Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
240 Cards in this Set
- Front
- Back
|
List the "new" 6 goals of therapeutic exercise. ***
|
- balance/postural control/stability
- coordination - cardiopulmonary fitness - mobility (flexibility) - muscle performance - relaxation |
|
|
In the "new" goals of therapeutic exercise, what constitutes balance/postural control/stability? ***
|
- ability to align body segments against gravity
- to maintain or move body within available BOS without falling - ability to hold proximal or distal body part stationary - perform superimposed movement |
|
|
In the "new" goals of therapeutic exercise, what constitutes cardiopulmonary fitness? ***
|
- ability to perform low-intensity, repetitive, total body movements over extended period of time
- endurance |
|
|
In the "new" goals of therapeutic exercise, what constitutes coordination? ***
|
- correct timing and sequencing of muscle firing
- accurate, efficient movement |
|
|
In the "new" goals of therapeutic exercise, what constitutes mobility (flexibility)? ***
|
ability of structures to move (actively or passively) to allow ROM for functional activities
|
|
|
In the "new" goals of therapeutic exercise, what constitutes muscle performance? ***
|
- ability of muscle to produce tension and do work
- strength, power, endurance |
|
|
In the "new" goals of therapeutic exercise, what constitutes relaxation? ***
|
- ability to release tension from muscles
- conscious effort and thought - manual techniques |
|
|
Definition of flexibility ***
|
- ability of a muscle to lengthen, allowing the joint(s) to move through a ROM. (Bandy & Sanders)
- ability to move joint(s) smoothly through unrestricted, pain-free ROM. (Kisner & Colby) |
|
|
Definition of stretching ***
|
- any therapeutic maneuver designed to lengthen pathologically shortened ST structures and thereby to increase ROM (Kisner & Colby)
- pathology can range from mild to severe (all of us probably have some limited ROM.) |
|
|
Definition of hypomobility ***
|
decreased ability to achieve ROM; or restricted motion
|
|
|
Definition of contracture ***
*** from her review session |
- adaptive shortening of ST around joint, resulting in significant resistance to stretch and limited ROM
-- name for action of shortened muscle |
|
|
Definition of adhesions ***
|
adherence between collagen fibers, resulting in loss of normal mobility
|
|
|
What are scar tissue adhesions? ***
|
those adherences between collagen fibers that develop in response to injury and the inflammatory response
|
|
|
Definition of overstretching ***
|
stretching beyond normal range
|
|
|
What is a selective stretch? ***
*** from her review session |
applying stretching techniques selectively to some muscles and joints but allowing limitation of motion to develop in other muscles or joints
(e.g., tenodesis action - not attempting to extend contractures of finger flexors to allow pt to form a hook) - also dislocation, subluxation (how??) |
|
|
What is elastic deformation? ***
|
when ST is stretched to new length, but returns to original length when stress is removed
|
|
|
What is plastic deformation? ***
|
upon prolonged, low degree of stress ST takes on new and longer shape
(also done with heat/thermal modalities) |
|
|
Describe a muscle spindle ***
|
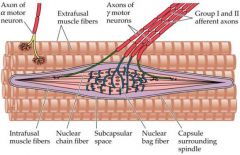
- sensory organ/proprioceptor (stretch receptor)
- responds to 1) change in muscle length, and 2) velocity at which length changes - facilitated by quick stretch |
|
|
How is a muscle spindle activated? ***
|
- by a quick stretch of muscle
- ends of intrafusal fibers connect to extrafusal fibers - {Type Ia and II} afferent sensory nerves of intrafusal fibers stimulated (excited) - afferent fibers send impulses to CNS - CNS sends impulse to muscle (via alpha motor neuron) - muscle contracts reflexively (protectively) (e.g., testing reflexes at the knee) |
|
|
What is a Golgi Tendon Organ? ***
|
- sensory receptor attached to fibers in the tendon at the junction of the tendon with extrafusal muscle fibers
- responds to change in tension of muscle-tendon unit via {type Ib} afferent fibers when the muscle 1) contracts, or 2) is passively lengthened |
|
|
To what actions is the GTO sensitive? ***
|
- active muscle contraction - low threshold (more sensitive to this)
- passive stretch - high threshold |
|
|
How is a GTO activated? ***
|
- muscle
1) contracts, or 2) is passively lengthened (book says if stretched for prolonged time period or during isometric contraction) - GTO fires {via type Ib afferents} - {Ib} afferents send impulse to spinal cord - excitation of Ib causes inhibition of alpha motor neuron - muscle relaxes (e.g., losing in arm wrestling—release to avoid tearing muscle, or a "negative" in weightlifting) |
|
|
What is autogenic inhibition? ***
|
- stimulation of a muscle that causes its neurologic relaxation
- GTO overrides excitatory impulse - causes relaxation (i.e., maximum and sub-max isometric contraction of muscle causes increase in tension in the GTO, leading to GTO activation, which causes the muscle to relax) |
|
|
What is reciprocal inhibition? ***
|
- in any synergystic muscle group, a contraction of the agonist causes reflextive relaxation of the antagonist (tight muscle)
- agonist muscle contracts - antagonist (tight) muscle is inhibited - allows smooth motion (e.g., contract the biceps, and the triceps relax) |
|
|
What are the characteristics of ST? ***
|
- contractile tissue (muscle)
- non-contractile tissue (tendons, ligaments, fascia) - both have elastic and plastic qualities |
|
|
Effects of immobilization on muscle tissue (contractile ST) ***
|
- if muscle is immobilized for a long period of time, muscle protein and number of sarcomeres decrease
- if muscle is immobilized in a lengthened position over a prolonged time, the number of sarcomeres will increase (thus if immobilization is absolutely necessary, better to be in lengthened position??) |
|
|
What happens when a stretch is applied to noncontractile ST? ***
|
the collagen bonds break (fail) and length increases
|
|
|
What is creep? ***
|
the permanent deformation of noncontractile ST when low load applied over extended time
|
|
|
Three basic types of stretching ***
|
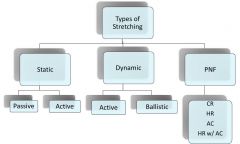
- static
- dynamic - Proprioceptive Neuromuscular Facilitation (PNF) |
|
|
Types of static stretching ***
|
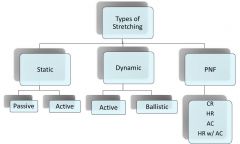
- passive
- active |
|
|
Types of dynamic stretching ***
|
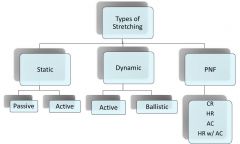
- active
- ballistic |
|
|
Types of PNF ***
|
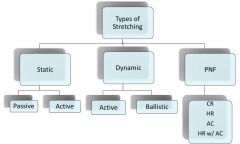
- contract-relax (CR) (similar to hold-relax but with original PNF style and a concentric contraction)
- hold-relax (HR) (autogenic inhibition) - agonist contraction (AC) (reciprocal inhibition) - HR w/AC (combination) |
|
|
What is static stretching? ***
|
- muscle is slowly elongated to tolerance; then prolonged holding in this position
- to the point of mild tension, not pain |
