![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
181 Cards in this Set
- Front
- Back
|
What type of bacteria dominate cellulitis infection? |
Gram+ and aerobic strep |
|
|
What type of bacteria dominate abscesses? |
mixed anaerobes (gram + and gram - anaerobes) |
|
|
Are antibiotics alone useful for treating abscesses? |
No! There is lack of blood flow due to body trying to isolate the bacteria from the rest of the body (may slow it down though but never 100% effective) |
|
|
what treatment does early cellulitis dictate? |
Antibiotics (Pen V or Amox) |
|
|
what treatment does abscess require? |
Pen V + Flagyl (For the gram -) and drainage |
|
|
What contraindicates prescription of flagyl? |
If patient is an alcoholic. They'll become really nauseated once they drink alcohol after flagyl |
|
|
What does cellulitis feel like upon palpation? |
Soft like edema, not well-defined and usually tender when palpated |
|
|
What does abscess feel like upon palpation |
Localized golf ball feeling. Not as painful upon palpation. |
|
|
potential complication with diabetic patient with infection? |
They feel sick, don't want to eat or take meds. DM gets worse, infection gets worse...dangerous! |
|
|
Patient with sunken in eyes, tight skin, dry mouth. What are you concerned about? |
Dehydration secondary to infection |
|
|
Patient mentions they have hives when taking Pen V...what is the danger of prescribing pen to them |
Hives is a precursor to anaphalaxis. |
|
|
You just prescribed antibiotics for a patient. The antibiotics isn't working if they dont' get better after ____________ days |
5 |
|
|
What's the biggest problem with Pen V? |
Can't take it with food because the stomach acid breaks down the Pen V. Compliance: hard to remember to take it every 6 hours. Patient must be compliant!! |
|
|
Patient is placed on Clindamycin. During the follow up the patient mentions that they have bloody diarrhea. What should you be concerned about? |
C. Difficile infection. |
|
|
Why should you never tell a patient to take immodium or anti-diarrhetic drugs when they are suffering from a C. Diff infection? |
The C. diff stays in the colon. Eventually this will lead to perforation of the colon. |
|
|
What are some things the patient should take if they have a C. diff infection? |
probiotic pills or yogurt. Stop the offending antibiotic. Prescribe Flagyl or Vancomycin for treatment (Gen med) |
|
|
What cc syringe and gauge is recommended for draining of an abscess? |
5 or 10 cc syringe with a 15 or 16 gauge needle |
|
|
Why is is a good idea to draw up air into a syringe before draining? |
Much easier to drain when there is air in the syringe already |
|
|
If you were to incise a true abscess, which area do you want to make your incision and why? |
fluctuant area. It's easiest to go through. (Unless anatomy prevents you from doing that, ie. chance of hitting of lingual nerve) |
|
|
Why do you never want to incise the fluctant area of an abscess on the side of the neck? Where do you want to Incise instead? |
Tissue at the biggest area is likely thinner, necrotic so will heal with a scar. You'd rather incise the healther area. Try to incise from inside the oral cavity whenever you can. |
|
|
What is the purpose of drainage? Will incision stop pus from forming? |
Drainage: Just provides relief and helps tissues fold over and heal well. doesn't stop the pus from forming. Tooth is still infected so will continue producing pus after you've done incision and drainage. |
|
|
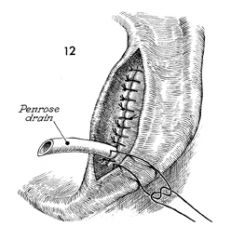
How long is a drain in for typically? |
Around 48 hours (amount of time it takes for the antibiotics to work). It's NOT a set rule. It depends on how severe the infection was, and if pus is still draining. If pus is still draining...leave the drain in! |
|
|
If a patient claims they have an "allergy" how do you differentiate between a true allergy and side effect? |
True allergy:- anaphylactic rxn - rash, swelling, etc Side effect: - runny stool from antibiotic, upset stomach w T3 |
|
|
Above what temperature is the patient considered to have a fever? |
>38 degrees = fever, but above 37.5 degrees in the oral cavity is considered fever |
