![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
196 Cards in this Set
- Front
- Back
|
Lynch syndrome (CEO - Colon, Endometrial, Ovarian) - the immunohistochemical staining tests for ________? note - colon = stomach & small bowel |
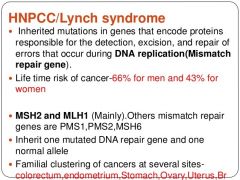
MLH1, MSH2 overexpression (TQ answer) PB says that the staining will show ABSENCE of these proteins Lynch syndrome = defects in mismatch repair - the insertion or deletion of additional nucleotides leads to micro satellite instability PRLG #1 PB #147 |
|
|
What is the 2nd most common cause of inherited ovarian cancer? |

The MCC = BRCA, duh 2nd MCC = Lynch Syndrome (CEO - ovarian cancer risk 4-24%) PRLG #1CO # 634 |
|
|
overexpression of PTEN |
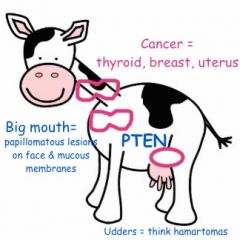
Cowden disease - AUT DOM Mutation in PTEN gene, phosphatase/tensin gene which is involved in cell cycle control Cancer: thyroid, breast & uterus Papillomas, hamartomas Risk of breast cancer 25-50% Risk of endometrial 5-10% PRLG #1 CO # 634 Hereditary Cancer syndromes |
|
|
TP53 mutations |

Li-Fraumeni syndrome soft tissue sarcomas, leukemia, adrenocortical cancer, breast cancer, brain cancer PRLG #1 CO # 634 Hereditary Cancer syndromes |
|

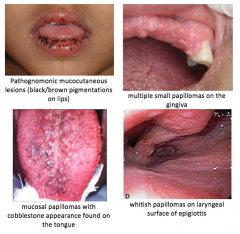
which syndrome? |
Peutz-Jeghers Syndrome Aut Dominant Mutations in serine/threonine kinase II (STK11) gene Presence of 2/3 criteria: 1) 2+ hamartomatous polyps in GI tract 2) mucocutaneous hyperpigmentation (mouth, lips, nose, eyes, genitalia, fingers) 3) family history of PJ syndrome Cancer: breast, ovarian, cervical, uterine, pancreas, lung, stomach, gastric, colon, ovarian sex cord tumors PRLG #1, CO #634 |
|
|
Which cancer syndrome DOES NOT include increased risk for breast cancer? |

Lynch syndrome think CEO - Colon (50-82%), Endometrial (25-60%), Ovarian cancer (4-24%) Well, there is very small risk of some types of breast cancer, but not compared to other syndromes PRLG #1 CO # 634 |
|

What syndrome? |
Cowden Syndrome Aut Dominant Mutation in PTEN gene, phosphatase/tensin gene which is involved in cell cycle control Cancer: thyroid, breast & uterus Papillomas, hamartomas Risk of breast cancer 25-50% Risk of endometrial 5-10% CO #634 |
|
|
45yo with diplopia, vertigo, dizziness found to have ovarian mass |
Paraneoplastic syndrome Systemic manifestations that are NOT caused by direct (local or metastatic) effects of tumor PRLG #3 |
|
|
what is low risk vs high risk gestational trophoblastic disease (GTD) ? |
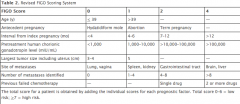
A factor that adds exactly 4 points is an interval from molar pregnancy to GTN diagnosis > 1 yr see graph PRLG #4 & PB #53 |
|
|
42yo with personal history of breast cancer at age 38, 1st degree relative with ovarian cancer - what is her risk of having BRCA mutation? |
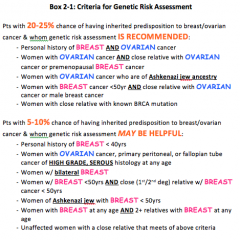
> 20% PRLG #2, PB #103 |
|
|
At what age should risk-reducing BSO be considered in women with BRCA1 or BRCA 2? |
age 40 or when childbearing is complete PB #103 |
|
|
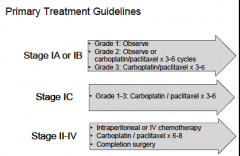
Explain when to use single-agent chemo vs multi-agent chemo for GTD |
single agent (either MTX or actinomycin) = stage I & low risk (score <7) stage 2/3 Multi-agent = stage 4 or high risk (score>7) stage 2/3 multi-agent = etoposide, MTX, actinomycin, cyclophosphamide + vincristine or MTX, actinomycin + vincristine PRLG #4, PB #53 |
|
|
POD #2, 65yo with SOB & tachycardia after radical vulvectomy, bilateral inguinal node dissection. Next step? |
CT- pulmonary angiography to r/o PE SN/SP both as high as 95% AND can detect other pulmonary abnormalities that could explain the clinical presentation IF pt has bad kidneys or allergy to contrast, then V/Q scan can be used PRLG #5 |
|
|
Topic: advance directives 76yo undergoes TAH, BSO, pelvic node dissection for endometrial cancer. POD #2 she suffers a stroke with neurologic deficit. Her 78yo husband is at bedside. After discussion, she states that she does not want to pursue additional treatment. Most appropriate action? |
assess her decision making competence (before signing DNR paperwork) PRLG #6 |
|
|
70yo BMI 40 undergoes ovarian cancer TAH/BSO + debulking, frozen path shows malignancy. What should you use for post-op DVT prophylaxis? |
SCDs + LMWH you need DUAL prophylaxis for VTE prevention in gyn cancer patients LMWH has several advantages over heparin (1) ease of use once a day (2) predictable pharmacodynamics (3) greater anti-factor Xa activity (4) less thrombin activity (5) reduced risk of thrombocytopenia PRLG #7 |
|
|
52yo h/o breast cancer on tamoxifen with postmenopausal bleeding. TVUS shows stripe 4mm Next step? |
Endometrial biopsy, duh. Any pt that has AUB while on tamoxifen needs EMB there is only risk for endometrial cancer in POST-menopausal women TVUS not useful b/c all women with tamoxifen will have thickened endometrium Both PRE- and POST- menopausal women will develop polyps with tamoxifen If you find polyp on sonohysterography -> OR (some polyps have been cancer, duh) If you find hyperplasia -> hysterectomy. You can restart tamoxifen for breast cancer prophylaxis after the hyst NOTE: there is a risk of uterine SARCOMA - RARE, 17 per 100,000 patient years versus none in placebo group PRLG # 8 CO #601 PB #126 (breast cancer) |
|
|
The most common side effect of tamoxifen is: |
hot flush PRLG #141 CO #601 |
|
|
Cervical cancer in pregnancy 38yo @ 16wks with 3cm SCC of cervix. After clinical staging, tumor confined to cervix. Pt wants definitive treatment of cancer, if that means terminating pregnancy. Next step? |
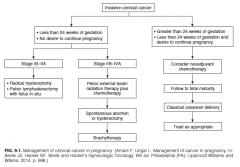
Stage IBI (tumor <4cm) Radical hysterectomy with fetus in situ and pelvic lymphadenectomy PRLG #9 |
|
|
most common GYN cancer in pregnancy |
Cervical PRLG #9 |
|
|
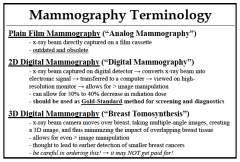
evaluation of palpable breast mass 52yo, annual visit, normal mammography 2 yrs ago. Note a firm, contender, fixed 1cm mass in R breast (upper outer quadrant) with no palpable axillary lymphadenopathy. Next step? A. Screening mammography of both breasts B. Ultrasound of right breast C. MRI of both breasts D. Diagnostic mammography of right breast |
D. Diagnostic mammography of R breast
- lack of tenderness is characteristic of cancer - Mammography vs ultrasound depends on age: <30 yrs without risk factors = ultrasound >30yrs = diagnostic mammography Get MRI in cases of: - silicone implants - breast-conserving surgery - known carcinoma for whom disease must be ruled out - an axillary mass and no identifiable primary tumor - extensive post-operative scarring - extremely dense breasts PRLG #10 |