|
|
Differentiate active and passive static stretching ***
|
muscle is slowly elongated to tolerance; then prolonged holding in this position
- if active, self-controlled - if passive, controlled by outside force (manual or mechanical) |
|
|
How does static stretching affect muscle spindles and GTOs? ***
|
- slow, prolonged stretch minimizes effect of muscle spindle (reduces the reflex contraction)
- may facilitate GTO because it places tension on the tendon and may spur GTO to fire, relaxing the muscle for further stretching |
|
|
How long should static stretches be held for? ***
(FOOT STOMP!!) |
- 30 seconds in most cases
- 60 seconds if patient is over 65 (FOOT STOMP!!) |
|
|
What is dynamic stretching? ***
|
- uses the force production of a muscle and the body’s momentum to take a joint through full available ROM;
- stretching while moving; prepares the body for physical exertion; sports |
|
|
Two types of dynamic stretching ***
|
- active
- ballistic |
|
|
What is ballistic dynamic stretching? ***
|
- repetitive bouncing
- 10 - 15 bounces, each one extending farther - potential to cause injury; causes muscle spindle to fire (thus a protective contraction prior to the next, further bounce--ouch!!) - controversial - appropriate for some athletes |
|
|
What is PNF? ***
|
Proprioceptive Neuromuscular Facilitation
- Hold-Relax (Autogenic Inhibition) - Contract-Relax (similar to hold-relax but with original PNF style and a concentric contraction) - Agonist Contraction (Reciprocal Inhibition) |
|
|
Describe performance of Autogenic Inhibition (a.k.a. Hold-Relax) ***
|
Hamstring stretch example:
- PTA - moves pt's leg to SLR as high as possible (max ROM) - Pt - isometrically contracts (pushes back) against resistance provided by PTA at proximal ankle and knee for 8-10 sec - Pt then relaxes - PTA - moves leg into greater hip flexion, increasing length of hamstrings (facilitates GTO) and holds for 10-15 seconds - repeat cycle 3-5 times |
|
|
Describe performance of Reciprocal Inhibition (a.k.a. Agonist Contraction) ***
|
Hamstring stretch example:
- PTA - moves extended leg into full SLR available ROM - Pt - actively moves leg into greater flex [PTA may add mild resistance in opposing direction or goal ("kick my hand") for cue, sort of giving the pt something to push toward/against] - PTA - maintains leg in new position and holds 10-15 seconds - repeat cycle 3-5 times |
|
|
Describe performance of Combination PNF (a.k.a. Hold-Relax with Agonist Contraction) ***
|
Hamstring stretch example:
- PTA - moves extended leg to full SLR, max ROM - Pt - isometric contraction against resistance for 8-10 seconds - Pt - actively moves leg with agonist contraction to greater flexion ("touch your toes to my hand....") - repeat cycle 3-5 times |
|
|
What are some clinical guidelines for stretching? ***
|
- warm up and cool down
- stretch exactly opposite muscle restriction - stabilize proximal - stretch distal before proximal (puts less force/compression on joints) - should not be painful - be mindful of speed ---- static stretch should be slow; force gradually applied and released ---- dynamic stretch should be “mindful & aware” (Stetz) - stretch within reason |
|
|
Describe Ehlers-Danlos Syndrome ***
|
- inherited connective tissue disorder
- defect in synthesis of collagen – too much elasticity - affects skin, muscles, ligaments, blood vessels, viscera - can be mild to life-threatening - no cure; just support |
|
|
Important points for stretching geriatric patients ***
|
- muscle extensibility and strength decrease with age
- warm-up more important - base stretching program on functional needs - milder stretching - hold stretches for 60 seconds if 65 or older |
|
|
Important points for stretching pediatric patients ***
|
- children are more flexible than adults
- no ballistic stretching because of strain at apophyses and epiphyses |
|
|
Precautions for stretching (other than pediatric/geriatric patients) ***
|
- recent fx
- osteoporosis - weak muscles - edematous tissue - do not stretch beyond normal ROM - be mindful of intensity (high-intensity) - if soreness lasts > 24 hours |
|
|
Duration and frequency of stretching? ***
|
duration
- hold for at least 30 seconds - hold for at least 60 seconds if over 65 frequency - 2-5 times per week |
|
|
Muscle performance ***
|
- capacity of a muscle, or group, to do work
- 3 elements: ---- strength ---- power ---- endurance |
|
|
Three elements of muscle performance ***
*** from her review session |
- strength
- power - endurance |
|
|
Resistance training may incorporate.... ***
|
- strength
- power - endurance (or any combination of these) |
|
|
What is "strength"? ***
*** from her review session |
- maximum force a muscle or muscle group can exert during a contraction (Bandy & Sanders)
- maximal voluntary force that can be produced by the neuromuscular system, usually demonstrated by the ability to lift a maximal load one time, called the one-repetition maximum (Bandy & Sanders) - the ability of muscle to produce tension & resultant force based on demands placed upon it (Kisner & Colby) |
|
|
How is strength increased? ***
|
by resistance training
- heavy load - low number of repetitions - short time period |
|
|
What is "power"? ***
*** from her review session |
- rate of doing work (performing muscular contractions) over a specific amount of time
(work/time) or (force X distance)/time [(mass X acceleration) X distance]/time - related to strength and speed of movement (example used of unloading a truck) |
|
|
What is anaerobic power? ***
|
a single burst of high-intensity activity
|
|
|
What is aerobic power? ***
|
repeated bursts of less-intense activity
|
|
|
How is power increased? ***
|
- increasing the amount of work a muscle must perform in a given time, or
- decreasing the amount of time required to produce a given force |
|
|
What is "endurance"? ***
*** from her review session |
- the ability of a muscle or group to perform repeated contractions
- sometimes used interchangeably with aerobic power |
|
|
With what other term is "endurance" sometimes used interchangably? ***
|
aerobic power
|
|
|
How is endurance increased? ***
|
- low loads
- high repetitions - long time periods |
|
|
Exercise muscle actions ***
|
- isometric (contraction with no change in muscle length)
- isotonic (concentric & eccentric) - isokinetic (concentric & eccentric) |
|
|
What is concentric muscle contraction? ***
|
shortening of the muscle against resistance
(muscle performs work on resistance) |
|
|
What is eccentric muscle contraction? ***
|
- lengthening of the muscle against resistance
(resistance performs work on the muscle) |
|
|
Production of force by concentric, eccentric, and isometric maximal contractions ***
|
- eccentric maximum contraction produces more force than
- isometric maximum contraction, which produces more force than - concentric maximum contraction E > I > C - eccentric muscle action can produce about 30% more force than concentric actions - concentric muscle actions take more energy to perform - strength gains between the two types are similar, however |