|
|
What is the course of action you need to take if a patient presents to your clinic with Ludwig's angina? |
Maintaining of ABC, call 911, they need hospitalization and IV antibiotics and airway management |
|
|
List the 12 Danger signs of infections |
1) Significant trismus 2) Significant odynophagia 3) Dysphagia 4) Dyspnea 5) Elevation of Tongue 6) Deviation of Uvula 7) Bilateral Swelling 8) Rapid, Severe swelling 9) Chest Pain 10) Obvious Systemic Toxicity 11) Eye signs 12) Clouding/LOC |
|
|
Infection spreading into what 2 spaces causes significant trismus? |
Masseter Space, pterygomandibular space. Muscles become inflamed, they contract and decrease mandibular opening. |
|
|
Dysphagia is a sign of what danger space being invaded? |
Retropharyngeal space |
|
|
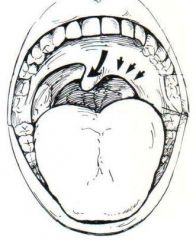
Invasion of what spaces causes Dyspnea? |
1) Invasion of the retropharyngeal space 2) and/or peritonsilar space. 3) Invasion of the sublingual space causing the tongue to lift up and block the airway |
|
|
Why should you be concerned if a regular patient of yours comes in with tooth pain and sounds funny compared to how they sounded like in the past? |
You're concerned that a infection has started to compromise the airway |
|
|
How can a wisdom tooth infection cause dyspnea? (ie. trace the path of its infection to the airway) |
first affects lateral pharyngeal space and then go posteriorly to retropharyngeal space |
|
|
What is deviation of the uvula indicative of? |
means a mass pushing from lateral pharyngeal space/soft palate has pushed its way onto the roof of the mouth. |
|
|
If the uvula is pushed to the right when the patient says "ahhh", which side is the source of the infection? |
Infection came from the left. |
|
|
Why is bilateral swelling a concern? |
-Dental infections should typically be on one side (unless mesiodens….) -This usually means that the infection is more severe and is having a systemic spread |
|
|
What is the danger triangle? |
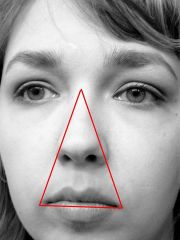
Infections that occur within the danger triangle can spread from one side to another because the veins in the face are valveless |
|
|
swelling that occurs under _____ hours is considered rapid swelling. What does this indicate? |
12. Usually a more severe infection and lots of bacteria. OR this can happen in a immunocompromised patient |
|
|
What are some reasons for mediastinitis? |
Swelling to Retropharyngeal space Danger space (to diaphragm) Prevertebral Space (to coccyx) |
|
|
Does mediastinitits affect the heart? |
No. Just the region around the heart. |
|
|
Why is mediastinitis so dangerous? |
indicates there is pus in the chest. Will require the chest to be opened, ICU and could be deadly (30-40% survival rate) |
|
|
What is ptosis? |
drooping of the upper eyelid |
|
|
What is chemosis |

conjunctiva of eyelid + eyeball should be tight, but chemosis is when conjunctiva is swollen -Looks like eye is popping out/ elevated (above sclera) |
|
|
What is epiphoria? |
tearing up (swelling causes blockage of lacrimal duct, tears can’t drain so pours out the eye) |
|
|
What is Opthalmoplegia? What are we concerned about if we see this? |
muscles of eye movement don’t fxn -cant move the eye up/down. Usually rectus muscle involved. We are concerned that infection is on the lid and also in the eye= more severe!. Concerned patient may lose eye, go back into cavernous sinus to cause meningitits and brain abscess |
|
|
What is Mydriasis? |
Dilated pupil |
|
|
What is diplopia? |
Tearing can cause blurriness (so blurriness isn’t the best marker of eye signs) -Diplopia is when they see double, this is concerning bc muscles of eye affected (can’t focus eyes) -PNS and SNS nerves can be affected |
|
|
What are we concerned about when we lose the field of vision (ie. the peripheral vision)? |
Concerned because the optic nerve is affected |
|
|
What eye signs suggests that the optic nerve has been compromised? |
Loss of visual field Loss of color vision Loss of vision |
|
|
How can infection in the canine space lead to Loss of consciousness? |
canine space → abscess → edema to preseptal space to superior + inferior eyelids → LOC |
