Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
140 Cards in this Set
- Front
- Back
|
What is the most common cause of SCI?
|
-Traumatic
-MVA |
|
|
A partial or complete paralysis of all four extremities, trunk, and pelvic organs resulting from lesions of the cervical cord is known as _____________ and results from an injury to the ____________?
|
-Tetraplegia (Quadriplegia)
-C-Spine |
|
|
T or F:
Nearly all patients are released to a home setting? |
TRUE: 88%
|
|
|
In general: the most common site for injuries is where?
|
-Junctions between Levels:
|
|
|
Secondary SCI include? (4)
|
-Crush
-Hemorrhage -Edema -Infarction |
|
|
T or F:
Glutamate and Glycine are good and assist with healing following initial SCI? |
FALSE:
***Sets off cascade of biochemical and cellular events -Nerve cell death -Demeylination of axons -Triggers inflammation response |
|
|
What accounts for improvement in function in Humans since regeneration does not occur?
|
-Neuroplasticity
|
|
|
What is one of the first and most important signs to determine if spinal shock is resolving?
|
Sacral reflexes:
-Bulbocavernosus Relfex -Anal "wink" reflex |
|
|
Initial clinical symptoms of SCI include? (3-4)
|
-Loss of movement or sensation
-chest wall weakness -Spinous process deformity -Inadequate ventilation |
|
|
This is the standard drug given following SCI to improve outcome.
|
-Methylprednisolone (MP)
|
|
|
T or F:
Initial/Immediate surgery can be controversial? |
TRUE:
- Some believe the injury needs to run its course before initial surgery |
|
|
Although they are not commonly used anymore, how long is a HALO device worn?
|
-approx 12 wks
|
|
|
KEGEL QUESTION:
-What challenges with mobility will patients with orthoses have? |
-Cervical orthoses limit ability to see the ground
-TLSO – can’t flex waist past 90° -“top heavy” -Rolling, supine to sit, lower body dressing, transfers |
|
|
What are some of the common Autonomic dysfunction symptoms?
|
-Cardiovascular System
-Temperature control -Respiratory System -Bowel and Bladder -Sexual |
|
|
Signs of Hypothermia?
|
-Irritability
-Mental confusion -hallucinations -lethargy -clumsiness -slow respiration -slowing of heartbeat |
|
|
About what level do we begin to think about problems with thermoregulation?
|
-Level T6
|
|
|
People with complete spinal cord lesions above what level cannot breathe independently?
|
C4
|
|
|
What is the little rhyme to remember level of assistance?
|
C3-4-5, Keep the guy alive
|
|
|
What nerve innervates the diaphragm?
|
Phrenic Nerve; C3-5
|
|
|
Excessive sympathetic nervous system activity, elicited by noxious stimuli below the lesion is known as?
|
-Excessive sympathetic nervous system activity, elicited by noxious stimuli below the lesion
|
|
|
Autonomic Dysreflexia is seen in patients with a level of _______ and above?
|
-T6
|
|
|
What will the patient with Autonomic Dysreflexia report?
|
-Patient reports pounding HA
-Become very anxious -Flushing of the skin and profuse sweating above level of lesion -Goosebumps below level of lesion -Tell you they really don’t feel good!! |
|
|
What vital changes are seen with Autonomic Dysreflexia?
|
-Abrupt increase in BP
-Decrease in HR -APPEARS FLUSH |
|
|
T or F:
Autonomic Dysreflexia is not a medical emergency? |
FALSE
|
|
|
What do you do if a patient has Autonomic Dysreflexia?
|
-SIT THEM UP!!!
-Remove noxious stimuli -Keep checking vitals |
|
|
WHAT IS THIS?
Extreme fall in BP and decrease in HR on assuming an upright position due to loss of sympathetic vasoconstriction and muscle pumping action for blood return. |
-Orthostatic Hypotension
|
|
|
How do you treat Orthostatic Hypotension?
|
-If patient faints recline and elevate legs
**This will encourage venous return to the heart -Ace wraps, abdominal binders, TED hose: designed to improve venous return |
|
|
___________ ______________ occurs in a large number of SCI due to LE paralysis and blood vessel damage.
|
-Pulmonary Embolism
DVT |
|
|
UMN signs are more severe with _____________ SCI?
|
-Incomplete
|
|
|
KEGEL QUESTION:
-What critical interventions should be implemented in the acute phase of rehabilitation to prevent development of pressure sores? |
-Positioning, turning schedule and nutrition are critical.
|
|
|
What are the benefits to Boots and special air mattresses?
|
-May help to prevent pressure sores, more specifically in the acute stages.
|
|
|
Sudden loss of ROM, swelling, local heat, erythema and nonseptic fever are common signs of what?
|
-Heterotopic Ossification
|
|
|
What can be done to help decrease the likelihood of Renal Calculi
|
-Vigorous hydration, early mobility, especially dynamic WB activities.
