: treat cause |
|
|
|
ABG icu pulmarb
high ph high HCO3 nml paCO2 |
uncomp met alk
Cause : hypokalemia , NG suction / vomit, contraction alkalosis, admin bicarb, steroid therapy Rx : treat caues, volume, diamox, NH4CL, arginine monohydochloride, HCL |
|
|
|
nml ph
high HCO3 high paCO2 |
comp met alk
Cause : hypokalemia , NG suction / vomit, contraction alkalosis, admin bicarb, steroid therapy Rx : treat caues, volume, diamox, NH4CL, arginine monohydochloride, HCL |
|
|
|
ABG pulm ICU
tidal volumes to use |
post op 8-12 ml/kg ideal BWt
restrictive lung dz 4 - 8 ml/kg (ARDS 6 ml/kg) obstrctive 8-10 ml/kg Alveloar vent = tidal vol - dead space Vent Ex = freq x tidal volume Main determ tidal vol is ht not weight Women 45.5 +2.3(ht inches -60) Men 50+2.3(hr inches-60) modify so airway press under 30 cm H2O |
|
|
|
ABG pulm icu
Failure to liberate from vent ? WHEANS not |
Wheezes
heart dz ELectrolyte (alkalosis) Anx, airway probs, alkalosis NM dz sepsis, sedation Nutri (over and under feeding) Opiates, obesity thyroid dz (RARE) |
|
|
|
ABG pulm icu
weaning readiness daily screen |
5crit
cough when suctioned no contin pressors or sed infusion PaO2/FIO@ over 200 PEEP <= 8 cm H2O f/Tv under 105 for one minute *** Ely author If pass this go to SBT 30 mins |
|
|
|
ABG pulm icu
SBT is what |
resp rate > 35 for over 5 mins
spo2 under 90% over 30 secs 20% inc or dec HR for over 5 mins SBP over 180 or under 90 for 60 consec seconds Agit/diaph > baseline for over 5 minutes |
|
|
|
vasc
where is dorsalis pedis ? |

Proximal base of metatarsals 1 and 2.
the dorsalis pedis, posterior tibial and femoral pulses are not palpable 8.1%, 2.9% and 0.0% of the time respectively (McGee, 1998). Absense of both DP corr to PAD though. |
|
|
|
vasc
ABI values nml and with rest pain ? |
1 nml
0.5 t0 7 claud under or equal 0.3 ~ ischemic rest pain and gangrene |
|
|
|
suture class
Wound classifications ER vs Or |
ER
aseptic -> clean (hair, sweat) _> contam (hair, gravel) DIRTY : 4-8 hrs infected is over 8 hrs sloghing or granulating OR clean clean-contam : hollow organ entered infected : est infection going |
|
|
|
Suture class
size is a 2-0 bigger or smaller than a 0 ? |
A 2-0 means 00
#2 #1 0 2-0 Or 00 3-0 or 000 |
|
|
|
Suture class
suture type these are what kind of sutures ? silk ethibond mersilene nurolone |
multi filiment
|
|
|
|
Suture class
suture type these are what kind of sutures ? ethilon prolene stainless steel |
monofilament
|
|
|
|
Suture class
suture type these are what kind of sutures ? plain gut chromic gut monocryl PDS |
absorbable
monofilament plain gut chromic gut monocryl ( 1-3 weeks) PDS ( 3-6 mos) |
|
|
|
suture class
these are what kind of sutures ? vicryl rapide vicyl panacryl |
multifilament absorbable
vicryl rapide (2 weeks) vicyl (3-4 wks) panacryl (3-6 mos) |
|
|
|
vasc
common site of leg clot PVD or claud ? |
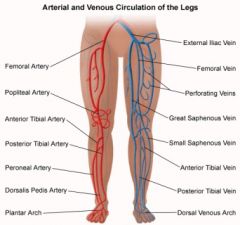
Bifurcation COMMON femoral artery : where splits to profundi/deep and superficial
which is In Hunters canal |
|
|
|
vasc
bypass of plaque in femoral bifurc - indications ? - req to work ? |
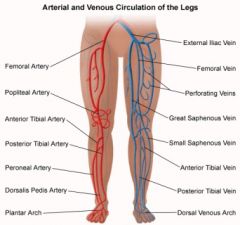
Indications :
Req to work : inflow via aorta, ouflow via patent downstream popliteal A, and 'Runoff' or posterior art in back of leg at trifurc (post tib and peroneal) patent |
|
|
|
vasc
true vs false aneur ? degf aneur |
true : dilation over 2x nl diameter ALL 3 layers
false/pseudo : not all 3 layers like hematoma with fibrous scar |
|
|
|
vasc
pt awakens at night hurts in foot esp over front of foot in this story what makes pain better ? |
REST PAIN
- distal metatarsals or front of foot - better if hangs foot over edge of bed or walks over as pain 2/2 ischemia not like DM neuropathy |
|
|
|
vasc
calf pain when walk better when stop and rest |
claudication
usually better after consist time of rest chronic Diff : neurogenic (nerve entrap ,shopping cart) arthritis, co-arc aorta ?? , popliteal A syndrome ?? , chr compartment syn ?? , neuroma, anemia , DM neuro |
|
|
|
vasc
young man of 35 soldier calf pain when walks better when rests diminished distal pulses observed with forced plantar- or dorsiflexion |
The popliteal artery entrapment syndrome
- rather uncommon pathology -SSX : claudication and chronic leg ischemia - The popliteal artery may be compressed behind the knee, due to congenital deformity of the muscles or tendon insertions of the popliteal space. This repetitive trauma may result in stenotic artery degeneration, complete artery occlusion or even formation of an aneurysm. - One Rx : The patient was treated with myotomy of the medial head of the gastrocnemius muscle and concomitant endarterectomy of the popliteal artery. They later reported four more cases and claimed incidence of this pathology in patients younger than 30 years old with claudication was 40%. Souce Wiki |
|
|
|
vasc
older guy of 65 with popliteal artery aneurysm Important tests to do ? |
Need exam all arteries !
- as over half have aortic/iliac aneu ! - 3/4 have an aneu somewhere - half bilat pop aneu Dx pop aneur : PE -> A gram, U/s Indication for ELECTIVE repair : equal over 2 cm INTRALuminal thrombus (atheroscler or rare bact infection etiol pop aneur) art defomation |
|
|
|
vasc
Size of aneur indicating sx repair ? |
thoracic aorta 7 cm
abd aorta 5.5 iliac 4 cm femoral 2.5 pop 2 |
|
|
|
An 85-year-old woman with newly diagnosed metastatic non–small-cell lung cancer was admitted for pain control. Two days after admission, bluish discoloration of the left great toe was noted. Doppler ultrasonography revealed a left femoropopliteal deep-vein thrombosis. Anticoagulation with heparin was initiated, but there was progressive swelling and cyanosis of the leg (Panels A and B). The patient was referred for prophylactic placement of an inferior vena cava filter. Fluoroscopy revealed that the clot had extended into the left iliac vein and lower inferior vena cava. Filter placement was successful. However, despite continued intravenous anticoagulation and attempts at mechanical thrombectomy, the clinical findings progressed to venous gangrene.
