Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
|
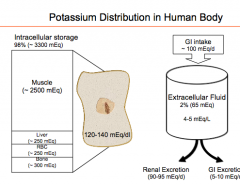
How is K distributed in the human body? Where is most of it? What is intracellular K concentration? What is extracellular? Where is the majority excreted?
|
|
|
|
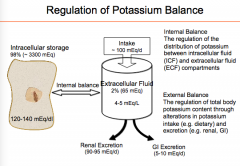
K concentration in the body is maintained how?
Internal balance of K is maintained by regulation of what? |
|
|
|
Identify the places where urinary potassium is excreted in the nephron. Where is K reabsorbed?
|

|
|
|
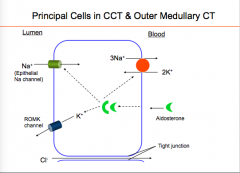
How does K+ enter and exit in cells of the thick ascending loop of Henle?
|

|
|
|
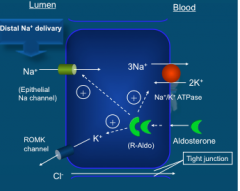
How does potassium enter the lumen in principal cells in the CCT and outer medullary CT?
What causes this? |
|
|
|
What are the factors that affect K secretion in the CT? What is the final step in K secretion affected by?
|
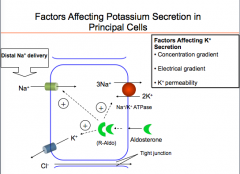
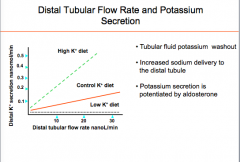
1. Concentration gradient of K across cell membrane (depends upon serum K concentration)
2. Electrical gradient across cell membrane (depends upon reabsorption of Na through Na channels in luminal membrane --> depends upon Na tubular lumen concentration --> distal delivery of Na. 3. K-permeability of the luminal membrane |
|
|
What if Na is not reabsorbed in the earlier part of the tubules (PCT or loop of Henle)?
What if the opposite occurs? |
More Na will be delivered tot he collecting tubule --> more Na reabsorption by ENa channel and K loss.
Not a large distal delivery --> will impair K secretion in collecting tubule |
|
|
What does K permeability of luminal membrane depend upon? What is this affected by?
|
Number of open K channels on luminal membrane
Aldosterone combines with receptor in the cells and increases the number of open luminal Na channels --> increase in NaK ATPase activity and open up K channel. |
|
|
What will the increase in aldosterone cause?
What will inhibition of aldosterone cause? |
Hypokalemia
Hyperkalemia? |
|
|
How does distal tubular flow rate affect distal potassium secretion?
|
|
|
|
What factors will decrease renal potassium secretion?
What will all of these factors also cause? |
Renal failure, distal tubular dysfunction, decreased distal tubular flow, hypoaldosteronism (will cause hyperkalemia).
Increased serum K levels (hyperkalemia) |
|
|
What can cause increased renal potassium secretion (4 categories)?
|
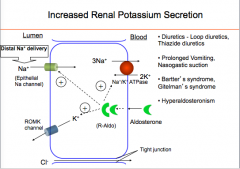
Diuretics (loop and thiazide), prolonged vomiting/nasogastric suction, Bartter's Syndrome/Gitelman's syndrome, hyperaldosteronism
|
|
|
How is internal potassium balance maintained?
|
By adjusting the K transport across the cell membrane (Na+ K+ ATPase is energy dependent)
|
|
|
How is K transported into cells?
|
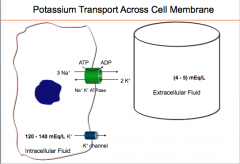
NaKATPase (3Na+ in for every 2K+ out)
Requires energy Main pathway to transport K inside cells ALL FACTORS THAT AFFECT K INTERNAL BALANCE WORK THROUGH THIS PUMP. |
|
|
What three factors favor K movement across the cell membrane?
What can directly affect the K diffusion out of the cells? |
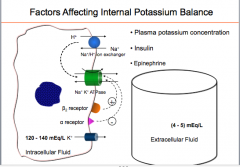
1. Plasma K concentration
2. Insulin 3. Epinephrine PLASMA K CONCENTRATION |
|
|
Describe the effect of insulin.
|
Insulin moves K inside the cells, but it does not directly work on this pump. Instead, insulin stimulate a NaH exchanger on the cell membrane that moves Na inside the in exchange for Na, this intracellular Na than activate the NaKATPase pump and moves K inside the cells. Other hormone epinephrine activate the NaKATPase pump by stimulating beta receptor. If there is deficiency of insulin as it happens in diabetic patients, or if we block the beta receptor by beta blocker, the activity of NKATPase pump will be impaired, with decrease movement of K from ECF to ICF. But the K channel which is not affected by the hormones will remain open and will continue to move K ICF to ECF which will result in elevated K in ECF.
� |
|
|
What are some factors affecting internal balance of potassium?
|
Acid-base distubance
Plasma tonicity Cell lysis and cell proliferation |
|
|
How do acid base disturbances affect internal balance of potassium? Which have a greater effect (metabolic or respiratory)?
With regard to organic acids or mineral acids, which have a greater effect? |