|
|
Common sequelae of dental extractions? |
-pain, swelling, bruising (non-extensive), trismus (stiffness, esp if mandib teeth) |
|
|
What some complications with dental extractions? |
-bleeding (bleeding when they go home), infection, paresthesia (numbness beyond LA), fractures |
|
|
healing stages post extraction? |
-Exo → clot → inflamm → granulation → ossification → normal healing |
|
|
What is the end product of the factor cascade? |
Fibrin (Factor I) |
|
|
Christmas Disease is characterized by deficiency of which factor? |
Factor IX |
|
|
What is the most common reason for Vitamin K deficiency? |
Small Intestine issues (other wise it's hard to be vit K deficient) |
|
|
What pathway does PTT look at? |
intrinsic pathway |
|
|
What pathway does INR look at? |
Extrinsic pathway |
|
|
What are some things that affect platelets? |
ASA Thrombocytopenia (low platelets) |
|
|
What are the platelet count cut offs for surgery? |
<50,000 elect not to do minor surgery <100,000 elect not to do major surgery |
|
|
What is the hierarchy of bleeding risk? |
0) no risks, normal bleeding i) Taking ASA - personal operator preference if you keep them on ASA or not ii) Coumadin w good control -Normal control: 2.5-3.5 (for stroke, afib) iii) Coumadin w poor control iv) Poorly controlled hemophilia |
|
|
What are some alterations you can make to the treatment plan for a patient with increased risk of bleeding? |
Remove less teeth, factor transfusion, platelet transfusion or refer |
|
|
How do you recognize there is a bleeding problem? |
Prolonged oozing (still oozing from socket 3 days later) -Fragile clots -Mechanical trauma to operative leads to bleeding of the socket (brushing) -Liver clots |
|
|
What is a liver clot? |
It's a collection of factors +platelets but has no useful function for coagulation. |
|
|
What is the tx for a liver clot? |
re-start coagulation cascade: suction + gauze; remove liver clot!!!! -Then find the socket, currette out any liver clot in there -If pt is healthy, they can bite on gauze + re-start (liver clot won’t necessarily re-form) -If pt is compromised, can put gel-foam |
|
|
What are 3 staples to treat any kind of bleed? |
Debride Pressure +/- Suture |
|
|
How does topical thrombin work? and what are the steps to use it? |
doesn’t rely on exrinsic or intrinsic pathway -Starts at common point (bypasses the beginning) -Dumps in thrombin to initiate clot (thrombin turns fibrinogen → fibrin = clot) i) Reconstitute w saline (thrombin is a dust particle, mix it w saline) ii) soak gel-foam w thrombin sol’n iii) plug socket quickly; gel-foam gets soggy quickly! iv) suture in place w figure 8 to prevent gel-foam from falling out |
|
|
What do you do when you have uncontrollable bleeding? |
Temporize (pressure) + get hematology consultation |
|
|
Why can smoking cause infections? |
-Smoking → vasoconstriction (less blood flow, less able to fight infexn) → chemicals poison your WBC, they don’t work as well → carbon monoxide in the smoke means your circulation carries less O2 |
|
|
What happens during dry socket? |
-Fibrin breaks down, clot dissolves, can get dry socket- not a true infection |
|
|
T/F: Tx for dry socket is antibiotics. |
F. Will be ineffective because it's not really a infection. |
|
|
S &S of dry socket |
Signs: None. Looks like a normal healing socket! Symptoms: Lots of pain with some granulation tissue |
|
|
Tx for dry socket? |
i) debride: curret the bottom of the socket to restart the bleed. ii) Sedative dressing (alvogyl) iii) Analgesics |
|
|
How soon should the patient expect pain relief after treating the dry socket? |
5-10 minutes after placing in the alvogyl. Pain continues to decrease 1-2 days later |
|
|
What is a sub-periosteal abscess that occurs after a extraction? |
Hard swelling, some tenderness, no pain but there is a gum boil at the site of the socket. Caused because there was debris during the extraction. Patient does not experience much pain. |
|
|
Tx for Sub-periosteal abscess |
1) Inision and drainage right down to the bone! 2) Culture +sensitivity (not if 1st time) 3) Antibiotics 4) Analgesics 5) Follow up |
|
|
Tx for Chronic Osteomyelitits? |
