Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
99 Cards in this Set
- Front
- Back
|
List the ossification center, ossification age, and fusion age for the ossification centers of the scapula (1 primary, 6 secondary)
|
CENTER OSSIFICATION FUSION
Body (primary) 8 wk (fetal) 15-20 yr (all) 6 Secondary: Coracoid (tip) 1 yr Coracoid 15 yr Acromion tip 15 yr Acromion 16 yr Inferior angle 16 yr Medial border 16 yr |
|
|
List the ossification center, ossification age, and fusion age for the ossification centers of the clavicle (3)
|
CENTER OSSIFIES FUSES
Primary: Medial & lateral 5 wk (fetal) 25 yr Secondary: Sternal 18 yr 25 |
|
|
What is the term for failure of union between the acromian tip and remainder of the acromion?
|
Os Acromiale
|
|
|
List the ossification center, ossification age, and fusion age for the ossification centers of the Humerus
|
CENTER OSSIFIES FUSES
Body (primary) 8 wk (fetal) Blends @ 6 yr unites _ @ 20 yr Head 1 yr Greater tuberosity 3 yr Lesser tuberosity 5 yr Capitulum 2 yr Blends unites w/ body at 16-18 Med epicondyles 5 yr Trochlea 9 yr Lat epicondyles 13 yr |
|
|
What are the 17 muscles that attach to the scapula?
|
Omohyoid, Supraspinatus, Infraspinatus, Rhomboid Major, Rhomboid Minor, Teres Major, Teres Minor, Pec Minor, Biceps, Triceps, Coracobrachialis, Latissimus, Trapezius, Deltoid, Levator scapula, subscapularis, serratus anterior
|
|
|
Is the glenoid retroverted or anteverted and to what degree?
|
Retroverted approximately 5 degrees
|
|
|
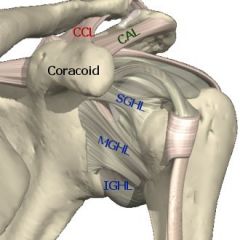
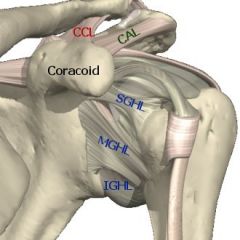
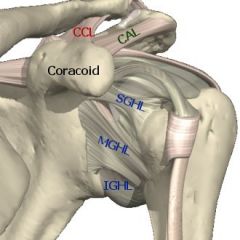
What are the 4 ligaments that attach to the scapula
|
SGHL, MGHL, IGHL
|
|
|
What 5 structures attach to the coracoid?
|
Coracoacromial ligament, coracoclavicular ligaments (conoid (medial) and trapezoid (lateral)), conjoined tendon (formed by coracobrachialis and short head of biceps), and pectoralis minor
|
|
|
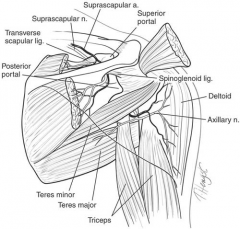
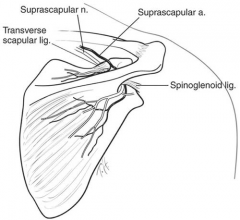
What separates the suprascapular artery from the suprascapular nerve?
|
Suprascapular notch has the superior transverse scapular ligament separating the suprascapular artery (superior) from the suprascapular nerve (inferior).
|
|
|
How might atrophy of the infraspinatus be caused at the spinoglenoid notch?
|
Usually labral disease causing compression of the suprascapular nerve at the spinoglenoid notch
At the spinoglenoid notch, the suprascapuloar artery and nerve are both inferior to the inferior transverse scapular ligament |
|
|
What is unique about the ossification and fusion of the clavicle?
|
Is the the first bone to ossify (5 weeks of gestation) and the last to fuse (at the medial epiphysis at 25 years of age)
|
|
|
What are the major and minor articulations of the shoulder?
|
One major: Glenohumeral Joint
3 minor: Sternoclavicular, acromioclavicular, scapulothoracic |
|
|
What are the 5 static restraints of the shoulder?
