Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
267 Cards in this Set
- Front
- Back
|
write the 4 principles of Osteopathic Philosophy
look for 4 blank lines... |
The body is a unit; the person is a unit of body, mind, and spirit
The body is capable of self-regulation, self-healing, and health maintenance Structure and function are reciprocally interdependent Rational treatment is based upon an understanding of the basic principles of body unity, self-regulation, and the interrelationship of structure and function |
|
|
define somatic dysfunction
|
the impaired or altered function of related components of the somatic (body framework) system
|
|
|
the therapeutic application of manually guided forces by an osteopathic physician to improve physiologic function and/or support homeostasis that has been altered by somatic dysfunction
|
OMT
|
|
|
define Facilitation:
|
the maintenance of a pool of neurons in a state of partial or sub threshold excitation ; in this state, less afferent stimulation is required to trigger the discharge of impulses
|
|
|
what is TART
|
Tissue texture abnormalities
Asymmetry Restriction of motion Tenderness |
|
|
what are the 3 motion barriers? define them..
|
Anatomic: the limit of motion imposed by anatomic structure; the limit of passive motion
Physiologic : the limit of active motion Direct: may also see it called the restrictive barrier; a functional limit that abnormally diminishes the normal physiologic range |
|
|
define how you would perform counterstrain
|
Find and label tender point 10/10
Position to relieve tenderness (2/10 or less) Fine-tune to 0/10 if possible Hold position for 90 seconds (some schools teach 120 seconds for the ribs) Slow passive return to neutral Retest tender point |
|
|
define how you would apply MFR
|
Diagnose restricted motion
Slowly move into position of laxity and follow release until completed (indirect) Slowly move into restriction and stretch until tissue give completed (direct) Retest motion |
|
|
what is unique in ME?
|
requires pt activity
Diagnose restriction Move into restrictive barrier Isometric contraction 3-5 seconds Stretch until give stops Repeat 3-5 times Retest motion |
|
|
define traction, kneading, inhibition, effleurage, and petrissage
|
Traction – longitudinal muscle stretch
Kneading – lateral muscle pressure Inhibition – sustained muscle pressure Effleurage – stroking pressure to move fluid Petrissage – squeezing pressure to move fluid |
|
|
give the acute vicerosomatic findings for
temp tissue texture red reflex |
hot
Moisture, fullness, edema, tension Increased or prolonged redness |
|
|
give the chronic vicerosomatic findings for
temp tissue texture red reflex |
cool
thickness, dryness, ropiness, pimples prolonged blanching |
|
|
write out the autonomic chart
|
|
|
|
where is the chapmans point for the appendix
|
tip of the 12th rib
|
|
|
what is the difference btw a chapman's point, counterstrain, and triggerpoint
|
Chapman’s point: viscerosomatic reflex
Conterstrain point: locally tender Trigger point: referred pattern of pain, motor dysfunction, autonomic phenomenon |
|
|
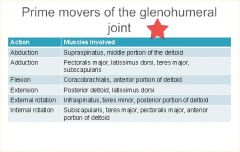
what are the rotatorcuff muscles?
|
supraspinatus, infraspinatus, teres minor, subscapularis
**SItS*** |
|
|
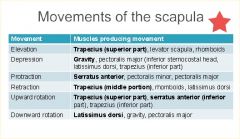
movements of scapula
|
|
|
|
The ulnohumeral joint moves in what direction with flexion/extension?
what will this do to the carrying angle |
The ulnohumeral joint passively ADducts with flexion and passively ABducts with extension
This cause the hand to deviate to the mouth during flexion -It is also responsible for the carrying angle |
|
|
describe ulnar abduction
|
Restricted adduction (lateral glide)
Patient may present with pain or restriction at endpoint of flexion Increases the carrying angle |
|
|
describe Ulnar Adduction
|
Restricted abduction (medial glide)
Patient may present with pain or restriction at endpoint of extension Decreases the carrying angle |
|
|
With a posterior radial head somatic dysfunction: (give ease and restriction)
how does this normally occur |
Ease of motion is posterior glide = PRONATION
-Restricted motion is anterior glide with SUPINATION** A posterior radial head somatic dysfunction is often caused by a fall forward onto an outstretched hand*** |
|
|
what are thoracic outlet syndrome, carpal tunnel, and double crush syndrome
|
Thoracic Outlet Syndrome
Pain and/or paresthesia in the upper extremity from brachial plexus compression Neural compression is more common than vascular compression Carpal Tunnel Syndrome Median nerve compression in the carpal tunnel associated with numbness, and pain in the arm and hand along the median nerve distribution Double Crush Syndrome mixture of above |
|
|
what is the Scalene compression test (Adsons maneuver)? shows the pt has?
|
Positive test = diminished pulse and/or reproduction or exacerbation of symptoms
Thoracic Outlet Syndrome |
|
|
Patient usually complains of pain of the palmar surface of the thumb, index and middle finger
|
Carpal tunnel syndrome
Compression of the median nerve within the carpal tunnel |
|
|
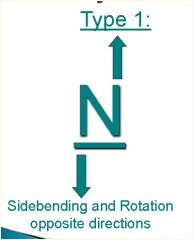
describe fryette type I
|
Law I = when the spine is in neutral (easy normal), sidebending and rotation are in opposite directions. (Type I Mechanics)
Occurs in neutral (facets not engaged) Found in thoracic and lumbar spines Forms long curves, multiple segments Compensatory |
|
|
describe fryette type II
|
Law II = when the spine is flexed or extended (non-neutral), sidebending and rotation are in the same directions. (Type II Mechanics)
Occurs in flexion or extension Facets engaged Occurs in thoracic and lumbar spines Type II-like motion in cervical spine Usually single segments Found at apices and crossovers and/or sites of viscerosomatic reflexes Primary somatic dysfunction Due to strain or viscerosomatic reflex |
|
|
describe fryette law III
|
Law III = when motion introduced in one plane it modifies (reduces) motion in other two planes
When a segment is brought up to a restrictive motion barrier it will move in the position of greatest ease in the other two planes. Restriction = direction it won’t go. Somatic dysfunction = defined by direction it will go with ease. |
|
|
flip for examples of t1 and t2 s/d
|
|
|
|
ant lumbar counterstrain points
|
Occur in 2 sets
Midline (T9-T11) Along the ilium (T12-L5) L2, L3, and L4 are all clustered around the AIIS and are differentiated by the direction in which you push Treated in similar manner |
|
|
what are the key fascial diaphragms?
|
Pelvic diaphragm (L5-S1)
Thoracic diaphragm (T12-L1) Thoracic inlet (T1, 1st rib) Suboccipital region (OA, AA) |
|
|
diaphragm compensatory patterns
|
|
|
|
Patient presents with a positive left standing flexion test. Left ASIS is cephalad. Left PSIS is cephalad. What is pelvic diagnosis?
|
Left superior Innominate Shear
|
|
|
Patient has positive ASIS compression test
on the left. Both left ASIS and left PSIS are caudad. What is your diagnosis? |
Left inferior innominate shear
|
|
|
Positive Standing tests on the left. Positive ASIS compression test on the left. What does this tell you? Left ASIS caudad. Left PSIS cephalad.