|
|
Most common benign breast mass is ______ Most common malignant breast mass is _______ |
benign = fibroadenoma malignant = invasive DUCTAL carcinoma PRLG #10 |
|
|
Laparoscopic complications You are dissecting left sidewall for obturator lymph nodes during robotic case, morbidly obese pt, suddenly end-tidal CO2, SaO2 and BP have dropped. Heart murmur (mill-wheel) heard while Lungs clear. Most likely diagnosis? |
Gas embolism - intravascular injection of gas may follow direct needle or tracer placement into a vessel, or it may occur as a consequence of gas insufflation into abdominal organ. - can also occur later in procedure, i.e. when dissecting tissue causes venous bleeding with open sinuses, allowing for venous accumulation of CO2 - sxs of embolism = tachycardia, cardiac arrhythmias, hypotension, increased central venous pressure, alteration in heart tones (mill-wheel murmur), cyanosis, EKG shows right heart strain PRLG #11 |
|
|
Treatment of gas embolism during laparoscopy |
(1) release of pneumoperitoneum (2) steep trendelenburg with turn to left side (Durant position) (3) place on 100% fraction of inspired oxygen PRLG #11 |
|
Next step for bowel obstruction from recurrent ovarian cancer A. NG T B. percutaneous endoscopic gastrostomy tube C. endoscopic colorectal stent D. ileostomy E. cecostomy tube |
C. endoscopic colorectal stent PRLG #12 Berek's 6th ed pg 902 |
|
|
Breast surveillance in pts who are BRCA (+) 35yo healthy woman comes for annual. Her mother was BRCA2 (+) with ovarian cancer at age 50. How should she be screened for breast cancer? |
Annual breast MRI alternating with semi-annual mammography "semi-annual"?? every 6 months they need a screening test, alternating MRI and mammo PRLG #13 PB #122 breast cancer screening PB #103 BRCA |
|
|
62yo comes to office for post-op check 2 weeks s/p exp lap, debulking for stage IIIC serous ovarian cancer. Tachycardic, CT shows PE. What is the preferred initial tx of PE? |
LMWH Cochrane review comparing LMWH vs heparin showed that LMWH was a/w decreased risk of recurrent DVT, decreased mortality, and decreased risk of hemorrhage In case of renal insufficiency, heparin is the 1st line therapy PRLG # 14 |
|
|
HPV vaccination - given to what age group? - do you test for HPV prior to giving the vaccine for a sexually active 24yo? - if a 24yo had HPV testing with pap and it was positive, should she get the vaccine? - do you give vaccine to HIV (+)? - do you give vaccine to pregnant pt? |
1. Target age is 11-12 yrs for girls & boys 2. vaccine approved age 9 - 26yrs 3. DON'T do HPV testing until age 30 with pap 4. If 24yo is HPV(+), she can still get the vaccine 5. give to HIV pts 6. do NOT give during pregnancy PRLG # 15 CO # 641 |
|
|
28yo POD #4 s/p C/S with fever (103F), P 125, uterus tender, ext 1+ edema. Abdominal incision is erythematous & edematous, leaking cloudy serous discharge, EXQUISITELY tender. Preg complicated by T2DM needing insulin. Next step? |
Dx: necrotizing fasciitis Next step: (after antibiotics) DEBRIDEMENT of wound Clues "dishwater fluid" - due to serous fluid and lysed inflammatory cells being produced in an area of facial necrosis, myositis, myonecrosis PRLG #16 |
|
|
Results of mammogram for 47yo: fibrocystic changes and small mass that, on biopsy, is c/w ductal hyperplasia without atypia Next step? |
Observation PRLG # 17 (need to read the explanation, no PB or CO about this) |
|
|
Blood product selection after massive hemorrhage 70yo with stage III ovarian cancer undergoing surgery with bleeding, EBL 1500cc, tachycardic 140's, BP 96/64, Hg 6.8. Next step? |
pRBCs + FFP + platelets, balanced as 1:1:1 units transfused note - stay away from options that give lots of crystalloid fluids. "a study of pts undergoing extensive debunking, with anticipated large blood loss and RBC transfusion requirements, demonstrated that early FFP with RESTRICTIVE crystalloid resuscitation reduced overall pRBC units transfused" PRLG #18 |
|
|
Topic: human chorionic gonadotropin (hcg) 47yo referred to you for amenorrhea x 2 yrs and recurrent CIN 3 by colposcopy. Plan for LEEP, but hCG level of 10 on two separate occasions. FSH & LH levels are 75mIU/mL. Next step? |
prescribed OCPs and recheck hCG level Why? some peri-menopausal women will have (+) hCG at very low levels, due to FSH/LH cross-reaction and possibly benign low-level pituitary hcG production if pituitary in origin, the hCG titer can be suppressed with small dose of OCPs over 1 week period PRLG # 19 |
|
|
Most important test for pre-op cardiac clearance 70yo with 10cm complex pelvic mass, PMHx T2DM, HTN. Can walk 4 blocks before stops for leg cramps. No CP or SOB Choices: EKG, Echo, Exercise stress test, CXR |
EKG * She only has one risk factor - T2DM * The leg cramp = think peripheral vascular disease * when to get ECHO? for dyspnea of unknown origin or congestive heart failure (CHF) if test has not been performed in the past year * when to get STRESS TEST? active "cardiac conditions" - i.e. angina, recent MI, AV block, arrhythmias, aortic or mitral stenosis OR 2+ risk factors PRLG #20 |
|
|
What's the recommended antibiotic prophylaxis? 36yo healthy woman scheduled for total laparoscopic hysterectomy (TLH) |
cefazolin prlg #154 |
|
|
What's the recommended antibiotic prophylaxis? 38yo with BMI 45 and echocardiogram confirmed MVP scheduled for total vaginal hysterectomy |
cefazolin prlg #155 |
|
|
What's the recommended antibiotic prophylaxis? 43yo with endometrial cancer and 18wk size uterus scheduled for total abdominal hysterectomy. She has a PCN allergy not caused by immediate hypersensitivity |
cefazolin prlg #156 |
|
|
What's the recommended antibiotic prophylaxis? 38yo with suspected cystic teratoma undergoing laparoscopic oophorectomy |
no antibiotic prophylaxis prlg #157 |
|
|
SIRS vs sepsis - what's the dx? 45yo postop pt with RR 27, HR 100bpm, plasma glucose 150, T38.4C, normal physical exam |
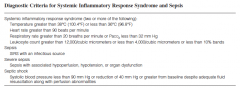
SIRS prlog # 151 |
|
|
SIRS vs sepsis - what's the dx? 65yo postop pt with BP 85/45 (after IVF boluses), T 37.0C, HR 115, RR 30, WBC 12.5 Hg 11 |
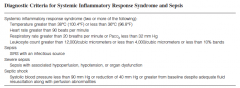
Septic shock prlg #152 |
|
|
SIRS vs sepsis - what's the dx? 34yo postop pt with RR 26, HR 92, T38.4, BP 130/80. Purulent drainage is present with erythema at wound site |
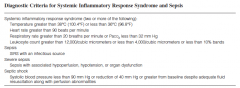
