Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
154 Cards in this Set
- Front
- Back
|
A patient comes in with chest pain…Best 1st test =
|
EKG
|
|
|
A patient comes in with chest pain…If 2mm ST elevation or new LBBB (wide, flat QRS), that means
|
STEMI
|
|
|
If STEMI, when do you see ST elevation?
|
Immediately
|
|
|
If STEMI, how long do inverted T waves last?
|
6hrs- years
|
|
|
If STEMI, how long do inverted Q waves last?
|
Forever
|
|
|
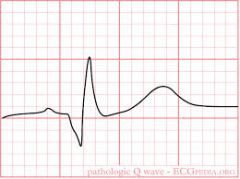
What does a pathologic Q wave look like?
|
|
|
|
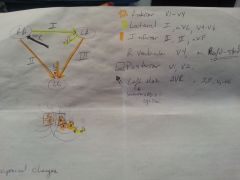
What vessel is affected and what do you see on EKG for Anterior Infarct?
|
LAD, V1-V4 |
|
|
What vessel is affected and what do you see on EKG for Lateral Infarct?
|
Circumflex, I, avL, V4-V6
|
|
|
What vessel is affected and what do you see on EKG for Inferior Infarct?
|
RCA, II, III and aVF
|
|
|
What vessel is affected and what do you see on EKG for Posterior Infarct?
|
V1, V2, Large R wave and upright T wave in V1 & V2
|
|
|
What vessel is affected and what do you see on EKG for Right Ventricular Infarct?
|
RCA, V4 on R-sided EKG is 100% specific
|
|
|
What do you see on EKG if the Left Main Coronary is occluded?
|
aVR** + usually ST DEPRESSION in I, II, V4-V6
|
|
|
Draw Picture of Leads and areas affected by blockage of specific arteries.
|
|
|
|
If patient comes in with chest pain and ST elevations, what do you do?
|
Emergency repurfusion: go to cath lab or thrombolytics if no contraindications ***check this to make sure it is right
|
|
|
If the patient has a right ventricular infarct, what symptoms might you see?
|
hypotension, tachycardia, clear lungs, JVD, and NO pulsus paradoxus
|
|
|
How do you treat Right ventricular Infarct?
|
DON’T give nitro. Tx w/ vigorous fluid resuscitation ** check this to see if there is more to this treatment
|
|
|
In a patient with chest pain, after the EKG, what is the next best test?
|
Cardiac Enzymes q8hrs x 3
|
|
|
What are the rise, peak and normalizations times of the cardiac enzymes?
|
Myoglobin Rises 1st, Peaks in 2hrs, nl by 24
CKMB Rise 4-8hrs, Peaks 24 hrs, nl by 72hs Troponin I Rise 3-5hrs, Peaks 24-48hrs, nl by 7-10days |
|
|
If someone comes in with chest pain, and MI is suspected/confirmed, how do you treat them?
|
1 - Immediately - MONA-B Morphine, Oxygen, Nitrates, Aspirin, Beta Blocker
2 - Do coronary angiography within 48 hours to determine the need for intervention. 3 - PCI is standard. 4 - Do CABG if Left Main Disease, 3 vessel disease, 2 vessel Disease + DM, >70% occlusion, pain despite maximum medical tx, or post-infarction angina |
|
|
Someone has an MI, what do you discharge them on?
|
“A BASS”
ACE Inhibitor IF CHF or LV dysfx Beta Blocker Aspirin (+ clopidogrel for 9-12 months if stent placed) Statin Short acting Nitrate or “BANAS” Beta Blocker Aspirin (+ clopidogrel for 9-12 months if stent placed) Nitrate Aspirin (+ clopidogrel for 9-12 months if stent placed) Statin |
|
|
What is the 1st test to workup for Angina?
|
Exercise EKG: Avoid Beta Blockers and CCB before
|
|
|
When can you not do an EKG stress test (other than patient’s physical condition)? What do you do intstead?
|
If the patient has an old LBBB or Baseline ST elevation or is on Digoxin.