|
NEJM case and image :
Phlegmasia cerulea dolens aka painful blue leg is an uncommon severe form of deep venous thrombosis which results from extensive thrombotic occlusion of the major and the collateral veins of an extremity. Sx: SUDDEN SEVERE PAIN, swelling, CYANOSIS and EDEMA SEQ ! - massive pulmonary embolism hig risk even under anticoagulation - Foot gangrene - An underlying malignancy in 50% of cases. This phenomenon was discovered by Jonathan Towne, a vascular surgeon in Milwaukee, who was also the first to report the "white clot syndrome" (Now called HIT= Heparin induced thrombocytopenia). Two of their HIT patients developed Phlegmasia cerulea dolens that went on to become gangrenous Other RF phlegmagsia : hypercoagulable syndrome, surgery, trauma, ulcerative colitis, gastroenteritis, heart failure, mitral valve stenosis, vena caval filter insertion, and May-Thurner syndrome (compression of the left iliac vein by the right iliac artery). Pregnancy has often been associated with phlegmasia alba dolens, especially during the third trimester when the uterus is large enough to compress the left common iliac vein against the pelvic rim (ie, milk leg syndrome). Finally, 10% of patients with phlegmasia have no apparent risk factors. source wiki NEJM |
|
|

An 85-year-old woman with newly diagnosed metastatic non–small-cell lung cancer was admitted for pain control. Two days after admission, bluish discoloration of the left great toe was noted. Doppler ultrasonography revealed a left femoropopliteal deep-vein thrombosis. Anticoagulation with heparin was initiated, but there was progressive swelling and cyanosis of the leg (Panels A and B). The patient was referred for prophylactic placement of an inferior vena cava filter. Fluoroscopy revealed that the clot had extended into the left iliac vein and lower inferior vena cava. Filter placement was successful. However, despite continued intravenous anticoagulation and attempts at mechanical thrombectomy, the clinical findings progressed to venous gangrene.
|

NEJM case and image :
Phlegmasia cerulea dolens aka painful blue leg Etiol : SEVERE venous OUTFLOW obst due to thrombosis major and collateral vesels -> the extensive venous clots lead to arterial impairment -> cyanosis Main root hypercoag as thrombosis of vessels. Sx: SUDDEN SEVERE PAIN, swelling, CYANOSIS and EDEMA SEQ ! - massive pulmonary embolism hig risk even under anticoagulation - Foot gangrene - An underlying malignancy in 50% of cases. This phenomenon was discovered by Jonathan Towne, a vascular surgeon in Milwaukee, who was also the first to report the "white clot syndrome" (Now called HIT= Heparin induced thrombocytopenia). Two of their HIT patients developed Phlegmasia cerulea dolens that went on to become gangrenous Other RF phlegmagsia : hypercoagulable syndrome, surgery, trauma, ulcerative colitis, gastroenteritis, heart failure, mitral valve stenosis, vena caval filter insertion, and May-Thurner syndrome (compression of the left iliac vein by the right iliac artery). Pregnancy has often been associated with phlegmasia alba dolens, especially during the third trimester when the uterus is large enough to compress the left common iliac vein against the pelvic rim (ie, milk leg syndrome). Finally, 10% of patients with phlegmasia have no apparent risk factors. source wiki NEJM |
|
|
|
vasc
30 yr old male smoker black finger |
BUERGER
digit gangrene gets amp Rx stop smoking sympethectomy Sx recall |
|
|

68 yr old
toes hurt swelling started 4 days ago PMH: HTN, afib on anti-HTN and warf PE : sharp demarc at base toes tender to touch, nml periph pulses legs, ABI nml |
Also known as "trashfoot," blue toe syndrome is an arterial embolic disorder. Thrombogenic and atherogenic sources for emboli need to be considered in the diagnostic work-up. Transthoracic echocardiogram was performed in this patient and was negative for vegetations or clots. Computed tomography scanning revealed no evidence of abdominal aortic aneurysm or atheromatous plaque.
A thrombogenic etiology initially seemed more likely in this patient, given his known atrial fibrillation, the distal location of the embolic event, and its simultaneous onset in adjacent toes. However, when review of laboratory values confirmed consistently therapeutic anticoagulation and no cardioembolic source was found on transthoracic echocardiogram, attention shifted toward a possible atherogenic source. He was admitted on abx as w/u pended but stopped. d/c pain meds. outpt consult vasc sx to see if need amp but wait it out Ref AAFP Cellulitis Erythema, edema, warmth, pain with or without fever Cryoglobulinemia Recurrent palpable purpura on lower extremities with or without arthralgias and renal disease Warfarin skin necrosis Onset during first week of warfarin use in areas of adipose accumulation Blue toe syndrome Acute onset of painful cyanotic discoloration caused by embolism in a vascular distribution pattern |
|
|

vasc
45 year old male also has ulcer on ankle |
Cryoglobulinemia may lead to purpuric or gangrenous lesions in the distal extremities, and its incidence is increasing recently because of its association with hepatitis C infection. Skin lesions from cryoglobulinemia typically would be more widespread and be unlikely to affect only two adjacent toes
Type 1 cryoglobulinemia is often associated with lymphoma. Type 2 cryoglobulinemia is often associated with hepatitis C infection. Symptoms may include a rash on the lower limbs, arthritis, nerve damage and tissue necrosis of affected areas. |
|
|
|
vasc
female takayasu |
Pictured below is a close–up view of an angiogram of the left vertebral and subclavian arteries in a patient with Takayasu's arteritis. Note the narrowing and irregularities that occur at several sites, and the “corkscrew” configuration of one vessel segment near the junction of the two arteries. These changes, caused by inflammation in the blood vessel wall, sometimes cause complete blockage of the artery.
signs of occusive phase (after inflam systemic one) - pain/claud limbs that occurs during repetitive activities, such as pain in the arm that occurs while using a handsaw - The symptoms also include dizziness upon standing up, headaches, and visual problems. - no palp pulses in the neck, elbow, wrist, or lower extremities - “bruits” - High blood pressure is common, but blood pressures taken in the arms may be read as falsely low if there is a narrowing of an artery high up in the arm. |
|
|
|
vasc
arteriogram pitfalls |
Prestudy : iodine, shellfish allergy, use under 200 cc
Dose-Independ rxns : asthma, laryngo edema, sasm, CV collapse post-agram expanding hematoma : would be pulsitile, direct pressure 30 min then explore wound vasc spasm : if dec pulses post-proc that are up to 1 hr ; of longer consider art injury or clot Relative CIL coagulopathy, allergy contrast, shellfish allergy, renal insuff, dehydr, metformin within 48 hrs, CHF, rencent MI, CT dz like ehlers-danos Orders to do pre-angio: hold warf 3-4 days hold metform pre Iodine contrast (ok before gadolin MRA) correct coagpathy and low plts clear liqs 8 hrs hydrate if entereing dirty area give abx if h/o asthama etc give rxn prohy |
|
|
|
vasc
What is DSA ? |
dig substraction angio
USES contrast inject dye vein or art computer floroscope subst bones and soft tissue so only see art tree Magnetic resonance imaging see patent distal vessels with minimal flow, eval carotid bifur or Abd aorta. NO CONTRAST uses gadolin |
|
|
|
vasc
imaging AAA ? |
spiral CT
|
|
|
|
vasc
Doppler types |
doppler pulsed wave : flow velocity and resistance to flow
doppler color : flow direction and turbulence nml doppler lower extremities : triphasic w. cardiac cycle with stenosis changes to monophasic pattern of forward flow in systole only (no more retro backwash with 1st pt diastole and low vel in late diastole) |
|
|
|
vasc
angiogram of aorta and head when do you enter R vs left side ? |
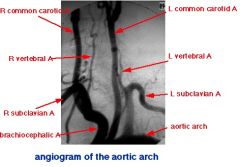
You enter LEFT subclavian as reduces stroke risk. Can get to asc aorta w/o crossing R brachioceph and L comm carotid.