What is the diagnosis? |
Left Anterior Innominate rotation
|
|
|
Positive Standing test left. Left ASIS is cephalad and left PSIS is caudad
What is the diagnosis? |
Left Posterior Innominate Rotation
|
|
|
Positive ASIS compression test on right. Right ASIS closer to midline relative to left. What is the diagnosis?
|
Right innominate inflare
|
|
|
Positive ASIS compression test left. Left ASIS further from midline relative to right. What is your diagnosis?
|
Left innominate outflare
|
|
|
during inhalation, how does the sacral base move
|
sacral base goes posterior
this is the S1 axis |
|
|
during cranial flexion, how does the sacral base move
|
Cranial Flexion→Sacral base extends/ counter-nutates/posterior
Cranial Extension→ sacral base flexes/nutates/ anterior |
|
|
what does a positive spring test show you?
negative? |
Lumbar Spring Test
**Positive Test** Resistance to springing→ sacral extensions (ie LUE) or backward rotation on oblique axis (ie L on R) **Negative Test** Ease of Springing→sacral flexions (ie LUF) or forward rotation/torsion (R on R) |
|
|
what does a pos/neg backward bend test show you?
|
**Positive Test**
increased sacral base asymmetry → sacral extensions (ie LUE) or backward rotation on oblique axis (ie R on L) **Negative Test** decreased sacral base asymmetry → sacral flexions (ie LUF) or forward rotation or torsion (ie L on L) |
|
|
Patient presents with sacroiliac pain. She has a positive seated flexion test on the right. She has a negative spring test. L2-5 are NRRSL. The right sacral base is anterior and the Left ILA is posterior. What is her sacral diagnosis?
|
Seated flexion test positive on Right:
-Right SI joint is restricted and has -Left oblique axis if engaged Negative spring test: L/S junction can flex, ie forward rotation L5 rotated right: Sacrum rotates left L5 sidebent left: Left oblique axis Right base anterior Left ILA posterior What is your diagnosis? *** Left on Left Sacral Torsion*** |
|
|
Seated flexion test positive on left. Negative backward bending test (findings become more symmetrical). L3-5 are NRLSR. Assuming physiologic motion between lumbar and sacrum, can you give diagnosis?
|
Seated flexion test positive on left:
- Left SI joint is restricted and has - Right oblique axis if engaged Negative backward bending test (findings become less asymmetrical): sacrum can flex (ie forward torsion) L5 rotated Left: Sacral rotation right L5 is sidebent to right Right oblique axis Left base would be anterior Right ILA would be posterior What is your diagnosis? *** Right on Right Sacral torsion*** |
|
|
Seated flexion test positive on right with positive spring test. L5 is rotated left. The right sacral base is posterior and the Left ILA anterior. What is the diagnosis?
|
Seated flexion test positive on Right
Left sacral axis Positive spring test L/S junction is extended (can’t flex)→ backward torsion L5 rotated left: sacral rotation right on oblique axis Right base posterior Left ILA anterior What is the diagnosis? *** Right on left torsion*** |
|
|
Seated flexion test positive on left with positive spring test. L5 is FRS(R). Assuming normal mechanics, what is the sacral diagnosis?
|
Seated flexion test positive on left
Right sacral axis Positive spring test L/S junction is extended (can’t flex)→backward torsion L5 rotated right: sacral rotation left L5 sidebent right: Right oblique axis What is the diagnosis? ** Left on Right torsion** |
|
|
Seated flexion/ASIS compression test positive on Left.
Negative Backward Bending Test (findings become less asymmetrical) Left base is anterior and left ILA is posterior and inferior. What is your diagnosis? |
Seated flexion/ASIS compression test positive on Left
Left SI restriction Negative Backward Bending Test (findings become more symmetrical) - Sacrum prefers flexion Left base is anterior Left ILA posterior and inferior What does this tell you? Not a torsion What is your diagnosis? ***Left Unilateral Sacral Flexion*** |
|
|
tx for Left on Left Sacral Torsion (forward)
|
Forward Torsion Muscle Energy
-Pt lying on the axis side with the chest down on the table; -Flex the knees and hips until motion is felt at the lumbosacral junction, usually at least 90° hip flexion; Allow the legs to hang down off the table with thighs supported by your leg Monitor the anterior sacral base and ask the patient to push the feet toward the ceiling for 3-5 seconds against your equal resistance; Slowly move the legs toward the floor to a new restrictive barrier; Repeat 3-5 times or until return of sacral mobility; Retest sacroiliac motion or sacral symmetry. |
|
|
tx for Left on Right torsion
|
Backward Torsion Muscle Energy
Technique (lateral recumbent): - Sit or stand in front of the patient who is lying on the axis side with the upper back on the table; -Extend the leg on the table until motion is felt at the lumbosacral junction; Flex the top leg and place the foot behind the other knee; Hold the shoulder to prevent the patient from rolling and allow the flexed knee to hang down off the table; Ask the patient to push the flexed knee toward the ceiling for 3-5 seconds against your equal resistance; Slowly move the knee toward the floor to a new restrictive barrier; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
tx for Right Unilateral Sacral Flexion
|
- Stand facing the patient’s head on the side of the unilateral flexion;
-place your thenar or hypothenar eminence on the involved inferior lateral angle and push it anteriorly and superiorly by leaning into it; Use your other hand to slightly abduct and internally rotate the lower extremity on the involved side; While the patient takes a deep breath, push the sacrum into extension during inhalation and resist sacral flexion during exhalation; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
Seated flexion test positive on left with positive spring test. L5 is FRSR. Assuming normal mechanics, what is the sacral diagnosis?
|
Seated flexion test positive on Left
What does that tell you? Right sacral axis Positive spring test What does that tell you? L/S junction is extended (can’t flex) → backward torsion L5 rotated right: sacral rotation left L5 sidebent right: Right oblique axis What is the diagnosis? *** Left on Right torsion*** |
|
|
Seated flexion/ASIS compression test positive on Left.
