Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
52 Cards in this Set
- Front
- Back
|
Peritoneum is...
|
1. Peritoneum is a large continuous sheet of serous membrane lining all surfaces
of the peritoneal cavity |
|
|
Function of the Peritoneum
|
provide a surface on which viscera can smoothly slide during peristalsis and the migration of the greater omentum etc
|
|
|
PARIETAL PERITONEUM
|
PARIETAL PERITONEUM which lines the abdominal cavity walls, except where viscera (i.e. EXTRAPERITONEAL VISCERA) are in direct contact with the wall.
|
|
|
VISCERAL PERITONEUM
|
•VISCERAL PERITONEUM which covers and surrounds all the viscera not in contact with the abdominal wall (i.e. INTRAPERITONEAL VISCERA)
|
|
|
Greater and Lesser Sac
|
|
|
|
What sits inside the peritoneal Cavity?
|
viscera (hollow or solid) within the abdominal cavity are actually outside the peritoneal cavity
|
|
|
PERITONEAL CAVITY
- clinical Uses |
•A potential space enclosed by the continuous PARIETAL and VISCERAL PERITONEUM.
•Contains only a few mils of lymph like fluid unless, - 1.Opened & air enters (e.g. laparotomy) 2.Fluid instilled (e.g. peritoneal dialysis) 3.Gas insufflated (e.g. CO2 with laparoscopic procedures). |
|
|
Peritoneal Cavity
-Pathological |
•ASCITES is a pathological accumulation of fluid in the peritoneal cavity
|
|
|
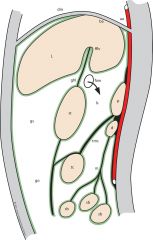
The opening between the greater and lesser sac is the...
|
Epiploic foreamen
Foremen of Windslo |
|
|
can compress portal and heptic supply to liver (pringles maneovour)
|
|
|
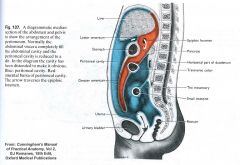
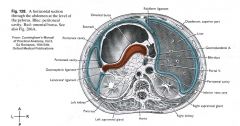
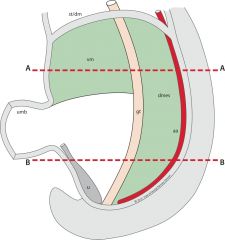
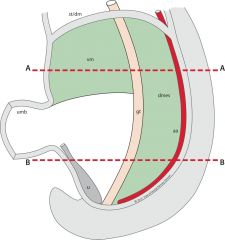
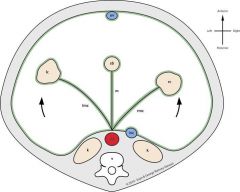
Horizontal Section through abdomen at the level of the pylorus
|
|
|
|
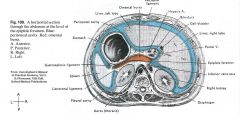
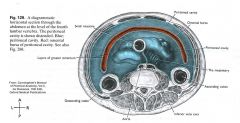
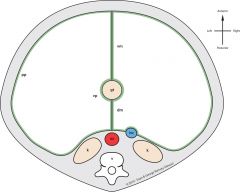
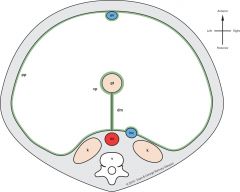
Horizontal Section through abdomen at the level of L4
|
|
|
|
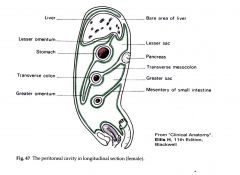
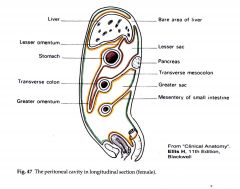
Difference b/w male and female peritoneal cavities
|
•MALE peritoneal cavity is a completely closed peritoneal sac
•FEMALE peritoneal cavity communicates with the exterior via the genital tract (via uterine tubes, uterine cavity and vagina). Hence ascending infections can occur (e.g. gonococcus and chlamydia). |
|
|
Are the ovaries covered in peritonium?
|
No
germinal epitheliun (NOT covered by pertinium) - otherwise the ova wouldnt be able to burst out |
|
|
Paritonium Innervations
|
•PARIETAL PERITONEUM has somatic dermatomal sensory innervation and hence when inflammed (e.g.peritonitis) pain receptors cause localised pain in the affected dermatomes.