1) Long term antibiotics (6 weeks, up to 6 months! Oral or IV) 2) Sequestrectomy (remove sequestrum/dead bone) or major resection (REFER) |
|
|
What are some iatrogenic causes for damaging a nerve? |
Instrument slip (fulcrum!) Bur misadventure Over-Zealous retraction Pushing on Canal |
|
|
What are the three classifications of Nerve injuries? |
Neuropraxia: mild (analogous to bruising) Axonotmesis: damage but nerve sheath maintained Neurotmesis: complete transection of the nerve |
|
|
Prognosis of Neuropraxia? |
Very good prognosis. Since axon +nerve sheaths are intact, the nerve block/tingling sensation returns to normal sensation within days & weeks |
|
|
What is Axonotmesis? |
Damage to nerve bundle but the sheath is maintained. There is degereration of axons distal to site of injury. Prognosis is moderate. Sensation retrurns 6 months -1year |
|
|
What is Neurotmesis? |
complete transection (loss of continuity betw axons + nerve sheath) -nerve response = proliferation of schwann cells, nerve buds, fibroblasts -results in amputation neuroma at end of peripheral nerve -prognosis: much poorer -partial recovery = if ends line up, nerve buds find connection -no recovery = permanent loss of sensation. >6-12 months |
|
|
What are the symptoms of Neurotmesis? |
Anaesthesia, Paresthesia and dysesthesia (pain) |
|
|
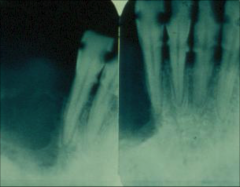
When assesing the lower 3rd molars and the relationship with the IAN, what 4 aspects need to be assessed? |
i. Overlap: do the root and canal overlap on the radiograph ii. Canal cortices: does the canal cortex disappear as the canal passes "over" the root iii. Tooth radiodensity: does the root darken or lose radio-opacity as the canalpasses "over" the root iv. Does the canal narrow as the canal passes "over" the root |
|
|
Ways to prevent damage to IAN? |
-Assess + ID incr risk -Normal caution: avoid lingual incisions, flaps, retraction -Precise surgery (prevent slippage, over-retraction, over-cutting) -Leave small root tips in situ if removal = risk of harming IAN -Refer if high risk |
|
|
How to manage IAN damage? |
Do IC beforehand Document -Reassurance -If not healed, Surgical intervention: Microsurgery, decompression, re-anastamosis, nerve grafting |
|
|
What is the most common cause of Jaw fracture? |
almost always due to excessive tensile or sheer Fs across superior border of mandible (3d M area) -Initiates the fx -Propagates along line of weakness (through 3d M socket, or canine root area) (ie using straight elevator to elevate 3rd Molar distally and occlusally OR if there was an extraction of 3rd molar and patient then experiences trauma which damages weakened area) |
|
|
Approximately how much time after 3rd molar extraction does the risk of jaw fracture return to normal? |
after 2 months |
|
|
What are the 2 classifications of Jaw fracture? |
-DISPLACED: operation req’d (moves w muscle pull) -NON-DISPLACED: operation may or may not be req’d (soft diet may be enough to manage) |
|
|
What are some risk factors that increase risk of Jaw fracture? |
-Depth of impaction -Density of Bone -#, Size and complexity of roots -Pre-existing pathology -Atrophy of jaw (i.e elderly) |
|
|
Things you can do to prevent jaw fracture? |
Don't remove excess bone Avoid heavy elevation with large elevators refer if high risk |
|
|
What are some things to help you dx jaw fracture during exo? |
suspect if large crack sound during exo, then loosening of resistant tooth -Pain may not be felt (2ndary to LA) -Inspect exo site; shows # through socket (may see fx line through exo socket) -Malocclusion if displaced (pt’s bite will be off) -Confirm dx w radiograph (ex PAN) |
|
|
Management of Jaw Fx? |
Prevent! IC Non-displaced: Soft diet + follow-up Displaced: OMFS |
|
|
High risk sites for Jaw fracture? |
Canines and lower 3rd molars |
|
|
What are 2 tx that OMFS can do for jaw fractures? |
ORIF: Open reduction, internal fixation (plates and screws) IMF: Intermaxillary fixation (wire jaw shut) |
|
|
Cause of Sinus perforation? |
Often iatrogenic (overzealous instrumentation) -Could be pre-existing with infected teeth -Can occur post-op (sneezing/nose blowing) |
|
|