sepsis prlg #151 |
|
|
Which GTD subtype has risk of persistence after D&E of ~20% |
complete mole PRLG #144 |
|
|
Which GTD subtype - fetal vessels often are seen on hematoxylin & eosin stain |
Partial mole PRLG # 145 |
|
|
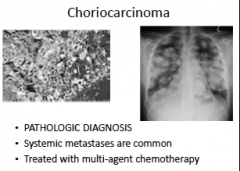
Which GTD subtype - systemic metastases occur frequently |
Gestational choriocarcinoma PRLG #146 |
|
|
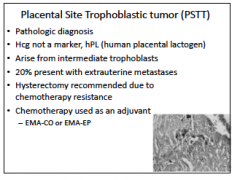
Which GTD subtype - histology characterized by proliferation of intermediate trophoblastic cells |
Placental-site trophoblastic tumor PRLG # 147 |
|
|
What type of hysterectomy for moderate sized fibroid uterus in multip? 57yo menopausal G3P3 with new-onset pelvic pressure & urinary frequency. No VB or discharge. Exam shows enlarged 11-wk size uterus, US shows 12cmx7cmx5cm with 5 cm fundal intramural leiomyoma and normal ovaries. No prior h/o fibroids or pelvic sxs. The preferred surgical treatment? |
vaginal hysterectomy (you want to avoid morcellation) PRLG #21 |
|
|
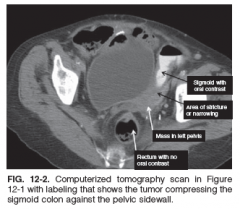
cytoreductive surgery - the best intraaoperative management 63yo with no co-morbidities, CC bloating +pelvic mass, BMI 33, Ca 125 2,400, U/S with ascites, paracentesis shows adenocarcinoma c/w primary ovarian tumor. Intra-op findings confirm ascites, mental caking, bilateral ovarian masses, 1cm mass to be invading sigmoid colon. |
complete resection with bowel resection PRLG #22 |
|
|
33yo, pap with atypical glandular cells, +HPV In addition to colposcopy, next step is: (a) repeat pap (b) EMB (c) ECC (d) ultrasound |
endoCERVICAL sampling (ECC) Note: endometrial biopsy is NOT needed if they are UNDER 35yrs, unless they have risk factors (AUB, chronic anovulation) PRLG # 23 |
|
|
How to calculate PPV: New ovarian cancer test, used with 503pts, 151 received diagnosis of cancer, 352 were benign. Of 223 predicted to have cancer by the test, 134 are confirmed to have cancer. Of 280 with negative test, 17 are found to have cancer. |
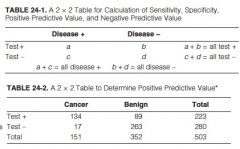
PPV = 60.1% (134 / 223) PRLG #24 |
|
|
Next step - stage IIIC uterine carcinosarcoma (a) whole abdominal radiation therapy (b) brachytherapy (c) adjuvant chemotherapy (d) tamoxifen |
Adjuvant chemotherapy PRLG # 25 |
|
|
Bone marrow toxicity from chemo: stage IIIC primary peritoneal cancer, with IV carboplatin/paclitaxel - found to have ANC 2000/mm, Hg 11, plts 70,000. She is afebrile Next step? |
delay chemo until recovery of her platelets Note: it's best to delay the next dose of chemo rather than decrease the dose. transfuse platelets if < 10,000 PRLG #26 |
|
|
What's the most common manifestation of bone marrow suppression from cytotoxic chemotherapy drugs? |
Neutropenia = ANC < 1,500 treatment: colony-stimulating factor (CSF) for febrile neutropenia |
|
|
the most likely primary site of pseudomyoma peritonei? |
appendix prlg #27 |
|
|
the best initial treatment for chemotherapy induced anemia? |
iron sucrose prlg # 28 |
|
|
what is the most likely primary site if the stain is (+) for CDX2, CK 20, CA 19-9 and negative for CK7, WT1, PAX8 and vimentin? |
gastrointestinal primary prlg #29 |
|
|
what is the most appropriate next step for pt who has gastric obstruction caused by carcinomatosis? |
percutaneous endoscopic gastrostomy tube placement topic: palliative care prlg #30 |
|
|
malignant ovarian germ cell tumor the best post-operative management is: |
observation prlg #31 |
|
|
the first step in management of hyperkalemia: |
calcium prlg #32 |
|
|
The NEXT STEP in management of uterine smooth muscle tumor of uncertain malignant potential |
Surveillance prlg #33 |
|
|
For prevention of chemotherapy-induced emesis, you can prescribe |
dexamethasone + selective type three 5-hydroxytryptamin (5HT-3) receptor antagonist prlg #34 |
|
|
What is the next step s/p TLH, BSO, staging for stage IA1 endometrial adenocarcinoma? |
3-6 month f/u with pelvic examination prlg #35 |
|
|
In addition to AGE, the prognostic factor common to most clinical prognostication models for breast cancer is |
tumor SIZE prlg #36 |
|
|
40yo women with (+)HPV - the most compelling reason to discuss the option of anal cytology is |
CD4 ct < 200cells/mm3 prlg #37 |
|
|
worried about ureteral injury during TLH, next step? |
transurethral cystoscopy #50 |
|
|
If you identify a ureteral injury intra-operatively, what is the next step? |
placement of ureteral stents #50 |
|
|
In contrast to endometrioid adenocarcinoma of the endometrium, the factor which uterine papillary serous carcinoma is a/w: |
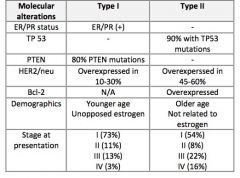
TP53 mutations Also: HER2/neu gene amplification #51 |
|
|
type I endometrial cancer (endometrioid type) is associated with what molecular profile? |
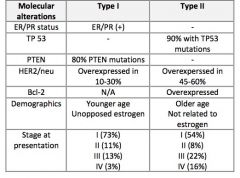
inactivation of the PTEN tumor suppressor gene mutations in beta-catenin and KRAS (Kirsten rat sarcoma viral oncogene) and defects in DNA mismatch repair resulting in micro-satellite instability #51 |
|
|
most likely side effect of aromatase inhibitor AI = anastrozole, exemestane, letrozole |
joint aches #52 |
|
|
FDA approved AIs for use in post-menopausalwomen with hormone receptor (+) breast cancer in 3 situations: |
POST-menopausal women (1) instead of tamoxifen for 5 years (2) Sequentially after 2-3 yrs of tamoxifen (3) Sequentially for 3-5 years after 5 yrs of tamoxifen use in women who remain disease free (extended adjuvant strategy) #52 |
|
|
best method to screen for colon cancer |
colonoscopy #53 |
|
|
Initial chemotherapy for ovarian cancer |
IV carboplatin and placlitaxel Note: carboplatin, not cisplatin (load up with carbs first!) Note: IP only for pts who are optimally debunked #54 |
|
|
pt who is 61yrs, BMI 62, menarche age 10, in utero exposure to DES. What is the greatest risk factor for developing breast cancer in this patient? What is the greatest risk factor in general? |
BMI is this pt's greatest risk Age is otherwise the greatest risk factor, RR 18 if older than 70yrs #55 |
|
|
Is IVF a risk factor for ovarian cancer? |
NO there is controversy but studies do not show link #56 |
|
|
34yo G0 undergoing IVF foranovulation (failed clomid) – she is obese, h/o 6yr OCP use, famhx of maternal aunt with gastric cancer & sister with melanoma. Her most significant RF for ovarian cancer |
nulligravidity Greastest RFs: age, endometriosis, famhx of ovarian cancer, BRCA mutation, early menarche, latemenopause, nulligravidity, infertility #56 |
|
|
Does pre-op bowel prep have advantages? |