•VISCERAL PERITONEUM has autonomic innervation (parasympathetic stretch receptors) and so generalised dull central pain experienced on swelling of viscus. •Example: Acute appendicitis. |
|
|
Acute Appendicitis Pain
|
- early dull pain around the umbillicus
- late and hugely inflamed; at mac burneys point |
|
|
Peritonitis
|
(i.e.inflammation of the peritoneum due to blood, bile, bowel content or infection etc) can result acutely in septicaemia.
- great absorption properties also allow rapid entry of bugs |
|
|
adhesions
|
•Chronically adhesions can occur tending to obliterate the cavity.
•This is beneficial as an attempt to localise the pathology. •However when severe can make laparoscopy impossible and laparotomy difficult and hazardous. •Adhesions may also cause bowel obstruction (can no longer move around as freely) |
|

|
loop of bowel caught around an adhesion
adhesion cut and the loop around it waiting for it to recover colour - flick to see if it perstalisis... this doent recover and needs resection |
|
|
SUPRACOLIC & INFRACOLIC COMPARTMENTS
|
divided by the transverse colon
|
|
|
SUBPHRENIC SPACES & PARACOLIC GUTTERS
|
where abscesses occur and radioloogist can find them and drain them
|
|
|
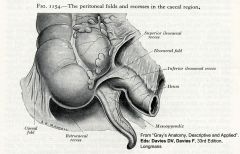
PERITONEAL FOSSAE
|
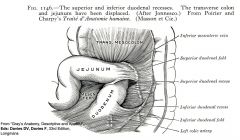
superior and inferior duodenal recess
superior and inferior ileocaecal recess pararectal fossa - INTERNAL HERNIAS |
|
|
superior and inferior duodenal recess
|
|
|
|
superior and inferior ileocaecal recess
|
|
|
|
Pararectal fossa
|
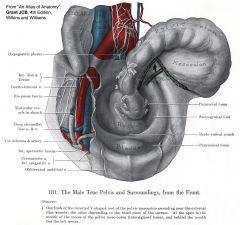
need to look for these hernias in explorative surgery
|
|
|
Embryology of the Peritoneum
|
simple straight tube
1. Development of gut tube and its derivatives (with mesenteries) 2. Development of gut tube and its derivitives (with mesenteries) 3. Development of the greater omentum and transverse mesocolon |
|
|
START: straight tube
|
|
|
|
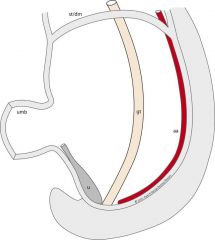
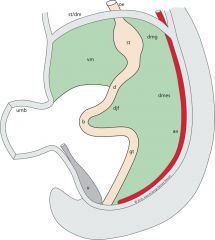
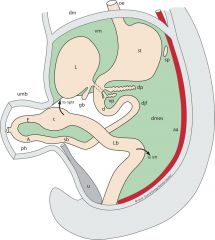
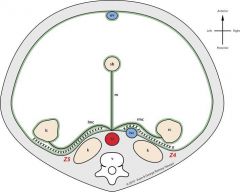
1. Development of gut tube and its derivatives (with mesenteries)
|
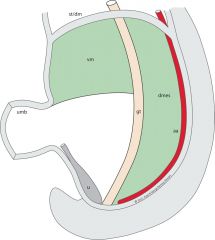
DM; dorsal mesentary
VM: ventral mesentary |
|
AA
|
|
|
BB
|
|
|
|
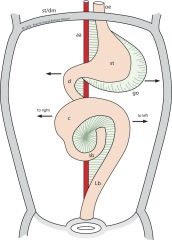
