Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
222 Cards in this Set
- Front
- Back
|
What ion rushing into the neuron causes the release of neurotransmitters from the pre-synaptic vesicle?
|
Calcium
|
|
|
DSM in psychiatry stands for?...
|
Diagnostic Psychiatric Manual
|
|
|
Name three of the seven neurotransmitters affected in schizophrenia.
|
Dopamine
Serotonin GABA Glutamate Acetylcholine Norepinephrine Neuropeptides like cholecystokinin |
|
|
Why does talking about chemical imbalances as a whole not work in psychiatric disorders?
|
Neurotransmitters have different functions and different levels of concentration in parts of the brain. Taking the average of all the parts does not help diagnosing CNS disorders.
|
|
|
A drug used to treat schizophrenia will have what effect on dopamine? What symptoms may be generated?
|
Lower dopamine
Too little dopamine = Parkinson-like symptoms |
|
|
The major neurotransmitter that is altered in schizophrenia is?...
|
Dopamine
|
|
|
Why does EEG make it obvious it's used in brain waves?
|
EEG = Electroencephalography
-Encephalo- = brain |
|
|
Of the 4 waves involved in EEGs, which one has the highest frequency? Which has the lowest?
|
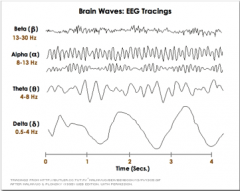
Beta has the highest frequency (13-30 Hz)
Delta has the lowest frequency (0.5-4 Hz) |
|
|
Which brain wave is common during sleep?
|
Delta waves
|
|
|
What brain wave is involved in intense activity?
|

Beta waves
|
|
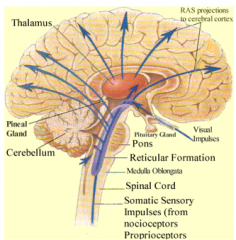
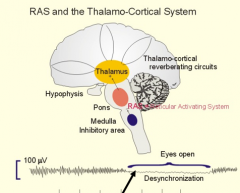
RAS stands for reticular activating system. What is its major function?
|
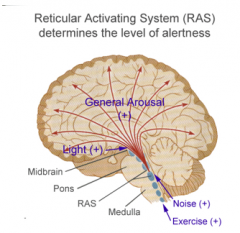
RAS determines level of alertness (awake and attentive vs. zoning out and sleeping)
When fully engaged, the RAS makes you fully aware to your surroundings |
|
|
The thalamus is a relay station for every sense except for which?
|
Smell
|
|
|
What other system is independent of RAS but also plays a role in alertness?
|
Thalamic system (the thalamus)
|
|
|
When you are focused and ignoring your surroundings, what system are you using?
What brain waves would most likely appear in an EEG? |
Thalamic system
Alpha waves |
|
|
You're studying and focused. What brain wave is most prevalent?
Suddenly an ******* blows a whistle. What brain wave is most prevalent now? |
Alpha wave
Beta wave |
|
|
In terms of survival and evolution, why do humans have a RAS?
|
RAS is a filter. A sound, visual or smell demands you pay attention to your surroundings and see if there is a threat. The RAS would be engaged at this time.
|
|
|
A theory of ADHD is that what two systems are "out of whack?"
|
RAS (reticular activating system) = attention to surroundings
Thalamic system = attention and focus |
|
|
ADHD itself involves hyperactivity. What is the reasoning behind giving them a CNS stimulant such as Adderall?
|
The stimulant in theory would bring the "out of whack" system (RAS or thalamic system) back into balance (according to the theory)
|
|
|
Hearing a car alarm while trying to sleep will keep you awake. What is the mechanism of action for this?
|
A car alarm is an external sound, thus activating your RAS to make you aware of your surroundings. This keeps you awake.
RAS promotes wakefullness |
|
|
What neurotransmitter promotes sleep?
|
Serotonin/serotonin precursors
Blocking serotonin can give insomnia |
|
|
Inhibiting 5-HT synthesis will have what effect on your sleep cycle?
|
Serotonin promotes sleep, so blocking its production can give long lasting insomnia
|
|
|
What happens to brain and body temperature during sleep?
|
Temperature decreases (likely due to metabolism but not positive)
|
|
|
Is sleep an active or a passive process?
|
Active process -- brain must actively inhibit arousal systems
|
|
|
Would the neurotransmitter GABA inhibit or promote sleep?
|
GABA = inhibitory NT in CNS
Promotes sleep |
|
|
Being awake is a mixture of what two brain waves?
|
Alpha and beta, depending on situation
|
|
|
If you look at an EEG reading of someone in REM sleep, what would it appear to be like?
|

It would appear as if they were awake
It would look like alpha or beta waves |
|
|
Entering REM for the first cycle takes about how long after falling asleep?
|
1 to 2 hors
|
|
|
How is the amount of time in REM sleep affected the longer you sleep?
|
Throughout sleep, the amount of time spent in REM increases with each cycle
|
|
|
What % of a night's sleep is spent in REM?
|
About 25%
|
|
|
If REM is the deep sleep that repairs mental aspects, why does the body still have other stages before REM sleep?
|
First 4 stages are thought to be a time for physical repair (even though metabolism is slowed down)
|
|
|
What age range experiences the most REM sleep?
|
Young children
Total REM sleep decreases with age |
|
|
Which neurotransmitter can paradoxically both promote sleep and wakefulness?
|
Serotonin
|
|
|
Which two neurotransmitters promote wakefulness and can also can be found in CNS stimulant drugs?
|
Dopamine
Norepinephrine |
|
|
Drug X is an antagonist to H1 receptors in the brain. What class would drug X fall into?
|
Anti-histamines
Blocking H1 would promote drowsiness as H1 agonists promote wakefulness |
|
|
Hypocretin/Orexin is a neurotransmitter in the brain. Does it promote drowsiness or wakefulness?
|
Wakefulness
|
|
|
GABA agonists promote sleep and inhibit the function of the RAS. What widely prescribed drug class would work through this mechanism?
|
Benzodiazepines
(Barbiturates technically also affect GABA) |
|
|
Trytophan is converted to what neurotransmitter that promotes sleep?