NO change in outcomes it was hypothesized (and extrapolated from colorectal) that a pre-op bowel prep would decrease infectious post-op complications such as anastomotic leaks, surgical site infections andsepsis others presume it could improve visibility and bowel handling. But it does NOT #57 |
|
|
have hemorrhage from uterine artery pedicle - next step? |
ligate hypogastric artery (internal iliac) #58 |
|
|
FSS for 26yo G0 with fungating, friable 2cm lesion confined to cervix with no parametrial or vaginal involvement. Biopsy confirmed SCC |
stage IB1 vaginal trachelectomy + pelvic lymphadenectomy note: some investigators havesuggested that pre-op MRI should be mandatory – data has suggested that MRI isthe most reliable modality to assess extent of cervical involvement #59 |
|
|
Hemorrhage during hysterectomy, you have cell savor set up, have irrigated with 1L saline and placed fibrin sealant for bleeding, what bloodproducts to give? Allogenic, salvage product or autologous |
Allogenic products only (NOT salvage product, because you irrigated with saline & used hemostatic agent) Allogenic = homologous = donor Autologous = cell savor (salvage) #60 |
|
|
19yo with acute LLQ pain,u/s shows 18cm complex mass, take her back for laparotomy & mass issuspicious with solid components, frozen path of LSO shows malignant germ cell tumor - next steps? |
leave the right ovary (ONLY USO) but perform staging with washings, omentectomy, pelvic & para-aortic nodes,staging biopsies #61 |
|
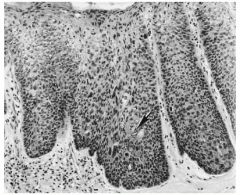
64yo with persistent vulvar itching, 2x2cm raised right labial lesion Biopsy sent Treatment? |
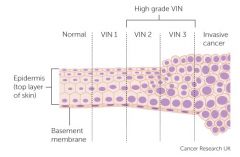
Dx: Vulvar intraepithelial neoplasia (VIN) 3 Tx: wide local excision #62 the picture on the front is from Melinda's: Carcinoma in situ of the vulva. There is full-thickness alteration in the architecture with elongation and distortion of the rete pegs. At arrow, there is intraepithelial pearl formation |
|
|
if the patient requires prolonged intubation, the best feeding system is parenteral (TPN) vs enteral |
enteral nutrition (OG or NG tube)
= lower risk of infections = maintains function & structural integrity of the gut and mucosal immunity, decreases oxidative stress, and down-regulates systemic immune response
#63 |
|
|
Path shows placental-site trophoblastic tumor from D&C; next step? |
total hysterectomy note: after surgery, then imaging to see if disease extensive - if stage II - IV, then EMACO (Etoposide, Methotrexate, Actinomycin, Cyclophosphamide, Vincristine/Oncovin) #64 |
|
|
ovarian cancer recurrence – the best surveillance duringremission is |
physical examination #65 |
|
|
30yo G0 undergoes surgery for complex ovarian mass; frozen path shows serous tumor of low malignant potential with noninvasive bladder implant; do you stage? Do you take both ovaries? |
No, just unilateral oophorectomy and removal of any gross disease #66 |
|
|
71yo, last pap 6 yrs ago was normal, new relationship for past 2 years, only gynecological problem is vaginal dryness with intercourse. What is the most appropriate cervical cancerscreening? |

no screening (stop age 65 if history of normal paps) #67 |
|
|
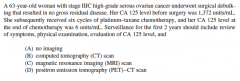
Screening for ovarian cancer 58yo, asymptomatic, 70yo cousin diagnosed with ovarian cancer, would like to be screened – best management? |
NO screening "counseling and review of ovarian cancer symptoms" Only screen high risk (BRCA & Lynch II) - start age 30-35 or 5-10 yrs before earliest age of diagnosis of ovarian cancer in family with Ca-125 + TVUS (if they do not have RR BSO) #68 |
|
|
C. Diff infection 62yo POD #7 s/p TAH, BSO,staging for ovarian cancer. Comes to office with diarrhea; T39.1C, WBC 22, Cr2.4 (up from 1 at discharge), stool study (+) for c diff next step? |
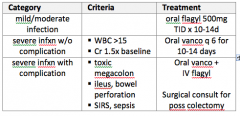
vancomycin alone this is a severe C diff infection based on the WBC >15 and Cr (>1.5x baseline) #69 |
|
|
Cervical cancer, colposcopy shows 2mm depth. Stage? Next step? |
Stage IAI cone biopsy for definitive tx of Stage IAI - extrafascial hysterectomy #70 |
|
|
How to correct injury to dome of bladder |
primary repair use synthetic absorbable suture, running fashion, either 1 or 2 layers #71 |
|
|
Post-treatment surveillance in cervical cancer – 54yo with stage 3B SCC s/p chemo 3 months ago with new leg pain & swelling, pelvic pain. In addition to pelvic exam, what’s the next step? |
PET-CT Scan While the organizations have different recommendations, this question makes a point that NCCN recommends PET-CT scan at 3-6 months after chemo #72 |
|
|
How to treat Heparin induced thrombocytopenia (HIT)? Plts: 210 - 85 - 55 in 5 days with pt on heparin post-op. |
stop unfractionated heparin and initiate argatroban
two tx rec of ACC - ARGATROBAN (direct thrombin inhibitor, ok if renal insufficiency) OR DANAPAROID (ok in pts with liver dysfunction or pregnant - does not cross placenta) #73 |
|
|
What is the mechanism of Type II HIT? |
immune-mediated disorder; IgG attacks heparin platelet factor 4 complex leads to platelet activation & micro particle release with subsequent arterial & venous thrombosis #73 |
|
|
Pathology shows low-grade serous ovarian cancer after laparoscopic USO. At time of surgery, there was a <1cm nodule in the omentum Next step? |
cytoreductive surgery low-grade serous cancer is relatively chemoresistant #74 |
|
|
activation in "mitogen activated protein kinase" pathway by mutations of BRAF or KRAF are seen in what type of cancer? |
Low-grade serous ovarian carcinoma #74 |
|
|
ovulation induction therapy is a risk factor for what type of ovarian cancer? |
low-grade serous ovarian cancer #74 |
|
|
Tx of recurrent platinum sensitive ovarian cancer |
carboplatin sensitive = interval >6 most resistant = < 6 months refractory = disease progresses during primary therapy #75 |
|
|
In performing TAH pt hassevere endometriosis; beforeremoving adnexa, what’s your first step? |
identify ureter # 76 |
|
|
What's the incidence of ureteral injury in gynecological procedures? |
0.5 - 2% only 1/3 are identified at time of surgery #76 |
|
|
what is the most common site of ureteral injury during routine hysterectomy with BSO? most common site during laparoscopic surgery for endometriosis? most common site during vaginal surgery? |
with BSO = at the level of the pelvic brim when attempting to ligate the ovarian vessels Laparoscopy = level of uterosacral ligaments Vaginal = near the trigone - can not only the ureter but also the bladder #76 |