Do Exercise ECHO instead |
|
|
What if the patient cannot physically exercise?
|
do chemical stress test w/ dobutamine or adenosine.
|
|
|
What is MUGA? What do you avoid before the test?
|
(Multi Gated Acquisition Scan) aka Radionuclide Scan. Shows perfusion of areas of the heart. Avoid caffeine or theophylline before.
|
|
|
What makes the Stress Test “Positive”. What do you do if it is positive?
|
Chest pain is reproduced, ST depression, or hypotension.
Now do Coronary Angiography |
|
|
Draw a flow diagram of the workup of Chest Pain
|
|
|
|
What is the most common cauase of Death Post-MI?
|
Arryhtmias, specifically V-Fib
|
|
|
Post-MI complications: New systolic murmur 5-7 days s/p?
|
Papillary muscle rupture
|
|
|
Post-MI complications: Acute severe hypotension?
|
Ventricular free wall rupture
|
|
|
Post-MI complications: “step up” in O2 conc from RA RV?
|
Ventricular septal rupture
|
|
|
Post-MI complications: Persistent ST elevation ~1mo later + systolic MR murmur?
|
Ventricular wall aneurysm
|
|
|
Post-MI complications: “Cannon A-waves”?
|
AV-dissociation. Either V-fib or 3rd degree heart block
|
|
|
Post-MI complications: 5-10wks later pleuritic CP, low grade temp? How do you treat it?
|
Dressler’s syndrome. (probably) autoimmune pericarditis. Tx w/ NSAIDs and aspirin.
|
|
|
A young, healthy patient comes in with chest pain…
• If worse w/ inspiration, better w/ leaning forwards, friction rub & diffuse ST elevation |
pericarditis
|
|
|
A young, healthy patient comes in with chest pain…If worse w/ palpation
|
costochondriasis
|
|
|
A young, healthy patient comes in with chest pain… If vague w/ hx of viral infxn and murmur
|
myocarditis
|
|
|
A young, healthy patient comes in with chest pain…If occurs at rest, worse at night, few CAD risk factors and migraine headaches, w/ transient ST elevation during episodes? How do you diagnose it? How do you treat it?
|
Prinzmetal’s angina
– Dx w/ ergonovine stim test. Tx w/ CCB or nitrates |
|
|
“Progressive, prolongation of
the PR interval followed by a dropped beat” |
Mobitz Type I, 2nd Degree AV Block
|
|
|
Cannon-a waves on
physical exam. “regular P-P interval and regular R-R interval” |
3rd Degree AV Block
|
|
|
“varrying PR interval with 3 or
more morphologically distinct P waves in the same lead”. Seen in an old person w/ chronic lung dz in pending respiratory failure |
Multifocal Atrial Tachycardia - d/t multiple sites of competing atrial activity
|
|
|
“Three or more consecutive beats w/ QRS <120ms @ a rate of >120bpm”
|
Atrial Tachycardia??
|
|
|
“Short PR interval followed by QRS >120ms with a slurred initial deflection
representing early ventricular activation via the bundle of Kent”. |
WPW - abnormal accessory electrical conduction pathway (bundle of kent) stimulates ventricles to contract prematurely
|
|
|
“Regular rhythm with a ventricular rate of 125-150 bpm and atrial rate
of 250-300 bpm” |
Atrial Flutter
|
|
|
“prolonged QT interval leading to
undulating rotation of the QRS complex around the EKG baseline” In a pt w/ low Mg and low K. Li or TCA OD |
Torsades de Pointe
|
|
|
“Regular rhythm w/ a
rate btwn 150-220bpm.” Sudden onset of palpitations/dizziness. |
Paraxysmal Supraventricular Tachycardia
there are three types: 1 - AV nodal Reentry 2 - Atrioventricular Reentrant Tachycardia 3 - Ectopic Atrial Tachycardia |
|
|
Renal failure patient/crush injury/burn victim w/ “peaked T-waves, widened QRS, short QT
and prolonged PR.” |
Hyperkalemia
|
|
|
“Alternate beat variation in direction, amplitude and duration of the QRS complex” in a
patient w/ pulsus paradoxus, hypotension, distant heart sounds, JVD |
Electrical Alternans - Cardiac Tamponade or severe pericardial effusion - basically d/t the heart wobbling around in the fluid
|
|
|
“undulating baseline, no p waves appreciated., irregular R-R interval in a patient with hyperthyroid or an old patient with SOB/Dizziness/Palpitations with CHF or Valve Disease
|
AFib
|
|
|
SEM cresc/decresc, louder w/
squatting, softer w/ valsalva. + parvus et tardus |
Aortic Stenosis
|
|
|
SEM louder w/ valsalva, softer
w/ squatting or handgrip. |
HOCM
|
|
|
Late systolic murmur w/ click
louder w/ valsalva and handgrip, softer w/ squatting |
Mitral Valve Prolapse
|
|
|
Holosystolic murmur radiates
to axilla w/ LAE |
Mitral regurge
|
|
|
Holosystolic murmur w/ late
diastolic rumble in kiddos |
VSD
|
|
|
Continuous machine like
murmur |
PDA
|
|
|
Wide fixed and split S2-
|
ASD
|
|
|
Rumbling diastolic murmur
with an opening snap, LAE and A-fib |
Mitral Stenosis
|
|
|
Blowing diastolic murmur with
widened pulse pressure and eponym parade. |
Aortic Regurge
|
|
|
A patient comes in with shortness of
breath… • If you suspect PE (history of cancer, surgery or lots of butt sitting) what do you do? |
Heparin!!!