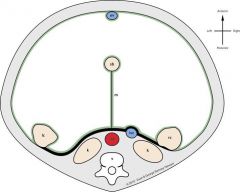
1. dilatation of stomach
2. bend for duodenum 3. mid gut loop |
|
|
|
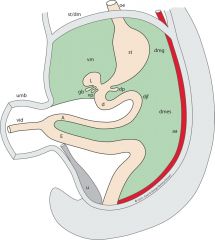
Buds\
- liver ventral pancreatic dorsal pancreatic and gall ballder mid gut loop almost connecting to the umblicus also now connected to the yolk sac vitiolo-duct (no nutritive value, hen atrophies) - if persist = meckels diveticulum |
|
|
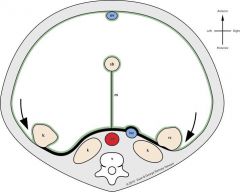
ph- physioological hernia
afferent limb of midgut loop smaller diameter than the effeerent |
|
|
AA. developemnt
|
|
|
|
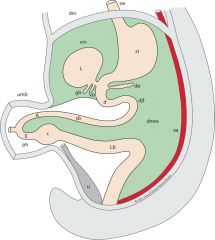
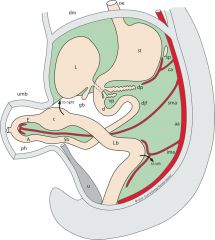
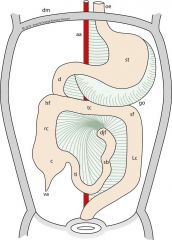
Rotation of the gut within and the return of the PH
|

- anticlockwise
|
|
|
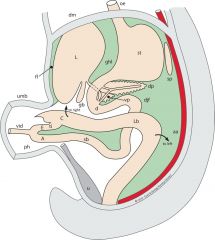
Rotation; lateral view
|
the differentil growth rates means the ventral and drosal pancreas now on the same side
liver is bigger and making falciform and stuff rotated loop and the twist in the DM and the small bowel beneath the transverse colon |
|
|
BS after rotation
|
|
|
|
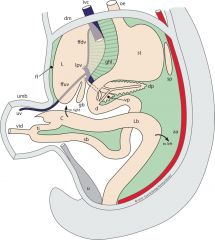
Pancreas Joining
|
|
|
|
Umbilical Vein
|
|
|
|
2. Development of gut tube and its derivitives (with mesenteries)
|
|
|
|
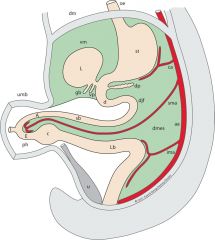
Later Stage Mesentary
|
|
|
|
Greater Omentum
|
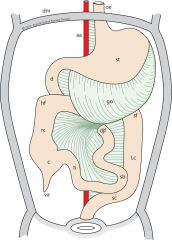
blowing out and stating to hang down
|
|
|
3. Development of the greater omentum and transverse mesocolon
|
|
|
|
Greater Omentum is ___ layers
|
fused 4 layer stucture (in greater omentum- getting rid of the lesser sac)
|
|
|
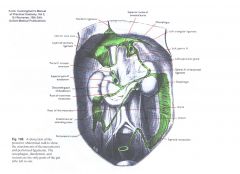
Surgical exposure of the lesser sac of peritoneum
|

1. lift the Greater Omentum
2. cut at the border of the GO and TC |
|
|
Right and left colons
- start off |

|
|
|
Dropping and fusiing
|
|
|
|
End up
|
|
|
|
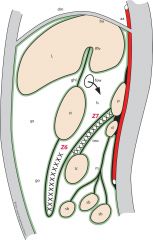
(Secondary retro-peritonealisation of the right and left colons and their surgical mobilisation)
|
|
|
|
Mobilised and ready for surgery
|
|
|
|
Peritoneal Attachments of the Liver 1
|
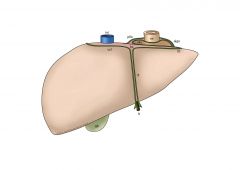
(i.e. Liver develops between the peritoneal layers of the ventral mesentery).
|
|
|
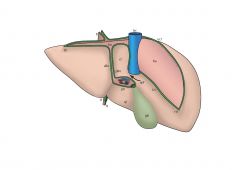
Peritoneal Attachments of the Liver 2
|
|