|
Serotonin
|
|
|
Coffee inhibits which neurotransmitter that promotes sleep?
|
Adenosine
|
|
|
When ATP is hydrolyzed it turns into what neurotransmitter?
|
Adenosine
Adenosine promotes sleep. Makes sense that when ATP is used up you would get fatigued. |
|
|
What neurotransmitter is associated with the circadian cycle?
|
Melatonin
|
|
|
How can the concept of jet lag be explained using the circadian cycle?
|
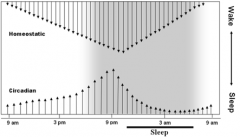
In jet lag, the homeostatic factor stays the same (your body), but by changing time zones you are changing what time you wake up and go to bed. This affects the circadian cycle
|
|
|
What are the two input signals for the circadian system model?
|
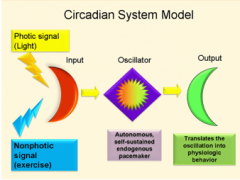
Light and darkness
|
|
|
What is the oscillator in the circadian system model?
|
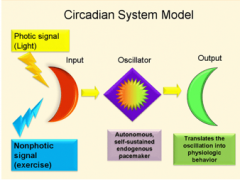
Suprachiasmatic nucleus
|
|
|
What neurotransmitter does the suprachiasmatic nucleus regulate?
|
Melatonin
|
|
|
Melatonin synthesis starts with what neurotransmitter?
|
Serotonin
|
|
|
What hormone peaks at the middle of the night?
|
Melatonin
|
|
|
What would inhibit the activity of the suprachiasmatic nucleus?
|
Light
The nucleus regulates melatonin which promotes sleep |
|
|
What is the rate-limiting enzyme in melatonin synthesis?
|

HIOMT (hydroxyindole-O-methyltransferase)
|
|
|
Melatonin is made in what gland?
|
Pineal gland
|
|
|
Does melatonin increase or decrease with age?
|
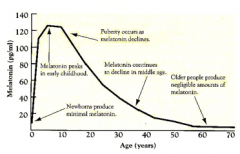
Decrease
REM sleep also decreases with age |
|
|
Why is SAD (seasonal affective disorder) most common in the winter?
|
In winter the sun sets early = less light
Light regulates the suprachiasmatic nucleus (which makes melatonin) and messing with hormones is thought to be a cause of SAD Behavorial changes in the winter can also play a role |
|
|
Orexin deficiency is thought to be the cause of what disease/condition?
|
Narcolepsy
Orexin is a wakefulness promoter, thus CNS stimulants are used in this condition |
|
|
What is Modafinil's mechanism of action?
|
It activates orexin/hypocretin neurons which promote wakefulness
Modafinil also has slight dopamine release and norepinephrine reuptake inhibition as well, but is not the main mechanism |
|
|
90% of patients have decreased orexin A levels in what disease/condition?
|
Narcolepsy
|
|
|
How is Modafinil's mechanism of action different from amphetamines?
|
Modafinil activates orexin neurons
Amphetamines release dopamine Orexin activates histamine neurons to promote wakefulness |
|
|
If you want to use a sedative-hypnotic for anxiety, what dose (low/medium/high) and what duration of action (short/medium/long) would be ideal?
|
A low doe but long acting sedative-hypnotic would be ideal.
|
|
|
If you want to use a sedative-hypnotic for sleep, what dose (low/medium/high) and what duration of action (short/medium/long) would be ideal?
|
A high dose and shorting acting sedative-hypnotic would be ideal.
|
|
|
Is it easier to overdose on alcohol or benzodiazepines?
|
Alcohol
|
|
|
A "metabolically-stable" barbiturate would have what general duration of action?
|
Longer acting
|
|
|
Methohexital, thiamyl & thiopental are all given by injection. What is their onset & duration of action?
|
Quick onset (1 minute or less)
Ultra-short duration (only lasts a few minutes) |
|
|
Phenobarbital has what general duration of action?
|
Long (Lasts 8-12 hours)
|
|
|
Even though phenobarbital is a sedative-hypnotic, it is not ideally used for insomnia. Why not?
|
REM supression
Don't want long-acting sedative-hypnotics for sleep (want high dose and short acting) Reduces respiratory drive |
|
|
What is the basic mechanism of action of benzodiazepines and barbiturates (although not identical)?
|
They reduce neuronal excitability by potentiating GABA
|
|
|
In terms of benzodiazepine abuse, what duration of action (short/medium/long) is preferred?
|
Short/medium preferred
|
|
|
Knowing what symptoms benzodiapines produce, what would benzodiazepine withdrawl symptoms be?
|
Benzodiazepines = drowsiness, relaxation, relief of seizures
Thus withdrawl = insomnia, agitation, seizures |
|
|
Why do some anti-histamines produce drowsiness while others do not?
|
The ones that promote drowsiness can cross the BBB and have a CNS effect
The non-drowsy ones do not cross the BBB |
|
|
The most common herbal used for sleep is Valerian. What is its mechanism of action?
|
Its active ingredient, valerenic acid, potentiates GABA (inhibitory NT) thus promotes sleep
|
|
|
What makes the CNS depressant Chloral Hydrate dangerous to be used with alcohol?
|
Both alcohol and Chloral Hydrate use the enzyme alcohol dehydrogenase. With only a limited amount of enzyme, you get higher serum concentrations of the two.
|
|
|
What hypnotic was marketed as a "safe barbiturate substitute" but later became a Schedule I drug?
|
Methaqualone
|
|
|
What three locations can you find receptors for melatonin
|
CNS (MT 1 & MT 2)
Retina (MT 2) Gut (MT 3) Technically also found in the suprachiasmatic nucleus but that would fall under CNS |
|
|
The drug Ramelteon (Rozerem) is a MT1/MT2 agonist. What would the effects of the drug be?
|
MT1 & MT2 agonists for melatonin both promote sleep
|
|
|
Doxepin is an anti-depressant/hypnotic agent that is an antagonist of what receptor?