|
|
What is the force-velocity relationship in a(n): ***
- concentric contraction? - eccentric contraction? |
- concentric contraction - muscle tension decreases as velocity increases
- eccentric contraction - muscle tension increases as velocity increases (theory is that this produces optimal actin-myosin overlap and creates increased muscle tension) |
|
|
Is the force-velocity relationship directly proportional or inversely proportional for ***
- concentric contractions? - eccentric contractions? |
- inversely proportional
- proportional |
|
|
Anatomy of a muscle fiber ***
|
- muscle fiber = muscle cell
- covered by endomysium - composed of myofibrils - myofibrils comprised of actin and myosin microfilaments |
|
|
What causes muscle contractions? ***
|
- motor unit (the alpha motor neuron and all the muscle fibers it innervates)
- alpha motor neuron stimulates the muscle fibers and the actin and myosin microfilaments create crossbridges and shorten the sarcomeres |
|
|
What is a motor unit? ***
|
- the functional unit of muscle
- a single motor cell (motor neuron--with body contained in anterior horn of spinal cord), plus - its axon and terminal branches, and - all muscle fibers supplied by the axon (5-100 or more) (an alpha motor neuron and all the muscle fibers it innervates) |
|
|
What affects strength of muscle contraction? ***
|
- motor unit recruitment
---- number of motor units recruited (multiple motor unit summation) and ---- frequency of stimulation (wave summation) (twitch, vermicular, tetanic) - cross section (larger = more tension) and fiber orientation (pennate produces more force than fusiform) |
|
|
Three muscle fiber types ***
|
Slow-twitch (Type I - red oxidative - SO)
-- Less tension, slow to fatigue -- Primarily for endurance Fast-twitch--fatigue resistant (Type IIa - FOG) -- Fast oxidative glycolytic -- Rapid contraction; slow to fatigue Fast-twitch--fast fatigable (Type IIb - FG) -- Fast glycolytic -- Rapid contraction, fatigue quickly |
|
|
What are some physical adaptations made by the body in response to resistance training? ***
|
- Neural adaptation - learned changes in the nervous system (motor unit better able to activate muscle via multiple motor unit summation and wave summation)
----- increase in strength manifests before the hypertrophy - Hypertrophy - in 2-8 wks (Kisner & Colby, p. 158) ----- increased fiber size (vs. hyperplasia-increase in # of fibers) ----- adults with no training lose 5-7 lbs muscle per decade - Metabolic rate increase ----- adults with no training lose 2% - 5% of metabolic rate per decade (because muscle is active tissue) - Body composition - decreased fat with weight training - Bone mineral density increases with weight training - Strength of bone, tendons, ligaments and fascia increases with weight training - Glucose metabolism increases - Resting blood pressure decreases - Blood lipid levels show improved profile - GI transit time increases |
|
|
Describe exercise "dosage" ***
|
dosage - general term for how much; can be modified in many ways
- mode (method of exercise; e.g., tubing or free weights) - repetitions - sets - given # of reps & rest - duration - # of sets & rest between - frequency - how often - volume - reps x resistance - rest intervals |
|
|
What is overload? ***
|
- increase in training load that leads to adaptation in muscle
- causes fatigue; the body recovers and adapts to overcompensate and increase fitness |
|
|
How are intensity and volume quantified? ***
|
- intensity = quality of effort - internal effort, VO2 max, lbs/lift
- volume = quantity of effort - total amt lifted, total miles run intensity and volume of training are integrally related and depend upon each other at all times |
|
|
What is specificity of training? ***
|
training should be specific to required activity for optimal benefits;
general training should precede specific training |
|
|
Which should come first, general or specific training? ***
|
general training should precede specific training
|
|
|
What is the benefit of cross training? ***
|
training in one mode may provide some transfer effects, (but has limited cross-over and is inefficient for increasing performance capacity)
|
|
|
What is overtraining? ***
|
- training loads that are too demanding, leading to fatigue, substitution, injury, performance deterioration, burn-out
- can also cause depression, chronic fatigue, anorexia, weight loss, insomnia, decreased libido, increased blood pressure, muscle soreness - can address by providing break periods, changes in routine |
|
|
What is periodization? ***
|
- advanced resistance training
- a training plan that changes the workout sessions at regular time intervals (gradual cycling of specificity, intensity, and volume) - helps to achieve optimal development of performance and prevent plateaus |
|
|
Precautions for resistance training ***
|
- pain
- inflammation - overtraining/overwork - acute muscle soreness - DOMS - fractures - cardiopulmonary disease - incorrect breathing during exertion (in general, exhale during lift) - substitute motions |
|
|
What is DOMS? ***
|
delayed-onset muscle soreness
- usually occurs within 48 hours after exercise, usually resolving within 72 hours - can last up to 1 week (eccentric mostly) - marked by edema, loss of active ROM, decreased ability to produce force - believed to be due to microtrauma to muscle and connective tissue (as the lactic acid and muscle spasm theories are now out of favor) |
|
|
What are the three theories behind DOMS? ***
|
- microtrauma to muscle & connective tissue ******
- lactic acid theory (X – old theory out of favor) - muscle spasm theory (X – old theory out of favor) |
|
|
Why is recovery time necessary after resistance training? ***
|
to avoid performance plateaus or deterioration
|
|
|
ACSM recommendations for resistance training exercise ***
|
- minimum of 8-10 exercises that train the major muscle groups
- perform one set of 8-12 repetitions to point of volitional fatigue - more sets may elicit slightly greater strength gains, but additional improvement is relatively small - perform exercises at least 2 days per week - more frequent training may elicit slightly greater strength gains, but additional improvement is relatively small - workouts should not be too long (> 1 hour are associated with high dropout rates) - adhere closely to the specific exercise techniques - perform exercises through the full ROM - perform exercises in a controlled manner - maintain a normal breathing pattern - exercise with a training partner when possible (they can provide feedback, assistance, and motivation) - elderly trainees should perform exercises in the maximum ROM that does not elicit pain or discomfort |
|
|
Strength increases in both genders linearly with chronological age until.... ***
|
age 14
|
|
|
What is open kinematic chain (OKC) exercise? ***
