Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
77 Cards in this Set
- Front
- Back
|
name the 5 px feet catagories
|
sach
single axis multi-axis flexible-keel dynamic response |
|
|
SACH foot
soft heel provides more/less stability? firm heel provides more/less KNEE flexion? |
solid ankle cushion heel
more stability more flexion |
|
|
the KEEL of the SACH foot replaces what fxn?
|
grastoc
|
|
|
heel compression in a SACH at IC/LR simulates what motion?
|
pf
|
|
|
describe the 5 K levels
|
K0- non prosthetic user
K1- limited, limited potential for ambulation K2- unlimited household, ability to transverse low level barriers K3- unlimited community , ability for variable cadence K4- active adult, athlete, child. ability beyond basic ambulation |
|
|
2 indications for SACH foot
|
majority of LL amputees
peds |
|
|
contraindications for SACH
|
Active individuals
when in/ev are required individuals who need increased knee stability |
|
|
name adv / disadv for a SACH foot
|
comesis, quiet, little maintenance
deteriorations of soft material, no torque absorption |
|
|
which px foot reaches foot flat most quickly
|
single axis articulated ankle
|
|
|
primary indication for single axis foot?
|
Pt needing increased knee stability
low activity, TF amputees |
|
|
a TF amputee with what sort of muscle weakness would be good for single axis foot?
|
isolated hip extensor weakness
|
|
|
what are the indications for multi-axis feet?
|
when inv/ eversion needed
torque absorption special activities- uneven surfaces TF amputee with isolated HE weakness golfers, hikers, community outdoors, surveyors |
|
|
advantages of multi-axis feet?
|
absorbs torque
shock absorption foot conforms to surface-accomidates irregularities by bending into pro/sup used in prep limbs, peds, CONTRAIND- runners who need fast pushoff- flexible rubber keel |
|
|
disadvantage of mult-axis feet?
|
cosmesis, increased maintenance , weight
|
|
|
indications for dynamic response foot?
|
active ambulators, community ambulators
|
|
|
contraindications for dynamic response feet?
|
one speed ambulators- anyone reluctant to load the forefoot
|
|
|
advantages of dynamic response feet?
|
smoother gait
less energy expenditure light weight cosmesis dynamic energy component |
|
|
disadvantages of dynamic response feet?
|
material durability
limited sizes expense |
|
|
indication for multi-axial dynamic response foot
contraindication? |
active individual
one speed ambulators |
|
|
advantages of multi-axial DR foot?
disadvantage? |
multi-axial
dynamic response expense and maintence |
|
|
name the four socket design types
|
PTB
Total surface bearing hydostatic weight bearing combination of the 3 |
|
|
describe PTB socket v. total surface bearing
|
PTB-pressure tolerant areas
pressure sensitive areas triangular in shape *foam insert interface typically indicated for thin/boney RL Total surface bearing- uses tension values to uniformly distribute weight over the entire limb *gel liners used as interface Global reduction fleshy/ cylindrical shapes |
|
|
name 4 types of materials soft liners are made of
|
pelite
silicone urethane elastomer/mineral oil (alpha) |
|
|
name the 7 mods of suspension
|
joint and corset
belt/cuff compression sleeve suspension supra - condylar pin suction/expulsion valve vacuum |
|
|
name 6 indications for joint and corset
|
incorporates thigh weight bearing (for short RL that can't tolerate full load bearing)
improves m-l stability heavy duty user patient preference short limb- fragile skin knee instability- laxity. hyperextension stop also |
|
|
advantages of joint and corset?
|
increases weight bearing surfaces
unloads RL increases M-L/A-P stability |
|
|
disadvantages of joint and corset?
|
heavy, bulky
uncosmetic inherent pistoning |
|
|
who is indicated for suprapatellar cuff and belt?
|
majority of TT amputees
pt's with good ligaments juvenile patients long residual limbs volume changes anticipated- dialysis, post edema, CA treatment |
|
|
advantages of suprapatellar cuff?
