Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
228 Cards in this Set
- Front
- Back
|
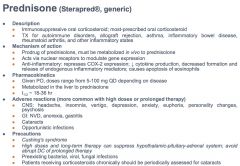
prednisone
|
|
|
|
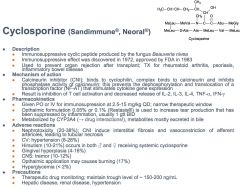
Cyclosporine
|
|
|
|
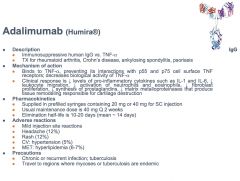
Adalimumab
|
|
|
|
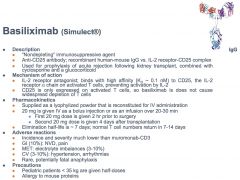
Basiliximab
|
|
|
|
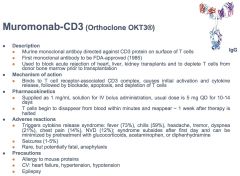
Muromanab-CD3
|
|
|
|
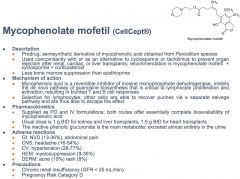
Mcophenolate mofetil
|
|
|
|
Azathioprine
|

|
|
|
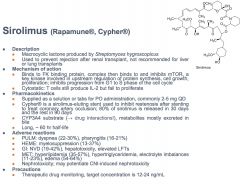
Sirolimus
|
|
|
|
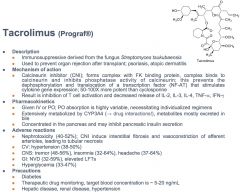
Tacrolimus
|
|
|
|
cyclosporine vs tacrolimus
|

Tacrolimus commonly associated with hyperglycemia, unlike cyclosporine
|
|
|
Bethanechol
|
|
|
|
Carbachol
|
|
|
|
Methacholine
|
|
|
|
Nicotine
|
|
|
|
Pilocarpine
|
|
|
|
Edrophonium
|
|
|
|
Neostigmine
|

|
|
|
Physostigmine
|
|
|
|
Echothiophate
|
|
|
|
Pralidoxime
|
|
|
|
Atropine
|

|
|
|
Ipratropium
|
|
|
|
Oxybutynin
|
|
|
|
Varenicline
|
|
|
|
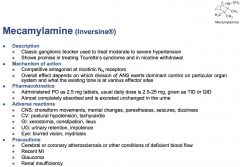
Mecamylamine
|
|
|
|
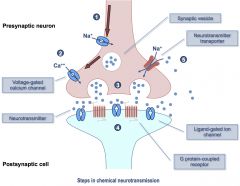
Review of Neurotransmission
|
|
|
|
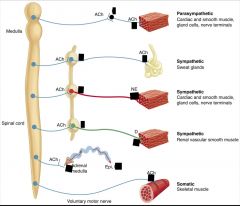
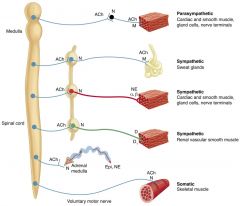
Cholinergic vs adrenergic neurons
|
Cholinergic: neurons that release acetylcholine (ACh)
-All motor neurons to skeletal muscle (somatic nerves) -All preganglionic ANS neurons; first synapse in ANS is always cholinergic -All postganglionic parasympathetic neurons -Some postganglionic sympathetic neurons -Most sweat glands -Some blood vessels in skeletal muscle Adrenergic: neurons that release norepinephrine (NE), epinephrine (E), or dopamine (DA) -Most postganglionic sympathetic neurons release NE -Adrenal medulla (a modified sympathetic ganglion) releases E and NE -Some postganglionic neurons release DA |
|
|
Acetylcholine biosynthesis and metabolism
|
Synthesized by Choline-acetyl transferase (ChAT) from choline and acetyl coA.
Metabolized by Acetylcholine esterase. |
|
|
|
|
|
Biosynthesis of catecholamines
|
Tyrosine hydroxylase: Tyrosine to DOPA
Aromatic amino acid decarboxylase: DOPA to Dopamine Dopamine B hydroxylase: Dopamine to Norepinephrine PNMT: Norepinephrine to Epinephrine |
|
|
Metabolism of Dopamine
|
Dopamine
Monoamine oxidase, Aldehyde dehydrogenase: Dopamine to DOPAC COMT: DOPAC to HVA Either of these enzymes can be used first, then the other will act. |
|
|
Metabolism of NE and E
|
MAO, ALDH, and COMT convert them to vanilylmandelic acid (VMA)
VMA is used as a diagnostic for catecholamine secreting tumores |
|
|
Differences between adrenergic and cholinergic synapses
|
Adrenergic: Vesicle transport protein is called VMAT. Adrenergic neurotransmitters are recycled (taken up by transporters)
Cholinergic: Vesicle Acetylcholine transporter protein (VAT) transports ACh into vesicle for release. ACh is degraded by acetylcholinesterase on postsynaptic cell and choline is recycled. |
|
|
Receptor Types that respond to ACh (cholinergic)
|
Muscarinic:
-G protein-coupled -Respond to the plant alkaloid muscarine -Five subtypes (M1-M5) Nicotinic: -Ligand-gated ion channels -Respond to the plant alkaloid nicotine -Two subtypes (NM, NN) |
|
|
Receptor types that respond to catecholamines (Adrenergic)
|
Two types of receptors respond to NE and E
-α receptors, two subtypes (α1, α2); each subtype has three subtypes (α1A, α1B, α1D and α2A, α2B, α2C) -β receptor, three subtypes (β1-β3) One type of receptor responds to DA -Five subtypes (D1-D5) |
|
|
Cholinergic Receptors and characteristics
|
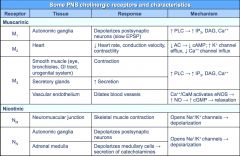
Focus on M2 and M3
|
|
|
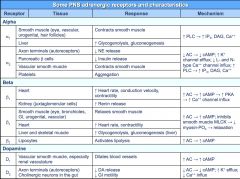
Adrenergic Receptors and characteristics
|
|
|
|
M1 receptor
|