EXCEPTION: Use right if want to study asc aorta, R subclavian, R vertebral or coronary arteries or L is bad. Note the three vessels taking off from the top of the arch from right to left: * the brachiocephalic (AKA "innominate") artery * the left common carotid artery * the left subclavian artery |
|
|
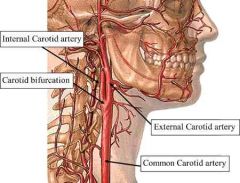
vasc
name branches of ext carotid in head ? |
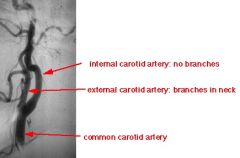
trick : ext carotid has no branches in head, branches in neck
|
|
|
|
vasc radio
what is gadolinium |
Gd atomic number 64
solid lanthanide, solid mathal at RT MRI : Because of their paramagnetic properties, solutions of organic gadolinium complexes and gadolinium compounds are used as intravenous MRI contrast agent to enhance images in medical magnetic resonance imaging, Ex, Magnevist. in the 3+ oxidation state, the metal has 7 unpaired f electrons. This causes water around the contrast agent to relax quickly, enhancing the quality of the MRI scan. As contrast, dangerfor those with renal dz who cannot chelate it and then it become sunbound and . Cz skin rxn. In X-ray, gadolinium emits green emahnce image. Gadolinium oxyorthosilicate PET as scit to detect neutrons |
|
|
|
vasc
doing a balloon PTC / PTA means what ? |
percut translum angioplasty
Indications : SHORT (under 5 cm) NON-occluding lesions with less extensive atherosclerosis athero, taka, fibromus dyspalsia, failure of graft When gradient is more than 15-40 in artery or more than 3 in vein Outcome : 5 yr patency 90% with 2nd inteventions too radrecell p 274 |
|
|
|
vasc
pt fails PTC what now ? |
repeat it
stent percut atheroectomy sx bypass laser ablate |
|
|
|
vasc
stent graft is what ? ind ? |
Ind : long seg of stenosis/occ so PTA (balloon less favorable) , ulcerated plaque, failed PTA (resid stenosis over 30/10 or dissection), recur
DEf: dacron/PTFE graft with self expanding metal frame, go via femoral usually for aortic diss/trauma/aneur Need annual f/u CT or MRI |
|
|
|
vasc ICU
PICC line CI |
CI
1. need line longer than 3-6 mnths 2. severe coaglopathy 3. central venous occ [realtive] 4. thrombophlebitis 5. bactremia sites: Arm basiclic, brachial, ceph antecub fossa, Comps : thrombophebitis #1 3-10% check this sepsis 1-3% |
|
|
|
vasc
what imaging favored for aneur - pre-op : angio for branch vessels and pre-op - follow over time : - accurate to measure size : - pt allergy contrast : - MRI benefits: |
vasc
- pre-op : angio for branch vessels and pre-op, assesses mesenteric ischemia, HTN, renal dysfx, horsekidney and claud - u/s to follow over time not for acute - accurate to measure size : CT, MRI - pt allergy contrast : MRI - CT: wall thickness, loc and if leak or rupture - MRI benefits: more detail about lumen and surface anat and relation to renal artery, acc size mesure, any place, contrast allergy, reproducible |
|
|
|
vasc
* CT : saccular anur shape, inflamm around it, breakdown of wall * Loc : aorta > cerebral . mesentary > spleen > renal Pt recently d/c from hospital |
MYCOTIC aneur
RF : bact endo, sepsis, IVDA , immcomp Need sx as expand and rupture Etiol: weak art wall at bfurc due to bacteria |
|
|
|
gi bleed
bleeding not seen well with tagged rbc or angio ? |
gastric varices or esoph VENOUS bleeds seen better with Ct
|
|
|
|
vasc gi
80 yr old man with afib, PVD, smoker. severe abd pain after eating weight loss fear of food |
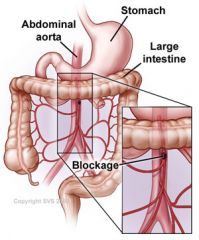
mesenteric ischemia
CHRONIC : only shows when all 3 branches occlude, Cz athero ACUTE : Cz emboli thrombi expanding aneur, hypotension, post-op Dx: trad gold standard selective mesenteric angio but now using CTA and MRA. 3 vessels celiac and IMA and SMA. Signs infracted bowel : gas in wall , thick wall, gas in portal vein (late sign), free air w. perf On Benema : "thumb printing" from gas in wall Rx: broad abx and agressive fluids. Lap and resect dead bowel. In 24 hrs can do re-look at bowel. Can try angio for stent, lysis clot if localized dz, papaverdine given if see occlusion on aGram. thrombectomy is possible but very risky. UCV sx p59 |
|
|
|
vasc
DVT gold stand dx |
venogram
acute : has menisucus, and tram tracks as contrast outlines thrombus chronic : "linear filling defects" as syncytia or collaterals detours vessels |
|
|
|
vasc
bad aorto illiac dx unilateral Pt : elderly 85 year old , bad risk for comps from abd sx, had prior graft and it is infected |
aXILLo BI femoral graft as better than unilateral
Other extra-anatomic bypass : best is femoral-femoral 5 yr patency 50-70% |
|
|
|
vasc
aorto femoral bypass VS aorta iliac bypass ind ? |
aorto femoral better patency
90% 5 yr patency, 10yrs is 75% Others : aorto-iliac endarterecomy if local and distal vessel nml |
|
|
|
vasc
pt has gangrene, rest pain, ulcers long term |
prob multisegment
poor life expectency get venous and art ulcers NonOp: no smoke, Meds: oentoxifylline and CILOSTAZOL OP: revasc , fem-pop bypass with synthetic or saph vein and RSVG best patency Endaterectomy not as useful as limited to sht lesions at adductor cancal or profunda origen |
|
|

vasc
left mild arm claud arm fatigue +/- syncope attacks , vertigo, confusion, blind, dysartria, PE: upper arm BP discrepency bruit above clavicle |
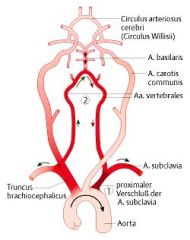
subclavian steal
Dx w/ angio flow reversal in vertebral A. When move ipsi arm (usually left) increased demand causes retro flow from vertebral Art "stealing" from vertebrobasilar circ. PAtho : dec flow post cerebral A when blood goes retro to vert A to SCA When OR: incompac arm claud hand emboli or to post cerebral circ symptoms subclav steal ** fix carotid first if have both issues Note: some pts only have arms sx not carotid. OR: sx bypass or endovasc stent |
(a) TOF sequence with a saturation band above the section demonstrates absence of signal in the left vertebral artery (arrow). (b) TOF sequence with a saturation band below the section demonstrates signal corresponding to retrograde flow in the left vertebral artery (arrow). (c) Coronal maximum intensity projection (MIP) image from contrast-enhanced MR angiographic study demonstrates occlusion of the proximal subclavian artery (arrow), with reconstitution distal to the origin of a patent left vertebral artery.