|
also known as PTB strap-one of the most common types of strap suspensioin
provides good suspension over patella adjustable can be used in combo with waist belt |
|
|
disadvantages of supracondylar cuff?
|
can be restrictive
doesn't provide m-l stability un-cosmetic some pistioning |
|
|
who is indicated for sleeve suspension?
|
most TT amputees
pt with good ligaments juvenile amputees long residual limbs ** supplementary suspension for sports** |
|
|
advantages of sleeve suspension
|
provides excellent suspension
conseals trimlines variety of materials |
|
|
disadvantage of suspension sleeves?
|
can cause skin problems
can cause increased perspiration difficult to don not indicated for vascular pt's |
|
|
who is indicated for SCSP socket?
|
very short residual limb
requires m-l stability pt who wants less straps ** good for people with visual/hand impairments |
|
|
advantages of SCSP
|
increased wt bearing surface
increased m-L stability improved cosmesis |
|
|
disadvantages of SCSP?
|
enclosing patella can inhibit some activities
difficult to achieve suspension on obese or muscular thighs |
|
|
who is indicated for SC socket?
|
pt's requiring increased m-l stability
pt's wanting unrestricted knee extension who want less straps upper extremity involvement |
|
|
advantages of SC socket
|
less restrictive then PTB SCSP
improved cosmesis |
|
|
disadvantages of SC?
|
loss of rigid hyperextension stop
difficult to suspend on obese and muscular pt's |
|
|
who is indicated for PTB silicone suction?
|
pt's with good subcutaneous tissue
pt's with full fxn of UE those who want less suspension straps |
|
|
advantages of PTB silicon suction socket?
|
excellent suspension
eliminates pistoning of RL increased propreoception |
|
|
disadvantages of PTB silicon suction?
|
difficult to don
can't be used on all limb shapes |
|
|
vacuum and suction suspension is indicated for what sort of pt?
|
good subcutaneous tissue
want less restrictive straps can't tolerate distal pulling of shuttle pin |
|
|
disadvanges of vacuum and suction suspension?
|
knee sleeve necessary which can easily damage, restrict KF, retain perspiration
|
|
|
what is verrucous hyperplasia?
|

wart-like dry/cracked skin on the distal end of RL due to lack of total contact and negative pressure
|
|
|
what is edema?
|
excessive accumulation of fluid in tissue spaces. caused by disturbance of fluid balance between capillaries and surrounding tissues
|
|
|
what is venous insufficiency?
|
inability to drain deoxygenated blood FROM a body part
|
|
|
what is arteriole insufficiency?
|
inability to deliver oxygenated - rich blood TO a body part
|
|
|
anterior distal pressure on the tibia during dynamic alignment is caused by what 5 reasons?
|
socket too flex/ foot too DF
foot too far posterior heel too stiff posterior wall too low |
|
|
anterior distal pressure on the tibia during dynamic alignment. what are the solutions?
|
extend socket/ pf foot
move foot more anterior soften the heel |
|
|
explain the role of the quads at heel strike?
|
contracting ECCENTRICALLY to control KF
|
|
|
what phase of gait produces the most force on the ant/distal tibia
|
heel strike/loading response
|
|
|
pt is getting ant/distal pain at HS, other then alignment changes, what can be done to adj px?
|
add socks
pre tibial pads |
|
|
why do we encourage knee flexion in gait?
|
to load pressure tolerant areas.
promote KF at heel strike discourage KE at heel off |
|
|
what is optimal foot to go with a J&C?
what is optimal alignment? |
single axis foot
18mm posterior, 12 mm inset |
|
|
Describe how you would align a foot with a J&C?