|
H1 antagonist (histamine)
Histamine normally stimulates wakefulness, thus an antagonist would be a hypnotic. |
|
|
Why is Doxepin a prescription anti-histamine while diphenhydramine is not?
|
Doxepin (H1 antagonist) has been shown to possibly create a tolerance as well as a
|
|
|
There already exist quite a few histamine antagonists. What advantage would H3 agonists (autoreceptors) have over them in terms of selectivity/side effects?
|
H3 agonists, being autoreceptors, inhibits the release of neurotransmitters
While H1 antagonists have CNS & allergy side effects, autoreceptors are only found in the CNS, thus H3 agonists would not affect allergy receptors |
|
|
Trazadone is a relatively common anti-depressant. What makes it also effective for insomnia? (What receptor does it target?)
|
It is a 5HT (serotonin) partial agonist
While serotonin can both inhibit and promote sleep depending on location/receptor, here it promotes sleep |
|
|
What potent benzodiazepine is frequently associated with date rape?
|
Flunitrazepam (Rohypnol)
Clonazepam and lorazepam are also used, but not nearly as potent |
|
|
GHB is a rapist's drug of choice for victims. What properties make it ideal for this sick use?
|
The onset of action is about 15 minutes
GHB is rapidly metabolized and is undetectable in the urine after 24 hours Produces amnesia Odorless & tasteless |
|
|
GHB-2 is a "dance club rape" drug. Why is this also abused by body builders?
|
They believe it raises growth hormone (no solid evidence in this)
|
|
|
What is the only drug that falls under two different control schedules?
|
GHB
C-III for narcolepsy use C-I otherwise |
|
|
GA's are relatively non-specific CNS depressants. Generally, these affect what area of the body?
|
Lipid-rich tissue, such as the brain, cardiac and smooth muscle
|
|
|
Why do GA's have a small narrow of safety?
|
They are non-specific and concentration dependent
|
|
|
What four essential components/symptoms make up anesthesia?
|
Analgesia
Hyponosis/Unconsciousness Depression of spinal motor reflexes Muscle relaxation |
|
|
What is the basic MOA of GAs?
|
Target lipid portion of cell membranes and dissolve. This disrupts normal composition, structure and function of proteins/ion channels embedded in the cell membrane
|
|
|
You have two GA gases: a low blood solubility gas and a high blood solubility gas. Assuming all other factors are negligible, which one would produce unconsciousness first?
|
Low blood solubility.
Low solubility means not much gas is dissolved and bound in the blood. Thus more molecules are "free" and able to interact with lipid tissues such as the brain. |
|
|
What portion(s)/area(s) of the brain are first to be affected by GAs? Last to be affected?
|
The top of the brain is affected first and the bottom (brain stem) is affected last. Since vital functions such as breathing are in the brain stem, you can produce unconsciousness without death (affected last)
|
|
|
In terms of circulation, why do inhalable GAs affect the brain so quickly?
|

The blood receives much of the arterial blood coming from the lungs
|
|
|
In terms of induction and recovery time, what is a major difference between low and high blood solubility GA gases?
|
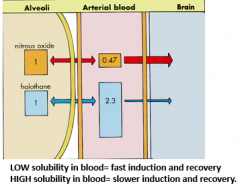
Low = fast induction and fast recovery
High = slow induction and slow recovery |
|
|
What is the general molecular makeup of inhalable GAs?
|
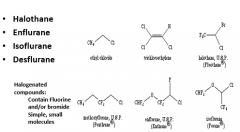
Simple, small molecules that are halogenated (usually with fluorine or bromide)
|
|
|
What is MAC and how does it apply to inhalable GAs?
|
Minimum Alveolar Concentration (MAC) of the anesthetic at one atmosphere (760 mmHg) that prevents movement in 50% of patients (ED50)
|
|
|
How were MAC values standardized? Why is this somewhat of an issue?
|
By 40 year old healthy individuals.
They aren't generally the type to undergo many procedures, while the elderly are. |
|
|
Which inhalable GA is more potent? Halothan with a MAC of 0.75% or Enflurane with a MAC of 1.63%?
|
Halothan is more potent
MAC is the anesthetic concentration at one atmosphere needed to make an ED50 (50% of people) unconscious. A lower MAC means less gas is required to produce ED50% and thus more potent. |
|
|
Isoflurane has a MAC of 1.17%. What does that mean?
|
MAC is the anesthetic concentration at one atmosphere needed to make an ED50 (50% of people) unconscious.
That means a 1.17% concentration of isoflurane in the air is needed to make 50% of people unconscious |
|
|
What gas has a MAC value of 104%? What does this mean?
|
Nitrous oxide (NO).
It means that by itself NO cannot induce anesthesia in 50% of patients. Also theoretically impossible to go over 100% as 100% = all the air in the lungs = NO |
|
|
Anesthetic MAC values change with the age of the patient. What is the general rule?
|
MAC values decrease with age by about 6% per 10 years and appear to be independant of which agent is used
|
|
|
What form of anesthetics is used for induction of anesthesia? What form is used for anesthetic maintenance?
|
Parenteral anesthetics by IV produces rapid onset. Inhalations used generally for maintenance.
|
|
|
The modern theory for how injectable GAs work is through what mechanism?
|
Modulation of GABA. Other theories include glutamate, glycine and ion channels.
It's possible that different symptoms/effects (amnesia, analgesia, etc.) occur through interaction of the anesthetic with different proteins |
|
|
How do anesthetics by injection differ in MOA from anesthetics by inhalation?
|
Injection: GABA enhancement
Inhalation: Lipid solubility --> disrupt lipid membranes |
|
|
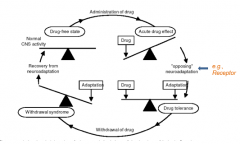
Tolerance is generally thought of as a reduction of response to a drug over time. How may tolerance be a good phenomenon?
|
Tolerance to side effects
The longer a patient is on L-DOPA, the less nausea they get |
|
|
Tolerance is reversible and dependent on what three factors?
|
The drug, the dose and the frequency
|
|
|
Over time, a patient experiences more of a response at any given dose. What is this called (the opposite of tolerance)?
|
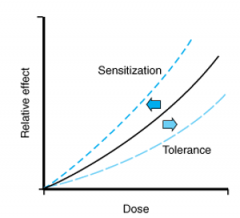
Sensitization
|
|
|
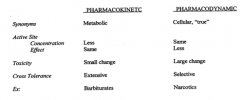
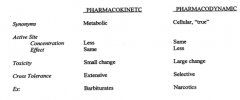
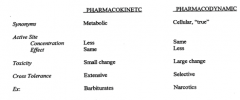
What is pharmacokinetic/dispositional tolerance?
|
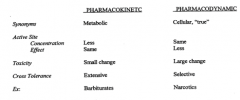
Says that tolerance is produced by a change (tolerance = decrease; sensitization = increase) in the concentration of drug that reaches the site of action.