Negative Backward Bending Test (findings become less asymmetrical) Left base is anterior and left ILA is posterior and inferior. What is your diagnosis? |
Seated flexion/ASIS compression test positive on Left
What does that tell you? Left SI restriction Negative Backward Bending Test (findings become more symmetrical) What does that tell you? Sacrum prefers flexion Left base is anterior Left ILA posterior and inferior What does this tell you? Not a torsion What is your diagnosis? **Left Unilateral Sacral Flexion** |
|
|
Seated flexion/ASIS compression
test positive on Left. Positive Spring test. Left base posterior (or right anterior) and Left ILA anterior (or right posterior). What is your diagnosis? |
Seated flexion/ASIS compression
test positive on Left: What does that tell you? Left SI restriction Positive Spring test: What does this tell you? L/S junction is extended (can’t flex)** Left base posterior (or right anterior) Left ILA anterior (or right posterior) What is your diagnosis? *** Left unilateral sacral extension*** |
|
|
tx for unilateral sacral extension?
|
Stand facing the patient’s feet on the side of the unilateral extension;
Place your thenar or hypothenar eminence on the involved sacral base, and push it anteriorly and inferiorly by leaning into it; Use your other hand to slightly abduct and internally rotate the lower extremity on the involved side. While the patient takes a deep breath, resist sacral extension during inhalation and ** push the sacrum into flexion during exhalation***; Repeat 3-5 times or until sacral mobility returns; Retest sacroiliac motion or sacral symmetry. |
|
|
what is normal rate and amplitude of CRI
|
Rate = cycles/min (10-14)
Amplitude = distance from flexion to extension (0- 5) |
|
|
how do unpaired and paired cranial bones move?
|
Unpaired bones move in flexion and extension.
Paired bones move in external rotation and internal rotation. Flexion of unpaired bones - external rotation of paired bones. Extension of unpaired bones - internal rotation of paired bones |
|
|
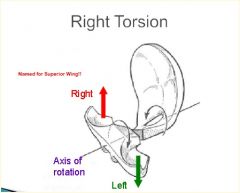
flip to see Conventions in naming cranial strain patterns
|
Torsions are named for the superior greater wing of the sphenoid.
Sidebending rotations are named for the side of head convexity. Sphenobasilar strains are named for the direction of basisphenoid movement (which is opposite to greater wing movement). |
|
|
define scoliosis
Two reversible causes of idiopathic scoliosis? |
Scoliosis is defined as a curve > 10°
Short leg syndrome with compensatory scoliosis (scoliotic posture) Trauma to the spine causing strain & resultant deformity in immature skeleton, if treated before skeletal maturity |
|
|
what are the most reliable Prognostic Indicators for scoliosis?
|
Most reliable
Future growth potential Age at diagnosis Menarche in females Risser sign Curve severity at diagnosis |
|
|
heel lift protocol? (short leg)
|
1/8 inch lift and lift at a rate no faster than 1/16 per week or 1/8 inch every 2 weeks
Fragile patients (arthritic, osteoporotic, aged, acute pain) 1/16 lift and lift no faster than 1/16 every 2 weeks Start low and go slow |
|
|
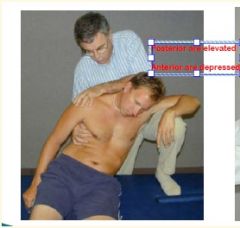
Mix & Match “Rib Basket”
Rib 1 Ribs 2-5 Ribs 6-10 Ribs 11-12 with the following: caliper motion bucket handle pump handle elevated or depressed subluxation inhalation or exhalation |
Rib 1: elevation/ depressed
Ribs 2-5: pump handle Ribs 6-10 :bucket handle Ribs 11-12: inhale/exhale |
|
|
What is the key rib?-
inhalation? Exhalation? |
What is the key rib?- refers to the rib in a group
Inhalation- the bottom rib is the key rib Exhalation- the top rib is the key rib |
|
|
Reminders on Sequencing Trx
|
First treat thoracic
type II, then type 1 Treat subluxed rib before a respiratory rib For a group of respiratory ribs, treat the key rib: top rib for exhaled ribs bottom rib for inhaled ribs may still have to treat individually |
|
|
Palpatory findings:
right ribs 2-4 exhalation dysfunction left ribs 5-9 inhalation dysfunction left rib 5 posterior rib subluxation T4-8 N S left R right T8 Flexed R left S left What is the sequence of treatment? |
in order:
t8 T4-8 N S left R right left rib 5 posterior rib subluxation then inhalation/exhalation |
|
|
50% of cervical flexion and extension occurs at the
50% of cervical rotation occurs at the |
50% of cervical flexion and extension occurs at the OA joint
50% of cervical rotation occurs at the AA (C1-2) joint |
|
|
please list C5-T1 DTRs/Strength test
|
C5 DTR-biceps, strength- biceps
C6 DTR-brachioradialis, strength- wrist extensors C7 DTR-triceps, strength- wrist flexors C8 DTR-none, strength- finger flexors T1 DTR-none, strength- interossei |
|
|
What are Rotation and Sidebending like in Fryette Type I's?
|
|
|
|
What does Fryette's 3rd law state?
|
when motion introduced in one plane it modifies (reduces) motion in other two planes
-When a segment is brought up to a restrictive motion barrier it will move in the position of greatest ease in the other two planes. |
|
|
Let's assume that the right facet on T8 is locked CLOSED...
When the patient extends you don't feel much change (no asymmetry).. What will happen when the patient flexes? |
During flexion, left facet will open...
Right facet is locked shut so T8 will rotate and sidebend TO THE RIGHT So, T8ESRr |
|
|
Let's assume the right facet of T8 is LOCKED OPEN...