|
|
|
M2 receptor
|

|
|
|
M3 receptor
|

|
|
|
Nm receptor
|

|
|
|
Nn receptor
|

|
|
|
a1 receptor
|

|
|
|
a2 receptor
|

|
|
|
B1 receptor
|

|
|
|
B2 receptor
|

|
|
|
B3 receptor
|

|
|
|
D1 receptor
|

|
|
|
D2 receptor
|

|
|
|
Methacholine Challenge Protocol
|
Used to diagnose asthma. Start at low doses and increase until reach a 16 mg/mL dose. If they reach this dose then they are not preasthmatic. But if at smaller doses they show sign, then they are preasmathic.
|
|
|
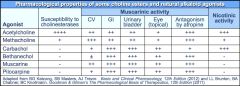
Compare choline esters to each other
|
|
|
|
Neostigmine vs physostigmine
|
Neostigmine does not cross BBB, so there is no CNS side effects. Better for treating myasthenia gravis because it restores peripheral skeletal muscle action without affecting CNS.
Physostigmine is drug of choice for counteracting toxic anticholinergic effects because it will fix the CNS as well. |
|
|
Myasthenia gravis
|
An autoimmune disorder against nicotinic receptors, so people have very low muscle tone.
|
|
|
Signs of excessive cholinergic activation
|
SLUDGE:
Salivation Lacrimation Urination Defication Gastrointestinal distress Emesis |
|
|
Signs of Deficient cholinergic activation
|
Mad as a hatter
Blind as a bat red as a beet hotter than heck dry as a bone bowel and bladder have lost their tone the heart runs alone (unopposed sympathetic activity) |
|
|
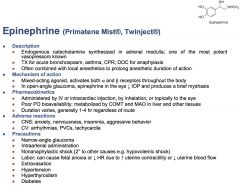
Epinephrine
|
|
|
|
Ephedrine
|

|
|
|
Norepinephrine
|

|
|
|
Clonidine
|

|
|
|
Phenylephrine
|
|
|
|
Albuterol
|

|
|
|
Dobutamine
|
|
|
|
Isoproterenol
|

|
|
|
Salmeterol
|
|
|
|
Phenoxybenzamine
|

|
|
|
Phentolamine
|

|
|
|
Prazosin
|

|
|
|
Tamsulosin
|

|
|
|
Atenolol
|

|
|
|
Metoprolol
|
|
|
|
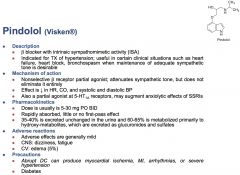
Pindolol
|
|
|
|
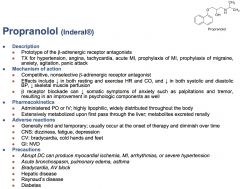
Propranolol
|
|
|
|
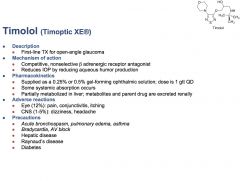
Timolol
|
|
|
|
3 Adrenergic Agonist Drugs
|
Ephedrine b1, b2, net
Epinephrine a1, a2, b1, b2 Norepinephrine a1, a2, b1 |
|
|
2 Alpha-adrenergic agonist drugs
|
Clonidine a2
Phenylephrine a1 |
|
|
4 Beta-adrenergic agonist drugs
|
Albuterol b2
Dobutamine b1, minor a1 b2 effects Isoproterenol b1 b2 Salmeterol b2 |
|
|
4 alpha-adrenergic antagonists
one extra |
Phenoxybenzamine a1
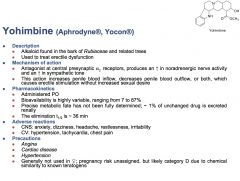
Phentolamine a1, a2 Prazosin a1 Tamsulosin a1A receptors Yohimbine a2 |
|
|
5 Beta-adrenergic antagonists
|
Atenolol: B1
Metoprolol: B1 Pindolol: Nonselective (partial agonist) Propranolol: nonselective Beta Timolol: nonselective Beta |
|
|
6 Cholinergic agonists
|
Acetylcholine: muscarinic and nicotinic
Bethanechol: Muscarinic only Carbachol: Muscarinic, and Nn Methacholine Muscarinic, some Nn Nicotine: nicotinic only Pilocarpine: muscarinic only |
|
|
5 Cholinesterase agents
|
Edrophonium
Neostigmine Physostigmine Ecothiophate Pralidoxime |
|
|
4 Cholinergic antagonists
|
Atropine: muscarinic
Ipratropium: muscarinic Oxybutynin: muscarinic Varenicline: nicotinic (partial agonist) |
|
|
1 Ganglionic blocker
|
Mecamylamine: Nn antagonist
|
|
|
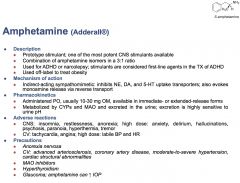
Amphetamine
|
|
|
|
Atomoxetine
|