Once it gets to the site, the receptor response is the same. Thought this happens when the drug induces self-metabolism |
|
|
What is pharmacodynamic/cellular/true tolerance?
|
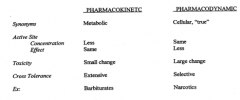
Says that tolerance is produced by a change (tolerance = decrease; sensitization = increase) in the receptor response.
The concentration of drug that gets to the target site is the same |
|
|
What is cross-tolerance?
|
You take drug A. When you switch to an equivalent dose of drug B, you get less of the expected response
|
|
|
Which of the two has a higher chance of producing toxicity when you attempt to counter tolerance: pharmacokinetic tolerance or pharmacodynamic tolerance?
|
Pharmacodynamic tolerance has more worry about toxicity when attempting to counter. The concentration of drug hasn't changed, so when you counter this tolerance, you further increase the dose throughout the body which can lead to toxicity
|
|
|
How can pharmacokinetic tolerance lead to cross-tolerance?
|
Pharmacokinetic tolerance is thought to be through self-metabolism, aka through enzyme induction. Drugs that use this same enzyme will thus produce less of an effect, appearing as cross tolerance.
|
|
|
How can pharmacodynamic tolerance lead to cross-tolerance?
|
Pharmacodynamic tolerance produces a less sensitive receptor. Drugs that use this receptor will produce less of an effect, thus appearing as cross-tolerance
|
|
|
What class of drugs most commonly produces pharmacokinetic tolerance? What class for pharmacodynamic tolerance?
|
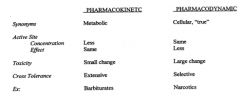
Pharmacokinetic tolerance = barbiturates = self-metabolizing/enzyme inducing
Pharmacodynamic tolerance = narcotics = less receptor response (Mu-opioid receptors) |
|
|
How can one safely counter pharmacokinetic tolerance? How can you counter pharmacodynamic tolerance?
|
Pharmacokinetic tolerance involves metabolism, thus you generally can increase the dose and still have therapeutic responses without toxicity
Pharmacodynamic tolerance involves receptors, thus there you can increase the dose to get a therapeutic response, but this may lead to toxicity in other parts of the body |
|
|
What is the most common yet broad psychiatric illness?
|
Anxiety
|
|
|
What does DSM 5 stand for?
|
Diagnostic and Statistical Manual #5
|
|
|
What is a major problem of diagnosing psychiatric illnesses between physicians?
|
Symptoms are subjective - symptoms stated by the patient
Physicians have to be complete and comprehensive in exams as otherwise the amount investigated by the doctor varies |
|
|
What is the difference between "mood" and "affect" in the mental status exam?
|
Mood is how the patients feel themselves
Affect is what is expressed by the patient, and may differ from mood. |
|
|
In mental status exams, why do physicians care about the patient's self-concept, thought process, judgment, insight, etc.?
|
These are all higher orders of brain activity and thus the information given by the patient is important in diagnosing psychiatric illnesses from other conditions.
|
|
|
Which of the following is an existing psychiatric rating scale?:
MMRS ESS AYM YMRA |
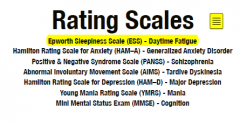
ESS = Epworth sleepiness scale (used to evaluate daytime fatigue)
|
|
|
What is a disadvantage to the various psychiatric rating scales?
|
While they can identify symptoms, they are unable to standardize symptom severity. Only the patient can tell you, making it subjective.
|
|
|
For psychiatric rating scales, high numbers generally mean negative outcomes. What rating scale is the exception?
|
Mini mental status exam (MMSE) (used to evaluate cognition)
|
|
|
What is the correlation between age and REM sleep?
|

Older = less REM sleep
|
|
|
What are the two subcategories of primary sleep disorders?
|
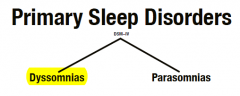
Dyssomnias and parasomnias
|
|
|
Which two classes if anti-depressants suppress REM sleep?
|
SSRIs and TCAs
|
|
|
What score on the ESS mental status exam would concern the MD for not sleeping enough/properly?
|
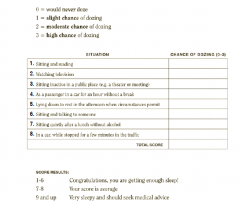
A score of 9 or higher = very sleepy
|
|
|
Approximate time needed to fall asleep (sleep latency) for zolpidem, eszopiclone and placebo
|
Zolpidem = 30 minutes
Eszopiclone = 30 minutes Placebo = 50 minutes |
|
|
What are the treatment goals for using medications to induce sleep?
|
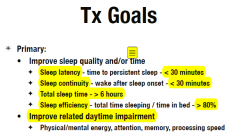
Sleep latency is under 30 minutes
Sleep continuity (waking up after sleep) is under 30 minutes Total sleep time is 6 hours or more Sleep efficiency (time asleep vs. time in bed) is 80% or more The basic goal is to "normalize" sleep |
|
|
Short term insomnia is often treated with what medications?
|
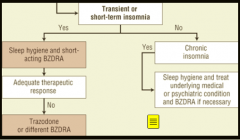
Trazodone or short-acting BZDRAs (Zolpidem, Eszopiclone, Zaleplon)
|
|
|
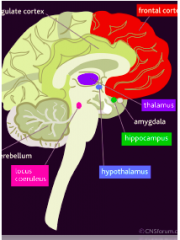
What tissue/center/area of the limbic system is involved in fear, aggression, jealousy and reward?