What would you feel in flexion? What would you feel in extension? |
Right Facet LOCKED OPEN:
Flex: no asymmetry Extension: -Left facet closes fine -Right facet still locked open - Rotation and sidebending occur to the LEFT T8FSRL **FLEXED, OPEN, OPPOSITE** |
|
|
What do you treat first? Type I's or Type II's?
|
Type II
|
|
|
Type I vs. Type II
-Facets engaged |
Type II
|
|
|
Type I vs. Type II
- occurs at apices, crossovers and viscerosomatic reflexes |
Type II
|
|
|
For the Lateral Postural Exam:
Where are the 6 points the weight-bearing line should pass through? |

1) Just ant. to lateral malleolus
2) middle of tibial plateau 3) Greater Trochanter 4) Body of L3 5) Middle of humeral head 6) External Auditory Meatus |
|
|
a patient has a Right Hip drop < 25° (positive test)
Will have restricted lumbar sidebending to the ________ **** |
left
|
|
|
What is defined as An abnormal lateral curvature of the spine in the coronal plane.
|
scoliosis
|
|
|
A patient with scoliosis shows a right-sided "Rib Hump" when they flex down to touch their toes.
When you ask them to sidebend toward the right, the "Rib Hump" disappears. Is this Structural or Functional Scoliosis? |
Functional
|
|
|
A patient with scoliosis shows a right-sided "Rib Hump" when they flex down to touch their toes.
When you ask them to sidebend toward the right, the "Rib Hump" remains visbile. Is this Structural or Functional Scoliosis? |
Structural
|
|
|
What is the a common cause of Functional Scoliosis (rib hump disappears with same-sidebending)?
*** |
SHORT LEG SYNDROME
- Sacrum & pelvis tilt toward the shorter leg. - Spine curves back in attempt to keep eyes level. |
|
|
A scoliotic curve is always named for the direction of __________
|
|
|
|
What is the most common tpye of scoliotic curve?
|
Double Major (L & R)
|
|
|
Respiratory Impairment can occur in patients with thoracic scoliosis and a Cobble angle greater than ______
Cardiac Impairment can occur in patients with thoracic scoliosis and a Cobble angle greater than ______ |
Resp. = Cobb Angle > 50 deg.
Cardiac = Cobb Angle > 75 deg. |
|
|
If a Cobb Angle is less than 20 degrees, you can treat with ______
|
OMT
|
|
|
If a Cobb Angle is between 20-45 degrees, you can treat with OMT + ______
|
Bracing
|
|
|
If a Cobb angle is greater than 50 degrees, the patient needs ______
|
surgery
|
|
|
What are the 2 absolute contraindications to OMT?
|
-Absence of Somatic Dysfunction
-Patient Refusal |
|
|
You have a tenderpoint on the right ASIS as you push medial to lateral. What is the name of the Counterstrain Tenderpoint?
*** |
Right Anterior L2 Counterstrain TP
|
|
|
You have a tenderpoint on the right ASIS as you push lateral to medial. What is the name of the Counterstrain Tenderpoint?
|
Right Anterior L3 Counterstrain TP
|
|
|
You have a tenderpoint on the right ASIS as you push inferior to superior. What is the name of the Counterstrain Tenderpoint?
|
Right Anterior L4 Counterstrain TP
|
|
|
You have a tenderpoint 1/2" medial to the right ASIS. What is the name of the Counterstrain Tenderpoint?
|
Right Anterior L1 Counterstrain TP
|
|
|
Lower Pole L5 vs. Piriformis Counterstrain:
-Patient lays on belly - Bend the knee on the tenderpoint side, flex hip to 90 degrees, ABduct and EXTERNALLY rotate the hip until tenderness is minimized |
Piriformis Counterstrain
|
|
|
Lower Pole L5 vs. Piriformis Counterstrain:
- Patient lays on belly - Flex Hip and Knee 90 degrees - Fine tune with hip ADduction until tenderness is minimized |
Lower Pole L5 Counterstrain
|
|
|
You are poking and prodding some poor bastard and you find a tender spot that when you press on it, the pain radiates and refers to different areas.
Is this a Counterstrain TP or a Trigger Point |
**Trigger Point**
Counterstrain TPs DO NOT have radiating pain.. |
|
|
Sherrington’s Law:
◦ When a muscle receives an nerve impulse to contract, its antagonists receive, simultaneously, an impulse to ______ |
Antagonists relax
(think of this as stepping on a nail) |
|
|
For patients with Acute/Severe problems, which types of techniques are used?
Low dose or high dose? |
Indirect Techniques
- Low Dose, fewer regions |
|
|
For patients with Chronic problems, which types of techniques are used?
Low dose or high dose? |
Any technique including direct
-higher dose, more regions |
|
|
Give me the fascial pattern consistent with the Common Compensatory Pattern
|
Occipitoatlantal -L
Cervicothoracic - R Thoracolumbar -L Lumbosacral - R |
|
|
The right head and right upper extremity have lymph drained by the ________
|
Right Lymphatic Duct
(Green Book adds: Heart and Lungs except for left apex) |
|
|
The left side of the head, left upper extremity, right AND left lower extremeties have lymph drained by the _________
|
Thoracic Duct
|
|
|
How many times does the thoracic duct drainage cross the thoracic inlet?
|
Twice
|
|
|
When treating lymph and fascial restrictions with OMT, do you remove fascial restrictions proximal to distal or distal to proximal?
|
proximal to distal
|
|
|
When trying to normalize lymphatic drainage, do you treat distal to proximal or proximal to distal?
|
distal to proximal
|
|
|
What is a good technique to treat the sympathetic component of bowel dysfunction?
|
abdominal plexus inhibition
(Contraindicated in peritonitis and bowel obstruction) |
|
|
What are 2 good treatments to treat the parasympathetic components of visceral disease?