-TILT TABLE |
|
|
This type of pain is commonly seen below the level of the lesion and involves electric burning pain in dermatomes?
|
-Neutopathic Pain
|
|
|
______________: pain evoked by a non-noxious stimulus, such as light touch, that does not normally evoke pain.
|
-Allodynia
-ALLodynia, ALL touch hurts |
|
|
What is one technique to help control or overcome allodynia?
|
-desensitization techniques
|
|
|
Anticonvulsants and Tricyclic Antidepressants are commonly used to treat what type of pain?
|
-Neuropathic Pain
|
|
|
What are some common psychosocial problems that individuals with SCI may face?
|
-Depression, suicidal thoughts
-Financial issues -Relationship changes |
|
|
_______________: sulcal arteries arising from ASA supply central portion of SC.
a) Centrifugal system b) Centripetal system |
A)
Centripetal supplies dorsal horns and columns and peripheral WM |
|
|
What is the main blood supply to the inferior spinal cord and has variable origins from the level of T9 to L3?
|
-Artery of Adamkiewicz
|
|
|
Which type of tract lesion/injury results in sensory loss in a dermatomal distribution?
|
-Segmental Signs
|
|
|
Vertical tract signs result in what types of deficits?
|
-Sensation loss below lesion level
-Muscle paresis with hyperreflexia -autonomic losses: of BP, pelvic viscera, thermoregulation. |
|
|
Brown-Sequard results from what?
Describe injury |
|
|
|
KEGEL: FILL IN THE BLANK
Segmental Signs:______________ Vertical Tract Signs: ___________voluntary motor control, conscious proprioception, and discriminative touch loss; ____________ pain and temperature loss (~2 segments below lesion). |
-IPSILATERAL
-IPSILATERAL -CONTRALATERAL |
|
|
What is a common MOI for an anterior cord syndrome?
|
-HYPER FLEXION INJURY
|
|
|
KEGEL: FILL IN THE BLANKS
Caused by trauma to:__________ and/or___________ Decreased_______________________ sensation below the lesion. Paralysis Intact____________________________ |
-to anterior cord or anterior spinal artery
-pain and temp sensation below lesion level -light touch and proprioception |
|
|
Central Cord Syndrome occur with _______________ injury in a person with _______________ ______________
|
-Hyperextension
-Spinal Stenosis |
|
|
KEGEL: FILL IN THE BLANKS
Damage to _______ part of spinal cord, usually at _______levels. Greater motor impairment in the _____ than in the _____ extremities (CST fibers). ___________ pain and temperature loss in a ____ distribution at level of lesion (crossing ST fibers). |

-Central
-Cervical -Upper than in the Lower -Bilateral -Cape Distribution |
|
|
Posterior Cord Suyndrome results from what types of conditions?
|
-Posterior Artery occlusion
-Tumor -Disc compression |
|
|
KEGEL FILL IN THE BLANKS:
Damage to ____________ Sensory Loss:_________________ Preservation of:________________________________________ Wide-based step gait |

-DORSAL COLUMN
- Descriminative touch and proprioception -Pain and Temp sensory function and motor function |
|
|
Cauda Equina Syndrome experience motor and sensory loss where?
|
-BUTT HOLE
|
|
|
KEGEL FILL IN THE BLANKS
Injury________damaging lumbar and/or sacral ___________ (LMNs). Sensory impairment and flaccid paralysis of________________________________________ |
-L1 or below
-Nerve roots (LMNs) -leg muscles, bladder, bowels and sexual function. |
|
|
What are two differences between the signs present with Cauda Equina and Conus Medullaris?
|
-Conus Medullaris may have spasticity of distal LE
-May have Babinski Sign |
|
|
What is often the first sign that a lesion is incomplete?
|
-SACRAL SPARING
butt hole wink ;) |
|
|
T or F:
Designation of a spinal lesion is determined by Neurological level alone? |
FALSE:
-2 criteria: The neurological level of injury Whether injury is complete or incomplete |
|
|
What is needed to classify a muscle as "normal"?