What is the most common teeth that Sinus perforation is associated with? |
Upper 6 (but can occur with all posterial teeth) |
|
|
Different Classifications of Sinus perforation |
-ACUTE OVERT ORAL-ANTRAL COMMUNICATION: opening obvious at surgery -LATENT ORAL-ANTRAL COMMUNICATION: antral lining has broken down, reveals a bony opening -ORAL-ANTRAL FISTULA: epithelial-lined tract (has been open at least 1 week) -CHRONIC ORAL-ANTRAL FISTULA W SINUSITIS: -Sinusitis = infexn of sinus. -Chronic reflux of fluids + inflamm, yields polyps on antral side -Oral fluids in, not out; leads to sinus infection (fluids go up but cant come down bc of polyp) |
|
|
Things to prevent sinus communication |
Assess and id risk -Precise -No heavy elevation and heavy luxation -No aggressive curretage -Suture sockets+ gel foam -Tips to patients: Try not to sneeze with mouth closed, no nose blowing, no straw, no smoke |
|
|
Signs and symptoms to help you Dx sinus communication? |
Bubbling in socket during exhale -Suction makes hollow sound in socket -GENTLE probing when suspicious finds no roof -Inspect roots and bone for antral mucosa -Confirm with Water's view -May have sinus infection post op |
|
|
Management of oral antral communication? |
At time of exo: 1) Gelfoam (acts as Root!) 2) Obtain primary closure (Buccal advancement, bone rongeurs) 3) Rx AntiB (Keflex-covers oral + sinus bact) and decongestant 4) Follow-up. May need vestibuloplasty (lose vestibule) Chronic oral-antral-fistula: managed by specialists |
|
|
Goal of Pre-prosthetic surgery? |
1) Restore best masticatory fxn + dental & facial aesthetics via comfortable tissue foundation to support the denture 2) Enlargement of denture-bearing area in attempt to provide stability for denture |
|
|
Three imaging techniques used in the Dx and Tx planning for pre-prosthetic surgery and their uses |
-PAN: overview screen for pathology, retained teeth/roots, anatomical restrictions (sinus, NVB) -Assess vertical component of alveolus (subjective assessment of bone quality) -Lateral ceph: assess anteroposterior position of jaws -CT: refined assessment of bone anatomy -qualitative assessment of bone volume -integrate w implant-planning software |
|
|
list some factors that best support and retain a denture |
→ Oral tissues free of significant dz → Proper jaw relationships in anteroposterior, vertical, transverse planes → Broad U-shaped alveolar bone, w parallel bony walls → abundant attached mucosa in denture bearing area → no osseous potruberances, exostoses, tori, undercuts → adequate vestibular death |
|
|
List muscles that interfere with dentures |
Genioglossus-affect lingual side Lower strap muscles (only with severe ridge resorption) Obicularis oris Mentalis |
|
|
If you want to exo teeth as part of pre-prosthesis, you want to limit the removal of _____ |
buccal plate |
|
|
Some ways to reduce the need for Buccal plate? |
Section teeth. |
|
|
Some situations where you would want to compress B/L after extraction? |
If there is excessive proclination of incisors. Squeeze to move the buccal plate back. |
|
|
When is a situation you don't want to compress B/L after extraction? |
If you want to maximize bone width for implants. Make a ridge knife edge increases bone resorption |
|
|
Indications for gingivoplasty, frenectomy? |
-for flabby ridge tissue/ high frena that interfere w denture support/ retention |
|
|
Why is it important to go subperiosteal for frenectomies? |
Even with removed muscle and periosteum intact will lead to recurrence of frenum. So take out periosteum AND muscle |
|
|
Why is it important to undermine more from the palatal side when doing a tuberosity reduction? |
This will increase the amount of keratinized tissue in the end result. If you remove from the buccal (non-keratinized), your tuberosity will be covered mostly in mobile tissue. |
|
|
Why do you want to go subperiosteal for tori reduction? |
This allows the lingual nerve to stay in the mucosa, but the patient is still likely to have some neuropraxia |
|
|
When is a situation you may want to consider orthognathic surgery for a patient? |