|
exercise in which the terminal segment is free to move
(e.g., biceps curl) |
|
|
What is isometric exercise, and when is it used? ***
|
- exercise in which tension is generated but the muscle remains the same length (e.g., muscle setting)
- limited carry-over in function, but can be very beneficial if no other exercises are tolerated |
|
|
How is isometric exercise implemented? ***
|
- hold 6-10 seconds - more research needed for ideal
- for strength gains - at least 50% (of what, maximum possible contraction??) - more research needed for ideal - multiple angle - strength gains in adjacent 30° ROM, with more ROM transfer when performed in lengthened position (thus it may make sense to exercise the muscles in the lengthened position) |
|
|
What is isotonic exercise? ***
|
literally means, “same tension,” but this is a misnomer since tension does change as length changes through full ROM due to changes in muscle length, angle of pull, and horizontal distance from resistance to joint axis
(the weight/resistance does not change--i.e., lifting the same barbell, dumbbell) better to think of it as "same weight" dynamic change in length - concentric (muscle shortens during activity) - eccentric (muscle lengthens during activity) most functional activities use both actions |
|
|
Two types of isotonic exercise ***
|
- same resistance - variable speed
(cuff weights, dumbbells, wall pulleys) - variable resistance- variable speed, using: ----- equipment (e.g.,Universal, Nautilus, Body Masters) ----- elastic resistance (e.g., Theraband) also same resistance--same speed? |
|
|
How is the length-tension relationship affected through the entire ROM of a muscle contraction? ***
|
- strength of active tension is optimal at resting length
[muscle's active length-tension force is greatest at midrange (e.g., 70-80 degrees of elbow flexion) and least at both extremes due to optimal crossbridge formation--see pp. 42-43 of "Essentials of Kinesiology for the PTA"] - strength of passive tension is optimal at slightly elongated length (1.2) and decreases as muscle is shortened or lengthened - more tension at mid-range |
|
|
What is a moment arm? ***
|
the perpendicular distance between axis of motion and line of action of muscle
|
|
|
The greater the moment arm...***
|
the greater the force produced by the muscle
|
|
|
What is isokinetic exercise? ***
|
- same speed, variable resistance
(Kin-Com, Lido, Biodex, Ariel) - easy quantification of pt info (peak torque, work, and power) - protocols usually include different velocities - stimulate maximal contraction of muscle throughout full ROM (compensates for changes in muscle length and angle of pull) - allows high speed of contraction |
|
|
Clinical guidelines for isometric exercise ***
|
- most often in early stages of rehabilitation
- can still be of benefit, even if done submaximally 6-10 second contractions multiple reps lengthened position - can be done daily if no increase in symptoms, otherwise alternate days |
|
|
What are some benefits of isotonic exercise? ***
|
- low cost
- varied equipment |
|
|
Describe the DeLorme protocol for PRE ***
|
- find 10 repetition maximum
- do 10 reps of 50% - then 10 reps of 75% - then 10 reps of 100% |
|
|
Describe the Oxford protocol for PRE ***
|
- opposite of DeLorme
- find 10 repetition maximum - do 10 reps of 100% - then 10 reps of 75% - then 10 reps of 50% |
|
|
What is closed kinetic chain exercise? ***
|
- terminal segment of limb is fixed while supporting some of the body weight
(e.g., squat, push-up) OR - joints (links) connected; and movement of one link causes motion at other links in a predictable wa. [e.g., pull-up (Lippert)] most activities are a combination of both |
|
|
Are most exercises OKC or CKC? ***
|
most are a combination of or have characteristics of both types, especially those involving the upper extremity kinetic chain
|
|
|
What is the physiological basis for CKC? ***
|
- re-establish proprioception (muscle spindles, GTOs, Pacinian corpuscles)
- induce co-contraction/force couples - improve stabilization, joint approximation - improve reflex stabilization - improve dynamic control - stimulate mechanoreceptors, closing pain gate |
|
|
What is a Colles'/Smith's fracture?
|
fracture of the distal radius
|
|
|
What is one of the most commonly seen wrist fractures?
|
Colles' (Smith's) fracture
|
|
|
Difference between Colles' and Smith's wrist fractures?
|
Colles' - distal fracture fragment displaced dorsally, wrist extended on impact; mostly older (female) patients
Smith's - distal fracture fragment displaced ventrally, wrist flexed on impact; mostly younger patients |
|
|
Primary cause of Colles'/Smith's fractures?
|
FOOSH
fall on outstretched hand |
|
|
What is RSD and how is it treated?
|
Reflex Sympathetic Dystrophy
- extreme sensitivity to touch - reduced grip strength - reduced ROM all directions - tissue swelling - cool, clammy skin treated with scrub and carry protocol (alternating compression and distraction) |
|
|
Physical therapy progression for treatment of Colles'/Smith's fractures
|
- AROM of fingers, elbow, shoulder in cast
- PROM and isometrics after cast removal, progressing to - AROM/intrinsic hand muscle exercise - strengthening, and - functional activities |
|
|
Outlook for Colles'/Smith's fractures
|
- malunion of fracture ("dinner fork" deformity) common
- stiffness and ache at joint may be permanent, especially in older patients - full recover takes at least a year |
|
|
What is adhesive capsulitis?
|
- joint capsule of shoulder becomes inflamed, thickened, and/or scarred and bones of shoulder unable to move freely
- pain in shoulder and loss of motion due to inflammation - worse at night and in cold weather |
|
|
Risk factors for adhesive capsulitis
|
- shoulder injury/surgery
- diabetes - open-heart surgery - hyperthyroidism - cervical disk disease of the neck |
|
|
Signs and symptoms of adhesive capsulitis
|
- decreased ROM in shoulder
- pain in shoulder (dull, aching) - stiffness in shoulder |
|
|
Development of adhesive capsulitis
|
Three stages
- painful stage - pain with any movement of shoulder; limited ROM - frozen stage - more stiffness and more loss of ROM - thawing stage - ROM improves |
|
|
Tests for adhesive capsulitis
|
none specifically
- X-rays can rule out arthritis - MRI can show inflammation - doctor can check ROM, and move arm for you to distinguish between frozen shoulder and rotator cuff injury |
|
|
Treatment for adhesive capsulitis
|
- stretching exercises to maintain mobility and increase ROM (therapy may be intense, but needs to be done daily)
- may include massage therapy; US, e-stim, cold packs can also be used - joint distension - injecting sterile water into joint to stretch tissue and increase ROM - NSAIDs, cortisone injections, OTC drugs - surgery - no heavy lifting, sudden jerking with that shoulder |
|
|
Cause of carpal tunnel sydrome
|
- pressure on median nerve
|
|
|
What is the most common entrapment neuropathy?