|
-“Normal” refers to muscle grade of 3/5 or above
|
|
|
T or F:
Neurological level of injury is the most caudal segment with normal SENSORY and MOTOR function bilaterally? |
-FALSE
normal sensory AND / OR motor function on both sides of the body. |
|
|
To be a complete lesion, at what level must there be no motor or sensory function?
|
S4 & S5
BUTT WINKER TEST |
|
|
What is the term for a patient who has a C7 lesion, but has some sensation in the thoracic spine?
|
-Zone of Partial Preservation
|
|
|
KEGEL EXAMPLE:
M LT PP C5 5 2 2 C6 3 2 1 C7 2 1 1 C8 0 0 0 T1 0 0 0 T2-L1 0 0 0 L2 0 0 0 L3 0 0 0 L4 0 0 0 L5 0 0 0 S1-5 0 0 0 Motor Level = ?? Sensory Level = ?? Neurological Level of Injury (NLOI) = ?? Zone of Partial Preservation = ?? ASIA classification? |
Motor Level = C6
Sensory Level = C5 Neurological Level of Injury (NLOI) = C5 Zone of Partial Preservation = C6-C7 ASIA classification = A |
|
|
What are some common conditions a patient with ASIA A might experience?
|
-Autonomic Dysreflexia
-Decreased sweating -Orthostatic Hypotension |
|
|
If a patient has normal light touch, but deminished/absent pin prick below the level of a lesion. What syndrome might you expect?
|
-ANTERIOR CORD
|
|
|
What are some factors that could increase or decrease the Prognosis of SCI?
|
-Age
-Level of lesion -Ventilator use |
|
|
T or F:
Central cord and Brown-Sequard have a better prognosis that Anterior cord? |
TRUE
|
|
|
What are two factors that increase likelihood of ambulation?
|
-touch and pinprick intact below lesion level
->3/5 quad strength 2 months post injury |
|
|
After a SCI, Explain how sensory input is INTACT below the level?
|
-THINK REFLEXES
-The sensory information is still going from the limb to the SC, but is unable to go all the way back to the brain. -Reflexes can still be used below lesion level |
|
|
T or F:
A person with a C6 complete injury can send a signal from the brain telling the leg to move? |
TRUE:
They can send the signal, but it will not work because the SC lesion will block transmission. |
|
|
T or F:
A person with a SCI cannot trigger reflexes below the level of the lesion? |
FALSE:
They can be triggered and in many instances they will be heightened due to the lack of other input to inhibit or block them. (hyperreflexia) |
|
|
List the muscle with the lesion level:
Biceps: Wrist Extensors: Diaphragm: Finger Flexors: Triceps: Abdominals: Gastroc: Anterior Tib: Quad: |

Biceps: C5
Wrist Extensors: C6 Diaphragm: C345 Finger Flexors: C8 Triceps: C7 Abdominals: T5-12 Gastroc: S1 Anterior Tib: L4 Quad: L23 |
|
|
What would the Neuro level be for a patient with Sensory T3 and lowest motor tested is C8?
|
T3 would be the Neuro level because you can not test the motor of the thoracic levels.
|
|
|
What areas of the body would you use to test proprioception?
|
-Index finger
-Big Toe |
|
|
What ashworth grade would be given for No increased tone?
|
Zero
|
|
|
Give 3 S/S of a suspected DVT?
|
-Swelling
-Pitting edema -Redness -Pain |
|
|
What clinical test can be performed for a suspected DVT?
|
-Girth Measurement
|
|
|
What should be discussed from the beginning and included with notes/goals?
|
-discharge plans and destination
|
|
|
What is one part of treatment that is very important for discharge from acute care to any setting?