|
The articular anatomy, glenoid, labrum, negative pressure, capsule, and GH ligaments.
|
|
|
What are the dynamic restraints of the shoulder?
|
The rotator cuff, biceps tendon, periscapular muscles, proprioception
|
|
|
What ligaments make up the sternoclavicular joint (4)?
|
Anterior and posterior sternoclavicular ligaments, an interclavicular ligament, and a costoclavicular ligament.
|
|
|
How much does the SC joint rotate with shoulder motion?
|
30 degrees
|
|
|
What is the difference in the types of motion of the AC and SC joints?
|
SC is double-gliding with an articular disc
AC is plane/gliding with a fibrocartilaginous disc |
|
|
Is the scapulothoracic articulation a true joint? What is the ratio comparison of glenohumeral motion with scapulothoracic motion with abduction?
|
No, it is not a true joint. The ratio is 2:1 (GH:scapulothoracic)
|
|
|
What ligament is found at the spinoglenoid notch and what is the relationship of the suprascapular artery and nerve at this location?
|
The inferior transverse scapular ligament; the artery and nerve are both inferior to the ligament
|
|
|
What structure is important for superoanterior restraint in rotator cuff deficiencies?
|
The coracoacromial ligament is important for superoanterior restraint in rotator cuff deficiencies and should be preserved during débridement of painful massive rotator cuff tears that cannot be surgically repaired.
|
|
|
What is the function of the rotator cuff muscles and where do they attach?
|
The rotator cuff muscles depress and stabilize the humeral head against the glenoid; all attach to the greater tuberosity except the subscapularis, which has a lesser tuberosity insertion (shoulder internal rotator).
|
|
|
Which muscles are stronger in the shoulder, the internal rotators or the external rotators? Name these muscles.
|
The shoulder internal rotators (pectoralis major, latissimus dorsi, teres major, and subscapularis) are stronger than the external rotators (teres minor and infraspinatus), which is why posterior shoulder dislocations are more common than anterior dislocations after electrical shock and seizures.
|
|
|
Injury to what location of the brachial plexus would not produce Horner's syndrome, a winged scapula, diaphragmatic paralysis, or rhomboid paralysis
|
Postganglionic injuries
|
|
|
Injury to cranial nerve XI would cause what deformity of the shoulder? Why would cranial nerve XI injury result in shoulder depression with scapular translation laterally and cause the inferior angle to be rotated laterally?
|
Lateral winging
Unopposed pull of the serratus anterior |
|
|
Injury to the long thoracic nerve (C5-C7) would cause what shoulder deformity?
|
Medial scapular winging. Results in superior elevation with scapular translation medially and the inferior angle rotated medially
|
|
|
When does the subclavian artery become the axillary artery?
|
After the subclavian emerges between the anterior and middle scalenes, it becomes the axillary artery at the outer border of the first rib
|
|
|
The axillary artery is conceptualized as divided into three parts on the basis of its physical relationship to what?
|
The pectoralis minor muscle (the first part is medial to it, the second is under it, and the third is lateral to it).
|
|
|
What are the branches of the axillary artery?
|

Each part of the artery has as many branches as the number of that portion, i.e., 1st part has 1, 2nd part has 2, 3rd part has 3.
Part 1: Supreme Thoracic Part 2: Thoracoacromial trunk, lateral thoracic Part 3: Subscapular, anterior humeral circumflex, posterior humeral circumflex |
|
|
What part of the axillary artery is the most vulnerable to traumatic vascular injury?
|
The third part at the origin of the anterior and posterior humeral circumflex arteries
|
|
|
What is the interval for the anterior (Henry's) approach to the shoulder?