|
|
|
vasc ortho
amp sites and why for ischemia ? |
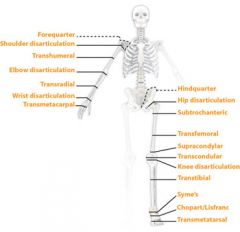
BKA : isch up to med malleoli, CI if dead above ankle and likley to fail if no femoral pulse; with pop pulse 95% success w/o 82%
AKA : alderly and non amb, contractures at knee/hip hip disartic : extensive leg ischem, prox gangrene, poor outcome for PVD with sepsis use guillitine not flap |
|
|
|
vasc AAA
|
75% asymto at dx
in pts 1 degree relative known AAA 11% risk so recc u/s screening RF rupture DIASTOLIC HTN, lr at dx, COPD |
|
|
|
vasc
Have AAA and want to do repair , pre op |
* no h, nml ECG -> repair
* stable known CAD -> echo/dipy or thall and consider revasc before * clin severe CAD -> Need Cor Art revasc before AAA repair unless percut If get a CABG wait 4-6 weeks to fix AAA. |
|
|
|
vasc
AAA and COPD |
more risk rupture
try repair retroperitonreal also bene's of this approach : less adhesions, no interfere GI or GU, see suprarenal better |
|
|
|
vasc
AAA repair pt 85 lots of co-morb |
try endovasc repair
|
|
|
|
vasc
AAA repair pt 85 lots of co-morb |
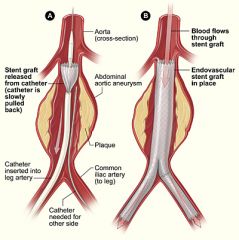
try endovasc repair
|
|
|
|
vasc
AAA rupture presenting signs A * pt has h/o AAA and unstable VS B * pt has no h/o AAA and stable |
A * GO to OR, no anesth until scapel in hand as anesth -> hypotension
B * CT then if needed OR Comps of repair : If reach hx alive mort 50% renal failure 75% isch colitis 5% bloody diarr, high wbc, perioitits spinal cord ischemia |
|
|
|
vasc
DM vasc dz features |
lower down on leg (spares aortoiliac) hits smalller vessels
younger |
|
|
|
derm plastic melanoma CA
skin cancer staging mets and work up ? |
bresLOW THICKness more accurate
Clark depth of invasion spread to bone : bone scan spread to liver : do u/s and CT nodular solid masses |
|
|
|
derm plastic CA
pre skkinv CA conditions |
2/3 melanoma de nov0
1/3 from pre malig conditions Actinic keratosis -> sqaum cell nevi super spreading a marker of inc risk congen nevi dysplastic nevi |
|
|
|
derm plastic CA
ABCDE diameter that is bad invasion level that needs prophy lymphadectomy ? |
over 6 cm ABCDE
under 0.75 mm invasion do not need prophy removal of LN. Can use sent node mapping. |
|
|
|
derm anal
obese woman , lots of cystic acne job where sweats alot 1st stage "cold" lump in groin,rounded and hard, painful, fever, induration. Skin near it shiny and swollen 2nd stage "mature" : liquid green pus tracts open at sides of lump draining as multiple fistula tracts |
suppurative hidradenitis
SItes in males perianal, female areaola, axilla in females #1 cold stage : abx and compresses warm : sx I&D if chr and scarring can need sx wide excision of apocrine tissue |
|
|
|
abd liver
scan shows periph nodular enhancement |
FNH
|
|
|
|
anal
chr anal fissures treatment |
Sx :
hypertrophic papilla anal ulcers , sentinal pile Do sigscope for crohns Rx: Lat internal sphincterotomy biopsy ulcers for cancer |
|
|
|
anal
anal fistula |
sx : anal itching , d/c on underwear
Use Goodsalls rule to tell if form ant or post crypt usually from anorectal abscess W/U : Recto sig scope for term colon and rectum and usually bar enema Can try fistulogram to define tract if needed Nearly always need sx fistulectomy to unroof tract leaving in seton (piece of material) to cz fibrosis on purpose CI sx are HIV and IBS comps are injury to puborectalis czing incont |
|
|
|
colon CA
old man alternate D and const wt loss dec stool caliber occ red blood in stool What side of colon ? |
More like in left colon :
rectum or sigmoid apple core as spread circum so cz obstructive symptoms |
|
|
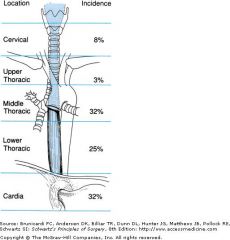
gi CA esoph
Pt : smoking man 75 yr Af Amer Sx hard swallow, losing wt Postive LN supra-clav on left (Virchows) anemia, |
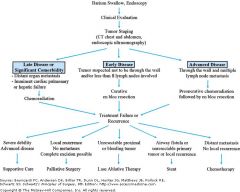
esoph CA
usually squamous which is in upper 2/3 spreads locally to mediastim easy, no serosa Dx: endo with biopsies multiple times as lots false negs Rx: If can be cured try Pre-op chemo and rad -> sx. Otherwise try pall radio or chemo VS adeno in lower 1/3 related Barretts |
|
|
|
abd biliary acute abd
pres of gallstone ileus |
elderly lady
h/o of 3 years of stomach upset / heart burn presents obstipation / bowel obstruction BUT no h/o sx, no hernias , no periotontis , nml liver tests Radio : dilated jej loops and "FILLING DEFECT" which is where stone is so contrast can't fill it Rx rapid lap sx and enterotomy pics ucv p43 |
|
|
|
gi
upper gi bleeds endo shows bleeding peptic ulcers Rx ? |
If bleeding active or see vessels at ulcer base : under endoscope use epi, polidocanol , cautery, laser sx.
Use IV PPI to reduce risk of re-bleeding. Most common bleeders are duod ulcers, 40% : vagotomy and pyloroplasty For severe gastric ulcers occ gastrectomy |
|
|
|
gi
upper gi bleeds endo shows hemmorg gastritis rx ? |
ice lavage
and angiographic vasopressin |
|
|
|
abd gi obst
how does obst lead to perf ? |
* pressure builds up stream of block as air and fluid accum
* then pressure in lumen exceeds post-capillary venule pressure impairing blood flow * bowel necrosis and ischemia |
|
|
|
abd gi
abd tympanic distended and tender no ridgid or rebound tenderness Bsounds high pitched and increased |
bowel obst
On KUB : string of beads of step ladder as air fluid levels above obst |
|
|
|
abd gi
causes bowel obst which bowels ? |
adhesions, hernia, cancer
infants : hernia, intuss volvulus : cecum or sig colon cz obs with less vomitingand of lg bowel ot sm bowel 75% is small bowel Rx NPO, fluids, NG aspir and decomp, fix lyte and acid/base imbalence Then lap and fix obst |
|
|
|
gi panc
what lies behind neck of panc ? |
SMV
|
|
|
|
gi panc
panc - itis effect on gut ? signs on films ? |
adynamic ileus
dehyd and shock fluid shifts AXR: sentinel loop** , colon cutoff ** sentinal loop most common sign on Abd xray. It is area of lg GI near area of inflammation so in panc it is jej and in appy can be RLQ. u/s : phelgmon and panc necrosis |
|
|
|
gi panc abd
ranson admit |
GA LAW
georgia's law glu over 200 age over 55 LDH over 350 AST over 250 WBC over 16,000 ** not amylase or lipase |
|
|
|
gi panc abd
ranson less than 48 hrs |
C HObbs like calvin and hobbs
ca under 8 Hct drop 10% O2 under 60 base deficit over 4 bun over 5 increase seq over 6 L |
|
|
|
gi panc abd
* cause of panc and Ca * % pts chr panc get panc ca |
high Ca -> panc so hyper PTH
2% get CA |
|
|
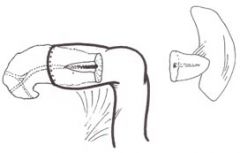
gi panc
treatment for chr panc when duct large/dilated and looks like chain of lakes |
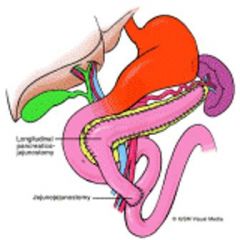