|
|
|
Botulinum toxins
|
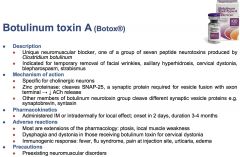
|
|
|
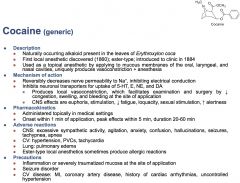
Cocaine
|
|
|
|
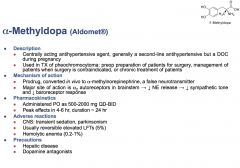
alpha-methyldopa
|
|
|
|
Alpha-methyltyrosine
|

|
|
|
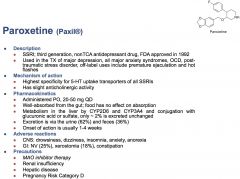
Paroxetine
|
|
|
|
Phenelzine
|
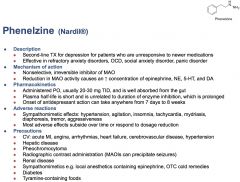
|
|
|
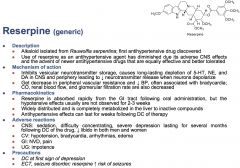
Reserpine
|
|
|
|
Tyramine
|
Tyramine-containing foods must be avoided with MAOIs
-Wine, beer, sherry, aged cheese, yeast extract, protein extract, soy sauce, fava or broad bean pods, smoked poultry, meats, fish (lox, smoked salmon), pickled poultry, meats, fish (pickled herring), chicken livers, fermented sausage (bologna, pepperoni, salami, summer sausage) or other fermented meat, bananas, avocados, over-ripe fruit Can produce a hypertensive crisis: hypertension, tachycardia, severe headache, fever, mydriasis |
|
|
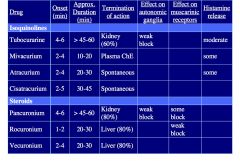
Benzylisoquinoloine Derivatives and Steroid Derivatives
|
2 structural classes of non-depolarizing Neuromuscular blockers, competitive antagonists. All are rigid & bulky structures that have a permanently “+” quaternary N atom, this makes them unable to cross BBB or cells. Distribution is limited to plasma because they are not lipid soluble.
Benzylisoquinolone derivatives: d-Turbocurarine Atracurium Mivacurium Cistracurium Steroid Derivatives: Pancuronium Vecuronium Rocuronium |
|
Compare Non-depolarizing Neuromuscular Blockers (chart)
|
|
|
|
Depolarizing Neuromuscular Blockers
|
Succinylcholine is main one
-AGONISTS of the NMJ nAChR -Depolarize the skeletal muscle membrane -Initially trigger muscle contraction -Disorganized contractions: fasciculations -Depolarization is prolonged -These agonists are not hydrolyzed by AChE -Prolonged depolarization inactivates voltage-gated Na+ channels in muscle |
|
|
Succinylcholine General properties
|
-Fast onset ( < 1 min)
-Short duration of action ( < 10 min) - Rapidly metabolized by plasma cholinesterase (succinate + 2 cholines) |
|
|
Succinylcholine Clinical Applications
|
-“Rapid sequence” induction / intubation
-Minimize chances of pulmonary aspiration of gastric contents -For very short procedures (<10 min) |
|
|
Succinylcholine Adverse Effects
|
Related to agonist activity at other AChRs
-Stimulates autonomic ganglia AChRs -Hypertension, tachycardia (adults) -Stimulates cardiac muscarinic receptors -Bradycardia (children) Histamine release Myalgias (from muscle fasciculations) Increased intracranial, intraocular pressures Hyperkalemia (potassium leaks out when it binds) happens more often in pts with: -Proliferation of extrajunctional nAChRs (5-10 d) -Denervation (e.g. spinal cord injury, stroke) -Burns, trauma, prolonged immobility -Myopathies (esp. Duchenne muscular dystrophy) |
|
|
Phase II block with succinylcholine
|
Usually succinylcholine is very predictable in it's duration. For unknown mechanisms, phase II block occasionally occurs and the patient is blocked for much longer than normal.
|
|
|
When would there be decreased metabolism of succinylcholine by plasma ChE?
|
Decreased circulating levels of plasma ChE
-Severe liver disease -Inherited (“K-variant”) Decreased activity of the plasma ChE enzyme -ChE inhibitors (neostigmine; organophosphates) -Inherited (“atypical variant”) |
|
|
Reversal of Neuromuscular Blockade
|
Inhibiting AChE at the NMJ increases the concentration of ACh in the synaptic cleft
Two agents are most commonly used: Neostigmine Edrophonium These are usually paired with Glycopyrrolate and Atropine, respectively, which are muscarinic antagonists to prevent excessive muscarinic side effects in the body. |
|
|
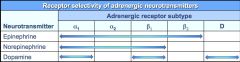
Receptor Selectivity of adrenergic neurotransmitters
|
|
|
|
What happens to Pulse rate, blood pressure and peripheral resistance with a a1, B1 agonist, such as norepinephrine?
|
BP and Peripheral resistance increase. Pulse rate decreases despite B1 activation, because of the baroreceptor reflex from increased blood pressure.
|
|
|
What happens to Pulse rate, blood pressure and peripheral resistance with a a1, B1, B2 agonist, such as epinephrine?
|
Decrease in peripheral resistance.
Systolic BP rises because of a1 tone, diastolic BP decreases because of B2 receptors. Pulse Rate increases because there is no baroreceptor reflex, allowing B1 and B2 to increase heart rate. |
|
|
What happens to Pulse rate, blood pressure and peripheral resistance with a B1, B2 agonist, such as Isoproterenol?
|
Pulse rate increases a lot (higher than with epinephrine)