THEY MUST HAVE WHAT? |
-Upright Tolerance
|
|
|
What are two areas in which you want to decrease ROM with a SCI?
|
-Low back extensors
-Finger flexors |
|
|
What is the name for a grip in which the finger flexors are tight, and useful for patients?
|
-Tenodysis grip?? spelling?
|
|
|
Name three areas in which you would want to increase ROM?
|
-Hamstring
-Shld Ext -Shld ER |
|
|
In order to transfer on an uneven surface, What movements/strength is needed?
|
-Shoulder ABD and FLEX
|
|
|
Uneven transfers require shoulder _________ and must have ___________
|
-Extension
-Triceps |
|
|
How often should position changes occur?
|
-15-20 min
|
|
|
Symptoms of Autonomic dysreflexia include?
|
in order:
-increased BP -Decreased HR -Anxious -Headache -Sweating |
|
|
What is the key different symptoms for Orthostatic hypotension when compared to autonomic dysreflexia?
|
-DECREASED BP
|
|
|
symptoms of Orthostatic Hypotension include
|
-feel dizzy
-faint -blurry vision -dec. hearing |
|
|
Treatment for orthostatic hypotension and autonomic dysreflexia?
|
-ORTHO: lay down and elevate feet
AUTO:sit up and remove irritant |
|
|
How does spasticity differ in patients with SCI?
|
-It tends to radiate or travel up and down the cord causing a full body reaction to a stimulus applied to the feet.
|
|
|
Who has worse spasticity, complete or incomplete injuries?
|
Incomplete
-Those with cervical and upper thoracic lesions have worse spasticity |
|
|
What type of orthosis would most likely be needed for a T10-11 injury?
|
-Knee-Ankle-Foot Orthosis
|
|
|
What would the Neuro injury level be to require a Hip-Knee-Ankle-Foot Orthosis?
|
T1-T9
|
|
|
Based on the evidence that the CNS is plastic, and the spinal cord is capable of learning with minimal supraspinal input is the definition of what?
|
-Recovery-Based Therapy
|
|
|
What are the four principles that guide locomotor training? (4)
|
-Maximize Load
-Optimize sensory input -Optimize kinematics -Maximize recovery/Minimize compensation |
|
|
T or F:
assistive devices are very beneficial when maximizing load for locomotion? |
FALSE:
-AD can be detrimental to recovery. -AD’s do not allow trunk rotation and unweight the limbs |
|
|
How can you optimize sensory input?
|
-use appropriate hand contact and sequencing.
|
|
|
How would you Optimize appropriate kinematics?
|
-ensure hip extension
-use arm swing -trunk rotation |
|
|
T or F:
Gait deviations are compensatory? |
TRUE:
|
|
|
During which phase of gait would the therapist assist by triggering medial HS and anterior tib?
|
-At toe off and through swing phase
|
|
|
What would you trigger during initial contact and stance? (2)
|
-Quadriceps tendon
-achilies? |
|
|
A patient who has no motor or sensory below the level of lesion would be ASIA ___?
|
-A
|
|
|
What is the Key difference between ASIA C & ASIA D?
|
-ASIA C has less than 1/2 of major muscles while ASIA D has greater than 1/2
|
|
|
Does the change from ASIA levels indicate an improved potential for recovery?
|
-NO.
-Recovery does not equal AIS conversion. Remember, recovery is the return to normal function …ASIA is a classification based on changes in impairments of strength and sensation …it has nothing to do with recovery. |
|
|
Distance gains were greatest with _______________ training?
|
-OVERGROUND
|
|
|
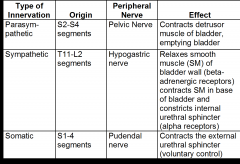
What type of innervation is used to URINATE, DEFICATE, & SEX?
|
-Parasympathetics
|
|
|
What are the two phases of normal bladder function?
|
-filling
-voiding |
|
|
Lesions of the CONUS MEDULLARIS cause ___________ bladder.
|
FLACCID
-non reflex LMN -due to flaccidity, trouble with voiding urine is noted |
|
|
Frequent and rapid voiding is caused by an UMN lesion is known as a ___________ _______________.
|
Spastic bladder / REFLEXIVE
|
|
|
What are the symptoms of HYPOreflexia/areflexia of the detrusor?
|
-Stess incontinence with laughing and coughing.
-dribbling -high residual volume |
|
|
How does a Detrusor-Sphincter dyssynergia present?
|
-Both the detrusor and external sphincter are spastic. Both contract simultaneously and little urine can come out.
|
|
|
Cystography is ??
|
radiograph with the bladder filled with a contract medium
|
|
|
What causes hydronephrosis?
|
-Obstruction of any part of the urinary tract causing kidneys to swell
|
|
|
Describe Vesicoureteral reflux?
|
Backflow of urine back into the ureters and into the kidneys
|
|
|
How does SCI affect giving birth in women?