|
|
|
A patient comes in with shortness of
breath… Give O2 if |
O2 sats < 90
|
|
|
A patient comes in with shortness of
breath… If signs/sxs of pneumonia ? |
Get Chest XRay
|
|
|
A patient comes in with shortness of
breath… If murmur present or history of CHF get what test? |
echo to check
ejection fraction |
|
|
A patient comes in with shortness of
breath… For acute pulmonary edema give what? |
nitrates, lasix and
morphine |
|
|
A patient comes in with shortness of
breath… If young w/ sxs of CHF w/ prior hx of viral infx consider? |
myocarditis (Coxsackie B).
|
|
|
A patient comes in with shortness of
breath… If pt is young and no cardiomegaly on CXR consider? |
primary pHTN
|
|
|
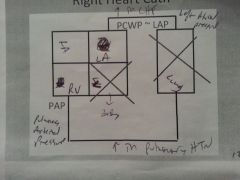
Draw the diagram of the right heart cath:
|
|
|
|
What is the EF in Systolic CHF?
What is the condition of the heart muscle? What are the causes? Which of the causes is reversible? |
Systolic- decreased EF (<55%)
– Ischemic, dilated • Viral, ETOH, cocaine, Chagas, Idiopathic • Alcoholic dilated cardiomyopathy is reversible if you stop the booze. |
|
|
What is the EF in Diastolic CHF?
What is the condition of the heart muscle? What are the causes? Which of the causes is reversible? |
• Diastolic- normal EF, heart can’t fill
– HTN, amyloidosis, hemachromatosis • Hemachromatosis restrictive cardiomyopathy is reversible w/ phlebotomy. |
|
|
How do you treat CHF and which ones improve survival?
|
ASDF B or SAD Boy Friend
ACE-I: Improves survival by preventing remodeling of the heart by aldosterone Spironolactone: Improves survival in NYHA class III and IV Digoxin: Decreases Sx and hospitalizations NOT survival Furosemide: Improves Sx (SOB, Crackles, Edema B-Blocker: (metoprolol, carvedilol) Improves Survival by Preventing remodeling by epi/norepi |
|
|
Pulmonology NEXT
|
next
|
|
|
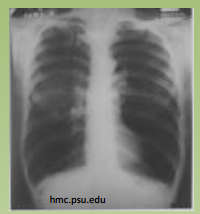
“Opacification, consolidation,
air bronchograms” |
Pneumonia
|
|
|
What does air bronchograms mean
|
air filled bronchi are made visible by opacification of surrounding alveoli that are filled with something other than air
|
|
|
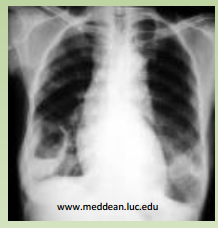
“hyperlucent lung fields
with flattened diaphragms” |

COPD
|
|
|
“hyperlucent lung fields
with flattened diaphragms” |
COPD
|
|
|
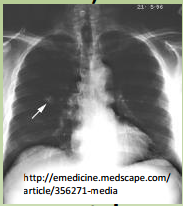
“heart > 50% AP
diameter, cephalization, Kerly B lines & interstitial edema” |
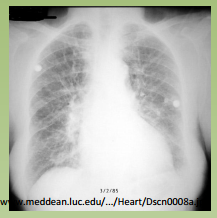
CHF
|
|
|
What are Kerly B lines?