Systolic BP increases and diastolic BP decreases Peripheral resistance drops a lot (lower than epinephrine) |
|
|
3 organs that have predominant sympathetic tone
|
arterioles, veins, sweat glands
everything else has parasympathetic tone |
|
|
Which NM blockers spontaneously degrade?
|
Atracurium and cistracurium
|
|
|
Which NM blockers are excreted by the kidney?
|
Turbocurarine, pancuronium
|
|
|
Which NM blockers are excreted by the liver?
|
Rocuronium, vecuronium
|
|
|
What type of G coupled protein are all the CNS receptors?
|
QISSS QIQ SIDD
a1, a2, b1, b2, b3, m1, m2, m3, d1, d2, nm, nn |
|
|
Yohimbine
|
|
|
|
Drugs used to prevent organ rejection (non-specific organ)
|
Prednisone
Cyclosporine tacrolimus |
|
|
Drugs recommended for Renal Transplant
|
Sirolimus,
Azathioprine Mycophenolate mofetil muromonab-CD3 Basiliximab |
|
|
Drugs recommended for liver transplant
|
Mycophenolate mofetil
muromonab-CD3 Not: sirolimus |
|
|
Drugs recommended for lung transplant
|
Not Sirolimus
|
|
|
Drugs recommended for cardiac transplant
|
Mycophenolate mofetil, muromonab-CD3
|
|
|
5Ht uptake inhibitors
|
Cocaine, Amphetamine, Paroxetine
|
|
|
Induction
|
Therapy given with the intent for complete remission
|
|
|
Consolidation
|
Treatment given after cancer has disappeared following initial therapy to kill any cancer cells left in the body.
Intent: Increase cure rate, prolong remission |
|
|
Adjuvant
|
Intent: Administer post-surgery to eliminate residual disease
|
|
|
Neo-adjuvant
|
Intent: Administered prior to surgery
|
|
|
Palliative
|
Intent: Control symptoms, prolong life, NOT curative
|
|
|
Salvage
|
Intent: Potentially curative, administered for recurrence. 2nd, 3rd, 4th line treatments.
|
|
|
Goldie-Coldman Hypothesis
|
Maximal chance for cure occurs when all available agents are given simultaneously
|
|
|
Principles of Combination therapy
|
Select agents known to have single agent activity against disease
Select agents with different -Mechanisms -Toxicity profiles Administer at regular intervals |
|
|
Alkylating Agents Mechanism of Action
|
Crosslink DNA, so that cells cannot divide.
|
|
|
Alkylating Agents Class Toxicities
|
-Overall Dose Limiting Toxicity: Myelosuppression
-Nadir at 7-10 days post administration -Gastrointestinal: Nausea and Vomiting -Dermatologic: Alopecia -Reproductive: Infertility -Secondary Malignancies -Latency period of 5-7 years |
|
|
Cyclophosphamide
|
Alkylating Agent
A pro-drug metabolized by P450 to active mustard. Cell Phase Non-Specific Oral and IV formulations Indications: Lymphomas: Hodgkin’s (HL), Non-Hodgkin’s (NHL) Breast Cancer Small cell lung cancer Bone marrow transplants Non-oncologic indications: Auto-immune disorders |
|
|
Cyclophosphamide side effects
|
Hemorrhagic Cystitis. Acrolein, a metabolite of cyclophosphamide accumulates in bladder and causes hemorrhage.
Prevented by hydration and MESNA |
|
|
Temozolomide
|
Alkylating Agent
Demethylated to MTIC which alkylates guanine Oral Agent Indicatioins: brain tumors, brain metastases Toxicities: moderately emetogenic, myelosuppresive |
|
|
Methotrexate
|
Dihydrofolate reductase inhibitor
-Enzyme involved in production of purine and thymidylate synthesis -Inhibition disrupts purine and thymidylate production Dose Range: 40 mg/m2 weekly -12,000 mg/m2 Oral and IV formulations High Dose Methotrexate: -Doses > 500-1000 mg/m2, which is fatal unless given leucovorin also. Sodium bicarbonate increases urine excretion. -Careful monitoring for drug interactions: Sulfa, Phenytoin, Tetracycline, NSAID, Salicylates, Vitamin C. THese things all interact with protein binding, which changes the bioavailability. |
|
|
What do you give if you have delayed clearance of methotrexate?
|
Give glucarpidase, but it costs a lot! A synthetic enzyme that metabolizes TMZ.
|
|
|
Methotrexate Toxicities
|
Dose limiting toxicities
-Myelosuppression -Renal toxicity Gastrointestinal: Mucositis CNS toxicity Acute hepatic dysfunction |
|
|
5-Fluorouracil
|
Inhibits thymidylate synthetase (TS)
-Leads to deficiency in thymidine Indications: MOstly solid organs -Breast -Colorectal, esophageal, GE junction, gastric Cancer -Pancreatic -Renal Cell Cell phase specific (s-phase) Intravenous administration: bolus or continuous infusion have different side effects. Capecitabine is an oral pro-drug of 5FU |
|
|
5FU bolus toxicities vs continuous infusion/capecitabine
|
Bolus: Dose limiting toxicity: myelosuppression
Continuous/Capecitabine: Dose limiting toxicity is hand-and-foot syndrome (hands and soles turn red), diarrhea, mucositis |