|
carpal tunnel syndrome
|
|
|
Signs and symptoms of carpal tunnel syndrome
|
- gradual onset with burning or tingling
- fingers may feel swollen and useless - pain at night may occur, with feeling on awakening of needing to "shake out" the wrist - weakness in grip and fine finger coordination - extreme chronic/untreated cases may result in wasting of muscles at base of thumb and loss of ability to distinguish hot/cold |
|
|
Tests for carpal tunnel syndrome
|
- Tinel's sign - tap median nerve at wrist; pain shoots into hand
- Phalen's test - flex wrist completely for 60 seconds to determine if it causes numbness, tingling, or weakness - electromyography - helps distinguish muscle weakness due to injury of a nerve from muscle weakness caused by neurologic disorder; can check nerve conduction velocity to assess damage to nerve - wrist x-rays to rule out arthritis or other issues |
|
|
Causes of carpal tunnel syndrome
|
- repetitive hand/wrist motions
- often congenital, some have small carpal tunnels - prior trauma/injury to wrist - associated with RA and thyroid disease - pregnancy due to fluid retention - females 3 times more likely to develop due to smaller carpal tunnels - most common in ages 30-60 |
|
|
Treatment for carpal tunnel syndrome
|
- splints - night only at first; if not helpful, daytime as well
- workplace adjustments - reduce stress on wrist (keyboards, mouse pads, etc.) - corticosteroids or lidocaine injections - OTC drugs to help with inflammation (aspirin, NSAIDs) - yoga has been shown to reduce pain and improve grip - exercises to prevent/relieve pain (wrist circles, forearm exercises, wrist stretches) - surgery - carpal tunnel release (cuts transverse ligament to enlarge carpal tunnel); open release surgery or endoscopic surgery |
|
|
Upon what does success of carpal tunnel syndrome surgery usually depend?
|
- how long the nerve has been compressed
- severity of compression |
|
|
Prognosis for carpal tunnel syndrome
|
symptoms often improve with treatment, but over 50% of cases eventually need surgery
- surgery is often successful, but full healing can take months |
|
|
What is De Quervain's disease?
|
- degeneration and progressive stenosing tenosynovitis of tendon sheaths of APL and EPB
- often accompanied by entrapment or irritation of superficial radial nerve |
|
|
What is the most common tendinitis of the wrist?
|
De Quervain's disease
|
|
|
Etiology of De Quervain's disease
|
- usually gradual onset of pain, but may be caused by trauma
- repetitive overuse in activities involving overexertion of thumb, radial deviation, ulnar deviation, simultaneous thumb and wrist movements (e.g., painting, golfing, fishing, typing, sewing) - arthritis is also predisposing factor - wristwatches and handcuffs may irritate nerve |
|
|
Signs and symptoms of De Quervain's disease
|
- main complaint is wrist pain near radial styloid
- may radiate up forearm or into thumb - ulnar deviation is limited and painful - area is tender and swollen |
|
|
Tests for De Quervain's disease
|
Finkelstein's test - pain on ulnar deviation
|
|
|
Treatment of De Quervain's disease
|
acute
- conservative PRICE - NSAIDs - modify ADLs, CP, PW US, iontophoresis subacute and beyond - mild stretching radial wrist and forearm - soft tissue mobilization, including radial nerve stretches - HEP to include radial nerve stretch - education to prevent injury and aggravating positions/activities if persistent, patient may benefit from - corticosteroid injection or - surgery to release roof of tendon tunnel, removing friction between tendons and tunnel |
|
|
Description of lateral epicondylitis
|
- "tennis elbow"
- pain at lateral elbow (lateral humeral epicondyle) - may radiate down posterior forearm - affects muscles associated with wrist extension, supination, and radial deviation - gradual onset - 4-7 times more common than medial epicondylitis |
|
|
Description of medial epicondylitis
|
- "golfer's elbow"
- pain at medial elbow (medial humeral epicondyle) - may radiate to forearm and wrist - affects muscles associated with wrist flexion and pronation - usually gradual onset, but may be sudden - 10-20% of all epicondylitis diagnoses |
|
|
Etiology of lateral epicondylitis
|
- varus stress
- inflammation of tendons at lateral elbow - microscopic tearing can lead to macroscopic tearing and failure of ECRB work or physical activity - poor technique/training/equipment - tools > 2.2 pounds - handling loads over 44 pounds 10+ times daily - repetitive movement > 2 hours daily |
|
|
Signs and symptoms of lateral epicondylitis
|
- pain at lateral elbow
- stiffness and diffuse aching - tender on palpation (ECRB, ECRL) - increased pain with supination, handshaking, gripping - frequently dropping objects held in pronated position - pain worsens with stabilizing or moving wrist with force |
|
|
Etiology of medial epicondylitis
|
- valgus stress
- inflammation of tendons at medial elbow - usually begins as microtear - development of fibrotic and inflammatory granulation tissue - most common site is between origins of FCR and pronator teres; sometimes includes palmaris longus, FCU and FDS to lesser extent |
|
|
Signs and symptoms of medial epicondylitis
|
- pain on medial aspect of elbow and/or forearm and wrist
- inflammation - wrist and grip weakness - numbness/tingling into fingers (typically 4th and 5th phalanges) - stiff elbow |
|
|
Management of lateral/medial epicondylitis
|
- decrease inflammation/pain (cryotherapy, phono/iontophoresis, e-stim, US, NSAIDs, injection)
- promote tissue healing (PRICE, avoid painful movement, friction massage) - increase flexibility - increase strength/endurance - increase functional activities and return to function |
|
|
What is glenohumeral instability?
|
- inability to maintain the humeral head centered int he glenoid fossa
- dislocation, subluxation, or apprehension - three types (anterior, posterior, or multidirectional) |
|
|
Which form of glenohumeral instability is the most common?
|
anterior instability--accounts for approximately 85% of all shoulder dislocations
|
|
|
What is anterior glenohumeral instability?