|
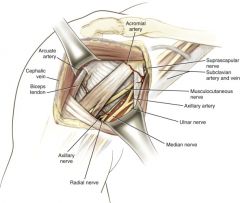
Deltoid (axillary nerve) and pec major (medial and lateral pectoral nerves)
Notes: Anterior (Henry's) surgical approach to the shoulder. In this approach, the interval between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves) is explored. To prevent injury to the musculocutaneous nerve, avoid excessive medial retraction (see medial retractor) on the coracobrachialis or avoid dissection medial to this muscle. Also avoid the axillary nerve, which is inferior to the shoulder capsule. Positioning the arm in adduction and external rotation helps displace the axillary nerve from the surgical field. |
|
|
What 2 nerves are at risk with the delto-pectoral approach to the shoulder?
|
Musculocutaneous nerve and Axillary nerve
|
|
|
Where is the Musculocutaneous nerve at risk in the anterior approach to the shoulder? How do you protect it?
|
This nerve usually penetrates the biceps/coracobrachialis 5 to 8 cm below the coracoid, but it enters these muscles proximal to this 5-cm “safe zone” in almost 30% of shoulders. Protect by avoiding vigorous retraction of the conjoined tendon and avoiding dissection medial to the coracobrachialis
|
|
|
Where is the axillary nerve at risk in the anterior approach to the shoulder? How do you protect it?
|
Just inferior to the shoulder capsule. Protected during procedures in this area with adduction and external rotation of the arm
|
|
|
What is the interval for the lateral approach to the shoulder? What is this approach used for?
|
There is no interval, this is a deltoid-splitting approach in which the deltoid is either split or subperiosteally dissected from the acromion.
This approach exposes the supraspinatus tendon so is used for cuff repair |
|
|
How far inferiorly can the deltoid be split with the lateral approach to the shoulder?
|
No more than 5cm below the acromion in order to avoid injury to the axillary nerve as it exits from the quadrangular space. If dissection is carried below here deneravation of the anterior portion of the deltoid could occur
|
|
|
What is the interval for the posterior approach to the shoulder?
|
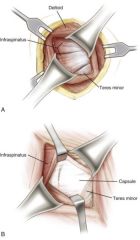
Infraspinatus (suprascapular nerve) and teres minor (axillary nerve). To access this interval the posterior deltoid must be split.
|
|
|
What structures are at risk with the posterior approach to the shoulder?
|
The axillary nerve and the posterior circumflex humeral artery run in the quadrangular space below the teres minor, so you must be sure to stay superior to this muscle
|
|
|
What defines the rotator interval?
|
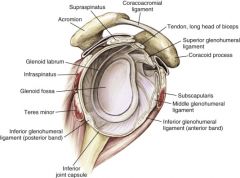
The rotator interval is between the anterior border of the supraspinatus and the superior border of the subscapularis
|
|
|
What structure is found within the rotator interval?
|
The superior glenohumeral ligament
|
|
|
What is the role of the superior glenohumeral ligament?
|
It is the primary restraint both in inferior translation of the adducted shoulder and in external rotation of the adducted or slightly abducted arm
|
|
|
What is the role of the middle glenohumeral ligament?
|
The middle glenohumeral ligament, absent in up to 30% of shoulders, is the primary stabilizer in anterior translation, with the arm slightly abducted (45 degrees)
|
|
|
What is the role of the inferior glenohumeral ligament?
|
The inferior glenohumeral ligament complex is the primary stabilizer for anterior and inferior instability in abduction. The inferior glenohumeral ligament complex is composed of the anterior and posterior bands of the inferior glenohumeral ligament
|
|
|
What is the attachment of the coracohumeral ligament?