|
|
Gemcitabine
|
Pyrimidine Antagonist
Incorporated into DNA and prevents appropriate stacking and replication Indications: -GI malignancies -Lung Cancer -Breast cancer -Uterine Sarcoma -Non-Hodgkin’s Lymphoma -Bladder/urachal cancers |
|
|
Gemcitabine Toxicity
|
Dose Limiting Toxicity: Myelosuppression
Flu like symptoms Rash Hemolytic uremic syndrome Rate Dependent Toxicity -Prolonging infusion of gemcitabine leads to increased -Neutropenia -Thrombocytopenia -Anemia |
|
|
Topoisomerase inhibitor class toxicities
|
Dose Limiting Toxicities:
-Myelosuppression -Irinotecan: Diarrhea Gastrointestinal: Nausea/Vomiting/Diarrhea Alopecia Secondary malignancies, like leukemia -Latency 1-2 years |
|
|
Irinotecan
|
Topo-isomerase I inhibitor
Stabilize topo-isomerase I and DNA link to prevent repair of DNA cleavage Indications -Lung cancer -Colorectal cancer Cell phase non-specific |
|
|
Irinotecan toxicities
|
Acute diarrhea: cholinergic, managed by atropine
Delayed diarrhea: secretory, managed by loperamide |
|
|
Etoposide
|
Topo-isomerase II inhibitor
Complexes with topo-isomerase II and forms single strand DNA breaks Indications (WIDE USE) -Leukemias -Lymphomas -Bone marrow transplants -Lung cancer -Germ cell cancers -Neuroendocrine tumors Cell phase specific: G2-S |
|
|
Anti-mitotic agents
|
Taxanes: Paclitaxel, Docetaxel, Cabazitaxel
-Natural Source: Pacific Yew Treat -Mechanism: Stabilizes tubulin polymerization and disrupts microtubule assembly/disassembly Vinca Alkaloids: Vincristine, Vinorelbine, Vinblastine -Natural Source: Periwinkle plant -Mechanism: Inhibits tubulin polymerization and disrupts microtubule assembly |
|
|
Paclitaxel
|
Stabilizes tubulin polymerization and disrupts microtubule assembly/disassembly
Indications: -Breast -Ovarian Dose limiting toxicity -Myelosuppression Hypersensitivity reactions -Require premedication: -Anti-histamine -Dexamethasone Cell phase specific: M-phase |
|
|
Vincristine
|
Stabilizes tubulin polymerization and disrupts microtubule assembly/disassembly
Indications: -Leukemias -Non-Hodgkin’s lymphoma Dose limiting toxicity -Neuropathy Cell phase specific: M-phase FATAL IF ADMINISTERED INTRATHECALLY |
|
|
Platinum Analogs
|
Mechanism of action: Alkylating like agents which crosslink DNA
Class members -Cisplatin: Lung, breast, bladder, head/neck, ovarian, germ cell -Carboplatin: Lung, breast, bladder, head/neck, ovarian -Oxaliplatin: Colorectal and GI malignancies Cell phase non-specific |
|
|
Platinum analogs class toxicities
|
-Acute and delayed nausea and vomiting
-Dose limiting toxicity: Myelosuppression -Neuropathy -Diarrhea |
|
|
Cisplatin specific toxicities
|
Renal toxicity
Ototoxicity Electrolyte wasting |
|
|
Carboplatin specific toxicities
|
Hepatic dysfunction
|
|
|
Oxaliplatin-specific toxicities
|
Cold-induced neuropathy
|
|
|
Bleomycin
|
A natural product used to induce single and double stranded DNA breaks via oxygen and iron dependent formation of free radicals
Indications -Testicular cancer -Hodgkin’s Lymphoma -Non-Hodgkin’s Lymphoma Cell Phase Specific: G2-M Phase |
|
|
Bleomycin toxicites
|
-Dose limiting toxicity: Pulmonary toxicity (cumulative effect, more common with total >400U/m2)
-Mucocutaneous toxicity -Fever -Hypersensitivity -Requires test dose |
|
|
Doxorubicin
|
A natural product that induces formation of covalent topoisomerase II-DNA complexes, strand breaking, and intercalates in DNA
Indications (WIDELY USED) -Breast, HL, NHL, sarcomas, lung cancers, neuorblastomas, Wilm’s tumor Cell phase NON-specific |
|
|
Doxorubicin Toxicities
|
Dose Limiting Toxicity
-CARDIOTOXICITY -Lifetime limit: 450-550 mg/m2 -MYELOSUPPRESSION Nausea and vomiting Alopecia Discoloration of urine and sweat VESICANT (if it gets outside of veins it will kill the tissue) |
|
|
Molecular targeted therapy vs biotherapy
|
Molecularly targeted therapy: Inhibit signal transduction pathways required for tumor cell growth and differentiation
Biotherapy: Modification of host immune response to cancer in hopes that immune system will play a role in limiting growth of cancer cells |
|
|
momab, ximab and xumab/zumab
|
"momab” = antibody derived from mouse
“ximab” = antibody that is chimeric or a mixture of mouse and human “xumab” or “zumab”= antibody that is humanized Mouse antibodies are more likely to give allergic reactions. |
|
|
Rituximab
|
Chimeric murine/human monoclonal antibody against CD20 antigen on the surface of B-lymphocytes. This results in the activation of the patient’s immune system and antibody dependent cytotoxicity or apoptosis of B cells.