|
- head of humerus displaced anterior to glenoid fossa
- main cause is trauma; combination force of abduction, extension and external rotation - most common (85%) |
|
|
What is posterior glenohumeral instability?
|
- humeral head displaced posteriorly, behind glenoid fossa
- main causes are seizures and electrical shock which cause forceful contractions of internal rotators - uncommon due to frequent misdiagnosis |
|
|
What is multidirectional glenohumeral instability?
|
- general laxity of the ligaments surrounding shoulder joint
- excessive mobility in all directions (anterior, posterior, inferior) - also known as atraumatic shoulder instability |
|
|
What is another name for multidirectional glenohumeral instability?
|
atraumatic shoulder instability
|
|
|
Etiology of glenohumeral instability
|
traumatic or
atraumatic - joint laxity due to repetitive activities - congenital - loose ligaments, abnormally shaped bones - seizures |
|
|
Signs and symptoms of glenohumeral instability
|
- pain
- numbness/tingling of involved arm/hand - "dead arm syndrome" - decreased ability and/or weakness of the involved arm - muscle guarding - apprehension - objective tests - x-ray |
|
|
Diagnosis of glenohumeral instability
|
- various tests for laxity and apprehension
- x-rays to verify dislocation |
|
|
Treatment of glenohumeral instability
|
three phases of treatment
- protective - immobilization and physical agents - mobility - PROM, AROM - strengthening - chiefly of muscle groups responsible for preventing further instability (rotator cuff, horizontal abductors/adductors, scapular stabilizers) |
|
|
What is a Bankart Lesion?
|
tearing of the labrum associated with glenohumeral instability
|
|
|
Description of impingement syndrome
|
- tendons of rotator cuff muscles or bursae are irritated, inflamed, or degenerated
- tendons insert on humerus, which does not have enough space to clear the acromion |
|
|
Etiology of impingement syndrome
|
- subacromial spurs
- type 2 and type 3 acromions (shapes which give smaller acromioclavicular roof) - osteoarthritic spurs of AC joint (includes subacromial spurs) - thickened or calcified coracoacromial ligament - loss of (balanced pull of) rotator cuff causing superior migration of humerus - anterior or posterior capsular contractures (adhesive capsulitis) - thick subacromial bursa |
|
|
Signs and symptoms of impingement syndrome
|
- general achy pain in shoulder and upper arm
- weakness and pain in performing over-the-head activities (e.g., combing hair) - pain at night that impacts sleep |
|
|
What is a Neer's test?
|
- test for impingement syndrome
- patient internally rotates and flexes shoulder - pain = positive test |
|
|
Management of impingement syndrome
|
- acute: PRICE, NSAIDs, PW US, lidocaine injection, pendulums (if tolerated)
- sub-acute: pendulums, pulleys, decompression, strengthening of rotator cuff, CW US - HEP: pendulums, pulleys, jobe's (13 shoulder exercises), towel glides |
|
|
Surgery for impingement syndrome
|
- when non-operative treatment hasn't worked
- can enlarge space beneath acromion to allow tendon sto glide freely (acromioplasty) - arthroscopic procedure |
|
|
Muscles comprising the rotator cuff
|
- supraspinatus
- infraspinatus - teres minor - subscapularis |
|
|
Purpose of rotator cuff
|
provide the muscular force to keep the humeral head firmly in the glenoid fossa
|
|
|
Which tendon is most frequently torn in rotator cuff injuries?
|
supraspinatus (but others can tear as well)
|
|
|
Supraspinatus tendon tears frequently occur in conjunction with/due to:
|
impingement syndrome
|
|
|
How are partial rotator cuff tears treated?
Full rotator cuff tears? |
partial
- tend to recur - may be treated w/o surgery (although if > 50% torn, usually requires surgery) full tear - may be less painful than partial tear - needs surgery |
|
|
Etiology of rotator cuff tears
|
- overuse (esp overhead, e.g., painting)
- heavy lifting (esp overhead) - trauma (sports--more youth, falling--FOOSH) - aging (>40 - collagen breakdown; >60 - highest injury rate) - poor posture/weak muscles |
|
|
Signs and symptoms of rotator cuff tears
|
- shoulder pain - mild to severe during ADLs, difficulty sleeping on affected side
- weakness - loss of motion - crepitation (popping or grinding) - swelling |
|
|
Management of rotator cuff tears
|
minor - usually lasts a few days
- rest, ice, NSAIDs - gentle stretching/ROM pain in excess of 1 week - 4-6 weeks PT - HEP - corticosteroid injection - education several months of pain - surgery may be needed |
|
|
Surgery for rotator cuff tears
|
- significant pain/dysfunction after several months of conservative treatment
- repeated dislocation of unstable joint - complete tear - young athlete (heal faster and more fully due better vascularity) those over 40 usually heal better with nonsurgical intervention, unless full thickness tear post-surgical physical therapy program until healed |
|
|
What is thoracic outlet syndrome?
|
- a group of disorders that occur when the blood vessels or nerves in the thoracic outlet — the space between the clavicle and first rib — become compressed
- can cause pain in shoulders and neck and numbness in fingers |
|
|
Three types of thoracic outlet syndrome
|
- neurogenic (neurological) thoracic outlet syndrome
- vascular thoracic outlet syndrome -nonspecific-type thoracic outlet syndrome |
|
|
Description of neurogenic (neurological) thoracic outlet syndrome
|
- characterized by compression of the brachial plexus (nerve network controlling movement/sensation in shoulder, arm and hand)
- in the majority of thoracic outlet syndrome cases, the symptoms are neurogenic |
|
|
In the majority of thoracic outlet syndrome cases, the symptoms are:
|
neurogenic
|
|
|
Description of vascular thoracic outlet syndrome
|
one or more of the arteries and veins under the clavicle are compressed
|
|
|
Description of nonspecific-type thoracic outlet syndrome
|
- a.k.a. disputed thoracic outlet syndrome or common thoracic outlet syndrome
- some doctors do not believe it exists, while others say it is a common disorder - patients have chronic pain in the area of the thoracic outlet that worsens with activity, but the cause of pain cannot be determined |
|
|
Other names for nonspecific-type thoracic outlet syndrome
|
- disputed thoracic outlet syndrome or
- common thoracic outlet syndrome |
|
|
Symptoms of neurogenic (neurological) thoracic outlet syndrome
|
- wasting in the fleshy base of the thumb (Gilliatt-Sumner hand)
- numbness or tingling in fingers - pain in shoulder and neck - ache in arm or hand - weakening grip |
|
|
Symptoms of vascular thoracic outlet syndrome
|
- bluish discoloration of the hand
- blood clot under the collarbone (subclavian vein thrombosis) - arm pain and swelling, possibly due to blood clots - throbbing lump near your collarbone - lack of color (pallor) in one or more fingers or the entire hand - weak or no pulse in the affected arm - tiny, usually black spots (infarcts) on fingers |
|
|
Causes of thoracic outlet syndrome
|
- anatomical defects
- poor posture - trauma - repetitive activity - pressure on joints - pregnancy |
|
|
Nonsurgical treatments for thoracic outlet syndrome
|
- physical therapy to strengthen muscles supporting clavicle and improve posture
- NSAIDs - weight loss - lifestyle changes/workplace adjustments |
|
|
Surgical treatments for thoracic outlet syndrome
|
- if physical therapy doesn't improve symptoms
- may remove a rib (or a portion of it) or specific muscles - may reroute blood vessels around the compression |
|
|
Prevention of thoracic outlet syndrome
|
- don't carry heavy bags over the shoulder--this depresses the clavicle and increases pressure on structures in thoracic outlet
- keep shoulder muscles strong and watch posture |
|
|
Definition of loss of flexibility
|
a decrease in the ability of the muscle to deform, resulting in decreased ROM about a joint
|
|
|
Benefits of enhanced flexibility
|
- reduced risk of injury
- pain relief - improved athletic performance |
|
|
Differentiate between intrafusal and extrafusal muscle fibers.