|
Thin, linear opacities caused by fibrosis or hemosiderin deposition that is caused by recurrent pulmonary edema
|
|
|
What does cephalization mean?
|
recruitment of upper lung vessels to carry blood
|
|
|
Cavity containing fluid air level
|
abcess
|
|
|
“Upper lobe cavitation, consolidation
+/- hilar adenopathy” |
TB
|
|
|
For a pleural effusion...
how much fluid do you have to see? On what type of image? And what do you do next? |
>1cm of fluid on
Lateral decubitus X-ray Do a thoracentesis |
|
|
If pleural effusino is transudative, what is the likely etiology?
|
CHF, Nephrotic, Cirrhotic
|
|
|
If pleural effusion is low in glucose what is the likely etiology?
|
Rheumatoid arthritis
|
|
|
If the pleural fluid is high in lymphocytes what is the likely etiology?
|
TB
|
|
|
If the pleural effusion is bloody what is the likely etiology?
|
Malignancy or PE
|
|
|
If the pleural effusion is exudative, what is the likely etiology?
|
Parapneumonic (complicated/uncomplicated/empyema), cancer, etc.
|
|
|
What is a complicated parapneumonic exudate?
What do you do for it? |
+ gram stain or culture, pH<7.2, and glucose <60
Insert chest tube for drainage |
|
|
What is Light's Criteria?
|
Pleural effusion is transudative if:
LDH<200 LDH Effusion/Serum <0.6 Protein Effusion/Serum <0.5 |
|
|
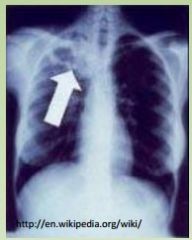
on CXR:
Thickened peritracheal stripe and splayed carina bifurcation |
- Left atrial enlargement
- Mediastinal lymphadenopathy (cancer) ??? |
|
|
Sx of PE
|
pleuritic chest pain, hemoptysis, tachypnea
Decr pO2, tachycardia. |
|
|
Random signs of PE
|

right heart strain on EKG, sinus tach,
decr vascular markings on CXR, wedge infarct, ABG w/ low CO2 and O2. |
|
|
What does right heart strain look like?
|
ST depression and T wave inversion in V1-V3 and inferior lead (II, especially III, aVL)
|
|
|
If PE is suspected, do what ist?
Then do what? Then what? |
give heparin 1st!
Then work up w/ V/Q scan, then spiral CT. Pulmonary angiography is gold standard. |
|
|
How do you treat confirmed PE?
|
--Tx w/ heparin warfarin overlap.
--Use thrombolytics if severe but NOT if s/p surgery or hemorrhagic stroke. --Surgical thrombectomy if life threatening. --IVC filter if contraindications to chronic coagulation. |
|
|
What is the Pathophysiology of ARDS?
|
inflammation --> impaired
gas xchange, inflam mediator release, hypoxemia |
|
|
What causes ARDS?
|
Sepsis, gastric aspiration, trauma, low perfusion,
pancreatitis. |
|
|
How do you diagnose ARDS?
|
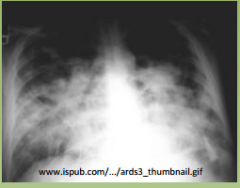
1.) PaO2/FiO2 < 200 (<300 means acute lung injury)
2.) Bilateral alveolar infiltrates on CXR 3.) PCWP is <18 (means pulmonary edema is non cardiogenic) |
|
|
How do you treat ARDS?
|
mechanical ventilation w/ PEEP (according to ARDS.net protocol)
|
|
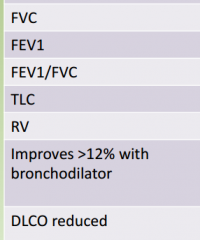
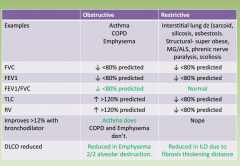
What happens to the following values in obstructive vs Restrictive lung disease?
|
|
|
|
What is DLCO?