|
Amygdala
|
|
|
How would an animal missing the amygdala area of the brain behave?
|
Docile
Amygdala is involved in fear, aggression, etc. |
|
|
What can regulate the amygdala by recognizing and appraising the actual "threat"?
|
The sensory cortex
|
|
|
When a "threat" is perceived, which reacts first: the amygdala or the cortex?
|
Amygdala (Fast and inaccurate)
The cortex is slower but better evaluates the threat |
|
|
What happens to the following when under stress:
BP Blood sugar Immune function |
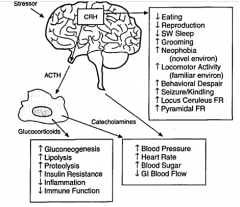
BP up
Blood sugar up Immune function down |
|
|
In the model for anxiety, what is different between the interactions of the amygdala and the cortex that results in constant stress?
|
Normally the cortex sends inhibitory signals to the limbic system/amygdala, blocking stress.
In anxiety, these inhibitory signals are reduced or not present at all. (Thus drugs will want to increase the inhibitory signals.) |
|
|
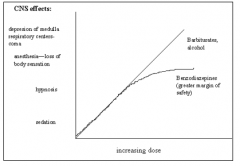
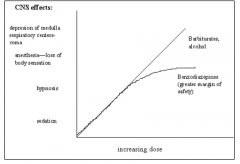
What is the major advantage of benzodiazepines over barbiturates?
|
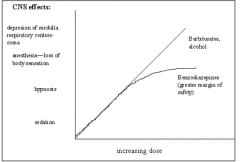
Benzos are less toxic (especially with alcohol)
Thus harder to overdose on with the above dose-response curve. |
|
|
How do doses and desired duration of action for benzodiazepines change when treating sleep vs. anxiety?
|
Anxiety- want low doses of long-acting benzos
Sleep - want higher doses of short-acting benzos |
|
|
GABA regulates what ion channel? What happens when an agonist binds?
|
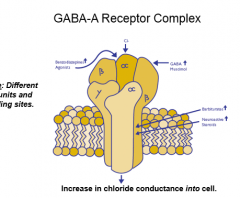
Chloride
When the channel is bound, the channel opens and allows chloride into the cell. This negative charge reduces excitability, hence why GABA promotes relaxation. |
|
|
On what subunits of the chloride ion channel do the following bind to:
GABA Benzodiazepines |
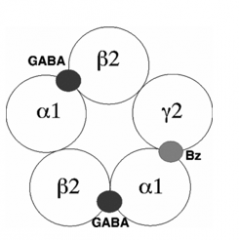
GABA to alpha and beta units
Benzodiazepines to alpha and gamma units |
|
|
What happens to the chloride ion channel when GABA and a benzodiazepine bind?
What happens to the channel when just a benzodiaepine binds? |
Binding of GABA + benzo increases the frequency of the channel opening, allowing more chloride in
A benzo binding without any GABA will not effect the channel much |
|
|
Flumazenil (Romazicon) reverses seizure protection of benzos through what mechanism?
|
Flumazenil is a competitive antagonist, thus can block the effects of benzos
This drug is given as an antidote to patients who try and OD on benzos |
|
|
DMCM is an inverse agaonist that binds at the benzo site and decreases receptor affinity for GABA. What physiologic effects would be produced?
|
Benzo/GABA = relaxation, thus inverse agonist = fear and anxiety
DMCM also increases the limbic system to raise HR and BP |
|
|
What sub-unit on the chloride ion channel is critical for benzos and GABA to exert their effects?
|
Alpha subunit
|
|
|
What alpha sub-type on the chloride ion channel exerts hyponotic properties? Which sub-type does anti-anxiety?
|
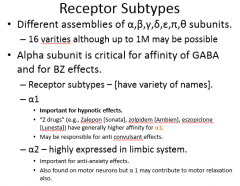
Alpha1 subtype does hyponotic effects (where zolpidem binds)
Alpha2 subtype does anti-anxiety effects (no selective drug yet) Benzos bind to both alpha 1 and 2 subtypes |
|
|
Gabapentin has a different MOA than benzos do. How does Gabapentin work?
|
While benzos bind to the alpha subunits of the chloride channel, Gabapentin increases GABA release and decreases excitatory NTs (by GABA-b).
|
|
|
How does barbiturates' MOA change from low concentrations to high concentrations?
|
At low concentrations, barbs bind to GABA-a mediated receptors and increases the mean channel opening time that is induced by GABA
At high concentrations, barbs keep the channel open, even in the absence of GABA This is why you can OD on barbs. You canot easily OD on benzos as they still require GABA for effect. |
|
|
Barbiturates and benzodiazepines both bind to the same ion channel. Why can barbiturates produce anesthesia while benzos cannot?
|
At high concentrations, barbs keep the channel open, even in the absence of GABA. Benzos need GABA for effect, which is why they plateau before reaching anesthesia
|
|
|
Endogenous peptides DBI and BCCE are inverse agonists to the NT GABA. What effects would they have?
|
Fear and anxiety
|
|
|
Some people drink to relieve anxiety, and to some extent it works. What is the mechanism of action for this?
|

Ethanol has a receptor site on GABA-a / chloride ion channel
|
|
|
What is buspirone? What is its MOA?
|
Buspirone is a 5HT1a partial agonist
5HT1a is an autoreceptor. Buspirone reduces the release rate of serotonin by reduced signaling. This inhibition is believed to reduce anxiety. (Agonist of 5HT1a = anti-anxiety) |
|
|
Is serotonin anxiogenic or anxiolytic?
|
It can be both anxiety causing and anxiety reducing depending on the region of the forebraiin involved and the receptor subtype that is stimulated
5HT2a is anxiogenic 5HT1a is anxiolytic |
|
|
A hypothetical 5HT2a antagonist would cause what symptoms?