|
|
Describe the path of the ureter |
The ureter enters the pelvis at the level of the bifurcation of the common iliac artery and runs under the IP ligament. Retroperitoneal location at this point is essential before ligating the ovarian vessels and can be accomplished by following the external iliac artery cephalic from the pelvis and exposing the medial broad ligament. The ureter then runs retroperitoneal along the pelvic side wall before it passes under the uterine artery ("water under then bridge") and enters the paracervical tunnel. At this level, the average distance from the ureter to the cervical edge is 2.3cm. (decreased in obese and <0.5cm in 12% of pts) #76 |
|
|
does pre-operative stents decrease ureteral injury |
NO they make it easier to identify ureters, but research has shown that it doesn't decrease incidence of injury #76 |
|
|
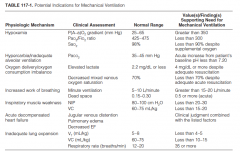
Tx of ARDS (s/p TAH, staging for ovarian cancer) SaO2 75%, 4L oxygen, CXR shows bilateral patchy infiltrates & no evidence of pleural effusions, negative spiral CT scan |
mechanical ventilation #77 |
|
|
Next step for PMB (BMI 50, TVUS shows stripe of 9mm) |
endometrial biopsy, duh #78 |
|
|
Is irritable bowel syndrome (IBS) a risk factor for colon cancer? |
NO but Inflammatory bowel disease (IBD), Crohn's disease and ulcerative colitis are RFs #79 |
|
|
What is the "highest risk" factor for colon cancer |
Family history / inheritable susceptibility Lynch Syndrome = the most common syndrome a/w colon cancer Familial adenomatous polyposis #79 |
|
|
endometriosis is a risk factor for which types of ovarian cancer? |
clear cell & endometrioid types #80 |
|
|
What is the important molecular change seen with clear cell carcinoma of the ovary? |
loss of the ARID1A gene loss of BAF250a, encoded by ARID1A gene #80 |
|
|
The agent responsible to the most common blood transfusion-associated infections in the US is |
gram (+) bacteria - typically staphylococcus (from the skin) highest risk occurs with bacteria-contaminated platelet transfusion because they are stored differently #81 |
|
|
What is the risk for HIV, Hep B & C to be transmitted in a blood transfusion? |
#1 Hep B 1 / 277,000 #2 Hep C 1 / 1.9 million #3 HIV 1 / 2.1 million #81 |
|
|
Next step 23yo pap with HGSIL, Colp CIN 2 |
colposcopy & cytology in 6 months if <25 for CIN 2 = repeat colp & pap in 6 month intervals for 12 months if CIN 2 persists > 2 yrs, CIN 3, or inadequate colposcopy then LEEP **HPV testing is not needed at age 23 #82 |
|
|
What is the most commonly diagnosed STD in the US?
|
HPV #82 |
|
|
Treatment of hot flashes in 40yo s/pTAH, BSO, staging for stage IA, grade II endometrioid adenocarcinoma |
estrogen there is a long explanation about the controversy, but the bottomline is that it's the most effective for vasomotor sxs and there aren't any cases of recurrent endometrial cancer in women given HRT #83 |
|
|
The prognostic factor thatmost consistently predicts poor outcome after pelvic exenteration for cervicalcancer that recurred after pelvic radiation |
time to recurrence also poor prog factor = (+) para-aortic nodes (NOT pelvic lymph nodes) #84 |
|
|
how to monitor for recurrence of endometrial cancer at the vaginal cuff? |
physical exam NOT pap smear! #85 |
|
|
What is the prognosis for stage I endometrial cancer? |
>95% 5 yr survival #85 |
|
|
Cervical cancer screening for women > 30 |
neg cytology & neg HPV = q 5 yrs neg cytology (+) HPV = repeat cytology & HPV testing in 1 yr or reflex testing for HPV 16/18 if reflex testing (+) 16 or 18 = colposcopy if neg 16/18 = contest in 12 months #86 |
|
|
Sepsis – 60yo PMHx ovariancancer, DM, HTN, pOD #7 s/p TAH BSO staging with T38.8, P130, BP 90/40, UOP15/hr, hypoactive bowel sounds, purulent drainage from vagina, WBC 17.5; nextstep? |
IV fluids and broad spectrum antibiotics #87 |
|
|
most effective method of risk reduction for 42yo with BRCA1 mutation, completed childbearing, smokes 1/2 PPD |
BSO #88 |
|
|
What are options to decrease risk of ovarian cancer in women who carry BRCA but are not ready to have ovaries removed? |
frequent surveillance with TVUS, physical exam, Ca-125 OCPs #88 |
|
|
28yo G0 with CIN3 undergoesLEEP, negative margins but AIS extending to deep margin of the specimen. Nextstep? |
re-excision via cervical conization
if she were done with childbearing, then next step is radical hyst for AIS FSS option = repeat cone for negative margins. Cold knife cone procedure better than LEEP if negative margins, then pap + HPV testing + colp with ECC in 6 months for surveillance #89 |
|
|
During abdominal hysterectomy, you see large amount of clear fluid filling up in the abdomen after identifying the IP ligament; next step? |
IV indigo carmine or methylene blue is the best way to investigate integrity of the ureters intra-operatively #90 |
|
|
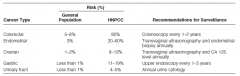
45yo with endometrial cancer Family history of 1st degree relatives with breast, lung, colon cancer What syndrome? What genetic testing? |
Lynch II Syndrome, (HNPCC) "CEO" testing = immunohistochemistry - MLH1, MSH2, MSH6, PMS2 breast cancer was a distractor? #1 |
|
|
54yo comes to you after finding out she has Lynch Syndrome. Both her father & brother had colon cancer What do you recommend for her - i.e. RR surgery or screening? |
most effective choice is Hysterectomy with BSO (esp since she is post-menopausal) #91 |
|
|
73yo with vulvar pruritus & burning exam: red, velvety, inflamed biopsy: large cells with prominent nuclei & coarse chromatin Dx? Next step? |
Dx: Paget disease next step: screening for cervical, breast, colon cancer with pap, mammography, colonoscopy - (15-30% have co-malignancy) #92 |
|
|
What is the stage of cervical cancer: on exam see 5cm friable mass, extends to upper 1/3 vagina all other workup negative, except CT scan shows enlarged nodes |
Stage IIA2 #93 |
|
|
Stage IB papillary serous uterine cancer next step after surgery? What is the recurrence rate? |
Papillary serous = Type II endometrial cancer Chemotherapy, specifically carboplatin - paclitaxel then brachytherapy recurrence rate = 60% #94 |
|
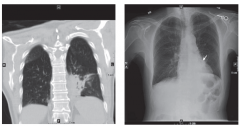
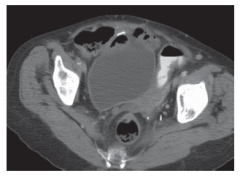
POD #3 after LAVH pt with SOB Pt with morbid obesity, poor dentition, HTN, DM, HIT See CT scan picture Dx? Tx? |
Dx: Aspiration Pneumonia Tx: Piperacillin with Tazobactam Imaging shows infiltrates in dependent regions of the lungs (posterior segments of the upper & superior segments of the lower lobes) #95 |