What is the role of the coracohumeral ligament? |
Attachment: arises from the lateral border of the coracoid process, and passes obliquely downward and laterally to the front of the greater tubercle of the
humerus, blending with the tendon of the supraspinatus muscle With SGHL, resists inferior translation in adduction; part of pulley to stabilize biceps tendon in joint and groove |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Trapezius |
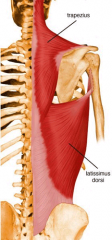
Origin: Medial third of superior nuchal line; external occipital protruberance, nuchal ligament, and spinous processes of C7 - T12 vertebrae
Insertion: Lateral third of clavicle, acromion, and spine of scapula Action: Elevates, retracts and rotates scapula; Innervation: Cranial nerve XI |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Latissimus Dorsi |
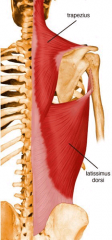
Origin: T6-S5, ilium
Insertion: Humerus, floor of intertubercular groove Action: Extend, adduct, internally rotate humerus Innervation: Thoracodorsal nerve (C6-C8) |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Rhomboid Major |
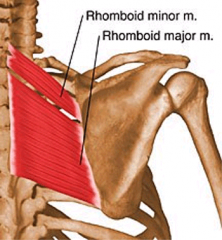
Origin: T2-T5 spinous processes
Insertion: Scapula (medial border) Action: Adducts scapula Innervation: Dorsal scapular nerve (C4-C5) |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Rhomboid Minor |
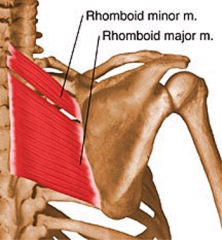
Origin: C7-T1
Insertion: Scapula (medial spine) Action: Adducts scapula Innervation: Dorsal scapular nerve (C4-C5) |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Levator Scapulae |
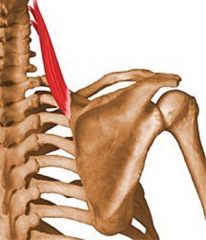
Origin: Transverse process C1-C4
Insertion: Scapula (superior medial) Action: Elevates and rotates scapula Innervation: Dorsal Scapular Nerve |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Pectoralis major |
Origin: Clavicular head: anterior surface of medial half of clavicle; Sternocostal head: anterior surface of sternum, superior six costal cartilages, and aponeurosis of external oblique muscle
Insertion: Humerus lateral intertubercular groove Action: Adducts, internally rotates humerus Innervation: Medial and lateral pectoral nerves |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Pectoralis minor |
Origin: Ribs 3-5
Insertion: Coracoid process medial border Action: Protracts scapula Innervation: Medial pectoral nerve (C8-T1) |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Subclavius |
Origin: Rib 1
Insertion: Inferior clavicle Action: Depressing clavicle Innervation: Upper trunk nerves (nerve to the subclavius) |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Serratus Anterior |
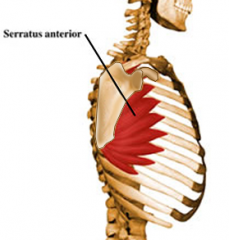
Origin: Ribs 1-9
Insertion: Ventral medial scapula Action: Draws scapula forward and upward; abducts scapula and rotates it; Innervation: Long thoracic nerve (C5-C7) |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Deltoid |

Origin: Three parts: Lateral third of clavicle, acromion, and spine of scapula
Insertion: Humerus (deltoid tuberosity) Action: Anterior part: flexes and medially rotates arm; Middle part: abducts arm; Posterior part: extends and laterally rotates arm Innervation: Axillary nerve (C5-C6) |
|
|
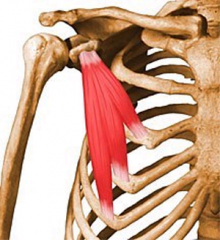
Name the origin, insertion, action, and innervation for the following muscle:
Teres Major |

Origin: Dorsal surface of inferior angle of scapula
Insertion: Humerus medial intertubercular groove Action: Adducts, internally rotates, and extends arm Innervation: Lower subscapular nerve (C6-C7) |
|
|
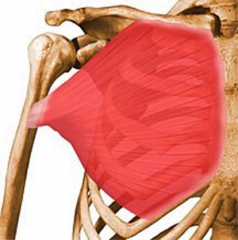
Name the origin, insertion, action, and innervation for the following muscle:
Subscapularis |

Origin: Subscapular fossa
Insertion: Humerus lesser tuberosity Action: Internally rotates arm, anterior stability Innervation: Upper and lower subscapular nerves (C5-C7). The upper and middle portions by the upper subscapular nerve, the lower portion by the lower subscapular nerve |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Supraspinatus |

Origin: Supraspinous fossa
Insertion: Humerus greater tubercle Action: Abducts and externally rotates humerus Innervation: Suprascapular nerve (C4-C6) |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Infraspinatus |

Origin: Infraspinous fossa of scapula
Insertion: Middle facet on greater tuberosity of humerus Action: Laterally rotate arm; helps to hold humeral head in glenoid cavity of scapula Innervation: Suprascapular nerve (C5-C6) |
|
|
Name the origin, insertion, action, and innervation for the following muscle:
Teres minor |

Origin: Dorsolateral scapula
Insertion: Inferior facet on greater tuberosity of humerus Action: Provides stability, externally rotates arm Innervation: Axillary nerve (C5-C6) |
|
|
What is injured in Erb-Duchenne palsy?
