Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
16 Cards in this Set
- Front
- Back
|
World Federation Neurosurgeons (WFNS) SAH grading
|
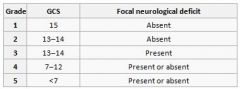
Score correlates with mortality
|
|
|
Child-Pugh Classification
|
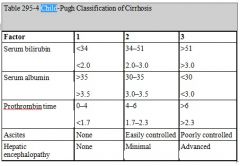
Operative mortality:
Score: 5-6 = Class A = low risk < 5% 7-9 = Class B = moderate risk 25% 10-15 = Class C = high risk > 50% |
|
|
Apgar Score
|

- Apgar’s are taken at 1 and 5min
- Memory aid: Activity (muscle tone) Pulse Grimace (reflex irritability) Appearance (colour) Respiration |
|
|
CHADS2
|
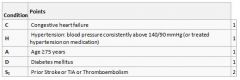
CHADS2=0, no therapy or Aspirin only is recommended
CHADS2=1, either Aspirin or Warfarin is recommended (depending on patient preferences) CHADS2 ≥ 2 should be managed with lifelong Warfarin (target INR 2.0-3.0) Overall risk of stroke in non-valvular AF is around 5% per year Warfarin reduces risk of CVA from 5% to 1% per annum Risk of major bleed 0.5% per annum |
|
|
Aortic Stenosis Severity (Echo)
|
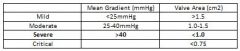
AHA Guidelines
|
|
|
Mitral Stenosis Severity (Echo)
|
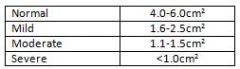
AHA Guidelines
|
|
|
Pulmonary Hypertension Severity (Echo)
|
Based on mean PAP:
Mild: 25-35 Moderate: 35-45 Severe: >45mmhg Based on RVSP: >40 has likely PHTN 50-60 moderate >60mmhg as severe |
|
|
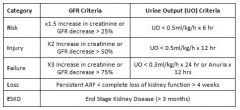
RIFLE Criteria
|
|
|
|
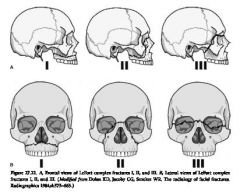
LeFort Fractures
|
|
|
|
Obstructive Lung Disease Severity
|
Severity based on FEV1% of predicted values (GOLD report on COPD 2011)
ᵒ Mild (stage 1) : >80% predicted ᵒ Moderate (stage 2): 50-80% predicted ᵒ Severe (stage 3): 30-50% predicted ᵒ Very Severe (stage 4) : <30% predicted |
|
|
STOP BANG
|
Snoring: loud snoring (can be heard through closed doors)
Tiredness: daytime somnolence Observed apnoea Plood pressure: Hx of hypertension BMI: >35 Age: >50 Neck Circumference: >40cm Gender: male >3 = High risk of OSA → refer for sleep testing |
|
|
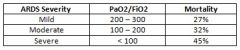
ARDS Severity
|
|
|
|
Soda Lime - Contents and reaction
|
Contains:
94% calcium hydroxide 5% sodium hydroxide 1% potassium hydroxide An indicator – such as ethyl violet Silica – increases hardness of the granules, minimising formation of alkaline dust which can be an airway irritant if inhaled The active ingredient is the sodium hydroxide, which acts as a catalyst, and is not actually consumed in the reaction: CO2 + H20 ↔ H2CO3 2NaOH + H2CO3 → Na2CO3 + 2H2O + heat Na2CO3 + Ca(OH)2 → CaCO3 + 2NaOH + heat |
|
|
Diastolic Heart Failure Echo Assessment
|
Transmitral flow velocity
E wave: peak filling velocity in early diastole A wave: peak filling velocity in late diastole E/A relationship Normal: E/A is > 1 As atrial kick only contributes 30% of filling Mild DD aka ‘Impaired relaxation’ E/A is <1 Relaxation is impaired and atrial contraction contributes relatively more to ventricular filling Moderate DD aka ‘Pseudonomral filling’ E/A normalises to E>A Compliance and relaxation reduced → impaired early diastolic filling and raised LAP → E >A Differentiated from normal by assessing transmitral flow with valsalva Severe DD aka ‘Restrictive filling’ E >> A LV compliance is extremely low → high LAP → high velocity E wave |
|
|
PONV
Apfel Simplified Risk Score Eberhart Simplified Risk Score |
Apfel Simplified Risk Score – In Adults
Four risk factors Female sex Non-smoker Hx of PONV or motion sickness Use of postoperative opioids Risk Score: 0 RF (baselines risk) = 10%, 1 RF = 20%, 2 RF = 40%, 3RF = 60%, 4 RF = 80% Eberhart Simplified Risk Score – In Children Four risk factors Age > 3 Surgery >30 mins Hx of POV, or PONV in 1st degree relative Strabismus surgery Risk Score: 0 RF (baselines risk) = 10%, 1 RF = 10%, 2 RF = 30%, 3RF = 55%, 4 RF = 70% |
|
|
MELD Score
|
Model for End-Stage Liver Disease (MELD) Score
Uses bilirubin, creatinine and INR MELD = 3.78[Ln serum bilirubin (mg/dL)] + 11.2[Ln INR] + 9.57[Ln serum creatinine (mg/dL)] + 6.43 Score correlates to 3month mortality |