|
5HT2a = anxiogenic, thus antagonizing it would produce relaxation
|
|
|
A knockout mouse missing the genes needed to make 5HT1a receptors will likely experience what?
|
Anxiety, as 5HT1a is anxiolytic
|
|
|
5HT transporters can have genetic variants. What version is likely to exhibit social anxiety?
|
S/L variant
|
|
|
The GABA system can affect many NTs. What effects would be produced when GABA acts on the following neurons:
5HT neuron DA neuron NA neuron |

5HT inhibition = anti-anxiety
Both NA and DA are excitatory and can produce sedation/anti-anxiety |
|
|
How would beta-blockers produce anti-anxiety effects?
|
Beta-blockers can block centrally acting NE, which is excitatory
|
|
|
CRF (corticotrophic releasing factor) regulates adrenal hormones. High amounts of CRF will likely produce what symptoms?
|
Anxiety/fear
CRF also increase central NE activity |
|
|
A CRF-1 antagonist will likely produce what symptoms?
|
Anti-anxiety
|
|
|
Does substance P increase or decrease with stress?
|
Increase
|
|
|
Oxytocin is involved in complex social behavior. What effects does it have?
|
Stimulates maternal behavior
Increases feelings of "intimacy" |
|
|
Vasopressin has what physiologic effects?
|
Pro-anxiety and may increase aggression (in males)
|
|
|
Someone with low levels of oxytocin may show what behavior?
|
Social anxiety, shyness
|
|
|
Oxytocin has what effect on 5HT release?
A 5HT2 antagonist will have what effect on oxytocin? |
Increases 5HT release
5HT2 antagonists block anti-anxiety effects of oxytocin |
|
|
TCAs and trazodone have what effect on sleep latency?
|
Decreased sleep latency
|
|
|
What is CBT?
|
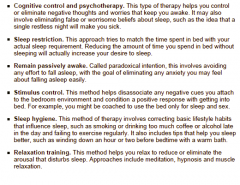
Cognitive behavioral therapy
Changing how you think and act will affect the way you feel. Can be used in insomnia |
|
|
What three benzodiazepines are FDA-approved for insomnia?
|
Flurazepam
Temazepam Triazolam |
|
|
Someone has used a "Z drug" (zolpidem, tec.) for 3 months and stopped without tapering. Besides insomnia, what is another patient disturbing side effect?
|
When the patient does fall asleep, REM will no longer be suppressed and they will have very vivid dreams
|
|
|
The majority of Rx drugs approved for sleep have what effects in common?
|
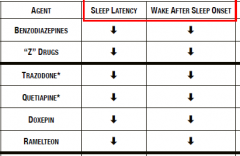
Decrease sleep latency and amount of awakenings during the night
|
|
|
Alcohol has what effects on sleep?
|
First-half of night: decreased sleep latency and REM, increased SWS
Second half: increased REM, fragmented sleep |
|
|
What are some side effects/adverse events when using the three benzodiazepines approved for sleep?
|
REM rebound risk when taken off
Tolerance to hypnotic effect with long term use Daytime hangover (long half-life CNS depression with higher doses |
|
|
Metabolism of benzos mainly go through CYP450 system. Which three are the exceptions that are glucuronidated?
|
Lorazepam
Oxazepam Temazepam |
|
|
Zolpidem and eszopiclone are metabolized by what enzymes? What are their half-lives?
|
CYP3A4
Zolpidem = 2.5 hours Eszopiclone = 6 hours |
|
|
Doxepin is a TCA (reuptake inhib. of NE/5HT) used in sleep. What is the dosing for sleep and what enzymes metabolize it?
|
3-6mg HS (much different from anti-depressant doses)
CYP2C19/2D6 Doxepin also is an H1 antagonist |
|
|
What is Trazodone's dosing for sleep and what enzyme metabolizes it?
|
50-150mg HS
CYP3A4 Trazodone also is an H1 and alpha1 antagonist |
|
|
What is Ramelteon's MOA? What enzyme metabolizes it?
|
Melatonin receptor agonist (MT1/2)
CYP1A2 (inhibited by fluvoxamine and induced by smoking) (Dose is 8mg 30 min before bed) |
|
|
Benzos suppress REM sleep and which brain wave?
|
Delta
Associated with deep sleep. |
|
|
What are some of Trazodone's important/serious adverse effects?
|
Priapism
Serotonin syndrome |
|
|
What may inhibit or induce Ramelteon's metabolism?
|
Anything that effects 1A2
Fluvoxamine inhibits 1A2 Smoking induces 1 A2 |
|
|
Ramelteon is rarely used as a sleep agent. Totally ignoring the previous statement, what is its dosing for sleep? What is its paradoxical side effect?
|
8mg given 30 minutes before bed
It can ironically cause insomnia as a side effect |
|
|
Melatonin is metabolized by what enzyme?
What is its half-life? |
1A2 (affected by smoking, fluvoxamine, tobacco)
MEHL = 0.5-1.0 hour |
|
|
Diphenhydramine should be used in caution when taking many drugs. Why?
|
2D6 substrate and 2D6 inhibitor
MEHL can be as long as 9 hours |
|
|
The herbal Valerian used for sleep should be avoided when taking what?
|
Alcohol or CNS depressants
This holds for many hypnotics |
|
|
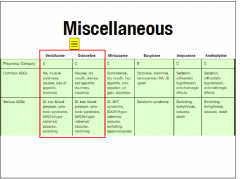
For insomnia,"", what is the max dosing for:
Flurazepam Triazolam Eszopiclone Zolpidem |
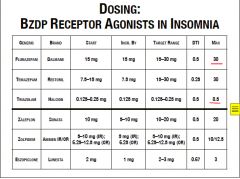
Flurazepam = 30mg
Triazolam = 0.5mg Eszopiclone = 3mg Zolpidem = 10mg IR or 12.5mg ER |
|
|
What is the target and max dose for the following in insomnia:
Quetiapine* Trazodone* Doxepin Valerian Diphenhydramine Melatonin (* = not FDA approved for insomnia) |
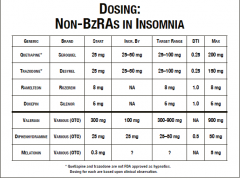
See chart
|
|
|
How would you start someone on zolpidem ideally?
