![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
22 Cards in this Set
- Front
- Back
|
White Lesions: What Causes Them? |
* Hyperkeratosis - Thickening of the horny layer of the epidermis or mucosa by increased keratin production which turns white when hydrated by saliva. * Necrosis of epithelial cells - Usually caused by an injury * Ischemia - Defective blood supply to the tissue |
|
Variations of Normal: Fordyce Granules |
* Normal Sebaceous glands found in the oral mucosa * Found in 80% of the population * Not found in children - sebaceous glands form at puberty. |
|

Variations of Normal: Leukoedema |
* Intracellular edema and tissue whiteness. * More common in African Americans. * Buccal Mucosa appears wrinkled * Does not rub off - disappears when stretched. |
|

Traumatic and Inflammatory: Geographic Tongue |
* aka Benign Migratory Glossitis * Rarely seen i nchildren. * More common in females in early to mid-adulthood * Cause of inflammation unknown * Appears as de-papillated area * Treated w/ corticosteroids |
|

Traumatic and Inflammatory: Frictional Keratosis |
* Physical irritation of oral mucosa produces keratin as protection against injury. * White plaque that does NOT rub off. * Not considered Leukoplakia because cause is known and does not become malignant lesion |
|

Traumatic and Inflammatory: Check Chewing |
* aka morsicatio buccarum and morsicatio labiorum * Location on lip or at the occlusal plane helps w/ diagnosis * Can be found on the tongue * Pt should be discouraged from habit |
|
Traumatic and Inflammatory: Nicotine Stomatitis |
* Keratotic change of palate mucosa by heat from smoking or chronically drinking hot fluids * Heat and irritation produce keratosis and irritation of minor salivary gland ducts on palate (red ducts) and edema (white/raised rings) * May lead to carcinoma |
|
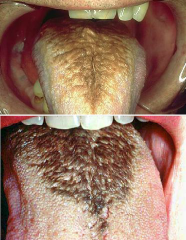
Traumatic and Inflammatory: Hairy tongue |
* Etiology Unknown * Can be white, black or brown * Elongation of filiform papillae w/ hair-like appearance * Brush tongue or use rinse (i.e. chlorhexidine) * Risk Factors: Antibiotics, Therapeutic radiation, Smoking, Oxygenated Mouthrinse, Overgrowth of oral flora |
|
Infections: Candidiasis. |
* Not in healthy people * Predisposing Factors: Systemic broad-spectrum antibiotic therapy, Corticosteroids, Smoking, Xerostomia, Systemic Disorders, Diabetes, Immune Function Disorders. |
|

Infections: Acute Pseudomembranous Candidiasis |
Candidiasis, Thrush * White plaque that CAN BE RUBBED OFF * Treatment: Nystatin oral suspension or glotrimazole croches or systemic fluconazole * Organisms grow on mucosa and produce necrosis of superficial keratinocytes - dead cells lie on surface as white plaque due to hyphae (elongated form) of organism* |
|

Infections: Chronic Hyperplastic Candidiasis |
* Rarest form * very low risk of malignant transformation * Thickened, raised, Whitish plaque that does NOT rub off * Affects tongue, commissures, mucosa * INDISTINGUISHABLE FROM LEUKOPLAKIA * Systemic anti-fungals to treat * Only candidiasis that shows malignant potential. |
|

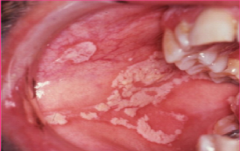
Infections: Hairy Leukoplakia |
* Infection of Ebstein Barr virus secondary to immunosuppression * Predictor of rapid progression - Latent HIV to AIDS * Whitish plaques of raised vertical ridges that do NOT rub off, usually on lateral borders of tongue. * Biopsy to diagnose * Antifungal to treat |
|