|
|
35yo with 1cm breast mass, needle biopsy shows Invasive ductal carcinoma treatment? |
lumpectomy with sentinel lymph node biopsy Distractor: sentinel node, not axillary node dissection! #96 |
|
|
Lumpectomy vs mastectomy - What factors preclude a patient from breast-conserving treatment (lumpectomy)? |
#96 |
|
|
Cervical cancer: 40yo, G2P2 4.5cm fungating cervical mass with extension to left pelvic side wall Stage? Next step? |
Stage IIIB Tx: chemo + radiation (cisplatin most common) She is NOT a candidate for surgery - surgery alone would not be curative chemo + radiation should be recommended b/c it improves progression-free survival and overall survival compared to radiation alone #97 |
|
|
40yo undergoes lumpectomy, axillary node dissection: Diagnosed with stage I breast cancer (1cm in size) and negative nodes. +ER/+PR, but considered low risk. Next step? |
Radiation therapy then tamoxifen note: Aromatase inhibitors only shown benefit in postmenopausal #98 |
|
|
74yo with vulvar cancer undergoing hemivulvectomy & lymphadenectomy. What is the greatest risk factor for long-term post-operative sexual dysfunction? options: age, extent of surgery, lymphadenectomy, HTN |
patient age studies show that increasing age is negatively associated with sexual function the extent of surgery and type of vulvectomy did NOT correlate with degree of sexual dysfunction in a study Other factors that increase risk for sexual dysfunction: age, depression, worsening performance status, pre-operative hypoactive sexual dysfunction #99 |
|
|
Basal cell carcinoma of labium minor (1cm in size, 1.5cm from urethral meatus) Next step? |
Wide local excision (margin 4-5mm) do NOT need nodes - considered small (cut-off ~2cm) #100 |
|
|
What is the best screening option to assess for lymph node involvement for cervical cancer |
PET-CT scan - high sensitivity in detecting retroperitoneal nodal involvement MRI is most sensitive to determine tumor extensive to lower uterine segment or vagina and to provide objective measure of tumor size so, depending on what they ask for, this could be tricky (ugh) #101 |
|
|
31yo, received HPV vaccination, had normal pap. What is the preferred next screening test? |
cytology + HPV cotesting q 5 years Why not cytology alone q 3 yrs? the increased sensitivity of contesting compared with cytology alone achieves slightly lower cancer rates with less screening and few colposcopy. #102 |
|
|
65yo with malignant ascites, family history of father with colon cancer at age 70. Most likely cancer? |
ovarian malignant ascites in pts with ovarian cancer is thought to be attributed to lymphatic obstruction, increased vascular permeability, release of inflammatory cytokines and direct increase of fluid production by cancer cells in peritoneal cavity #103 |
|
|
Endometriosis associated with what type of cancer? |
clear cell carcinoma # 104 |
|
|
You are going to operate on a patient with HIV, obesity, asthma & 30 pack yr smoking history with emphysema the factor most likely to cause a reduction in functional residual capacity (FRC) is? |
obesity FRC = volume of gas remaining in the lungs at passive end expiration things that decrease FRC = mechanical factors - pregnancy, obesity, pleural effusion, posture # 105 |
|
|
49yo undergoes TAH, BSO, nodes for stage IB1 cervical cancer. Final path shows small cell cancer margins negative Next step? |
Chemotherapy, even for early stage disease (stage IB) because metastasis is common with small cell neuroendocrine tumors cisplatin - etoposide regimen preferred #106 |
|
|
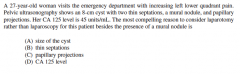
papillary projections why? with laparoscopy you worry about spilling contents that may be malignant during removal. Worried about spillage, you don't want to do something with papillary projections laparoscopically #107 |
|
|
What are the cut-off levels for Ca-125 to refer removal of adnexal mass to gyn onc? |
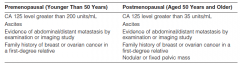
Pre-menopause >200 Post > 35 #107 |
|
|
32yo with BMI 51 with grade I endometrial cancer. No evidence of mets on MRI Wants children Trying to lose weight Next step? |
IUD IUD was better choice than high dose progestin therapy b/c oral progestin at high dose will hinder this patient's weight loss efforts #108 |
|
|
Needlestick injury, patient with HIV on HAART, last titer 800 RNA copies/mL What drugs for post-exposure prophylaxis? |
Emtricitabine, Tenofovir, Raltegravir #109 |
|
|
What is the risk of HIV transmission from needle-stick of HIV (+) pt? with Hep B (+) pt? |
HIV: 0.3% after percutaneous exposure to HIV infected blood 2 - 60% after exposure to Hep B infected blood #109 |
|
|
What is the most appropriate, evidence-based treatment recommendation for contraception while following beta-hCG levels for GTD? |
OCPs #110 |
|
|
42yo with recurrent stage IIB SCC of cervix. Undergoing 3rd course of chemo. On exam skin & sclera are jaundiced, abdomen distended with fluid wave, abnormal LFTs, imaging shows extensive liver mets, pulmonary nodules. Admitted for pain control, requiring large doses of IV analgesics Next step? |
Palliative care #111 |
|
|
What's the best way to fix an abdominal hernia from laparotomy for large fibroid uterus? |
Laparoscopic repair with mesh #112 |
|
What are the recommendations for observation of stage IIIC ovarian cancer? |
No imaging! Surveillance is pelvic exam + Ca125 level Imaging only when indicated (symptomatic) #113 |
|
|
Stage IIB cervical cancer, s/p radiation therapy and chemo. c/o hematuria 5 yrs after treatment. Most likely cause? |
radiation hemorrhagic cystitis (5.8% in 5 yrs, 7.4% in 10 yrs) is more likely than recurrence (cure rate 50%) Perform cystoscopy to confirm diagnosis of hemorrhagic cystitis #114 |
|
|
68yo s/p optimal debulking surgery for ovarian cancer. You are considering placing an IP catheter for adjuvant chemo. This patient's most significant risk factor for catheter-related complications is: |
segmental rectosigmoid resection Note: the primary reason for dc'd IP chemo is complications related to the catheter - infection is the most common left colon- rectosigmoid resection is the procedure that has the highest risk for infection/ complications #115 #115 |
|
|
Most important part of surveillance of stage IB grade 3 endometrial cancer is
|
history & physical examination SGO guidelines specifically address the lack of evidence behind pap tests, CA-125, CXR, CT scanning in surveillance of survivors - these tests only increase cost & anxiety without improving detection # 116 |