Fig. 2A —Puestow procedure = lateral / longitud pancreatico-jejuno-ostomy
Diagram of anatomy after modified Puestow procedure. The pancreas is filleted to expose main duct from neck to tail, and ductal calculi are removed. Roux loop of jejunum is anastomosed to "capsule" of pancreas with direct drainage of main and secondary pancreatic ducts into lumen of jejunum over 8-10 cm segment. This procedure is best performed if main pancreatic duct is significantly (>6 mm) dilated. |
|
|
|
gi panc
to drain panc |
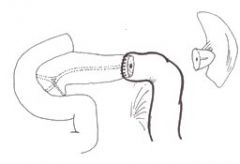
Duval :
partial drainage of panc to help pain distal/caudal amp of panc which is a near total panc-ectomy Developed on the basis of presumption that a single stricture of duct of Wirsung near the ampulla was responsible for the obstructive pathology and terminal drainage would treat the condition. It consists of a distal pancreatectomy with splenectomy and retrograde drainage of the main duct into a defunctioned jejunal loop (Fig. 1). |
|
|
|
gi panc
frey's |
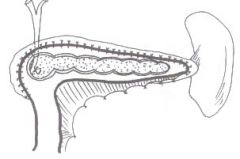
for chr panc
* Ind : chr panc with comps liek cysts or still pain after puestow / lateral panc jej. * CI in cancer as leaves behind panc head but does a core resection of head * also saves duodenum |
|
|
|
gi panc
pt with acute panc but pain still there after ? 2 weeks mild fever wt loss tender epigastrium and ileus |
Suspect panc pseudocyst
W/u amyylase/lip ,bili, CBC See high SBS US : fluid fillled mass and CT will show mult cysts ERCP to tell if common or non-commun (connect to panc duct or not) MUST biopsy cyst wall to rule out cystadenoCANCER (adenoma or carcinoma) Comps include bleed into cyst Rx wait 6 weeks to resolve, half do, before drain for walls to get thick to hold sutures Drain : infeccted ones (percut drainage and IV abx) , over 5 cm, caldify wall or thick wall |
|
|
|
gi panc
cyst not sticking to stom or duod (in which you take out part of that) |
roux en Y cysto-jejunoostomy and drain into roux limb jej
|
|
|
|
gi ulcer
duod males 35, burninf pain empty stomach H pylori ? ESt Dx ? Ca ? Who ? r/o ? |
H pylori duod 70-90% vs stomach only 50-70
Loc : 1-2 cm from distal pylorus Est Dx : endoscopy with antral biopsy 90% and does beyond duod, CLO test, serology, VS upper GI series only sees duod and 70-80% accurate CA : rarely Who ? If multiple r/o Zoll-Ellison |
|
|
|
gi ulcer
med mgt and when do sx |
6-8 weeks med mgt :
PPI cytprotective agents treat h pylori : lansoprozole, amoxi, clarithro Try sx if not better after 8 to 12 weeks OR bleeding that won't stop and trans over 6 units, usually with post ulcers and into gastduod ulcers OR perf, more with anter and acute pain and free air OR gastric outlet obst more duodo r near bulb |
|
|
|
trauma airway
emergent airway page a trach falls out what to do ? |
rookie move is to shove new trach in old hole, often get in wrong space.
FIRST : plain old endo tracheal intubation Second : can't do ETT (airway cancer or Max-fac trauma that was cause for trach) use NG/cook/eschmarr into trach hole. Then use this a guide to feed in new trach. |
|
|
|
Gi panc
tests for steattorhea ? |
fecal fat
fecal lactase |
|
|
|
gi panc
role of octreotide ? AE ? |
convert high output fistula to low output fistula.
Will not close hole. SE include cut off blood to spleen. |
|
|
|
CA syndromes
lynch ? |
lynch
hered non polyposisi coli auto dom CA stomach DREbyrly age 40 + FOBS |
|
|
|
CA Gi stomach
RF ? |
Prior gastric sx (reflux of bile)
including partial gastrectomy atrophic gastitis pern anemia h pylori |
|
|
|
Gi CA stomach
spread ? |
* drop mets to pelvis like to shelf above rectum (note : note drop mets as pieces to lumen)
* direct * lymph * hemat So met w/u : * CT abd + pelvis * CXR chest and if + do CT chest NO BONE scan and NO brain scan Top distant mets are liver and lung Source : Mont Reid Prof hr ITSessions |
|
|
|
chest thoracic lung
mediastinoscopy |
mainstay to eval cervical LN
Ind : stage lung CA or dx cause of hilar LN Better than VATS Have to sample nodes at 3 stations, ipsi and contra lateral paratracheal nodes levels 2,3,4 and subcarinal 7 Can access nodes AorPulm window. AE: risk 1-2% bleed into chest req opening chest Incision 1 finger above sternal notch |
|
|
|
Gi ulcer
define peptic ulcer disease |
includes ulcers in stomach and duod
|
|
|
|
gi ulcer
what cells make acid ? loc ? stimulus ? |
Parietal cells make acid and intrinsic factor
Body and fundus (NOT antrum even though sometimes remove this in sx) + gastrin from antrum via blood + Ach (vagus) + histamine H2 cephalic phase Stim for gastrin ? stretch antrum stretch aa gastric phase acid secn |
|
|
|
vasc
5 days post AFBG 1 loose BM some red blood |
* concern for IMA mesenteric ischemia
* Dx sigmoidoscope / proctoscope If see black spots it is real late and to to OR ASAP. If this is negative do not need colonscope, it is not mes ischemia as IMA only up to ___ flexure and you see with sig-scope. |
|
|
|
vasc
10 year post AFBG hemetemsis |
aorto enteric fistula
|
|
|
|
derm CA
cancer bulging red / black local spots recur after excise |
merckel cel carcinoma
neuroendocrine tumor do excision, LN excision rad/chemo f/u LN exams has 50% local recur rate stage 2 if regional nodes, stage 3 if N1 |
|
|
|
trauma
deaths are when ? |
golden hour : head injury, hemm shock ,
min to hours : exsang, PTX 14-21 days : "second hit" MOFS , sepsis |
|
|
|
peds gi embry
desc why mid gut volvulus using embry terms ? |
embry
midgut goes out umbil week 6 returns week 10 whilst spinning COUNTER clockwise 270 degrees SMA. Abn rotation causes Ladds bands fixing at 2ND part DUOD and all of midgut hangs on SMA -> obst and vomit about day of life 2. VERSUS midgut volvulus when impair perfusion and SMA -> atresia or gangrene, Foregut : 90 rotate celiac A ....hepatic divertic and panc buds mid 270 CClock SMA .... hind septates IMA foregut rotates 90 degree |
|
|
|
peds gi embry
sm int "apple peel" appearence |
midgut fails to rotate properly as returns to gut,
impairs perfusion SMA -> necrosis/gangrene -> atresia of sm int "apple PEEL" appearence no dorsal mesentary affected gut spirals around vessel |
|
|
|
anat step 1
gi abd divisions blood structures nerves |
foregut celiac tr , great splanchnic T5-9
...abd esoph, stomach, duod part, liver, GB, panc, spleen midgut SMA lesser sphlancnic t10-11 ....aftermaj duod papilla to 2/3 trans colon hindgut IMA least sphlannic ... splenic flexure to anus |
|
|
|
gi cancer CA hemmorroids anat
anus anal canal rectum nerves and blood to here ? |
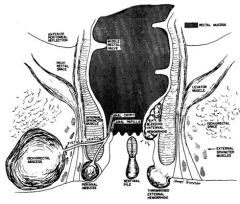
ABOVE pectinate line ?