|
Start low and slow as with everything
5mh QHS x 7 days If not responding, can increase dose to 10mg Use for shortest duration possible as hypnotic effect can wear off fast |
|
|
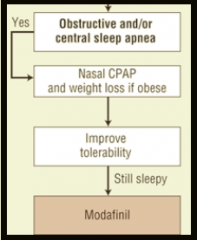
What is the last-line treatment for obstructive sleep apnea?
|
Modafinil
|
|
|
What is first-line therapy for obstructive sleep apnea?
|
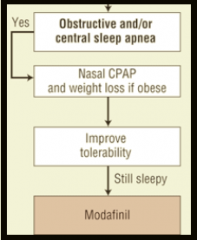
CPAP (continuous positive air pressure)
|
|
|
Modafinil in OSA:
MOA? Metabolism? Does it inhibit/induce an enzyme? Target dose? |
MOA is dopamine reuptake antagonist
Metabolized by 3A4 Unique drug as 2C19 inhibitor AND 1A2/3A4 inducer Target dose is 100-400mg daily F not determined |
|
|
Armodafinil shares what similarities with Modafinil? What is the major difference between the two/.
|
Shares pharmacology (dopamine reuptake inhibition), F not determned, 3A4 substrate, 2C19 inhibitor AND 1A2/3A4 inducer, adverse effects
The major difference is in the dosing. Modafinil's dosing is 100-400mg daily, while Armodafinil's is 150-250mg daily (narrower dose range)) |
|
|
For Modafinil and Armodafinil in OSA, how long does it take to reduce ESS scores by approximately 50%?
|
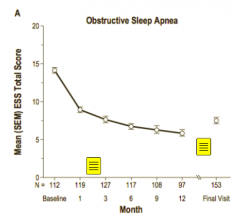
Several weeks to months. Takeaway is that it's not instantaneous
|
|
|
Shift work and jet lag are both circadian rhythm disorders. How do their pharmacological treatments differ?
|
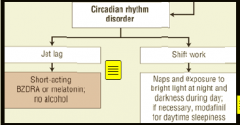
Modafinil can be used for day-time sleepiness in shift work
Short-acting benzodiazepines can be used for sleep induction in jet lag |
|
|
What are some of the diagnostic criteria in GAD?
|
Excessive worry/anxiety for at least 6 months
Anxiety is difficult to control Irritability, restlessness and sleep disturbances |
|
|
What part of the brain is involved with anxiety and fear, receives input from the thalamus and cortex, and reports to the hippocampus?
|
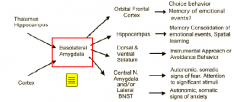
Amygdala
|
|
|
What three neurotransmitters are involved in GAD pathophysiology?
|
Norepinephrine, serotonin, and GABA
Serotonin and GABA are both inhibitory NTs and enhancing them would reduce anxiety |
|
|
What NTs and areas of the brain are involved in GAD? Which are in excess and which are impaired?
|

Overactive amygdala
Excessive norepinephrine from locus ceruleus Impaired serotonin quantities from dorsal raphe Impaired GABA function |
|
|
What substances would exacerbate GAD symptoms?
|
Caffeine
Stimulants Medications that enhance dopamine or norepinephrine |
|
|
What medications can be used as first-line monotherapy GAD treatment?
Which medication may seem counter-intuitive and why? |
SSRIs
SNRIs Benzodiazepines Buspirone (5HT1 partial agonist) SNRIs may seem counter-intuitive as excess norepinephrine from locus curleus is a cause of anxiety, and SNRIs and would be further enhancing this |
|
|
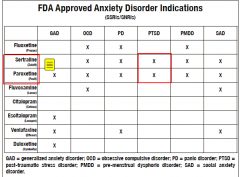
What four medications are FDA-approved for GAD?
WHich four are FDA-approved for OCD? |
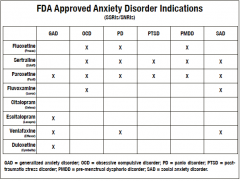
GAD: paroextine, escitalopram, venlafaxine, duloxetine
OCD: fluoxetine, sertraline, paroxetine, fluvoxamine |
|
|
What one wonder medication is FDA-approved for GAD, OCD, PD, PTSD, PMDD, and SAD?
|
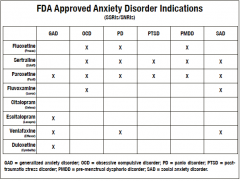
Paroxetine
|
|
|
What are first-line medications for GAD?
|
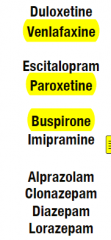
SNRIs venlafaxine and paroxetine
5HT1 partial agonist buspirone The four benzodiazepines used (lorazepam, diazepam, clonazepam, alprazolam) typically aren't first-line, but may be depending on situation |
|
|
How would you start a patient on paroxetine for GAD?
|
10mg QAM x5-7 days (starting low and going slow)
The drug takes ~5 half-lives to reach steady state, so tell patient results will not be immediate Increase by 5-10mg weekly to get to target dose of 20mg daily A benzo may be used initially with paroxetine to ease initial side effects - e.g. lorazepam 0.5-1mg TID PRN for two weeks |
|
|
How would you start a patient on venlafaxine for GAD?
|
37.5mg QAM x5-7 days
A benzo may be used initially with paroxetine to ease initial side effects - e.g. lorazepam 0.5-1mg TID PRN for two weeks Increase by 37.5mg weekly to target dose of 150mg daily |
|
|
Which medication generally takes longer to reach target doses when following recommended weekly increases in GAD: venlafaxine or paroxetine?
|
Venlafaxine (Start: 37.5mg - 37.5mg weekly increments - target dose of 150mg)
Paroxetine reaches target dose quicker (Start 10mg - 5-10mg weekly increments - target dose of 20mg) |
|
|
Why do SNRIs have varying symptoms depending upon the dose/concentration?
|
SNRIs have a stronger affinity for serotonergic sites. At low doses, they will act as SSRIs occupying serotonin sites.