What is the deficit? |
Upper roots: C5-C6
Weakness of deltoid, rotator cuff, elbow flexors, and wrist and hand extensors “Waiter's tip" |
|
|
What is injured in Klumpke's palsy?
What is the deficit? |
Lower roots: C8-T1
Weakness of wrist flexors and intrinsic apparatus, Horner's syndrome |
|
|
What has a better prognosis, Erb-Duchenne or Klumpke's?
|
Erb-Duchenne
|
|
|
What is the course of the supreme thoracic artery?
|
Comes off first part of the axillary artery and runs medial to serratus anterior and pectoral muscles
|
|
|
What are the branches of the thoracoacromial trunk?
|
Deltoid, acromial, pectoralis, clavicular
|
|
|
What is the course of the lateral thoracic artery?
|
Comes off second part of axillary artery and descends to serratus anterior
|
|
|
What are the 2 branches of the subscapular artery?
|
Thoracodorsal and circumflex scapular (triangular space)
|
|
|
What is the major blood supply to the humeral head?
|
Anterior humeral circumflex provides the arcuate artery Comes off third part of the axillary artery and provides blood supply to the humeral head via the arcuate artery lateral to bicipital groove
|
|
|
What is the course of the posterior humeral circumflex artery
|
Comes off third part of the axillary artery and runs in the quadrangular space with the axillary nerve
|
|
|
What structures define the triangular space and what is found within it?
|
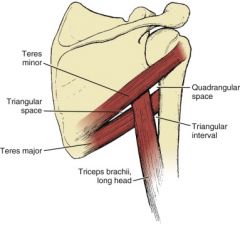
Triangular space: bordered by teres minor (superiorly), teres major (inferiorly), and long head of biceps brachii (laterally)
Contains the circumflex scapular vessels |
|
|
What structures define the quadrangular space and what is found within it?
|
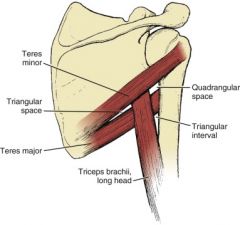
Quadrangular space: bordered by the teres minor (superiorly) and teres major (inferiorly); medial border formed by the long head of the triceps, and lateral border formed by the humerus
Transmits the posterior humeral circumflex vessels and the axillary nerve |
|
|
What structures define the triangular interval and what is found within it?
|
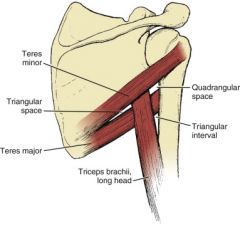
Triangular interval: immediately inferior to the quadrangular space and bordered by the teres major (superiorly), long head of the triceps (medially), and lateral head of the triceps or the humerus (laterally)
Through this interval, the profunda brachii artery and radial nerve can be seen |
|
|
What fascia extends between the coracoid prcoess, the clavicle, and the thoracic wall?
|
Clavipectoral fascia
|
|
|
What are the boundaries of the axilla?