When the maxilla has severely resorbed due to edentulism to the point where trying create lip protrusion with a denture will result in placement of anterior teeth off the ridge (which means poor retention). Orthognathic sx moves the anterior forward so the alveoli are in line where denture teeth should be |
|
|
List the 4 classifications of Behaviour |
Mild/ normal: behaviours = co-operative, approp Moderate: behaviours = mod anxiety, tears, squirming Severe: behaviours = marked anxiety, sobbing, hand/head movements Extreme: behaviours = overwhelming anxiety, crying, sitting, standing, is combative |
|
|
What are some methods to deal with behaviour issues |
Shorter appts Pre-meds: Sedatives (benzo) Intra-op sedation: nitrous, IV -GA -Refer |
|
|
What is the normal interincisal opening? |
40-65mm |
|
|
List the levels of difficulty with respect to interincisal opening: |
1) 35-40 2) 30-35 3) 25-30 4) <25 |
|
|
List some things that can cause trismus |
Infection Myofacial pain (from severe bruxism) TMJ pathoses Coronoid Hyperplasia Tumors (Primary or metastatic) -Scarring 2ndary to submucous fibrosis |
|
|
List the levels of difficulty with respect to posture
|
1) Neck stiffness: can adjust head-rest, or use a pillow… would be ok 2) Wheelchair bound, orthopnea (can’t lie flat) 3) Torticollis: fully turned to one side, can’t turn the other way (due to severe contraction of SCM) 4)Athetoid movements (in cerebral palsy) = trashing around |
|
|
You observe indentation of the sinus by roots of the 6s on a PA. What other type of imaging can you use to confirm that the roots are close to the sinus? (Other than Cone beam CT) |
PA (Can be taken at different angles) |
|
|
What is the threshold of radiation after which a patient is at risk of getting ONJ? |
5000 |
|
|
T/F: The greater amount of time that has passed since the Radiation therapy, the smaller the risk of ONJ |
False. Risk increases with time! (Cells get lazier with time) |
|
|
What is a possible preventative procedure to decrease risk of Radiation related ONJ (RONJ)? |
Hyperbaric Oxygen chamber (20 sessions pre op, 10 sessions post op) |
|
|
Rationale behind Hyperbaric Oxygen chamber. |
Actually might not do anything. In fact can do more harm than good. -This is when you are pressurized (2 atm at pressure) w 100% O2 -theoretically more O2 pumped, more O2 diffused from vessels to bone -bone more vasc, more likely to heal |
|
|
Risks with Hyperbaric oxygen chamber
|
may get blurry vision, cataracts, glaucoma -not good if pt only has 1 lung…. -Also very costly |
|
|
Other treatments other than hyperbaric oxygen to minimize risk of ONJ on a patient with radiation? |
Minimally traumatic surgery, primary closure perioperative Abx |
|
|
List the levels of difficulty with respect to Dental factors |
1)Posterior teeth 2) Fragile adj teeth 3) Malposed or submerged teeth: more submerged - worry about jaw fx! 4) Impacted teeth: ex Cleidocranial dysplasia = multiple supernumerary impacted teeth |
|
|
List the levels of difficulty with respect to Anesthestic Factors |
1) Normal response 2) Mild infexn: may have to do infiltration higher up, or do a block -Ex infraorbital block for ant max teeth -Ex for lower molars, may need to block nerve to mylohyoid (if still feeling after reg block) 3)Moderate infexn or hx of difficulty 4)Severe infexn or hx of major difficulty |
|
|
What are some ways to manage cases where you're having trouble obtaining anesthesia? |
-Change technique (block or infiltrate) -Tx infection first! -Refer for sedation or GA -Tough it out (as unpleasant as it is for you, harder on pt!) |
|
|
List the levels of difficulty with respect to Bone factors (levels of bone loss) |
1) Severe bone loss (>75%) = easier exo 2) Mod bone loss (35-70%), but if dense, may be harder than normal bone levels 3) Mild (<25%) 4) Normal bone levels, but if you lose the crown → considered higher bone level = harder exo |
|
|
List the levels of difficulty with respect to Bone Density |
1) Osteoporotic bone: look for contrast (see lower density) 2) Normal density 3) Focal sclerotic areas/ small exostoses 4) Generalized sclerotic bone/ large exostoses |
|
|
List the levels of difficulty with respect to Crown Factors |