-Produces a response, not a CURE. B cells remain depleted for 6-9 months in 83% Indications: relapsed or refractory low grade or follicular CD20 positive B-cell Non-hodgkins lymphoma. -CD 20 positive CLL -First-line treatment of large B-Cell, CD-20 positive, non-hodgkin's lymphoma in combination with CHOP |
|
|
Rituximab Adverse Effects
|
Adverse effects include infusion related reactions (more common in first infusion) such as fever, chills/rigors, nausea, tiara fatigue, headache, bronchospasm, hypotension. Pretreat w/ APAP, diphenhydramine. Symptoms decrease from first infusion to the second infusion (80% to 40%).
|
|
|
Trastuzumab (Herceptin)
|
Humanized monoclonal antibody targeted against the Human Epidermal Growth Factor Receptor (HER2). HER2 is overexpressed in a number of cancers, including 25-30% of primary breast cancers also associated with colon, lung, and prostate cancer.
-Antagonizes the growth signaling properties of HER2 and thereby inhibits proliferation of tumor cells that overexpress HER2. -Signals immune cells to attack and kill malignant cells with this receptor -Adds to the cytotoxicity of traditional chemotherapy |
|
|
Clinical applications of trastuzumab
|
Breast cancer:
-Increased disease free survival (DFS) -Increased relapse free survival (RFS) -Increased time to death due to disease free survival (DDFS) -Favorable impact on overall survival (OS) But side effects are considerable |
|
|
Trastuzumab Adverse effects
|
Cardiovascular effects
-Can result in the development of ventricular dysfunction and congestive heart failure -Left ventricular function should be evaluated prior to therapy and during treatment -Discontinuation may be necessary |
|
|
Cetuximab (Erbitux) Indications
|
-Metastatic colorectal cancer in comb. with irinotecan
-Head and neck cancer in comb with radiation in pts with locally or regionally advanced SCC. -Head and neck cancer as single agent in recurrent or metastatic squamous cell carcinoma. |
|
|
Cetuximab (erbitux) Mechanism of Action
|
-Chimeric monoclonal antibody
-Binds to the cell surface epidermal growth factor receptor (EGFR-1) preventing EGF and TGF-alpha binding and signal transduction. IgG1 monoclonal antibody K-ras wild type patients appear to benefit most. (K-ras mutation testing predicts lack of response to therapy with antibodies targeted to the EGFR) -Patients with mutated k-ras bypass the upstream signaling of the EGFR receptors |
|
|
Cetuximab Side Effects
|
-Infusion reactions (3%) with rare associated fatality
-Fever (5%) -Dermatologic reactions (1%) -Interstitial lung disease (<0.5%) Additional information: cost estimate $3,000/dose (generally given weekly) |
|
|
4 Tyrosine Kinase Inhibitors
|
Imatinib - CML and GIST
Gefitinib - NSCLC Erlotinib - NSCLC, pancreatic Sunitinib - Renal Cell, GIST |
|
|
Imatinib
|
Gleevec:
Inhibits Bcr-Abl tyrosine kinase, which is created by the Philadelphia chromosome translocation seen in CML. This results in apoptosis of Bcr-Abl positive cells. Indications: new Ph+ CML, ALL or CML in blast crisis, accelerated phase, chronic phase, KIT(CD 117)-positive unresectable and/or metastatic GIST Dose: 400-600mg orally once daily Side Effects: Edema, fluid retention, nausea, vomiting, neutropenia, thrombocytopenia, hepatotoxicity Additional points: Cost ($$) and multiple drug interactions |
|
|
Erlotinib and Gefitinib
|
-Inhibit the intracellular phosphorylation of several tyrosine kinases associated with transmembrane cell surface receptors, including the tyrosine kinases associated with the epidermal growth factor receptor (EGFR-TK) that is overexpressed on the cell surface of 50-80% of NSCLC. This inhibition may decrease the growth, invasion, metastasis, angiogenesis, and resistance to apoptosis of NSCLC tumor cells.
Mutations in EGFR tyrosine kinase domain may predict response. CYP3AF substrate, increased INR when given with warfarin |
|
|
Erlotinib Indications
|
Locally advanced or metastatic NSCL after failure of at least one chemotherapy regimen, pancreatic cancer in combination with gemcitabine
|
|
|
Erlotinib Side Effects
|
Rash and diarrhea (grade 3 or 4), acne, dry skin, N/V. Interstitial lung disease in ~1% of patients (but fatal in 33% of these)
|
|
|
Sunitinib
|
TKI of multiple receptor tyrosine kinases including: platelet-derived growth factor receptors, vascular endothelial growth factor receptors, stem cell factor receptor and others which are involved in tumor growth and metastasis.
Indications: Renal Cell Carcinoma and Gastrointestinal Stromal Tumor (GIST) |