|
Suboccipital Inhibition (Vagus/CN X)
Sacral Rocking (S2-S4) |
|
|
Head and Neck
Sympathetic: Parasympathetic: |
Sympathetic: T1-4
Parasympathetic: Vagus |
|
|
Cardiovascular
Sympathetic: Parasympathetic: |
Sympathetic: T1-5
Parasympathetic: Vagus |
|
|
Respiratory
Sympathetic: Parasympathetic: |
Sympathetic: T2-7
Parasympathetic: Vagus |
|
|
Stomach, liver, gallbladder
Sympathetic: Parasympathetic: |
Sympathetic: T5-9
Parasympathetic: Vagus |
|
|
Small Intestine
Sympathetic: Parasympathetic: |
Sympathetic: T9-11
Parasympathetic: Vagus |
|
|
Ovary, Testicle
Sympathetic: Parasympathetic: |
Sympathetic: T9-T10
Parasympathetic: S2-4 |
|
|
Kidney, Ureter, Bladder
Sympathetic: Parasympathetic: |
Sympathetic: T10-T11
Parasympathetic: S2-4 |
|
|
Muscle most often found to have trigger points?
|
Trapezius
|
|
|
Large Intestine
Sympathetic: Parasympathetic: |
Sympathetic: T8-L2
Parasympathetic: Vagus & S2-4 |
|
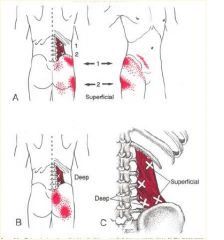
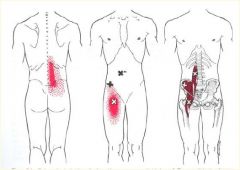
• Easily mistaken for lumbar
radicular pain (coughing or sneezing may increase the pain) or piriformis syndrome • 2 superficial and 2 deep trigger points • Activation: 1) simultaneous bending over and reaching to one side to pull or lift 2) trauma • Perpetuation: short leg, small hemipelvis, short upper arms, a soft bed with a hammock like sag, leaning forward with poor elbow support over a desk, and weak abdominal muscles |
Quadratus Lumborum
"Joker of Low Back Pain" |
|
|
Uterus
Sympathetic: Parasympathetic: |
Sympathetic: T10-T11
Parasympathetic: S2-4 |
|
|
OMT for trigger point directed to the quadratus lumborum muscle
|
Muscle energy to the 11-12th ribs
|
|
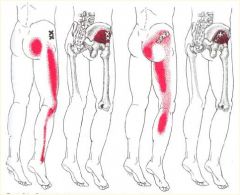
What's this Trigger Point?
|
***Gluteus Minimus***
- Pain is often attributed “ Pseudo-sciatica”to “sciatica” • The more anterior the trigger point, the more lateral the referral zone • Activation: acute or repetitive overload (walking too far or too fast), SI joint dysfunctions, nerve root irritation • Perpetuation: prolonged immobility (esp. driving a car), SI joint dysfunctions, sitting on a wallet placed in a back • Corrective exercises: have pt roll over a tennis ball in the area of the trigger point; sleeping on side with thighs flexed and pillow between knees |
|
|
Prostate
Sympathetic: Parasympathetic: |
Sympathetic: L1-2
Parasympathetic: S2-4 |
|
Trigger Point?
|
***Iliopsoas m.***
- It serves many important functions but Travell considered it as relatively inaccessible • Symptoms are aggravated by weight bearing activities and relieved by recumbency • Activation: prolonged sitting with the hips flexed • Perpetuation: short leg, small hemipelvis, repetitive vigorous contractions (situps) • Correction of somatic dysfunctions of the thoracic, lumbar, or sacral areas and avoid prolonged sitting |
|
|
Chapman's Point:
Middle Ear |
superior to medial clavicles
|
|
|
Chapman's Point:
Sinuses |
inferior to medial clavicles
|
|
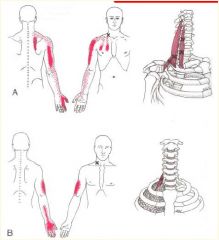
Trigger Point
|
**Scalene Muscles***
- Common source of back, shoulder, and arm pain • Often confused with cervical radiculopathy • Symptoms include myofascial pain or secondary sensory and motor disturbance due to neurovascular entrapment • Activation: pulling, lifting, tugging with the arms or overuse of these muscles in respiration • Perpetuation: tilted shoulder girdle axis • Corrective exercises: neck stretches or coordinated respiration (piston breathing) |
|
|
Chapman's Point:
Pharynx |
Inferior to SCM joints
|
|
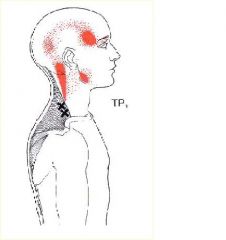
Trigger Point?
|
**Trapezius m.**
- Muscle most often found to have trigger points • Frequently overlooked source of temporal and cervicogenic headache • Activation: commonly results from the stress of sustained elevation of the shoulders and trauma • Corrective exercises: trapezius tension release exercises • OMT would be very similar to those for the scalenes |
|
|
Chapman's Point:
Tonsils |
Medial 1st intercostal spaces
|
|
|
Chapman's Point:
Tongue |
Medial 2nd Ribs
|
|
|
Chapman's Point:
Esophagus, Thyroid, Heart |
Medial 2nd INTERCOSTAL
|
|
|
Chapman's Point:
Upper Lung, Arm |
Medial 3rd INTERCOSTAL
|
|
|
Chapman's Point:
Lower Lung |
Medial 4th INTERCOSTAL
|
|
|
Chapman's Point:
Liver |
Right medial 5th and 6th INTERCOSTALS
|
|
|
Chapman's Point:
Stomach Acidity |
Left medial 5th INTERCOSTAL
|
|
|
Chapman's Point:
Gallbladder |
Right medial 6th INTERCOSTAL
|
|
|
Chapman's Point:
Pancreas |
Right medial 7th INTERCOSTAL
|
|
|
Chapman's Point:
Spleen |
Left medial 7th INTERCOSTAL
|
|
|
Chapman's Point:
Small Intestine |
Medial 8th-10th INTERCOSTAL spaces
|
|
|
Chapman's Point:
Pyloris |
Midline Body of Sternum
|
|
|
Chapman's Point:
Rectum |
Lesser trochanters
|
|
|
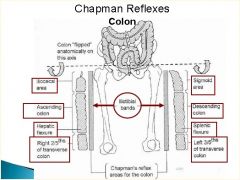
Chapman's Point:
Colon |
Anterior iliotibial bands
|
|
|
Chapman's Point:
Prostate/Broad Ligament |
Lateral iliotibial bands
|
|
|
Here's a pic showing how the Chapman's Points work for the colon
|
|
|
|
The talus glides _____ with plantar flexion (toes down)
|
anteriorly
|
|
|
A patient with restricted plantar flexion in the left foot will have a ___ talus
|
posterior talus
(restricted in anterior glide) |
|
|
The talus glides ____ with dorsiflexion (toes up)
|
posteriorly
|
|
|
A patient with restricted dorsiflexion of the right foot will have a _____ talus
|
anterior talus
(restricted in posterior glide) **Will have (+) Ankle Swing Test** |
|
|
A patient with a positive ankle swing test on the left has ______ restriction
|
dorsiflexion restriction = anterior Left talus
|
|
|
Extension Ankle Vs. Lateral Ankle Vs. Medial Ankle Counterstrain:
-TP is found in proximal gastrocnemius muscle - flex patient's knee, rest your foot on the table and rest the foot on your thigh -fine tune by pushing patient's foot into your thigh |
Extension Ankle Counterstrain
|
|
|
Extension Ankle Vs. Lateral Ankle Vs. Medial Ankle Counterstrain:
-TP anterior and inferior to lateral malleolus -Patient lies on EFFECTED SIDE, EVERT the foot by pushing calcaneus to the floor |
Lateral Ankle Counterstrain
|
|
|
Extension Ankle Vs. Lateral Ankle Vs. Medial Ankle Counterstrain:
- TP is inferior to medial malleolus - patient lies on OPPOSITE side, INVERT the foot, fine tune with internal rotation |
Medial Ankle Counterstrain
|
|
|
What are the common somatic dysfunctions of the foot?