|
-Increase risk of UTI
-High risk of Autonomic Dysreflexia -Pressure Sores -C-Section frequently required |
|
|
T or F:
The ability for men to be fertile and produce children is affected after SCI? |
TRUE:
-Higher % of dead sperm or less mobile (why??) -Increased difficulty with ejaculation |
|
|
___________ ________________ _______________ uses vibration to induce ejaculation in men with a SCI
|
Penile Vibratory Stimulation (PVS)
|
|
|
What is one common risk with both Penile vibration and rectal probes to induce ejaculation?
|
-The risk of inducing autonomic Dysreflexia
|
|
|
T or F:
Both men and women experience the same type of orgasm both pre and post SCI? |
FALSE:
-While women typically experience the same type of orgasm, men do not. -The is due to sensory loss |
|
|
What are two sexual aids for men?
|
-Viagra
-Pumps |
|
|
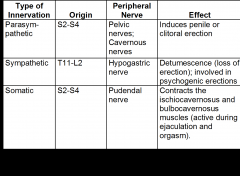
Which of the two types of erection is a result of direct stimulation to the genital area?
a) Reflexogenic erection b) Psychogenic erection |
A) Reflexogenic
-from direct stimulation of the genital area. Involves a reflex arc between the genital area and parasympathetic fibers from S2-S4 cord segments |
|
|
Penile/Clitoral erection is a result of which nervous system?
|
-Parasympathetic
-Pelvic Nerve |
|
|
The sympathetic nervous system is never good because ?
|
it causes you to lose an erection.
"whiskey dick" |
|
|
Upon arousal, Both men and women experience a __________ in HR, BP and RR?
|
-INCREASE
|
|
|
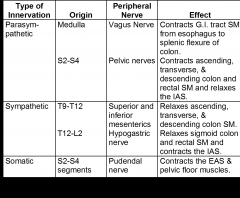
Which muscle pulls the rectum superior and forward, in essence, closing it off?
|
-Puborectalis muscle
|
|
|
What is the purpose of the Intrinsic nervous system in relationship to bowel mobility?
|
-Coordinates colonic wall movement and advancement of stool through the colon.
|
|
|
The sympathetic nervous system is "fight or flight", therefore it is responsible for ________________ the colon.
|
-RELAXING
-you cant poop when you are fighting DUH |
|
|
A diagram
|
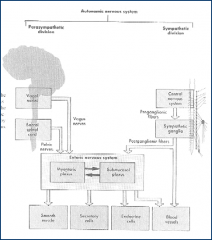
pic
|
|
|
What three things work together to keep you from pooping?
|
-Internal Anal Sphincter
-External Anal Sphincter -Puborectalis muscle |
|
|
Which sphincter can we control to prevent pooping with coughing?
|
-External anal sphincter
striated muscle continuous with pelvic floor; proximal to anus. |
|
|
If in doubt with Pee, Poop or Sex, which spinal cord segments do you guess?
|
-S2-S4
|
|
|
Internal Anal sphincter is activated but what?
|
Stretch receptors in the Anal canal
|
|
|
Damage to an UMN can result in what type of bowel?
|
-Spastic/reflexive
-There is no direct damage to the reflexes, therefore they can still be used to defecate. -Spasticity may cause constipation due to spastic external anal sphincter and pelvis floor |
|
|
A lesion directly do the ___________________ ________________ will result in a flaccid/areflexic bowel?
|
-Conus Medullaris
-may cause fecal incontinence and slowed bowel motility |
|
|
What type of pharmacological treatment may be used to increase motility? (basic)
|
-Colonic Stimulants
|
|
|
What type of pharmacological treatment may be used for a patient with spastic bowel syndrome? (basic)
|
-Stool softners
-Assistive techniques: Valsalva maneuvers, push-ups, abdominal massage, leaning forward |
|
|
A patient with a flaccid bowel syndrome may require what?
|
-Manual evacuation (disempaction) of the stool in the upright or side-lying position (every other day)
-Firm, formed stool is required to prevent fecal incontinence and to be manually evacuated easily. |
|
|
A successful bowel program follows the S.E.L.F. model?
|
S: Schedule
E: Exercise L: Liquids F: Food |
|
|
How much liquid intake is given for a successful SELF program?
|
-8-9 (8oz) glasses to prevent constipation.
|
|
|
What type of food is recommended for a patient with SCI?
|
-Foods high in fiber
|
|
|
Chart
|
|
|
|
Chart 2
|
|
|
|
Chart 3
|
|