Infections: Parulis |
* Swelling of the gingiva * Caused by draining of sinus tract from an odontogenic infection of periodontal or pulpal origin. Listed as white because purulent exudate is seen clinically as yellow or white. |
|
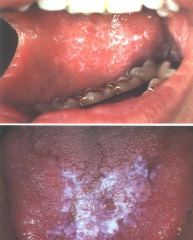
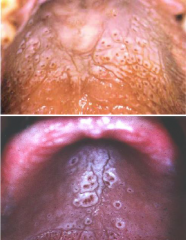
Immune System Disorders: Lichen Planus |
* Immune-mediated mucocutaneous disorder * T-lymphocytes recruited to skin damage epithelium * Wickham striae (lacy pattern) on buccal mucosa, usually bilaterally; gingiva (Koebner phenomenon), or tongue * No treatment needed unless change/growth * Suspicious for malignancy if erosive |
|
|
Koebner Phenomenon |
* aka isomorphic reaction (in same form) * Most widely known phenomena in dermatology * First described by Heinrich Koebner (1872) * Some patients had developed psoriasis at site of excoriation (abrasion from scratching), a horse bite, or a tattoo. * usually describes response where new lesions develop on healthy skin that has suffered trauma in patients with skin conditions * Pt w/ psoriasis + trauma to healthy skin = new lesion resembling psoriasis lesions |
|

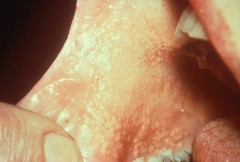
Immune System Disorders: White Sponge Nervus (WSN) |
* RARE - inherited mutation of certain keratin genes * usually apparent in childhood * widespread keratinization of buccal and labial mucosa * Lesions do NOT rub off * affect buccal mucosa folds - help in diagnosis since you can not bite buccal folds * no treatment needed |
|

Immune System Disorders: Leukoplakia |
* Most common form of premalignant lesion * " White patch or plaque... does NOT rub off... can not be diagnosed clinically or pathologically as any specific disease" * Diagnosis by exlusion of other conditions * Frictional keratosis should not be mistaken for leukoplakia because leukoplakia is premalignant and frictional keratosis is not. * Highly variable in size, shape, and location (any mucosal surface) * Usually single and soft when palpated, some may feel leathery (degree of keratinization) * Firm indurated mass indicates malignancy * ventral tongue and floor of mouth (HIGHEST RISK AREAS) show more microscopic evidence of premalignancy or malignancy * arises from microscopic mutations of epithelial cells following exposure to carcinogens * 20% likely to become invasive * Treatment includes eliminating risk factors (smoke/smokeless tobacco cessation), or surgical/laser removal w/ follow up observations *other risk areas influde: lateral tongue, retromolar trigone, lateral soft palate, and lower lip from sun exposure (actinic cheilitis) |
|

Immune System Disorders: Speckled Leukoplakia |
* Exhibits both red and white components * May have redness, ulceration or pebbly appearance * appears on lateral borders of tongue |
|

Immune System Disorders: Proliverative Verrucous Leukoplakia |
* Aggressive * High incidence of oral canver * progressive * Tendency to form on gingiva where associated w/ greatest potential for malignant transformation. * biopsy should be performed to look for epithelial dysplasia, representing malignant change |
|

Immune System Disorders: Smoking-Related Leukoplakia |
* Most important etiologic factor is tabacco (smoked and smokeless) * 50% of leukoplakias in smokers will resolve with smoking cessation and over 95% of smokeless tobacco will will resolve * Lesions are painless and persistant |
|

Immune System Disorders: Leukoplakia of the Lower Lip |
* aka actinic chelitis * Related to chronic sun damage * Atrophy of vermillion border * erosion and crusted appearance |
|

Immune System Disorders: Oral Submucosal Fibrosis |
* Areca nut or betel nut chewing * Genetic predisposition and genetic mutation * Generalized stomatitis that develops numerous vesicles and ulcers * Second tissue develops white thickening of tissue * Third stage is formation of premalignant leukoplakia lesions in about 25% of cases * NO treatment. Pt should stop chewing betel nut. |