|
|
|
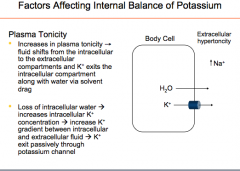
How does plasma tonicity affect internal balance of potassium?
|
|
|
|
Does plasma tonicity or osmolality also affect serum K? How?
What conditions will this happen in? |
Hypertonic ECF --> movement of ICF water to ECF, when water moves out of the cell, drags K along with it. (SOLVENT DRAG)
Water movement out of cell with ECF hypertonicity increases intracellular K, which increases gradient between ICF and ECF --> more K diffusion out through K channel --> hyperkalemia Diabetic ketoacidosis or diabetic hyperosmolar state --> ECF tonicity due to elevated glucose concentration |
|
|
How does cell lysis and cell proliferation affect internal balance of potassium?
|

|
|
|
What are some causes of hyperkalemia?
|

|
|
|
What are some causes of excessive potassium intake?
|
Oral or parenteral intake
|
|
|
What are some causes of decreased renal excretion?
|

|
|
|
What are some causes of internal redistribution?
|

|
|
|
What are some EKG manifestations of hyperkalemia?
Put them in order serum K? |

|
|
|
What are some signs and symptoms of hyperkalemia? Think cardio and neuro.
|

|
|
|
What do clinical manifestations of hyperkalemia primarily result from?
What does prolonged depolarization cause? |
Depolarization of resting cell membrane potential in myocyes and neurons.
Prolonged depolarization decreases membrane Na+ permeability through the inactivation of voltage-sensitive Na+ channels producing a reduction in membrane excitability. |
|
|
What are the two main big things to do to treat hyperkalemia?
|
Stabilize cardiac muscle cells
Lower serum K+ |
|
|
What are two general ways to lower serum K+?
|
Moving K inside the cells
Moving K outside the body |
|
|
How do you move K inside the cells?
|
Insulin
B-agonists (albuterol) Bicarbonate |
|
|
How do you move K outside the body?
|
Diuretics
Resins (kayexalate) Dialysis |
|
|
Where do insulin and albuterol act (net effect)?
|
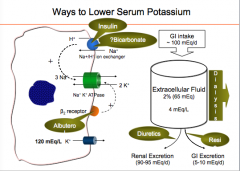
Potentiate the activity of Na K Atpase pump and move K inside cells
|
|
|
Where does insulin also act? Where does albuterol act? (both initially)
|
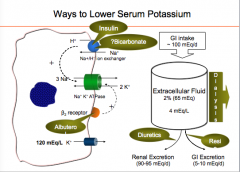
Insulin = Na+ H ion exchanger
Albuterol = B2 receptor |
|
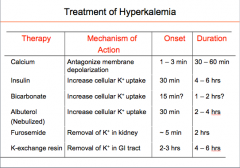
Know this table?
|