|
Inversion Dysfunctions of the Navicular and Cuboid Bones
|
|
|
The major motions of the knee are flexion and extension:
Flexion results in _____ glide of the tibial plateau |
anterior glide of tibial plateau
|
|
|
The major motions of the knee are flexion and extension:
Extension results in _____ glide of the tibial plateau |
Posterior glide
|
|
|
A patient presents with restriction in knee extension and pain at the end of knee extension.
You suspect that the tibial plateau is restricted in ______ glide |
posterior glide
**Anterior Tibial Plateau** |
|
|
A patient presents with restriction in knee flexion and pain at the end of knee flexion.
You suspect that the tibial plateau is restricted in ______` glide |
anterior glide
**Posterior Tibial Plateau** |
|
|
Fibular head dysfunction often occurs with a____ sprains
|
ankle
|
|
|
If the fibular head is restricted in posterior glide, that means the distal head of the fibula (near the ankle) is ________
|
posterior
|
|
|
A patient comes in complaining of knee pain. You find that the fibular head is restricted in anterolateral glide.
What is the Dx? How would you do Muscle Energy on this patient? |
Posterior Fibular Head =restricted in anterolateral glide
ME: -Flex the knee to 90 degrees - Pull Fibular Head anteriorlaterally -Hold the foot in DORSIflexion (toes up) -Ask pt. to PLANTAR flex against your resistance -Repeat and stretch |
|
|
Which way do the distal and proximal fibular head glide with EVERSION of the foot?
|
Distal Fibular Head = posterior glide
Proximal Fibular Head = Ant. glide |
|
|
Which way do the distal and proximal fibular head glide with INVERSION of the foot?
**Most Common Ankle Injury** |
Distal Fibular Head = Ant. Glide
Proximal Fibular Head = Post. glide |
|
|
ME for a anterior fibular head?
|
(Same as posterior fibular head ME but you push POSTEROMEDIALLY)
-Flex knee to 90 degrees - Push fib head POSTEROMEDIALLY while holding the foot in DORSIflexion (toes up) - Have patient PLANTAR flex foot against your resistance |
|
|
During a posterior fibular head thrust you want to rotate the tibia ______
|
externally
(pg 57) |
|
|
During an anterior fibular head thrust you want to rotate the tibia _______
|
internally
(pg 57) |
|
|
The ____ nerve is compressed by a posterior fibular head. It causes parathesia on the top of the foot and the 1st-4 1/2 toes....
|
Fibular (common peroneal) nerve
|
|
|
You find a patellar tendon tenderpoint on a patient's knee...
How would you treat it with counterstrain.. |
-Place your knee up on table and rest patient's leg over your knee
-Find TP, label 10/10 and push the distal femur downward to EXTEND the knee... (pg. 39) |
|
|
You find a medial meniscal (or lateral meniscal) tenderpoint on a patient's knee.
-How do you set them up for counterstrain treatment? |
-Find the TP
-Flex the knee 60 degrees while dropping it off the table -fine tune with slight tibial internal roatation and ADduction (pg 40) |
|
|
You find an ACL tenderpoint under the distal femur and above the knee
-how do you do counterstrain treatment? |
- Find the TP
-Place pillow ABOVE the knee - Push tibia POSTERIORLY (down toward table) (pg 41) |
|
|
You locate a PCL tenderpoint in the popliteus muscle near the tibeal plateau (behind the knee)
-how would you set them up for counterstrain? |
-Find TP
-Place a pillow BELOW the knee -Push femur POSTERIORLY (down torward table) (pg 42) |
|
|
What is the movement restriction if the Hip (acetobular joint) is restricted in POSTERIOR GLIDE?
|
Internal Hip Rotation
|
|
|
What is the movement restriction if the Hip (acetobular joint) is restricted in ANTERIOR GLIDE?
|
External Hip Rotation
|
|
|
A patient is complaining of hip pain and you find a Lateral Trochanter tender point.
-How would you do counterstrain tx? |
- Find the TP
-ABduct and EXternally rotate the leg (pg. 30) |
|
|
Where would you find a Piriformis Counterstrain TP?
-Treatment? |
TP will be in the mid-buttock halfway between the top of the greater trochanter and midline of the sacrum
-Tx: bend knee on TP side, flex hip 90 degrees, ABduct and EXternally rotate the the hip until tenderness is minimized |
|
|
You find a tenderpoint 1" medial and slightly inferior to the ASIS.. What is it?
