Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
21 Cards in this Set
- Front
- Back
|
GU systems come from embryonic:
When, how many, cervical nephrotomes appear? Fxn? Mesonephros: What, how many, when, where? What do fxnal nephric units form from? How many by the 5th week? |
intermediate mesoderm, nephrogenic cord
4th week, 5-7 - no fxn 4th week, tubules within nephrogenic cords, about 40, craniocaudal mesonephric tubules - about 20 pair |
|
|
Where do mesonephric tubules drain to?
How does this form? |
fusion of tubule tip with duct provides
passage from excretory unit--> cloaca |
|
|
When, where do mesonephric ducts form?
Empty where? When do mesonephros degenerate? From when to when are they functional? Terminal (3rd) kidneys form from? Where do they form? |
24 days - dorsolateral to mesonephric tubules
into ventrolateral cloaca post week 10 functional weeks 6-10 metanephros - form from sacral intermediate mesoderm, ascend to final position induced to form metanephric blastema by the ureteric buds |
|
|
What induces metanephros formation?
How long do the metanephros develop lobules (i.e how long ureteric bud bifurcation and lobule formation continue)? What comes from the metanephros (ureteric buds)? |
ureteric buds signalling
until week 16 ureter, renal pelvis, major/minor calyces, collecting ducts |
|
|
What buds out of cloaca and what does it become?
|
Allantois (lumen), closed it becomes the urachus (median umbilical ligament)
|
|
|
Expressed by mesenchyme, makes tissue ready for ureteric bud induction:
stimulates branching of ureteric bud: proliferation of mesenchyme: Blood plasma from glomerular capillaries begins to be filtered by: |
WT1
GDNF, HGF FGF2, BMP7 by the 10th week |
|
|
Where are kidney's "formed"
|
pelvis but ascend to lumbar region with progressive revascularization from common iliac and aorta
|
|
|
Fxn of urine in embryo?
bilateral renal agenesis/obstruction may cause: Kidneys fused at base (lower pole): (occurence) What is the cloaca divided into? Urinary bladder and urethra develop from: |
supplement amniotic fluid (floating in pee)
oligohydramnios- insufficient amount of amniotic fluid horseshoe kidney- most common hindgut endoderm cloaca divided by urorectal septum into urogenital sinus & rectum |
|
|
What gives rise to spongy/penile urethra?
membranous/prostatic urethrae? What becomes the bladder? Mesonephric ducts will eventually become: |
definitive urogenital sinus
neck of urogenital sinus vesical portion of urogenital sinus the ductus deferens |
|
|
Describe the movement of the mesonephric ducts, ureteric buds in the bladder:
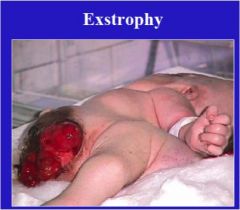
portion of bladder incorporated from mesonephric duct: Failure of midline closure of inferior abd wall: |
mesonephric ducts move inferiorly, open into the prostatic urethra, ureters open into bladder
trigone exstrophy of the bladder |
|

|
|
|
|
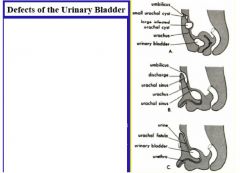
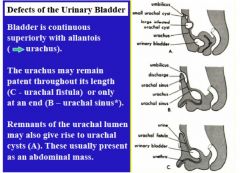
Three defects of the urinary bladder/urachus:
Two defects of ureters: Ectopic more common in boys/girls? |
continuous with allantois
urachal fistula, urachal sinus urachal cysts bifid, ectopic (DUPLICATE) more common in girls |
|
|
|
|
|
Persistent allantoic diverticulum
allows urine to escape through umbilical sinus |
urachal sinus
|
|
|
Unilateral renal agenesis - can be discovered during workup for what?
What causes agenesis? increased eye width, flattened nose, large low-set ears from oligohydramnios: |
male infertility
absence/abnormality of mesonephric duct Potter facies- associated with bilateral renal agenesis |
|
|
Renal dysplasia/agenesis often result from mutations in what gene?
Congenital polycystic kidney disease: Inheritance? Morphology? Tx for adult polycystic disease? Inheritance? |
GDNF
autosomal recessive - 1:10000 lesions in PCT, dilation/cyst formation, tissue destruction - cysts are dilated nephrons transplant - autosomal dominant |
|
|
Cancer of kidney, usually affects kids under 5, mutations in WT1 gene:
Failure of Rathke's folds to develop: What is defect? Failure of Rathke's and Tourneux's folds to develop: Results in what for femailes? |
Wilm's tumor
rectoprostatic fistula- defect in partitioning of the cloaca rectovesical fistula in females - two vaginas, uteruses emptying to bladder |
|
|
Anal canal ends as blind sac below pelvic diaphragm:
Rectum ends as blind pouch above the pelvis diaphragm: Clinical prognosis for rectovesical fistula? Why? Clinical prognosis for rectourethral fistula? Why? |
Anal agenesis
anorectal agenesis - more common poor - poorly developed sacral bones, sphincters good- needs colostomy before definitive repair period |
|
|
Between weeks______ mesonephric duct and ureteric bud incorporation into _____ ______ of urinary bladder.
|
Between weeks 4-6, mesonephric duct and ureteric bud incorporation into posterior wall of urinary bladder.
|
|
|
RESULT from growth of two ureteric buds... problems arise with bladder development original, caudal ureter opens normally, cranial ureter follows mesonephric duct
|
duplicate or ectopic ureter
|
|
|
Characterized by multifocal lesions of the
proximal convoluted tubule, loop of Henle… that result in dilation and cyst formation and destruction of the surrounding tissue. |
Congenital polycystic kidney disease
|