|
|
Sunitinib Effects
|
Hand-foot syndrome, Hypertension, Nausea, Diarrhea, Skin changes (discoloration in ~33% of patients), hypertension, mouth pain/irritation, taste disturbance
|
|
|
Imatinib Drug Interactions
|
Cyp3A4 substrates as well as inhibitors. Inducers (phenytoin) decrease imatinib levels. Inhibitors (cimetidine,itraconazole) increase imatinib levels. Substrates (simvastatin, cyclosporine). Also inhibits CYP2C19 and CYP2D6, use caution when administering substrates of these enzymes
|
|
|
Sunitinib Drug Interactions
|
Similar to erlotinib and imatinib—metabolized mainly by CYP3A4
|
|
|
mTOR inhibitors
|
-The mammalian target of rapamycin (sirolimus) (mTOR) signaling pathway functions as an important intermediary in a variety of cell signaling events to regulate cell growth and cell proliferation and angiogenesis
-These agents inhibit mTOR resulting in cell cycle arrest and possibly decreasing the expression of proteins such as vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), transforming growth factor (TGF) and others involved in angiogenesis and cell growth |
|
|
Temsirolimus and Everolimus
|
mTOR inhibitors:
Indicated for advanced renal cell carcinoma, pancreatic cancer Most common toxicities are rash, asthenia, mucositis, nausea, edema, and anorexia. |
|
|
Poly (ADP-ribose) Polymerase (PARP)
|
-Key role in the repair of DNA single-strand breaks through the base excision repair pathway
-Binds directly to sites of DNA damage -Recruits other DNA repair enzymes |
|
|
PARP inhibitors
|
PARP1 is a protein that is importnat for repairing singlt-stranded breaks in DNA. BRCA1 or BRCA2 deficiency sensitizes cells to PARP inhibition
Olaparib (still in development) |
|
|
Olaparib
|
A PARP inhibitor, still in development for BRCA ½ breast cancer, ovarian (III), depression (III)
|
|
|
Which chemotherapies are Non-cell cycle specific?
|
Irinotecan
cyclophosphamide gemcitabine (mostly S phase) platinums doxorubicin |
|
|
Which chemotherapies are M phase specific
|
Paclitaxel
Vincristine |
|
|
Which chemotherapies are S phase specific?
|
5-FU
Methotrexate |
|
|
Which chemotherapy is G2 and S phase specific?
|
Etoposide
|
|
|
Which chemotherapy is G2 and M phase specific?
|
Bleomycin
|
|
|
Which system does accomodation in the eye?
|
M3 activation contracts the ciliary smooth muscle, which relaxes the ligament an accommodates for near vision.
B2 activation slightly does the oppostie |
|
|
What receptor promotes bronchoconstriction?
|
M3
B2 relaxes |
|
|
Bronchial glands symp and parasymp effects
|
M3-->mucous secretion
B2-->watery secretion via CFTR |
|
|
What is special about M3 activation in vascular endothelium?
|
They are not innervated by the parasympathetic system, but can locally produce acetylcholine to activate M3 receptors and relax.
|
|
|
What is the effect of M2 receptor activation in the heart?
|
Gi decreases I,f current and I,ca channel. Activate I,K. This all slows heart rate, slows conductivity.
|
|
|
Symp and Parasymp activity in Kidney and Bladder
|
D1 activation: vasodilation and increased GFR
B1: stimulates renin release M3: contraction of bladdur detrusor, relaxation of trigone and sphincter to urinate B2: Relaxes detrusor, urinary retention a1: constricts trigone and sphincter, urinary retention |
|
|
Symp and parasymp in Penis
|
M3 activation relaxes vessels: erection
a1 activation contracts seminal vesicles, prostatic capsule, vas deferens: ejaculation |
|
|
Symp and parasymp in uterus
|
Nonpregnant B2 activation: relaxes uterus
Pregnant: -M3: contracts uterus a1: contracts uterus B2: relaxes uterus |
|
|
Parasymp and symp in sweat glands
|
M3 activation: stimulates salivary, nasopharyngeal, pulmonary, GI and eccrine sweat glands
a1: stimulates apocrine sweat glands, viscous salivary secretions |
|
|
Organs with single innervation
|
All sympathetic:
-Blood vessels -Spleen -Piloerector muscles -Sweat Glands |
|
|
Chemo drugs that Myelosuppression is NOT the dose limiting toxicity
|
5-FU continuous or Capecitabine: Hand and Foot
Irinotecan: 2 types of diarrhea (other topoisomerase inhibitos are myelosuppressive) Vincristine: Neuropathy Bleomycin: Pulmonary effects All targeted therapies |
|
|
What do you have to give in combination with methotrexate
|
Leucovorin, it is a rescue from the high dose of methotrexate given. Need to carefully monitor drug interactions: sulfa, phenytoin, tetracyclin, NSAID, salicylates, vit C.
|
|
|
What do you give for delayed clearance of methotrexate
|
Glucarpidase
|
|
|
Chemo drugs where myelosuppression is a dose limiting toxicity