At higher to therapeutic doses, the serotonergic sites fill up and then the drug expresses its SNRI properties |
|
|
How would you start a patient on buspirone for GAD?
|
Start 7.5mh BID x5-7 days
Increase by 7.5-15mg weekly to target dose of 30mg daily A benzo may be used initially with paroxetine to ease initial side effects - e.g. lorazepam 0.5-1mg TID PRN for two weeks |
|
|
Buspirone is a 5HT1 partial agonist. Why is it used in GAD?
|
Buspirone does not directly release serotonin (and has nothing to do with norepinephrine).
Buspirone actually acts upon the post-synaptic serotonin receptor itself, basically a mimic of serotonin |
|
|
How can buspirone be a agonist and antagonist of 5HT1a receptors?
|
It is a partial agonist, thus effect depends on local environment's serotonin concentration
In high concentrations of serotonin, buspirone competes for the 5HT1a receptor. Since it is a partial agonist with 40% of serotonin's affinity, it acts as an antagonist. In low serotonin concentrations, buspirone's 40% affinity is better than nothing, thus as an agonist. |
|
|
What SSRIs used in anxiety are considered low potency and thus need higher doses?
Which are higher potency and thus need lower doses? |
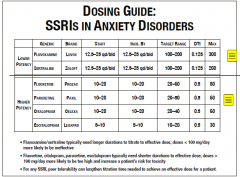
See chart
|
|
|
Sort the drugs below into 2D6 inhibitors, 1A2 inhibitors and 2C19 inhibitors:
Paroxetine Modafinil Fluoxetine Duloxetine Fluvoxamine Armodafinil Bupropion Diphenhydramine |
2D6 inhibitors:
Paroxetine Fluoxetine Duloxetine Bupropion Diphenhydramine 1A2 inhibitors: Duloxetine (again) Fluvoxamine 2C19 inhibitors: Modafinil Armodafinil |
|
|
If a patient needs a benzodiazepine for anxiety and is on fluvoxamine, bupropion, and fluoxetine (hypothetically of course), which would be ideal?
|
Since you have CYP inhibition everywhere (1A2, 2D6, 3A4) you want benzodiazepines that do not use CYP enzymes
Three benzos that are glucuronidated are lorazepam, oxazepam and temazepam The one ideally for anxiety is lorazepam. The other two are generally for insomnia. |
|
|
What rating scale is used to measure GAD?
|
HAM-A
A 28+ would be a high score |
|
|
After four weeks of SSRIs like sertraline, what % are HAM-A scores lowered by? (Generally)
What score is desired and indicative of remission of anxiety? |
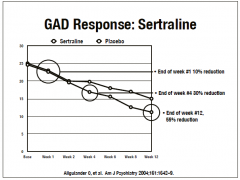
About 40-50%
A score of 7 or less is desired |
|
|
If monotherapy fails in the treatment of anxiety, what is the next step for most patients?
|
CBT (cognitive behavioral therapy)
|
|
|
Compared to SSRIs, how do benzos like alprazolam or diazepam affect HAM-A scores?
|
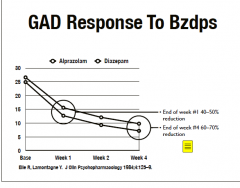
They lower scores to a greater extent (60-70%) and faster (<4 weeks)
Want HAM-A score of 7 or less (remission) Abuse potential is the downside as monotherapy |
|
|
For SNRIs in anxiety, what are some common side effects? What are some serious side effects?
|
Common:
GI upset Headache Insomnia Sexual dysfunction Serious: Suicidal idealization Hyponatremia (due to ADH) EPS side effects (extra-pyramidal; tremors, stiffness, restlessness for long periods) Serotonin syndrome |
|
|
A patient with hypertension and needs a medication for anxiety should avoid what class of drugs?
|
SNRIs like venlafaxine and duloxetine
Will raise BP with medium+ doses. This is not a contraindication however. |
|
|
What are common side effects of benzos upon initiation or dose increases?
|
Sedation
Cognitive impairments Ataxia Anterograde amnesia REM suppression Pregnancy category D (except for clonazepam) as chance for cleft palette and baby can have withdrawal |
|
|
If smoking causes 1A2 induction, why do nicotine patches not have this induction?
|
1A2 comes from aromatic hydrocarbons in tar, thus smoking and tobacco has 1A2 induction
There is no tar in patches |
|
|
What is the pathophysiology of OCD?
|

Overactivity between basal ganglia and hypothalamus
Excess dopamine from substantia nigra Not enough serotonin (to inhibit dopamine) from Raphe Ideal treatment is SSRIs GABA has no effect here thus benzos will not help |
|
|
What benzo would you use in OCD?
|

Trick question, GABA is not involved in OCD thus will have no effect. Buspirone also has little effect
SSRIs are ideal treatment to raise serotonin |
|
|
Which condition, OCD or GAD, would have a higher dose for paroxetine
|
OCD has higher doses
OCD has 50-80mg of paroxetine |
|
|
Citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline and clomipramine are all FDA-approved for what condition?
|
OCD
|
|
|
How would you start a patient on sertraline for OCD?
|
Assuming no poor tolerance:
25mg BID x 3 days, increase by 25mg to initial target dose of 75mg daily |
|
|
What scale measures OCD symptoms?
|
Y-BOCS (Yale Brown obsessive compulsive scale)
|
|
|
PTSD is diagnosed partly of a traumatic event re-experienced consistently in dreams, thoughts, perceptions. ALso includes hypervigilance and increased "arousal".
What drug would prevent the night-terrors? |
Prazosin
|
|
|
What is the pathophysiology of PTSD?
|
Increased amygdala activity (fear)
Low pre-frontal cortex activity Thalamus, hypothalamus, locus ceruleus involved in stress Low cortisol Smaller hippocampus |
|
|
What drugs are FDA-approved for PTSD?
|
Sertraline and paroxetine
Paroxetine is a 2D6 inhibitor |
|
|
Why can't you use benzos in PTSD or OCD?
|
GABA not part of pathophysiology
|