Medial wall: Lateral wall: Posterior wall: Anterior wall: Base: Apex: |
Medial wall: Upper ribs and their intercostal muscles and serratus anterior muscle
Lateral wall: Humerus Posterior wall: Subscapularis, teres major, lats Anterior wall: Pec major and minor Base: Axillary fascia Apex: interval between clavicle, scapular, & 1st rib |
|
|
What 3 groups of arteries form the arterial anastomoses around the scapula?
|
1. suprascapular, descending scapular, and circumflex scapular
2. Acromial and posterior humeral circumflex 3. Descending scapular and posterior intercostal |
|
|
The clavicle is the most commonly fractured bone in the body, where is the weakest point?
|
At the junction of the 2 curves (middle 1/3, it is the narrowest part with no muscle attachments). Clavicle has a double curvature with sternal ventral and acromial dorsal curves
|
|
|
The sternal end of the clavicle has a small facet as well as a depression laterally to this, what are these for?
|
The facet is inferior and it is for articulation with the first rib. The depression is for attachment of the costoclavicular ligament
|
|
|
The roughened acromial end of the clavicle is for attachment of what?
|
Superior surface roughened for deltoid anteriorly and trapezius posteriorly
|
|
|
What ligaments attach to the inferior surface of the clavicle? What is their orientation?
|
Conoid ligament attaches at the conoid tubercle. There is an oblique line extending from here called the trapezoid ridge where the trapezoid ligament attaches.
Conoid is medial, trapezoid is lateral. These ligaments attach the clavicle to the coracoid (CC ligaments) |
|
|
What is the purpose of the clavicle?
|
Serves as a fulcrum for lateral movement of the arm & serves as an attachment for the upper extremity
|
|
|
What does a Zanca view evaluate and how is it done?
|
Evaluates AC joint. AP of ACJ with 10 degrees cephalic tilt
|
|
|
What view is used to evaluate the SC joint? How is it performed?
|
Serendipity. 40 degree cephalic tilt to the manubrium
|
|
|
What XR views can be used to evaluate for a hill-sachs? What view for bony bankart?
|
Hill Sachs: Stryker notch. Hand on head, 10 deg cephalic tilt
Bony Bankart: West Point. Prone, beam into axilla. Assesses the anterior inferior glenoid |
|
|
If an axillary lateral cannot be performed secondary to pain, what view can take its place?
|
Velpeau. Done by having patient lean backward at 45 degrees (leaning back with table at low back) with beam pointed direction superior to inferior at the shoulder joint
|
|
|
Clavicle fractures are divided into group 1-3 with group 1 being middle 1/3, 2 being distal 1/3, and 3 being proximal 1/3. Type 2 is broken down further, describe these
|
I: Lateral to CC ligaments
2a: Medial to CC ligaments 2b: Between CC ligaments (conoid torn, trapezoid intact) 3: Fx into AC joint |
|
|
What are the grades of AC joints separation?
|
Rockwood grades:
I: AC ligament sprain II: AC tear, CC intact III: AC & CC ligament tears <= 100% superior displacement IV: Grade III w/ posterior displacement V: Grade III <= 300% superior displacement VI: Grade III w/ inferior displacement |
|
|
What is the treatment for the different grades of AC injury?
|
Grades I&II: sling, rest, PT
Grade III: controversial. Nonop for most, CC reconstruction for high level athletes & laborers Grades IV-VI: CC ligament reconstruction |
|
|
What makes up the parts associated with the neer classification for proximal humerus fractures?
|
Anatomical neck, surgical neck, greater tuberosity, lesser tuberosity.
To be called a part, must be displaced > 1cm (0.5 for greater tuberosity) or angled > 45 deg |
|
|
What are the attachments and role of the following ligament?
Superior glenohumeral ligament |
Attachments: Anterosuperior glenoid rim/labrum to proximal lesser tuberosity
Resists inferior translation and ER in shoulder adduction. Resists posterior translation in 90 degrees of forward flexion |
|
|
What are the attachments and role of the following ligament?
Middle glenohumeral ligament |
Anterosuperior glenoid rib/labrum (inferior to SGHL) to just medial to lesser tuberosity
Resists anteroposterior translation in 45 deg of abduction. Secondary restraint to translation & ER in adduction |
|
|
What are the attachments and role of the following ligament?