1) Intact crown or small resto 2) Moderate caries (loss <25% = avg MOD resto) 3) Advanced caries (25-70% tooth loss) =large 4) amalgam or crown Caries to bone level |
|
|
What is severe attrition usually associated with? |
Exostoses. Combined with the small crown makes extractions difficult |
|
|
List the levels of difficulty with respect to Root Factors |
1) Single straight root 2) Multiple convergent roots or endo tx 3)Mild dilacerations/ mild hypercementosis/ multiple parallel roots 4) Marked dilacerations / marked hypercementosis/ multiple divergent roots, or ankylosis -Think about sectioning the tooth |
|
|
Key ideas that will help you manage difficult extractions |
Access= approp retraction of cheeks, tongue, flap -Presurgical 3D mapping of tooth and anat -Plan flaps, bone removal, sectioning -Proper instrument use -Practice -Approp referral |
|
|
List the 5 factors that are used to categorize the difficulty of any extraction |
systemic factors 1-4 pt management 1-4 local considerations 1-4 bone factors 1-4 tooth factors 1-4 |
|
|
Differentiate between acutely traumatic, infection and cancerous in terms of timelines |
Acute: lesion present over days Infection: Days to weeks Cancerous: Present for months |
|
|
DDx you should think of when you see a gingival lump on Buccal alveolar ridge? |
-If bilateral, think exostoses -If unilateral, exostosis still on ddx, but not your #1 -think more along lines of epulis (fibroma would be #1) |
|
|
DDx you should think of when you see a large lump on tongue |
-Depending on hx of trauma.. . -If present since birth - think hemangioma |
|
|
DDx you should think of when you see mucosal changes (tongue or cheek)? |
-Typical lesion on tongue w white border ; ask pt if it changes in position, if multiple -likely geographic tongue -if they just finished a course of Abx, and they’re prone to fungal infexns, think atrophic candidiasis |
|
|
DDx you should think of when you see mucosal ulceration on the hard palate? |
-If pt ate something really hot - burn, won’t do much -If multiple lesions on face, arms… think along lines of vesicular bullous dz |
|

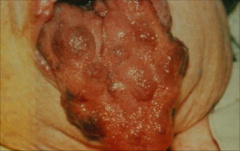
Dx? |
Verrucous Carcinoma. Thick, shaggy plaque that can easily confused with hyperplasia |
|
Dx? |
Hemangioma |
|
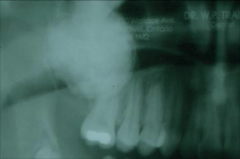
Ddx? |
Presence of a follicle structure..liked a complex odontoma, or a Osteoma |
|
|
Signs and Symptoms that make you think you are dealing with a abnormal lesion |
Swelling, bleeding, Numbness, Metastasis, Color change Loss of function |
|
ddx? |
Not regular pDz. Rarely ever goes that apical like this. Ddx: SCC, Histiocytosis X, Central giant cell granuloma |
|
|
Features of Cancer |
Growth Invasion Metastasis Abberations in: Cell division and adhesion. |
|
|
Features of Infection: |
Pain, Swelling, Fever Production of toxins and host responses Hx: Pain, Rapid swelling, Cavity, post-op, wound or impaction. |
|
|
Typical Hx of Cancer |
Hx: Painless(Can be painful), slow growing with interference in function |
|
|
Clinical presentation of Cancer
|
Ulceration (alone is not cancer) Rolled margins Color Change Deep invasion or metastasis Lack of well defined borders |
|
|
Clinical presentation of Infection |
-induration or fluctuence -Tenderness/heat -purulence -source |
|
|
Generally, what are the principles for taking a incisional biopsy? |
1. Include Abnormal tissue (include both erythroleukoplakia and leukoplakia in the same sample if possible) 2. Include some normal tissue (Only in really specific situations!) 3. minimal Damage to sample |
|
|
Why do you not want to include Normal tissue in a incisional biopsy if you suspect the lesion to be carcinoma or dysplasia? |
may alter the margins with the biopsy (spreading the cells)-take biopsy throughmiddle of the tumor (go deep) to see how much invasion there is. |
|
Why do you generally want to take incisional biopsies in the shape of an ellipse? |
It allows the biopsy site to be closed in a straight line. |
|
|
What is the general pattern for a excisional biopsy? |
|
|
|
How do you excise a mucocele? |
1) Give LA Depends on how long the patient has had the mucocele.. Chronic for years: Need to make excision to biopsy because of scar tissue. Ellipse over top of mucocele, undermine, cut around it and excise. Fresh: Just pop with pinching |