How do you do the counterstrain treatment? |
**Iliopsoas Counterstrain TP**
-cross ankles, with TP side on top, flex the knees and hips 90 degrees allowing the hips to EXternally rotate |
|
|
Patient presents with pelvic pain. R ASIS is inferior. R PSIS is superior
|
R Anterior Innominate
|
|
|
Patient presents with pelvic pain. L ASIS is superior. L PSIS is inferior
|
L Posterior Innominate
|
|
|
Patient presents with pelvic pain. R ASIS is superior. R PSIS is superior
|
R Superior Innominate Shear
|
|
|
Patient presents with pelvic pain. L ASIS is inferior. L PSIS is inferior
|
L Inferior Innominate Shear
|
|
|
Patient presents with pelvic pain. R ASIS is medial. R PSIS is latera
|
R Innominate Inflare
|
|
|
Patient presents with pelvic pain. L ASIS is lateral. L PSIS is medial
|
Innominate Outflare
|
|
|
look at pages 77-87 for pelvis treatments
|
I'm getting lazy
|
|
|
How do you treat posterior T10-L5 counterstrain tenderpoints?
|
-Find TP
-Stand on opposite side of TP and lift the thigh on that side to cause hip extension **Remember, Lower-pole L5 is different** |
|
|
Location of Lower-Pole L5 posterior tenderpoint?
|
Inferior surface of PSIS
(pg. 114) |
|
|
Location of Upper-Pole L5 posterior tenderpoint?
|
Superior surface of PSIS
(pg 114) |
|
|
Where is the posterior L4 counterstrain tenderpoint felt?
|
iliac crest in posterior axillary line
|
|
|
What is the Rule of 3's regarding the Thoracic spine?
|
1. T1-T3: same level as its vertebral body
2. T4-T6: 1/2 vertebral level down 3. T7-T9: 1 vertebral level down 4. T10-T12: same vertebral level |
|
|
You are palpating for anterior thoracic tenderpoints:
You find a TP on the sternal notch while pushing inferiorly |
T1
|
|
|
You are palpating for anterior thoracic tenderpoints:
You find a TP on the middle of the manubrium |
T2
|
|
|
You are palpating for anterior thoracic tenderpoints:
You find 2 TPs at the sternum at the level of Rib 3 and Rib 4 insertion |
T3-T4
|
|
|
You are palpating for anterior thoracic tenderpoints:
You find a TP 1" above the xiphisternal junction or at the rib 5 cartilage |
T5
|
|
|
You are palpating for anterior thoracic tenderpoints:
You find a TP at the xiphisternal junction or at the rib 6 cartilage |
T6
|
|
|
You are palpating for anterior thoracic tenderpoints:
You find a TP at the tip of the xiphoid process or rib 7 cartilage |
T7
|
|
|
You are palpating for anterior thoracic tenderpoints:
You find a TP 1.5" below the xiphoid process or at chondral mass |
T8
|
|
|
Tx for Rib 1-2 counterstrain TPs?
|
-Patient lays on back
-Find TP -Flex, rotate and sidebend the head TOWARD the TP |
|
|
How do you treat Anterior Rib 3-10 TPs with counterstrain?
|
|
|
|
How do you treat Posterior Rib 2-10 TPs with counterstrain?
|
-Place foot on table (on same side as TP)
-Drape patient over your thigh (ooh-la-la) -make patient lean into your thigh |
|
|
Rib Exhalation Muscle Energy:
Rib 2... How do you treat and what muscle is contracting? |
- Pull INFERIORLY on the superior rib of the group
-flex the head which is slightly rotated away --> POSTERIOR SCALENE CONTRACTION (pg. 189) |
|
|
Rib Exhalation Muscle Energy:
Ribs 3-5... How do you treat and what muscle is contracting? |
-pull superior rib INFERIORLY
-push elbow of ABducted arm across the chest - PECTORALIS MINOR MUSCLE |
|
|
Rib Exhalation ME:
Ribs 6-10... How do you do the Tx? what muscle is being contracted? |
-pull superior rib INFERIORLY
-push ABducted arm down toward the side of the table -SERRATUS ANTERIOR CONTRACTION (pg. 189) |
|
|
What is the key rib to treat for an Exhalation Dysfunction of ribs 3,4 and 5?
|
Rib 3
(Top Rib) |
|
|
What is the key rib to treat for an Inhalation Dysfunction of ribs 3,4 and 5?
|
Rib 5
(Bottom Rib) |
|
|
Here's a table we're supposed to know all about
|
weeeeeeeeeeeee!!
|
|
|
What are the Steps of the Spencer Technique for the upper extremity?
|

-Extension
-Flexion -Circumduction/Compression -Circumduction/Traction -ABduction -INTERNAL Rotation -ABduction with Lymphatic Pump "Every Fat Cat Tries Absinthe in Paris" |
|
|
For every 3 degrees of aBduction:
- ______ occurs in the glenohumeral joint -_______ occurs at the scapulothoracic articulation |
2 degrees occurs in the glenrohumeral joint
1 degree occurs in the scapulothoracic articulation |
|
|
For every 3 degrees of aBduction:
- ______ occurs in the glenohumeral joint -_______ occurs at the scapulothoracic articulation |
2 degrees occurs in the glenrohumeral joint
1 degree occurs in the scapulothoracic articulation |
|
|
here's another table for the UE...
|
enjoy...
|
|
|
Medial glide of the ulnohumeral joint causes ____ of the forearm
|
ABduction
|
|
|
You have diagnosed a patient with Ulnar ABduction. Will they have pain when extending or flexing the forearm?
|
**Ulnar ABduction** = medial glide
-restricted lateral glide - pain with FLEXION -Increases carrying angle |
|
|
You have diagnosed a patient with Ulnar ADduction. Will they have pain when extending or flexing the forearm?
|
**Ulnar ADduction** = lateral glide
-restricted medial glide -pain with EXTENSION -decreases carrying angle |
|
|
Near the end of full PRONATION, the radial head glides ______
|
posteriorly
|
|
|
Near the end of full SUPINATION,
the radial head glides ___ |
anteriorly
|
|
|
With an anterior radial head somatic dysfunction: (give ease and restriction)
how does this normally occur |
Ease of motion is anterior glide = SUPINATION
-restricted in posterior glide with PRONATION An anterior radial head may be caused by a fall backward on an extended arm |
|
|
A 45 year old man was playing basketball and fell backwards on his exted right arm.
Now he has restricted pronation. Dx? |
Anterior Radial Head
-ease of supination -restricted pronation |
|
|
How does rotation and sidebending occur in the C2-C7 cervical vertebrae?
|
Rotation/Sidebending occur in SAME DIRECTION
|
|
|
What is the primary movement of the OA (C0-C1)?