|
you can inset more in order to narrow the BOS
you want an extension moment thru stance phase to load the px |
|
|
describe hydrostatic socket
|
Based on Pascals Law
increase elongation increase stiffness increase stability of boney anatomy fluid loading TSB with elongation global reduction, cylindrical shape |
|
|
what happens if J&C are positioned:
too anterior? too proximal? too distal? too posterior? |
patella tendon bar pressure
pistioning distal end pressure popliteal pressure |
|
|
what type of px is indicated for pt with genurecuratum?
|
j&c
scsp |
|
|
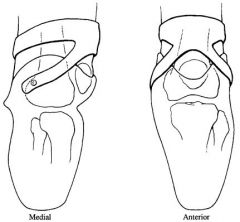
what muscles cross the knee?
|

|
|
|
what 7 anatomical considerations do you look at when evaluating a TT pt?
|
ht, wt, DOA, COA, length/shape of limb, edema, redundent tissue (verrocous hyperplasia; > 1/2"), strength/ ROM
*consider sound side limitations condition of the skin |
|
|
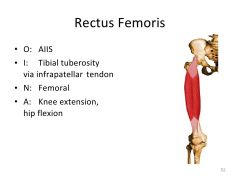
Rectus femoris- O, I, N, and A?
|
|
|
|
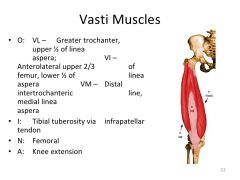
Vasti muscles- O, I, N, and A?
|
|
|
|
posterior muscles of thigh?
|
|
|
|
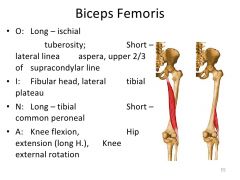
biceps femoris muscles- O, I, N, and A?
|
|
|
|
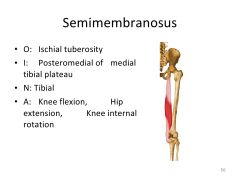
semimembranosis- O, I, N, and A?
|
|
|
|
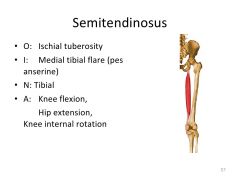
semitendonosis- O, I, N and A?
|
|
|
|
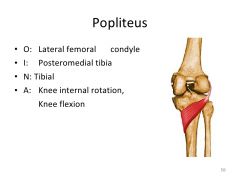
popliteus- O, I, N and A?
|
|
|
|
name the pes anserine muscles
|
|
|
|
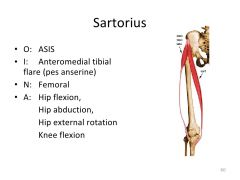
Sartorius- O, I, N and A?
|
|
|
|
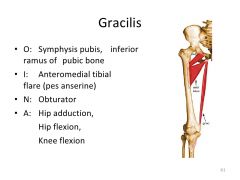
gracilis- O, I, N and A?
|
|
|
|
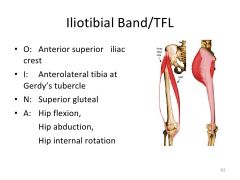
Illiotibial band/TFL- O, I, N, and A?
|
|
|
|
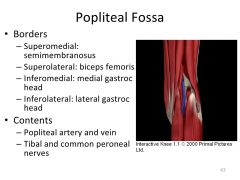
popliteal fossa-boarders and contents?
|
|
|
|
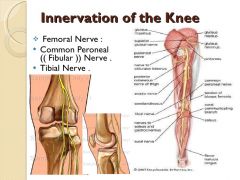
what 3 nerves innervate the knee?
|
|
|
|
congenital malformations often necessitate what sort of Px socket design?
|
fenestrations/ windows
socket strength is effected though |
|
|
what is one of the most common forms of atatomical suspension?
|
wedge above the medial femoral condyle
|
|
|
when would you use a distal end pad?
|
often on PTB sockets.
to ensure total contact distally, increase comfort, protect distal portion of RL as a result of volume loss |