|
|
What is critical to do during removal of an existing mucocele to make sure you don't have recurrence? |
make sure you didn't damage adjacent minor salivary glands |
|
|
What is a unique surgical technique is used specifically to treat large KOTS? How does it work? |
Marsupialization (make incision and put a drain in).Normally KOTs enlarge thanks to the keratin shreds in the middle. Keep the drain in to evacuate keratin and reduce pressure. This shrinks the KOT. This allows you to remove KOT without damaging adjacent structures. The lining of KOT also becomes scarred due to chronic inflammation of drain which again helps removal. |
|
|
Does the marsupialization help shrink Daughter KOTs as well? |
No. Only acts on Central KOT. The daughter KOT may require additional marsupialization |
|
|
How long does a KOT/Ameloblastoma need to be monitored for after removal? |
5-10 years at least. Recurrence! |
|
|
Patient on Coumadin with INR 2.5. Do you anticipate a lot of bleeding? |
Still could bleed significantly! INR is not reliable! |
|
|
What does Pradaxa/Equilis target? What is the bridging options for this medication? |
Factor 2. NO bridging options |
|
|
What does rivaroxaban target? Why is it gaining popularity? |
Factor X. (anything with "xaban" inhibits factor X) -Only need to take 1x a day anytime, no measurements, diet not complicated |
|
|
What is the issue for us dentists with rivaroxaban? |
It's irreversible! |
|
|
What are some decisions that help guide you if the patient should come off rivaroxaban? |
-if 3 or less teeth, dont need to reverse pt’s meds but also take into account complexity -if 3/more, or more bleeding (tori reductions, tongue release)... -discuss w MD about coming off the anti-coagulant |
|
|
Patient claim they are allergic to LA because they get faint/sweaty/LOC or palpitations/flush. Is it a true allergy? What likely happened at that appointment? What can you do to further verify the claim? |
Most likely the injection went IV. Get the patient to see MD to work up allergies |
|
|
What are some options to manage a patient with a true allergy to LA/epi |
refer benadryl (intramucosal injection may work) can do GA or nitrous |
|
|
Why might it be a good idea to refer a patient who report multiple chemical sensitivities? |
Patients are likely manic, have high expectations. |
|
|
Patient have history of malignant hyperthermia. What are some known triggers? |
GA, succinyl choline (paralyzing agent for GA) |
|
|
What is a tx for malignant hyperthermia? |
dantrolene (have this in your office!) |
|
|
is N2O or LA a risk factor for malignant hyperthermia? |
No. |
|
|
Patient has hemophilia. What needs to be given to them before you do any procedure |
Factors by nurse/MD |
|
|
What is the risk of giving LA to patient who report having taken cocaine in the last 48 hours |
-if you then give LA (intravascularly) = epi → over-stressed -can go into severe vasoconstriction, ischemic stroke, myocardial ischemia, severe HTN -if you suspect pt is on cocaine, don’t give LA w epi. Generally. Don't tx patients who are high |
|
|
any risks to txing patient who smokes marijuana? |
Not really. Make sure they comprehend IC. Ask them to repeat it back to you |
|
|
For leukocytes, under which value would you not treat? |
1 |
|
|
For neutrophilss, under which value would you not treat? |
<0.5. Definitely don't do it <0.1!!! |
|
|
What test is used to measure Heparin? |
PTT |
|
|
Why shouldn't you use nitrous for a patient with COPD/emphysema? |
It expands lungs and can cause lungs to burst |
|
|
What two factors need to be present in order for proper blood clotting to occur? |
Fibrin and Platelet aggregation |
|
|
What are some things that can impair the production of bleeding factors? |
Hemophilia liver disease Vitamin K deficiency Drugs (Warfarin) |
|
|
What are some factors that can impair the proper function of platelets? |
ASA Thrombocytopenia |
|
|
What are the 3 types of post operative infections? |
Early-acute fibrinolytic (dry socket) Intermediate-Acute suppurative Delayed- Chronic Suppurative |