insensate and adenoCArcinoma Visceral nerves IMA : superior rectal A vein sup rectal -> IM vein -> portal vein Below ? ext hemm painful and sqaum cancer nerve : somatic blood : inf rectal from internal pudendal A Vein : inf rectal -> internal pudendal -> int iliac ->IVC |
|
|
|
peds gi
day 2 - polyhydram - bile vomit and stomach distension |
duod atresia
failure to recanulate (unlike sm int atresia which is ischemia from failed midgut rotation and block SMA) - polyhydram - bile vomit and stomach distension |
|
|
|
gi
patient with ascites esophageal varices never drank alcohol splenomegaly ? UNrelated : hemm that alcoholics get, painful or not ? |
slpenic A clog ->
gastric vein varies only which are esophageal ones and in lower esophagus and drain to azygus alcoholic hemm not painful as get internal ones, as sup rectal drains to portal and painless |
|
|
|
gi stom
where is antrum body fundus |
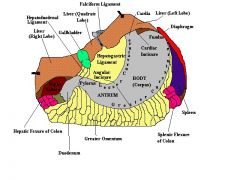
|
|
|
|
gi
CCK stimulus ? inhibition ? action ? |
made by : I cells duod and juj
Stim : Fatty acids and monoglyc , small pepetides, aa and decreased by secretin and stomach ph under 1.5 ACtion: + GB contract, relax sph Oddi, + panc enz secn, i nhibit stom empting |
|
|
|
gi
secretin source ? stimulus ? action ? |
source ? S cells duod
stimulus ? FAtty aids in duod, low ph in duod action ? inc panc bicarb secn, inc bile production, dec stomach acid secn action ? |
|
|
|
gi
K and colon ? iron and duod ? |
K actively secretied by colon if excess K diet and stim by aldosterone
free heme iron absorbed by duod |
|
|
|
gi esoph
what is esoph web vs schatzi ring |
a web is above arch and a muscosal fold in upper esoph and related to sq cancer esoph and post cricoid
VS schatzi ring ring musoca at squamocolumnar junction below aortic arch |
|
|
|
gi stom
2 kinds gastritis A and B ? |
gastritis A Fundal
autoimmune reltd pern anemia, achlorhydria, and no Ifactor 90% antibodies par cells and 60% to IF gastritis B due to H pylori , a "reactive like gastritis" and most common and related to metaplasia |
|
|
|
gi stom esoph
anor wt loss anemia epigastric pain left supraclav LN enlarged |
stomach Carcinoma CA
Sites: antrum and pylorus in 60% RF hypochlor nitromasmine diet Histo : signet ring cells sign gastric carcinoma |
|
|
|
gi stom ulcer
with head trama burns ? become CA ? |
head cushing
burn curling rare stomach ulcers -> CA no duod ones |
|
|
|
gi CA
lymohoma found what type usualy ? |
non hodkins lymphoma large cell diffuse
If immunosp could be primary lymph of sm int MALToma more slow prog related to h pylori and may regress with abx |
|
|
|
tropical sprue
|
related licing tropics , vietna, P rico
like celiac but not better with no gluten and ALL of sm bowel relate dto toxogenic e coli |
|
|
|
gi
man malabsorb LN adeno joint pain |
whipple dz
Rare PAS+ bug bacilla trophery whippelli macros in lamnia propia |
|
|
|
gi bleed
loc most bleeds angiodysplasia |
lg bowel
esp cecum |
|
|
|
gi CA
peutz what type polyps they get ? |
harartoma so not premalignant and in all of GI tract
|
|
|
|
gi ca
dental abn tumor in jaw with soft tissue and bone in it as teen colon polyps |
gardner syndrome
colon polyps and desmoid tumors : have soft tissue and bone and often in mandible risk colon CA 100% |
|
|
|
gi liver
portal HTN ascites with high ptn VS low ptn |
portal HTN
ascites with high ptn / exudate : Budd chiari (pancreatitis) low ptn transudate cirrhosis |
|
|
|
ascites gi liver
high ptn exudate |
peritonitis or CA in peritoneum
portal HTN and panc or Budd Chairi hypothyroid lymph obst |
|
|
|
ascites gi liver
low ptn transudate |
cirrhosis
....hypo ptn emia nephrotic syndrome .....hypoalbuminemia CHF consti pericarditis / R heart failure |
|
|
|
gi
acute tachycardia fever jaundice shock ileus high amylase (lipase high after 3 days) high leukocytes |
acute hemmoragic pancreatitis
|
|
|
|
gi peds
biliary atresia extra vs intra hepatic |
extra hepatic
first weeks of life jaundice , dark urine, light stool, hepatosplenomegaloy intrahepatic sometimes related to alpha1antitryp def infancy presentation cholestiatis, itching, growth retardation, high serum lipids ictrus when bili at 2 |
|
|
|
gi peds
neonatal hepatitis |
50% idio
30% alpha 1 anti tryp rest TORCH, viral, metabolic, extra hep bil atresia |
|
|
|
gi liver
women of 40 itchy , xanthomas high alk phos what is dz ? what specific tests ? |
prim bil cirrhosis
anti mitco ab in over 90% high chol On ERCP : see biliary tree VS secondary biliary cirr see bile lakes due to stasis histo path : granulomas destroy bile ducts |
|
|
|
gi liver
man with diarrhea pale stool and dark urine |
pri sclerosing cholangitis
pANCA ERCP : "beading" as alt structure and dilate and dz in extra and larer intra-hep ducts |
|
|
|
gi liver
women 20-40 yr old anorexia malab , fatigue, abd distension, dark urine and itch LFT and bili high |
high IgG and ANA
AUTOIMMUNR hep relap and remit course retd autothyroid and sjorgens have chr anemia and high ESR |
|
|
|
gi liver
bad cancer liver related to vinyl chloride ? |
angiosarcoma
|
|
|
|
peds gi liver CA
child hepatomegaly vomit and diarr wt loss high AFP |
hepatoblastoma
maligmant |
|
|
|
gi liver CA
assoc with hepatocell CA ? |
ascites
wt loss fever POLYCYTEMIA HYPOGLYCEMIA 50-90% HIGH AFP death from bleed or liver failure. mets often 1st to lungs via hematos portal and IVC. |
|
|
|
gi liver
lab signs fulm metabolic hepatitis |
hypo glycemia
high amm low K low cacemia acid base abn coag abn |
|
|
|
endo thyroid
pecent people pyramidal lobe ? |
75-80% goes UP from isthmus
|
|
|
|
endo thyroid
percent ppl pyramidal lobe thyroid ? |
75-80%
it goes UP from middle isthmus bridge |
|
|
|
endo thyroid
|
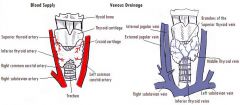
2 arteries :
Superior thyroid artery from EXTernal carotid Inferior thyroid A from subclavian thrycervical trunk sometimes Ima from aortic arch or innomicate A Veins (3) superior thy V -> interal jug middle thyroid V to in jug inferior thy vein to brachiocepgalic |
|
|
|
endo thyroid
hyperthyroidism A. scan show diffuse uptake ? B. scan shows multiple nodules hot ? |
A. graves and TOC radioabltion
B. Toxic multinod goiter and recc surgery (radio less successful and med less less effective) .... if one nodule nodule or lobectomy .....multi nodules ..lobetomy or contraleteral subtotal lobectomy |
|
|
|
endo thyroid
when sx for grave's ? |
TOC is radioablation
Sx when can't do radioablate ...pregnant ...young First get patient euthyroid with PTU/methamozol and b blockers Is an immediate cure VS radio take 2 months |
|
|
|
endo thyroid
post subtotal thyroidectomy pt with distoriented fever tachy vomit and diarr |
thyroid storm