|
It is decreased in any condition that affects the effective alveolar surface area
|
|
|
COPD
Criteria for diagnosis? |
Productive cough >3mo for >2 consecutive yrs
|
|
|
COPD
Treatment? |
|
|
|
COPD
• Indications to start O2? |
PaO2 <55 or SpO2<88%. If cor pulmonale, <59
|
|
|
COPD
Criteria for exacerbation? |
Change in sputum, increasing dyspnea
|
|
|
COPD
Treatment for exacerbation? |
O2 to 90%, albuterol/ipratropium nebs, PO or IV
corticosteroids, FQ or macrolide ABX, |
|
|
COPD
Best prognostic indicator? |
FEV1
|
|
|
Shown to improve
mortality? |
1.) Quitting smoking (can decr rate of FEV1 decline
2.) Continuous O2 therapy >18hrs/day |
|
|
Why is our goal for SpO2
94-95% instead of 100%? |
COPDers are chronic CO2 retainers. Hypoxia is
the only drive for respiration. |
|
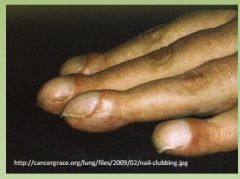
Your COPD patient comes with a 6
week history of clubbing. What is the other name for it? What is likely causing it? |
Hypertrophic Osteoarthropathy
Lung Malignancy |
|
|
Describe the stages of asthma and their treatments
|
Mild Intermittent: If pt has sxs twice a week and PFTs are normal
Albuterol only Mild Persistent: If pt has sxs 4x a week, night cough 2x a month and PFTs are normal Albuterol + Inhaled steroids Moderate Persistent: If pt has sxs daily, night cough 2x a week and FEV1 is 60-80%? Albuterol + Inhaled Steroids + long acting beta ag (salmeterol) Severe Persistent: If pt has sxs daily, night cough 4x a week and FEV1 is <60%? Albuterol + inhaled CS + Salmeterol + montelukast (if obes/smoker/ASA sensitive) + Oral Steroids |
|
|
How to treat an asthma exacerbation
|
tx w/ inhaled albuterol and PO/IV
steroids. Watch peak flow rates and blood gas. PCO2 should be low. Normalizing PCO2 means impending respiratory failure --> INTUBATE. |
|
|
What is a weird complication of asthma
|
Allergic Brochopulmonary Aspergillus
|
|
|
1cm nodues in upper lobes w/
eggshell calcifications. |
Silicosis. Get yearly TB test!.
Give INH for 9mo if >10mm |
|
|
Reticulonodular process in
lower lobes w/ pleural plaques. |
Asbestosis. Most common cancer is
broncogenic carcinoma, but incr risk for mesothelioma |
|
|
Patchy lower lobe infiltrates,
thermophilic actinomyces. |
Hypersensitivity Pneumonitis =
“farmer’s lung” |
|
|
Hilar lymphadenopathy, ↑ACE
erythema nodosum. – Hypercalcemia? – Important referral? – Dx/Treatment? |
Sarcoidosis.
hypercalc: 2/2 ↑ macrophages making vitD referral: Ophthalmology uveitis conjunctivitis in 25% Dx by biopsy. Tx w/ steroids |
|
|
So you found a pulmonary nodule…
1st step |
look for an old CXR to compare!
|
|
|
Characteristics of benign pulmonary nodules:
How to treat? |
- Popcorn calcification = hamartoma (most common)
– Concentric calcification = old granuloma – Pt < 40, <3cm, well circumscribed • Tx w/ CXR or CT scans q2mo to look for growth |
|
|
Characteristics of malignant nodules:
What to do next? |

– If pt has risk factors (smoker, old), If >3cm, if eccentric
calcification • Do open lung bx and remove the nodule |
|
|
A patient presents with weight loss, cough,
dyspnea, hemoptysis, repeated pnia or lung collapse. MC cancer in non-smokers? |
Adenocarcinoma. Occurs in scars of old pnia
|
|
|
Location and mets of adenocarcinoma
|
Peripheral cancer. Mets to liver, bone, brain and adrenals
|
|
|
Characteristics of effusion of lung adenocarcinoma
|
Exudative with high hyaluronidase
|
|
|
Patient with kidney stones,
constipation and malaise low PTH + central lung mass? What cancer? What are important lab values? |
Squamous cell carcinoma.