|
- intrafusal fibers are specialized fibers within the muscle spindle
- extrafusal fibers are ordinary skeletal muscle fibers |
|
|
Contrast the muscle spindle and the GTO
|
- spindle responds to a quick stretch and causes protective contraction
- GTO responds to isometric contraction (and prolonged passive stretch) and causes muscle to stretch/relax |
|
|
Most important thing to remember with PNF
|
you need to know which is the antagonist (the tight muscle)
if patient is unable to flex, the extensors are tight if patient is unable to abduct, the adductors are tight if the patient is unable to externally rotate, the internal rotators are tight and vice versa |
|
|
Which type of stretching has the greatest potential for trauma?
|
ballistic
|
|
|
What should the patient do if, during a static stretch, the mild tension subsides (i.e., the GTO fired and the muscle has relaxed)?
|
change position/increase stretch to achieve a more aggressive stretch and to feel the mild pull or tension again
|
|
|
How can the PT/PTA enhance patient compliance with a home static stretching program?
|
integrate it into the patient's daily activities (on the phone, at the desk, in the car, in line at the grocery store, etc.)
|
|
|
If possible, the muscle to be (static) stretched should be
|
isolated
isolating the muscle is more effective than performing a general stretch that works 2-3 mucles (e.g., toe touch) |
|
|
What can happen if the patient (static) stretches past the point of mild tension into painful ROM?
|
- muscles will actually tighten
- aggressively stretching tight muscles can lead to microscopic tears, which may lead to formation of inelastic scar tissue - scar tissue will not adapt to normal demands made on the muscle, leading to injury caused by lack of blood supply and disturbed afferent input |
|
|
In which portion of the body is easier to isolate muscles for more effective static stretching?
|
lower extremities (and neck)
stretches for the upper extremities and trunk are more generalized as it is difficult to isolate muscles |
|
|
What causes age-related connective tissue stiffening?
|
- decrease in water content of tissue
- increase in collagen bundling - increase in elastin crosslinks result in decrease in distensibility and tensile strength of muscles, fascia, tendons, skin, and bones |
|
|
How is strength assessed?
|
in terms of
- force (mass X acceleration) - torque (rotational work) - work (force X distance) and - power (work/time) |
|
|
What is force?
|
that which causes change in an object's motion
mass X acceleration |
|
|
What is torque?
|
the concept of rotational work compared with the idea of force as linear motion
angular velocity, or displacement around an axis at the rotational speed |
|
|
What is work?
|
force X distance
(mass X acceleration) X distance the product of the force exerted on an object and the distance the object moves in the direction of the force |
|
|
Where do muscle fibers begin and end?
|
they do not all run through the entire length of the muscle, or even through a fasciculus
they can - begin in the periosteum and end in the muscle - begin in the tendon and end in the muscle - begin and end in the muscle |
|
|
Because the muscle fibers do not run the full length of the muscle, what needs to happen to transmit the force of muscle contraction?
|
connective tissue sheaths (endo/peri/epimysium) must transmit the force of muscle contraction from fiber to fiber, then to fasciculi, and on to tendons which then act on bones
|
|
|
What makes up the contractile element of a muscle?
|
actin and myosin filaments
|
|
|
What is sarcolemma?
|
the membrane which encases the myofibrils
|
|
|
What is an innervation ratio?
|
the total number of motor axons divided by the total number of muscle fibers in a muscle
- muscles involved in delicate or intricate movements have lower ratios (like 1:4) - muscles involved in larger, gross motor or postural movements have higher ratios (1:150) |
|
|
How does a motor unit contract only a portion of the fibers it innervates?
|
it cannot
the motor unit operates on an "all or none" principle, thus all fibers contract and exert force or none of them do they also contract completely or not at all |
|
|
During submaximal efforts, muscular contraction is obtained by using a combination of:
|
- multiple motor unit summation
and - wave summation |
|
|
How do multiple motor unit summation and wave summation work together to produce a
- weak contraction? - strong, but submaximal, contraction? |
- only one or two motor units contract at only 2-3 times per second, with the contractions spread one after another among different motor units to achieve a tetanized state
- more motor units work simultaneously and fire more frequently |
|
|
Asynchronous vs. synchronous firing of motor units
|
- asynchronous - fewer motor units fire out of phase and less frequently to produce weaker contraction
- synchronous - majority of motor units discharge together at maximal frequency (tetanic) |
|
|
Characteristics of SO, FOG, FG muscle fibers
- diameter - muscle color - capillary bed |
SO............FOG............FG
small .....intermed.......large red............red.............white dense.....dense.........sparse |
|
|
Characteristics of SO, FOG, FG muscle fibers
- myoglobin content - mitochondria |
SO............FOG............FG
high.......intermed.........low many.......many.............few |
|
|
Characteristics of SO, FOG, FG muscle fibers
- speed of contraction - rate of fatigue |
SO............FOG............FG
slow...........fast............fast slow........intermed.......fast |
|
|
Characteristics of SO, FOG, FG muscle fibers
- motor unit size - conduction velocity |
SO............FOG............FG
small....intermed/lg.....large slow...........fast.............fast |
|
|
Immobilization leads to muscle atrophy, but which is more pronounced, loss of muscle mass or loss of function?