|
Alkylating agents
-TMZ Methotrexate+renal toxicity 5-FU bolus Gemcitabine Topoisomerase inhibitors (not Irinotecan) Paclitaxel Platinum Analogs Doxorubicin+Cardiotoxicity |
|
|
CYP3A4 substrates that you should know this block
|
Cyclosporine
Tacrolimus Sirolimus Oxybutinin Tamsulosin Amphetamine Paroxetine |
|
|
precautions for Cholinomimetic drugs
Which drugs are these? |
Carbachol, Methanachol, Bethanochol, Physostigmine, Neostigmine,
Acute cardiac failure (bradycardia) Asthma Hyperthyroidism (results in atrial fibrillation from sensitivity to adrenergic reflex) Peptic ulcer Urinary tract obstruction Bethanochol and Carbachol have parkinsonism |
|
|
Pilocarpine Precautions
|
Asthma
Iritis Posterior Synechiae Retinal detachment Heart Disease |
|
|
Nicotine Precautions
|
-Angina, arrhythmia, MI
-Caution with HTN, pheocromocytoma, insulin-dependent diabetes, vasospastic disease, thyroid disease -Pregnancy D for transdermal form |
|
|
Varenicline Adverse effects and precautions
|
Adverse effects: GI effects
Precautions: -Renal insufficiency -Black box warning for psychiatric symptoms |
|
|
Edrophonium Precautions
|
GI obstruction
Urinary tract obstruction Asthma Heart Disease |
|
|
Echothiophate Precautions
|
Uveitis (causes stinging in the eye)
|
|
|
Pralidoxime Precautions
|
Renal Insufficiency
AChE inhibitor TX for myasthenia gravis |
|
|
Atropine Precautions
|
-Acute MI
-Bladder obstruction/urinary tract obstruction/prostatic hypertrophy -Glaucoma -GI obstruction -Hyperthyroidism Chronic pulmonary disease Avoid things that elevate core body temperature |
|
|
Oxybutynin precautions
|
GI obstruction
Toxic megacolon, ulcerative colitis Urinary retention or Urinary tract obstruction Uncontrolled narrow-angle glaucoma CYP3A4 metabolism |
|
|
Ipratropium Precautions
|
Glaucoma
Urinary retention/bladder obstruction |
|
|
Mecamylamine Precautions
|
Cerebral or coronary atherosclerosis/deficient bloodflow
Recent MI Glaucoma Renal Insufficiency |
|
|
Neuromuscular blockers that have some effect on muscarinic receptors
|
Pancuronium and rocuronium (weaker)
|
|
|
Neuromuscular blockers that have some effect on autonomic ganglia
|
Tubocurarine and pancuronium
|
|
|
Neuromuscular blockers that have some effect on histamine release
|
Tubocurarine (moderate), mivacurium (some) atracurium (some)
|
|
|
Which drug needs a leucovorin rescue?
|
Methotrexate in high dose.
Also requires careful monitoring for drug interactions: sulfa, phenytoin, tetracycline, NSAID, salicylates, Vit. C. Glucarpidase is administered if renal clearance is low. |
|
|
mydriasis
|
Pupil dilation
|
|
|
Myosis
|
Pupil constriction
|
|
|
Cycloplegia
|
Loss of accomodation
|
|
|
Precautions for Epinephrine
|
Narrow-angle glaucoma
Intraareterial administration Nonanaphylactic shock Labor Extravasation Hypertension Hyperthyroidism Diabetes |
|
|
Precautions for phenyephrine
|
CV dieases
Narrow-angle glaucoma Labor Extravasation Hyperthyroidism |
|
|
Side effects of Clonidine
|
First dose effects: sedation, dizziness
Precautions Avoid abrupt withdrawl so prevent rapid epinephrine outflow. Breastfeeding Heart disease (may decrease CO too much) |
|
|
What adrenergic receptor dominates Systolic BP?
Diastolic BP? |
systolic: a1 increases
diastolic: B2 decreases |
|
|
Adverse effects of salmeterol and albuterol
|
CAD
Hypertension Hyperthyroidism Diabetes |
|
|
Phentolamine Adverse Side Effects
|
Adverse Reactions: Dizziness, orthostatic hypotension, reflex tachycardia, arrhythmias. Nasal congestion
MI, coronary insufficiency, angina |
|
|
Phenoxybenzamine Adverse Reactions
|
CNS: dizziness, syncope, fatigue
Reflex tachycardia, orthostatic hypotension Impotence Miosis Nasal congestion Precautions: Congestive HF, CAD, renal disease, hypotensive effects can worsen these conditions |
|
|
Amphetamine vs cocaine
|
Amphetamine blocks uptake, but also promotes efflux via reverse transport.
Cocaine is a pure uptake blocker. |
|
|
What classes of chemo cause secondary malignancies
|
Topoisomerase Inhibitors: 1-2 yrs later
Alkylating agents: 5-7 years later Platinums (but less so) |
|
|
How to prevent cholinergic and secretory diarrhea
|
Cholinergic: atropine
Loperaminde (immodium): Secretory |
|
|
Indications of paclitaxel vs vincristine
|
Paclitaxel: breast and ovarian
Vincristine: liquid tumors: leukemia, non-hodgkins |
|
|
"wide use" chemotherapies
|
Doxorubicin
Etoposide |
|
|
Drugs with Diabetes as a counterindication
|
NIcotine
Epinephrine Isoproterenol Albuterol Salmeterol Propranolol Timolol Metoprolol Pindolol Phenelzine |