Inferior glenohumeral ligament |
MOST IMPORTANT LIGAMENT, FORMS SLING THAT TIGHTENS IN ABDUCTION & ER (ANTERIOR BAND) / IR (POSTERIOR BAND)
Attachments: - Anterior Band: Anterior glenoid/labrum (3 o'clock) to inferior humeral neck - Posterior band: Posterior glenoid/labrum (9 o'clock) to inferior humeral neck. Resists posterior translation in IR & 90 deg flexion |
|
|
What is a Buford complex?
|
Thickened MGHL & absent anterior/superior labrum
|
|
|
From where does the 3 sisters vasculature arise and where is it found?
|
3 sisters run transversely across the inferior border of the subscapularis. These are branches from the anterior humeral circumflex. The axillary nerve runs just inferior
|
|
|
Where does the musculocutaneous nerve penetrate the biceps/coracobrachialis?
|
5-8 cm below the coracoid
|
|
|
Where is the axillary nerve located in relation to the posterior corner of the acromion? From the midportion?
|
5.5 cm from posterior corner
8 cm from the mid-portion |
|
|
Where is the dorsal scapular nerve found in the shoulder?
|
Deep to the rhomboid major and minor 1-2 cm medial to the border of the scapula
|
|
|
Where can a superior portal be placed in order to protect the suprascapular nerve?
|
Placement at the junction of the medial two thirds and lateral third of the superior scapular border provides >= 10mm distance
|
|
|
What is the course of the axillary nerve?
|

The nerve travels anterior to the subscapularis 3-5 mm medial to the musculotendinous border,
wraps around the surgical neck of the humerus, and passes through the quadrangular space to innervate the teres minor and deltoid muscles. The nerve lies between 4.3 and 7.4 cm from the lateral edge of the acromion.1 After entering the posterior third of the deltoid, the nerve travels along the deep deltoid fascia to innervate the middle and anterior thirds of the deltoid sequentially. The nerve to each head of the deltoid does not branch until it crosses each raphe. |
|
|
What is the course of the suprascapular nerve?
|
The suprascapular nerve originates from the fifth and sixth anterior cervical roots. The suprascapular
nerve takes form at Erb’s point from the upper trunk of the brachial plexus. The nerve then travels laterally, across the posterior cervical triangle, deep to the posterior belly of the omohyoid muscle. It then traverses posteriorly into the supraspinatus fossa through the suprascapular notch under the transverse scapular ligament giving off motor fibers to the supraspinatus. It then travels obliquely along the floor of the supraspinatus fossa toward the rim of the glenoid. The nerve then travels around the spinoglenoid notch into the infraspinatus fossa under the spinoglenoid ligament (inferior transverse scapular ligament) |
|
|
What are the 3 broad categories that the muscles of the scapular region can be classified into? Which muscles are in each category?
|
Superficial extrinsic: Join axial skeleton to the appendicular skeleton (Trapezius, latissimus dorsi). Together, these muscles originate from the entire length of the thoracic vertebral column (C7-T12) and insert laterally onto the clavicle, scapular, and humerus
Deep extrinsic muscles elevate and retract the scapula. There are 3 of these (levator scapulae, rhomboid minor, rhomboid major) Deep 'intrinsic' or true scapular: Include the rotator cuff, the deltoid, and teres major. |
|
|
Describe the anastomotic network of arteries around the scapula with the axillary artery ligated distal to the thyrocervical trunk
|
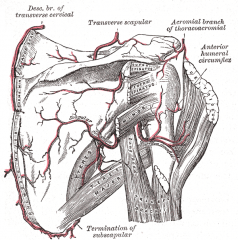
If the axillary artery were ligated distal to the thyrocervical trunk, blood would flow from the subclavian through the thyrocervical trunk into the transverse cervical and suprascapular arteries. The transverse cervical anastomoses with the Dorsal scapular artery to supply the medial aspect of the scapula and the inferior angle. The Suprascapular artery anastamosis with the circumflex scapular artery which is a branch from the subscapular artery. The subscapular artery would supply back flow to the axillary artery to continue with the blood supply to the remaining upper extremity.
|