|
|
|
What are some causes of hypokalemia?
|

|
|
|
What are causes of external K losses?
|

|
|
|
What are some causes of internal redistribution?
|

|
|
|
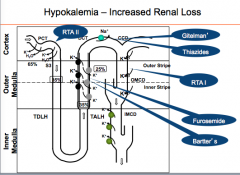
What are the two different types of renal losses that result in hypokalemia?
|
|
|
|
What are the two types of normotensive disorders?
|
With metabolic alkalosis
With metabolic acidosis |
|
|
What are some causes of hypokalemia normotensive with metabolic alkalosis?
|
Diuretics (loop, thiazide)
Prolonged vomiting, nasogastric suction Bartter's syndrome, Gitelman's syndrome |
|
|
What are some causes of hypokalemia normotensive disorders with metabolic ACIDOSIS?
|

|
|
|
Where does RTAII, furosemide, Bartter's, Gitelman, Thiazides, and RTA I affect the nephron leading to hypokalemia?
|
|
|
|
What are some causes of hyperreninemia?
What are some causes of primary hyperaldosteronism? How do these cause hypokalemia? |
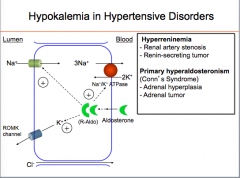
Diuretics and these 2 syndromes cause hypokalemia by increasing distal Na delivery.
|
|
|
What other two cause hypokalemia in hypertensive disorders?
|
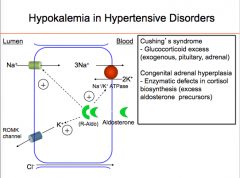
Again, by increasing distal Na delivery
|
|
|
What are the major clinical manifestations of hypokalemia (general locations)? Is this in acute or chronic situations?
|
1.) Cardiac
2.) Smooth muscle 3.) Skeletal muscle 4.) Renal Acute --> chronic is asymptomatic |
|
|
What are the cardiac manifestations?
|
EKG changes
Arrhythmias--Tachyarrhythmias |
|
|
What are the smooth muscle manifestations?
|
Hypertension
Ileus |
|
|
What are the skeletal muscle manifestations?
|
Weakness
Rhabdomyolysis |
|
|
What are the renal manifestation?
|
Nephrogenic diabetes insipidus
|
|
|
What are the EKG manifestations of hypokalemia? Put in order of decreasing K.
|

|
|
|
What is the treatment of hypokalemia?
What change indicates a deficiency of 200-400 mEq of potassium? What is the used for treatment? Oral and intravenous |

|
|
|
What diuretics are used to treat hypokalemia?
|
Potassium sparing diuretics = usually in chronic, both types work on collecting tubule
ENaC sodium channel inhibitors = amiloride, triamterene Mineralocorticoid antagonists = spironolactone, eplerenone |
|
|
How do the aldosterone receptor agonists act?
How do the ENa channel inhibitors act? |
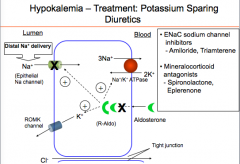
1. Aldosterone receptor antagonists: Which act by preventing the binding of aldosterone with the aldosterone receptors.
2. ENa channel inhibitors: These act inhibiting the ENa channel Inhibiting this channel will increase the +ve charges in the lumen, which in turn will prevent K secretion. |
|
|
True or false:
1. None of the bodies potassium is intracellular. 2. All the potassium is excreted through feces. 3. Proximal tubule is the major site of potassium reabsorption. 4. Distal tubule is the major site of potassium secretion. |
1. False = almost all is INTRACELLULAR
2. False = excreted by KIDNEY 3. True 4. False = COLLECTING TUBULE is the site of potassium secretion |
|
|
What are the important determinants of potassium secretion?
|
Serum aldosterone level and distal sodium delivery
|
|
|
Both high and low "what" can cause serious cardiac rhythm abnormalities.
|
Serum potassium levels
|