Best avoided by being euthy w/ drugs pre-op Rx fluids PTU/meth b blockers NaI or lugols hydropcrotisone cooling blanket (and with subtotal can get persistant hyperthyroid) |
|
|
|
endo thyroid
female unilateral neck pain thyroglossal duct cyst perhaps or goiter fever EUTHYROID dysphagia |
thyroiditis
Rx IV abx , sx drainage RF thyroglossal duct and/or goiter bugsL come via lymphs, staph, streppyogenes, pnem coccs |
|
|
|
endo thyroid
female HYPERTHYROID post URI tired, sad, neck pain and fever unil lat sweling thyroid and over it is red firm tender thyroid |
subacute deQuervain
get transient hyperthy then hypothyroid Rx: it is self limited pain rx with NSAIDS |
|
|
|
endo thyroid
Pt alz / downs / fam hx thyroid dz painless enlargement of thyroid ab present euthyroid or 20% at diag hypothyroid Rx ? |
hashimoto's AI thyroiditis
see cell hyperplasia Rx thyroid hormone and often goiter regresses if no regessino of goiter partial thyroidectomy |
|
|
|
endo thyroid
reidels fibrosis replaces thyroid and isthmus |
if airway issue can do
isthmectomy othewise med tx with steroids |
|
|
|
endo thyroid
percent thy single masses that care malignant ? FNA rates false + and - ? |
15% malignant
false + rate 1% false - 5% FNA less reliable if h/o radiation so try OR biopsy |
|
|
|
endo thyroid
role of u/s ? |
tells if multiple nodules
If FNA benign can use u/s to follow size and thryglob levels to track over time. |
|
|
|
endo thyroid
FNA of nodule is " suspicous" what next ? If "malignant " |
usually follicular (incl huethle cell)
Do I 123 scan 85% will be cold and those are 10-20% malignant FNA "malignant" surgery 5% are hot and 1% malignant |
|
|
|
endo thyroid
cyst what to do ? what cysts go to OR ? |
drain it completely
GO to OR for eval and biopsy if : over 4 cm or complex recur after 3 drainage tries |
|
|
|
endo thyroid
role of uptake scans for nodules ? |
less use now with FNA
if FNA benign -> watch with u/s and labs If FNA malig -> OR Only if FNA suspiscius might you use scan |
|
|
|
Endo thyroid
After thyroid sx A pt is hoarse B pt has airway obst C deeper and quieter voice , |
A unilat recur laryngeal cut
B bilat recur laryn cut C superior laryn cut |
|
|
|
Endo thyroid
TRH vs TSH Synthyroid, |
A2
Endo thyroid TRH from hypo TSH from ANT pit Synthyoid = thyroixine = T4 T12 is 7 days, |
|
|
|
Endo thyroid
Nodule Multiple non diagnositic FNA Low TSH What test next ? , |
A3 I123 scan
|
|
|
|
,Endo thyroid
Nodule Thyrotoxicosis Low TSH What test ? |
I123 scan
|
|
|
|
Endo thyroid
When sx for multi nod goiter ? |
cannot rule out CA (1% multi nod are malignant)
Compressive symptoms Cosmetic |
|
|
|
Endo thyroid
ho radiation nodule neg FNA what to do ? |
most remove nodule
|
|
|
|
Endo thyroid
Pt has gardner’s Had neck irradiation for hodkins Now had thyroid nodule What kind of CA are you worried about ? , |
Papillary
|
|
|
|
Endo thyroid
How pap thyroid CA spread ? |
P Papillary means Palpable Lymph nodes
Lymph to cervi nodes, and slowly LN + not related to prognosis really, |
|
|
|
Endo thyroid
papaillary thyroud CA Under 1.5 cm No ho radioation to neck Rx ? , |
Thyroid lobectomy and isthectomy
Neat total thyroidmectomy Total thyroidmectomy Post-op thyroid meds to suppress TSH, |
|
|
|
Endo thyroid
Thyroid pap CA Over 1.5 cm Bilat + Cerv node mets, OR ho neck rad Rx ?, |
Total thyroidectomy
Post-op thyroid meds to suppress TSH (if + lat nodes need mod rad uni neck dissection) (if + cerv nodes need central neck dissection), |
|
|
|
Endo thyroid
What is “lateral palpable cervical LN” ? , A11 a misnomer, it is pap CA of thyroid |
Rx with modified uni neck dissection,
|
|
|
|
Endo thyroid
Post op fu pap CA thyroid |
Use Thy hormone to suppress TSH
Scan with I123 for mets outside thyroid area, |
|
|
|
endo thyroid
spread of follicular CA ? what percent of CA ? |
follicular os 10% thyroid CA
spread hematogenous -> often to bone. F's follicular far away mets : blood and to bone Female 3:1 FNA ...NOT favorable rubbery and encapsulated 50% 10 yr survival Cannot dx invasiveness by FNA as need to tell if into capsule or vessels. |
|
|
|
endo thyroid
follicular CA thyroid RX ? |
thyroidectomy TOTAL
post-op I123 scan |
|
|
|
what is huerthle cells CA thyroid ?
|
a type of CA from follicle cells
5% total NO UPTAKE OF iodine FNA can tell cells but not maignancy Mets via lymphs Rx total thyroidectomy |
|
|
|
endo thyroid
meduLLRY |
5% TOTAL
M's medullarly MEN II aMyloid makes calcitonin Median LN dissection if LN involved Modified neck dissection if lateral modes + does spreads lymoh and hemetog POOR Iodine upake |
|
|
|
endo thyroid CA
meduLLRY survival |
if found from screening fam members w. calcitonin 10 yr survival is 95%
if when CA palpable under 20% |
|
|
|
endo thyroid CA
medullary rx ? |
total thyroidectomy
PLUS median lymph mode dissection if lat nodes+ then modified neck dissection |
|
|
|
endo thyroid CA
anaplastic CA what does it arise from often ? |
areise from follicular CA
Very poor Iodine uptake dx FNA Rx: small tumors total thyoidectomy +/- ext beam xray lg tumors debulking sx and trach |
|
|
|
endo thyroid CA
what if comprimise blood to parathyroids during sx ? |
can move parathroids to autograft into sternocleaido mastoid m or forearm
also post op in all thyroid sx check Ca levels. |
|
|
|
endo thyroid CA
post -op thyroid sx pat has dyspnea ? |
hematoma
bilat cut recurrnet laryngeal nerve |
|
|
|
endo pth
number pts with 3 pth glands ? 5 ? embryo sup and inf pth glands ? blood ? |
10% pts have 3 PTH glands
5% have 5 and often by thynus sup PTH glands from 4th phar pouch inf pth gland from 3rd pouch (careful, couner intuituve) blood ? inferior thyroid Art and 80% ppl have this Art only give blood to all 4 pth glands |
|
|
|
endo pth
role of pth |
INCREASE serum Ca
..bone breakdown, gi absorb, resorb renal, decrease serum phosphate ....renal exrete |
|
|
|
endo pth
how image pth glands |
sestamibi scan
|
|
|
|
endo adrenal
after a bilat adrenal ectomy in 60's pt now has pigemented skin maybe visual disturbances amenorhea |
Nelsons syndrome
due to excess ACTH and MSH Can treat with pituatary ablation surgically trans-sphenoidal |
|
|
|
gi rectal
what is a stercoral ulcer ? |
fecal impaction leading to perf and ulcer -> sepsis and req emergent laparoromy
|
|
|
|
gi
stomach treatment of post vagotomy diarrhea |
cholestyrameine as it is partly due to unabsorbed bile salts
if that fails consider sx reversal part of sm int to prolong transit time and inc absorbtive capacity |
|
|
|
gi rectal
incontinence work up |
anal manometry : pressures of sph
endoanal u/s : more acureate vs manometry, detects occultlesions pelvis floor EM<G to tell anat vs neurogenic probs like childbirth pudendal N injury and to predit likley success of sx repair a pudendeal nerve terminal motpr latency |
|
|
|
gi CA