|
loss of function
|
|
|
Endurance exercise improves cardiovascular fitness, but does not prevent
|
loss of muscle tissue
|
|
|
OKC and CKC exercises produce markedly different...
|
- muscle recruitment and
- joint motions |
|
|
Most human movements contain a combination of what types of motion?
|
OKC and CKC motion
|
|
|
To realize meaningful results while observing the law of specificity, exercises should be performed near the absolute intensity limit only....
|
55-60% of the total training time during preparation period
(intensity is increased to 80-90% during competitive period) |
|
|
Progress for the beginner is demonstrated by a linear increase in
|
intensity (quality) and
volume (quantity) |
|
|
At the elite level, linear increases in intensity and volume will not yield desired results and ____ ____ may be required to stimulate further improvement.
|
load leaping
|
|
|
When speed and strength are the main demands ____ must be emphasized.
|
intensity
|
|
|
When endurance is the main demand, ____ represents the principal stimulus for progress.
|
volume
|
|
|
Performance of a muscle is affected by:
|
- motor unit activation (multiple motor unit summation and wave summation
- cross-sectional area - force-velocity relationship |
|
|
What factors affect the amount of torque produced by a muscle contraction?
|
- length of moment arm (longer = more force)
- angle of muscle insertion (closer to 90 degrees = more force; greater or lesser than that and torque is lost to compression or distraction---e.g., biceps vs brachioradialis/spurt vs shunt) |
|
|
Describe DAPRE
|
Daily Adjusted Progressive Resistance Exercise
uses previous performance to calculate following workout - based on 5- or 7-repetition maximum; from there, do: ----10 reps with 50%, followed by ---- 6 reps with 75%, then ---- to failure with 100% and adjust per chart for 4th set ---- to failure again with adjusted weight use 4th set to determine (per chart) starting weight for next workout and start as above with 10 reps at 50%, etc. |
|
|
When starting an isotonic program, what is critical to remember, especially for patients with musculoskeletal pathology?
|
- low reps/high resistance (strength building) may cause injury
- must avoid causing swelling and discomfort while having patient work to maximum exercise tolerance - high repetitions (2-3 sets of 10-12 repetitions) and low resistance (endurance) should be used initially - patient should work submaximally (limited progressing to full ROM submaximally, then culminating in full ROM with maximum effort) |
|
|
Clinical advantages of isokinetic exercise
|
- ability to control velocity of movement of exercising limb segment (can exercise at multiple speeds--velocity spectrum and recruit desired fibers SO, FOG, FG)
- accommodating resistance that allows for maximal muscle loading throughout ROM - quantitative performance assessment |
|
|
Most common isometric muscle sets for the lower extremities
|
- gluteal sets (pinch together)
- quad sets (supine - push back of knee into mat) - hamstring sets (supine - push heel into mat to produce isometric hip extension contraction) |
|
|
Describe multiple-angle isometrics
|
can be done with isokinetic machine or in free space
usually done with "rule of 10" - 10-second contraction - 10-second rest - 10 repetitions - 10 sets (one each at 10 different angles) |
|
|
Open-chain activities are associated with _____ forces across the joint, especially parallel to the _______.
|
shearing
tibiofemoral joint |
|
|
Although open-chain resistance training is not particularly functional, it provides a means of _______
|
isolating muscle groups
(e.g., can help strengthen quadriceps muscles, which, when weak, are associated with increased chair rise times and difficulties climbing stairs) |
|
|
Athletes with reduced cocontraction and strength imbalances cannot appropriately dissipate....
|
ground-reaction forces, thus are at increased risk of knee injury because other static tissues (e.g., ligaments) are excessively stressed
CKC can help with this by providing joint compression, increasing neuromuscular control and enhancing joint stability |
|
|
How are CKC exercises generally progressed?
|
- from static to dynamic
- from stable to unstable - from straight planes to diagonal planes - from single-plane to multiplane movements - from wide base of support to narrow BOS - from bilateral support to unilateral support - from no resistance to resistance - from rhythmic stabilization to resistance throughout ROM - from fundamental movements to dynamic, challenging movements - from consistent movements to perturbation training |
|
|
Treatment for acute orthopedic syndromes
*** from her review session |
rest, ice
(PRICE and isometrics?) |
|
|
Treatment for subacute orthopedic syndromes
*** from her review session |
- strengthening
- flexibility - (P)ROM |
|
|
Treatment for chronic orthopedic syndromes
*** from her review session |
back to function
|
|
|
Contrast PROM and stretch
*** from her review session |
PROM - move extremity through available ROM
stretch - beyond ROM, trying to stretch something that is pathologically tight |
|
|
Differentiate plastic and elastic deformation
*** from her review session |
- plastic deformation - soft tissue stays elongated (at least to a degree and for a bit of time)
- elastic deformation - goes back after stretch |
|
|
Role of the muscle spindle
*** from her review session |
- responds to quick stretch
- contracts the muscle protectively - a reflex by a sensory receptor/proprioceptor in the muscle |
|
|
Intrafusal vs. extrafusal
*** from her review session |
- intrafusal - within the muscle spindle
- extrafusal - skeletal muscle fibers |
|
|
Role of the GTO
*** from her review session |
- also a proprioceptor (like muscle spindle)
- reflexively relaxes muscle in response to: 1) strong contraction (more effective here) or 2) passive stretch (held for a long time) |
|
|
What proprioceptor does autogenic inhibition activate?
*** from her review session |
GTO
|
|
|
Term used (somewhat) interchangeably with autogenic inhibition
|
hold-relax
|
|
|
How does reciprocal inhibition work?
*** from her review session |
the agonist contracts, spurring the antagonist (tight muscle) to relax
|
|
|
Can muscles be transformed from slow twitch to fast twitch?
*** from her review session |
no
nor is increase in size due to hyperplasia (making more fibers) it is due to hypertrophy (increased size in existing fibers) |
|
|
How are muscles lengthened?***
|
by breaking sarcomeres
1 sarcomere splits into 2 |
|
|
What is the Rockwood 5?
*** |
a protocol of 5 shoulder exercises performed with elastic tubing
flex, extend, abduct, ER and IR |
|
|
If the therapist is wanting to do PNF stretching, but the patient cannot tolerate hold-relax/autogenic inhibition, what should the therapist do?
|
try agonist contraction/reciprocal inhibition
it is milder and may be better tolerated |