Paraneoplastic syndrome 2/2 secretion of PTH-rP. Low PO4, High Ca |
|
|
Patient with shoulder pain, ptosis,
constricted pupil, and facial edema? |
Superior Sulcus Syndrome from Small
cell carcinoma. Also a central cancer. |
|
|
Patient with ptosis better after 1
minute of upward gaze? |
Lambert Eaton Syndrome from small
cell carcinoma. Ab to pre-syn Ca chan |
|
|
Old smoker presenting w/ Na = 125,
moist mucus membranes, no JVD? |
SIADH from small cell carcinoma.
Produces Euvolemic hyponatremia. Fluid restrict +/- 3% saline in <112 |
|
|
CXR showing peripheral cavitation and
CT showing distant mets? |
Large Cell Carcinoma
|
|
|
IBD
Involves terminal ileum? What does it mimic? What deficiency can it cause? |
Crohn’s. Mimics appendicitis. Fe deficiency.
|
|
|
IBD
Continuous involving rectum? |
UC. Rarely ileal backwash but never higher
|
|
|
IBD
Incr risk for Primary Sclerosing Cholangitis? |
UC. PSC leads to higher risk of cholangioCA
|
|
|
IBD
|
Fistulae likely?
|
|
|
IBD
Granulomas on biopsy? |
Crohn’s.
|
|
|
IBD
Transmural inflammation? |
Crohn’s.
|
|
|
IBD
Cured by colectomy? |
UC.
|
|
|
IBD
Smokers have lower risk? |
UC. Smokers have higher risk for Crohn’s.
|
|
|
IBD
Highest risk of colon cancer? |
UC. Another reason for colectomy.
|
|
|
IBD
Associated w/ p-ANCA? |
UC.
|
|
|
IBD
treatment? |
Treatment = ASA, sulfasalzine to maintain remission. Corticosteroids to induce
remission. For CD, give metranidazole for ANY ulcer or abscess. Azathioprine, 6MP and methotrexate for severe dz. |
|

IBD Complication
|
Toxic Megacolon in Crohn's
|
|
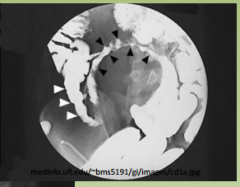
IBD
|
String Sign in Crohn's
|
|

IBD Complication
|
Pyoderma Gangrenosum
UC |
|

IBD Complication
|
Erythema Nodosum
|
|
|
AST>ALT (2x) + high GGT
|
Alcoholic Hepatitis
|
|
|
ALT>AST & in the 1000s
|
Viral Hepatitis
|
|
|
AST and ALT in the 1000s after
surgery or hemorrhage |
Ischemic Hepatitis (“shock liver”)
|
|
|
Elevated D-bili
|
Obstructive (stone/cancer) or Dubin’s Johnsons, Rotor
|
|
|
Elevated I-bili
|
Hemolysis or Gilbert’s, Crigler Najjar
|
|
|
Elevated alk phos and GGT
|
Bile duct obstruction, if IBD --> PSC
|
|
|
Elevated alk phos, normal
GGT, normal Ca |
Paget’s disease (incr hat size, hearing loss,
HA. Tx w/ bisphosphonates. |
|
|
Antimitochondrial Ab
|
Primary Biliary Cirrhosis – tx w/ bile resins
|
|
|
ANA + antismooth muscle Ab
|
Autoimmune Hepatitis – tx w/ ‘roids
|
|
|
High Fe, low ferritin, low Fe
binding capacity |
High Fe, low ferritin, low Fe
binding capacity |
|
|
Low ceruloplasmin, high
urinary Cu |
Wilson’s- hepatitis, psychiatric sxs
(BG), corneal deposits |
|
|
What is Dubin Johnson?
|
Auto-recessive - increased direct bilirubin, normal AST and ALT, Asymptomatic, Black Liver, Normal Corproporphyrin in Urine
|
|
|
What is Rotor Syndrome?
|
Same as Dubin but no black liver, and Increased Corproporphyrin in Urine
|
|
|
What is Gilbert's
|
Genetic deficiency of glucuronyl transferase. usually asymptomatic, but can jaundice when sick or stressed
|