|
|
65yo POD #3 s/p bowel resection, anastomosis for SBO. She had index procedure for endometrial cancer 2 yrs ago. SICU page re: RR 36, P 130, BP 90/55. SaO2 89% on 2L NC. Next step for respiratory distress? |
Intubation In the post-op period, most pts can be managed with O2 nasal cannula. Indications for intubation: combination of a failure to adequately oxygenate, ventilate, or meet metabolic demands of a physiologically stressed patient SaO2 <90% or PaO2/FiO2 less than 200-300mgHg s/sxs to dx respiratory distress: tachycardia, arrhythmia, hypotension, tachypnea, use of accessory muscles, diaphoresis, cyanosis #117 |
|
|
After post-op patient is intubated what settings to know? |
FiO2 100% (1.0) - then titrated downward to maintain SpO2 at 92-94% Tidal volume (TV) 8-10 mL/kg RR 12-15 breaths/minute (target pH, not PaCO2) if ARDS - then TV 4 - 6 ml/kg to prevent barotrauma, satisfy "air hunger" whether to use volume- or pressure- controlled ventilation is generally at the discretion of the clinician (SIMV vs VC/AC, PC/AC) #117 |
|
|
57yo with vulvar cancer. 2.5cm raised lesion, biopsy shows grade 2 SCC with 2mm depth. On exam, palpable inguinofemoral lymph node. The factor that determines that the patient is NOT a candidate for sentinel node dissection is: |
palpable groin node "the detection rate and sensitivity of sentinel node mapping is decreased in pts with clinically palpable nodes - the lymphatic system is obstructed by tumor cells that prevent radioactive isotope and dye from correctly identifying the sentinel node." #118 |
|
|
57yo with vulvar cancer; 2.5cm raised lesion, biopsy shows grade 2 SCC with 2mm depth. On exam, palpable inguinofemoral lymph node. Does she need lymphadenopathy? |
Yes, depth > 1 mm needs lymphadenectomy. Don't do sentinel node mapping when nodes are palpable, however #118 |
|
|
What are the ideal patients for sentinel lymph node mapping in treatment of vulvar cancer? |
Lesions < 4cm squamous etiology exam without palpable lymph nodes #118 |
|
|
Treatment of vulvar cancer: |
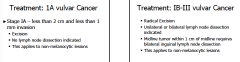
1A: <2cm in size, <1mm in depth 1A -> excision withOUT lymphadenectomy IB - III = radical excision, with lymphadenectomy if within 1cm of midline, need bilateral lymphadenectomy #118 (but this is from perinatal resources) |
|
|
Tx of DCIS after excision + lymphadenectomy Biopsy = 3cm in size, neg ER/PR, closest margin 1mm She does not want surgery |
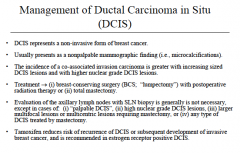
Next step: Radiation Observation if surgical margin <3mm If she wanted surgery, could do simple mastectomy #119 |
|
|
s/p TAH for endometrial cancer, BMI62. POD #2 difficulty walking - foot is limp & unable to dorsiflex. What nerve? What could have prevented this injury? |
Nerve: Peroneal nerve Cause: prolonged malposition To prevent: appropriate positioning of legs in stirrups #120 |
|
|
Sharp, burning pain over suprapubic area, labia, thigh What nerve? The common cause of this injury? next steps? |
Ilioinguinal / iliohypogastric (L1-L2) occurs during transverse abdominal incision or tracer site insertion Tx: self- limiting if persistent, then pain can be treated with gabapentin severe pain - local nerve blocks #120 |
|
|
What nerve is commonly injured during SSLS? S/Sxs? Tx: |
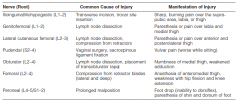
Pudendal nerve Typically entrapment injury Sxs: pain Tx: release of the entrapped nerve #120 |
|
|
What is the most common compression injury from retractors during hysterectomies? sxs? |
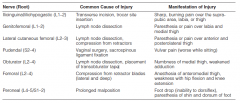
femoral nerve (L2-L4) sxs: sensory change of anteromedial thigh, motor weakness with hip flexion & knee extension #120 |
|
|
Best breast cancer screening option for healthy 45yo woman with dense breasts Choices: Ultrasound MRI Digital mammography Film mammography |
digital mammography Note: dense breast are a/w a modestly increased risk of breast cancer #121 CO #593 |
|
|
Next step for intra-operative rupture of malignant ovarian cyst Path: high grade serous carcinoma grade 3 All other specimens including washings, are negative |
IV chemo because of high-grade histology Note: chemo is needed not only because of the rupture, but also b/c of the high grade #122 |
|
|
What is the appropriate post-op treatment for patient taking methadone, to prevent withdrawal symptoms? Undergoing TAH for fibroid uterus |
continue methadone Note: in many patients, a fetanyl patch will be effective to treat persistent mod-severe chronic pain. The patch can be applied for up to 72hours for continuous pain relief. Fentanyl was not the right answer b/c it won't prevent withdrawal #123 |
|
|
The strongest scientific evidence for the benefit of acupuncture in cancer patients is for: |
chemo-induced nausea & vomiting acupuncture's effect on pain is not well defined #124 |
|
|
Tx of CIN I in pregnancy |
reassess postpartum #125 |
|
|
Tx of CIN 2/3 in pregnancy |
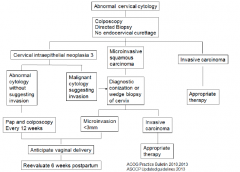
pap & colposcopy every 12 weeks deferral to postpartum is alternative option (not preferred) #125 |
|
|
42yo undergoes diagnostic laparoscopy for pelvic pain Findings: 3cm right ovarian tumor, carcinomatosis with diffuse mental involvement and ascites. Frozen path reveals serous carcinoma The surgery-related complication this patient is most at risk for: |
port-site metastasis Incidence 0.24% #126 |
|
|
Post-op DVT prophylaxis for 68yo s/p TAH, BSO, debulking for high grade serous ovarian adenocarcinom |
LMWH for 4 weeks postoperatively #127 |
|
|
42yo s/p surgical repair of bowel perforation attributed to bevacizumab therapy. RR 24, BP 90/60, PaO2 70mmHg, FiO2 60%, SaO2 95% Next step? |
Continue intubation #128 |
|
|
85yo with serous ovarian cancer, diagnosed after thoracentesis that removed 1L of ascites h/o CAD, MI, CHF, wheelchair bound. Work-up finds PE, massive ascites, mental caking, 8cm complex pelvic mass best recommendations for management of her cancer is: |
IV chemo (NOT primary cytoreductive surgery) #129 |
|
|
54yo with 6cm ovarian mass, Ca-125 45. Undergoes laparoscopic LSO, washings. Frozen reveals grade 2 serous adenocarcinoma of ovary Next step? |
hysterectomy, contralateral SO, omentectomy, lymphadenectomy, washings, peritoneal biopsies #130 |
|
|
What intervention has been shown most beneficial in decreasing post-operative ileum? |
early post-operative feeing #131 |
|
|
What is the Dx & Tx:
38yo h/o stage IIB cervical cancer. Now 3 yrs s/p chemoradiation c/o abdominal pain, N/V. CT scan shows inflammation around the terminal ileum and proximal colon |
Dx: radiation enteritis Tx: Bowel rest, IVF, correction of electrolytes, antiemetics, analgesics #132 |
|
|
Okay for HRT in BRCA pts? 37yo BRCA1 s/p BSO & bilateral mastectomy. C/o hot flashes, vaginal dryness. The BEST therapy for her? |
hormone therapy **if uterus is still in place, then progestin therapy should be included to decrease risk of developing endometrial cancer #133 |
|
|
The greatest risk factor for lymphedema? 55yo with stage I3C1 endometrial cancer treated with laparoscopic radical hysterectomy, BSO, pelvic & para-aortic lymphadenectomy. Then completed chemo and radiation. BMI 32. |
Answer: multimodality therapy Lymphedema in GYN depends on type of cancer, extent of lymphadenectomy & location of nodes being removed. Studies show age & BMI are NOT independent risk factors **Vulvar cancer with highest incidence **Lymphadenectomy alone increases risk ** but addition of radiation to lymphadenectomy increases risk more! (duh) #134 |
|
|
Treatment of Stage 4B cervical cancer 31yo with friable mass, extension to pelvic sidewalls, palpable supraclavicular lymph node, multiple lung lesions on imaging. |
chemotherapy alone Stage 4B cervical cancer is NOT amenable to surgery or radiation - is a/w poor prognosis, and is rarely curable Primary tx consists of systemic chemotherapy with the goal to prolong survival and improve quality of life Combination chemo - cisplatin + (paclitaxel, topotecan or gemcitabine) #135 |
|
|
26yo s/p complete mole beta-hCG 3,000 - 7000 - 13000 (over 3 weeks) Exam: benign CXR: normal U/S: abnormal soft tissue hyper vascular lesion in the fundus, stripe 2cm Next step: |
single-agent chemo She has GTD (beta-hCG increase more than 10% over 2 weeks) and low risk (memorize the chart!) #136 |
|
|
The step to reduce risk of wound infection |
use of chlorhexidine-alcohol surgical prep **wound infxns comparable whether movie vs scalpel used for incision **Chlorhexidine is the most effective skin cleasing agent and shown to be superior to povidone-iodine in reducing skin infections *shaving skin can increase risk of skin infection, but clipping hair just prior to incision does NOT increase risk *placing drains to reduce risk of infection is controversial #137 |
|
|
34yo wants FSS for ovarian cancer Path: endometrioid ovarian cancer, grade I no evidence of extra ovarian disease |
FSS = preserve uterus & contralateral ovary So - USO, washings, omentectomy, pelvic & para-aortic nodes *** should also perform endometrial biopsy to check for risk of synchronous primary cancer in this age group, most common types of ovarian cancer are germ cell tumors or borderline ovarian tumors #138 |
|
|
Acute Kidney injury (AKI) - next step? 48yo POD #2 s/p TAH for fibroids. Hypotension during procedure - given salvaged rbcs, crystalloid, vasopressors. Cystoscopy at end of procedure normal. BP 120/70, P 90, R 18, UOP low but increased 1 mL per kg/ hr overnight. Hg 9.8 and Cr 2.3 (1 at baseline) |
maintenance IVF AKI is pre-renal (hypotension) - vs postrenal (ureteral injury) because cystoscopy was normal "management for post-op AKI not due to surgical urinary tract injury is mainly supportive and should be directed at making sure the volume is replaced until natural recovery occurs. Sepsis should be rule out. Hypotension and volume overload should be avoided because both affect perfusion)" crystalloid fluids preferable #139 |
|
|
65yo G3P3 with grade 3 endometrial cancer. BMI 32 What's the procedure that she needs & the best surgical route (fewest complications)? |
TLH, BSO with pelvic lymph node dissection (she needs lymphadenectomy - grade 3 - so vaginal route eliminated) laparoscopic better than open (duh) #140 |
|
|
The most common adverse effect of tamoxifen |
hot flushes #141 |
|
|
Next step in management: 27yo with adenocarcinoma in-situ (AIS) on colposcopy, underwent conization, showed invasive adenocarcinoma with diameter 5mm and depth of 2mm, negative margins, no LVSI |
Final diagnosis = stage IAI Next step: routine cervical cancer surveillance examinations (does not need node dissection, hysterectomy or re-excision) #142 |
|
|
9yo has a complex adnexal mass and precocious puberty. The tumor marker most likely to assist in your pre-operative evaluation is |
inhibin B level (Granulosa cell tumor) #143 |
|
|
Which GTD - Risk of persistence after D&C is ~ 20% |
complete mole #144 |
|
|
Which GTD - Fetal vessels often are seen on hematoxylin and eosin stain |
partial mole #145 |
|
|
Which GTD - systemic mets occur frequently |
gestational choriocarcinoma #146 |
|
|
Which GTD - Histology characterized by proliferation of intermediate trophoblastic cells |
Placental-site trophoblastic tumor #147 |
|
|
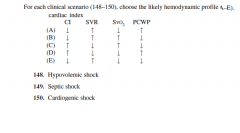
Hypovolemic shock - E Septic shock - C Cardiogenic shock - A |
|
|
Abx prophylaxis for: 38yo with suspected cystic teratoma who is scheduled for a laparoscopic oophorectomy |
none #157 |
|
|
Abx prophylaxis for: 36yo healthy women scheduled for TLH |
Cefazolin #154 |
|
|
Abx prophylaxis for: 38yo with BMI 45 and echocardiogram confirmed mitral valve prolapse scheduled for vaginal hysterectomy |
cefazolin #155 "level I evidence supports the use of 1st generation cephalosporins for women who undergo TAH or total vaginal hysterectomy" "Level III evidence supports prophylaxis for minimally invasive surgery - either TLH or LAVH" |
|
|
Abx prophylaxis for: 43yo with endometrial cancer and 18wk size uterus scheduled for an abdominal hysterectomy. She has a penicillin allergy not caused by immediate hypersensitivity |
Cefazolin |
|
|
Which hemostatic agent? acidic plant-based extract that saturates with blood at the bleeding site and forms a brownish or blackish gelatinous mass, which aids in the formation of a clot via the intrinsic coagulation pathway |
Oxidized regenerate cellulose "Surgicel" - supplied as mesh, "Nu-Knit", "Fibrillar", "SNoW" #158 |
|
|
Which hemostatic agent? Purified bovine-based agent that attracts platelets to a bleeding site, initiating the formation of a physiologic platelet plug |
microfibrillar collagen #159 supplied as sheets "actifoam, Avitene, helistat" |
|
|
Which hemostatic agent? Bovine or human extracted agent that converts fibrinogen to fibrin in addition to cross-linked granules that aid in platelet adhesion & aggregation |
flowable gelatin matrix with thrombin #160 supplied as liquid, "thrombin - JMI" |