sequence genes colorectal CA |
APC loss or mutation
loss DNA methylation Ras mutation loss DCC Gene loss of p53 |
|
|
|
gi syndrome
pt gi polyps alopecia nail dystrophy hyperpigmentation |
cronkite-canada
minimal malig potential |
|
|
|
gi CA syndromes
peutz jeugers get what cancers |
panc
breast lung ovasry uterus |
|
|
|
CA gi syndrome
lynch I vs II |
Lynch I
mult polyps, R side colon cancer Lynch II same as I but also extra-colion CA like uterus, ovary, cervex, breast |
|
|
|
desc blood to spleen
|
vein: splenic vein joins SMA to portal vein
Art: splenic off celiac tr some by sht gastric which are off and L gastroepiploic |
|
|
|
spleen
splenolegaly vs hypersplenism |
splenomegaly = physically big spleen, see in 2% nml people as when can feel it. Nml function
hypersplenism = one kind of splenomegaly where big AND increased FUNCTION #1 cause = portal HTN ; - primary, rare, females, idio, DOExcl - seconday: hemolysis, ITP, TTP, neoplasm/MDS, inflamm states, seconday includes congestive splenomegaly : portal HTN, cirrhosis (60% get splenomegaly, 15% hypersplenism) , splenic vein thrombosis, CHF, infection, |
|
|
|
spleen
young woman bleeding mennorrhagia easy bruise mucosal bleeding petechia |
ITP
Rx 1st steroids , inc PLTs in 3-7 days. Sx when steroids fails (yrs) and TCP recurs. |
|
|
|
spleen
arthritis eye issues smear Howell jowell bodies pappelheimers (iron) acanthrocytes heinz bodies Dz? Rx? |
hyposplenism
sickle IBS collagen vasc AI dxz Rx? prophy encapsuled bugs Note: this is a FUNCTIONAL hyposplenism and spleen can be physically lg, sm, normal. |
|
|
|
25 year old male
cyclic fever wt loss sup vena cava syndrome |
hodkins lymphoma
Reed sternberg cells stage: clinical vs laparoscopy spleen can be primary site. starts localized and regional. lap staging : liver, splenectomy(2), LN samples (3), iliac crest (4) For 2 consider radiation alone otherwise chemorad. |
|
|
|
spleen
systemic s/s at dx men SVC |
non hodkins
chemo limited role of splenectomy |
|
|
|
spleen
man over 50 abd full due to big spleen brusing as low plts infections low wbc wt loss, weak, LITTLE LYMPHADENOPATHY |
HAIRY CELL
LITTLE LYMPHADENOPATHY unlike CLL cells in red pulp of spleen. Def Dx by BM bx RX: alpha interferon w/ 80% response rate splenectomy for symptoms from abd fulness from it, canimprove cell counts and dec risk of hemmorage |
|
|
|
spleen
man 60's big LN big spleen due to AI hemo anemia hepatomegaly smear: leukocytosis immature leuks |
CLL
chemorad remove spleen : just helps symptoms not prolong life |
|
|
|
BIG spleen common finding
BM has ++ cells smear myelos and fibros alk phos low in bad cells |
CML
phili chromo Rx chemo and for some w./ symptoms can remove spleen which helps symptoms but not lifespan |
|
|
|
spleen
tumors |
most common non lymphoid
hemangioma : risk rupture, plt seq, dx and rx splectomy haram,toma : incidental, can be cysticsolid, clin insig, need splenectomy to dx Lymphanioma as with liver angioma and those in body , removing spleen dx and rx |
|
|
|
spleen
mucosal bleeding guicac pos stool TTP on CBC |
ITP DOExcl
rx steroids, or IvIG if severe can remove spleen to prevent recur |
|
|
|
spleen
one unit plts inc plt count how much ? |
10,000
|
|
|
|
etiology TTP
|
hemo anemia from abn VWF multimers in vesssels
RF: infection like HIV , OI57, CA, AI, pregnancy, |
|
|
|
scenario : HIV man 27, fever, changing mental status, hematuria or rising BUN
CBC : pancytopenia or low rbc |
TTP
hemo anemia from abn VWF multimers in vesssels |
|
|
|
spleen
rx TTP |
never give plts
plasma pheresis daily untli plt count nml or give FFP if no pheresis possible can give RBCS if symp from anemia treat cranail bleeds |
|
|
|
spleen
Pt [ infection, hematoma, IVDA) fever chills LUQ tender and guarding +/- palp spleen U/S lg spllen with areas of lucency CT: area of lower attenuation |
Rx
usually splenectomy or if lg solitary juztracapsular abscess try percut drainage |
|
|
|
spleen
function ? |
stores 33% plts
filters RBCS makes opsonins : tuftsins, properdin makes IgM site phagocytosis ** does NOT stores RBCs in humans |
|
|
|
spleen
pt had motorcycle acc 2 weeks later presents shock and abd pain s/sx hemoperitoneum Kehrs sign LUQ pain Test to Diag ? |
delayed splenic rupture
from subcap hematoma or psueudo anuer Diag splenic rupture : stable pts -> CT unstable --> u/s or DPL |
|
|
|
spleen
treat splenic rupture ? |
Non OR :
stable pt isolated spleen injury no hilar involvement not complete rupture UNSTABLE pt DPL/FAST and then laporatomy with removal of sleeen ( splenorrhaphy) or splenectomy. Select pts embolization. |
|
|
|
Eponym sign for what ?
1. Localisation of trauma in the upper abdomen. 2. Demonstration of internal bleeding. 3. Spread, localized and fixated dullness in the left flank also when changing position. |
Ballance's sign
Associated persons: Sir Charles Alfred Ballance Description: A trias of clinical signs of rupture of the spleen in abdominal trauma: 1. Localisation of trauma in the upper abdomen. 2. Demonstration of internal bleeding. 3. *** LUQ DULLNESS TO PERCUSSION Spread, localized and fixated dullness in the left flank also when changing position. |
|
|
|
spleen
what is splennoraphy ? |
means a spleen salvage op:
wrap with vicrl mesh topical hemostasis agents partial splectomy |
|
|
|
post splen comps
|
thromboCYTOSIS
subpherenic abscess atelectaisis pancreattitis gastric dilation OPPS : --adults under 1% --vs kids 1-2% with 50% mortality |
|
|
|
spleen
post splennectomy pts presents fever lethargy cold and URI |
Can be OPPS
and mortality of 50% #1 bug S pna Neis men, H flu PRophy: IMMEDIATE PENNY for all minor infections and illness and medical carefor major illness and fever |
|
|
|
spleen
when vax pts for splenectomy |
preop best
or 2 weeks post op |
|
|
|
spleen
changes in labs postp spleeen ectomy |
WBC inc 50% over BL
MARKED THROMBOCYTOSIS RBC smear abn : pappen, Howell, Heniz |
|
|
|
ACLS
After shock ? If pulse ? |
CPR after shock
If pulse -> check BP |
|
|
|
ACLS
No pulse / cardiac arrest (Even if see ECG tracing) |
CPR until AED
|
|
|
|
ACLS
asystole |
ECG gain/senstivity up, leads ok
epi, no shock atropine 1 mg leapfrog with epi |
|
|
|
ACLS
V fib and V tach |
shock shock epi
amiodarone 300 mg then 150 mg OR lidocaine 1 mg/kg then 1/2 @ 5-10 minute interals |
|
|
|
ACLS
PEA |
epi , no shock
atropine 1 mg if brady rhythm |
|
|

ob neonate
new baby has fingers like this. likly diag ? |
Tri 18
Edwards characteristically clenched overlapping fingers seen in the image are highly specific for trisomy 18 (Edwards syndrome). Microcephaly, microphthalmia, malformed ears, micrognathia or retrognathia, microstomia, and other congenital malformations are also associated with this disorder. |
|