If sidebending is introduced, does rotation occur in the same direction? |
Primary Motion = Flex/Extend
"Yes/No Joint" When sidebending is introduced, rotation occurs in the OPPOSITE direction. |
|
|
You find that your patient's OA is extended and sidebent to the left. In which direction is the OA rotated?
|
rotated right
|
|
|
What are the facets like on C2-C7?
|
Facets oriented backward,
upward, and medial. (BUM)** - Facets articulate at 45 degree oblique plane |
|
|
You find that your patient has C4 Flexed and and restricted translation to the left.
In what direction is C4 rotated? |
Rotated Left
Resrtricted translation left = patient is sidebent LEFT and can't sidebend right **C2-7 = rotation/SB on SAME SIDE** |
|
|
If you translate a patient's head to the left which way are you sidebending the cervical spine?
|
right
|
|
|
How do you set up Posterior C2-C7 OR Anterior C2-C6 or C8 Counterstrain treatment?
|
-Find TP
-Sidebend away, rotate away from TP **SARA** |
|
|
How do you set up anterior C7 Counterstrain treatment?
|
-Find TP
-Sidebend toward, away rotate **STAR*** |
|
|
Treating Inhalation and Exhalation Ribs 11 &12 stretches the _______
Inhalation Restriction - thumb on rib shaft Exhalation Restriction - thumb on costotransverse articulation |
Quadratus Lumborum
|
|
|
Your patient is complaining of cervical pain and you find a tenderpoint just superior of the medial clavicle.
What is the TP? |
Anterior C8 Counterstrain TP
treat with **SARA** |
|
|
Your patient is complaining of cervical pain and you find a tenderpoint just superior to the clavical along the SCM muscle.
What is the TP? |
Anterior C7 Counterstrain TP
treat with **STAR** |
|
|
How do you treat a Posterior C1 counterstrain TP?
|
Push the back of the head inferiorly and EXTEND the occiput
(pg 206) |
|
|
How do you treat an Anterior C1 counterstrain TP?
|
-Rotate the head away from the TP
(pg 208) |
|
|
A patient presents complaining of cervical pain. You find a tenderpoint just posterior to the mandibular angle.
Dx? |
Anterior C1 Counterstrain TP
(can also be palpated at tip of C1 transverse process) |
|
|
A patient presents with cervical spine pain and is found to have a SIDEBENDING RESTRICTION to the right while extending the cervical spine.
How would you treat this with muscle energy? |
-Move the head into its flexion/extension barrier (here, extension) , and sidebending restrictive barrier (here, right)
-Rotate the head AWAY from restriction to better localize the barrier -Have them Sidebend away from the barrier |
|
|
A patient presents with cervical spine pain and is found to have a ROTATION RESTRICTION to the right while extending the cervical spine.
How would you treat with ME? |
-move head into flexion/extension and rotation restrictive barriers
-Sidebend head AWAY from rotation restrictive barrier to better localize the barrier -Have them rotate away from the barrier |
|
|
List the 5 primary components of the Primary Respiratory Mechanism:
|
1. Motility of brain and spinal cord
2. Fluctuation of CSF 3. Mobility of dura (Reciprocal Tension Membranes) 4. Mobility of Cranial Bones 5. Inherent mobility of sacrum between ilium |
|
|
Name the 2 unpaired bones of the skull for this exam
|
Occiput
Sphenoid |
|
|
Name the 3 Paired bones of the skull for this exam
|
Frontal
Parietal Temporal |
|
|
As the sphenoid and occiput is are in flexion, the frontal bones ______ rotate
|
externally rotate
|
|
|
As the sphenoid and occiput extend, the frontal bones ______ rotate
|
internally
|
|
|
The head feels ______ in FLEXION
|
fatter/wider
|
|
|
The head feels _________ in EXTENSION
|
Skinnier
|
|
|
During cranial flexion, the SBS _____
|
rises superiorly
|
|
|
During cranial extension, the SBS _______
|
falls inferiorly
|
|
|
You are seeing a patient who has been complaining of headaches.
During a cranial exam you notice: -Using the vault hold, the right index finger moves anteriorly -Feels like unscrewing a lid off a jar -The right greater wing of the sphenoid is superior, the right occiput is inferior |
Sphenoid and occiput rotate in opposite directions about
an anterior-posterior (AP) axis |
|
|
You are seeing a patient who is complaining of headaches.
During the cranial exam: -feel a down and out sensation to the left using the vault hold - the left side of the head seems like it's bulging -the left greater wing of sphenoid is inferior and anterior, the left occiput is inferior and posterior |
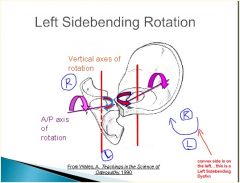
- Occiput and sphenoid sidebend in opposite directions
◦ Rotation is towards the convexity |
|
|
You are evaluating a football player who took a nasty helmet to helmet hit. Instead of sending him to the hospital, you decide to do the vault hold.
You feel right and left greater wings of the sphenoid are INFERIOR and the right and left occiput are SUPERIOR |
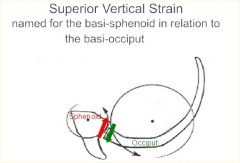
◦ Will feel opposite motion on palpation because you are
monitoring the greater wings of the sphenoid i.e., Using the vault hold, both index fingers will rise on a inferior vertical strain ◦ Named for relative position of the sphenoid base to the occipital base **Superior vertical strain: sphenoid base superior **Inferior vertical strain: sphenoid base inferior |
|
|
A 24 year old man presents after being struck in the head at softball game with a bat.
The right greater wing of the sphenoid feels medial and anterior, the right occiput feels medial and posterior |
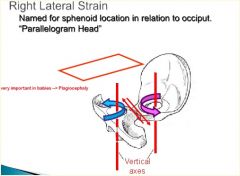
- Caused by a shearing force applied just anterior or posterior to the SBS (i.e. a bat nailing you on the side of the head)
◦ This forces causes the rotation of the sphenoid and occiput in the same direction (both clockwise or counterclockwise) around two parallel vertical axes ◦ Again, you will feel opposite motion on palpation -using the vault hold, both index fingers shift to the right and the pinky fingers shift to the left with a left lateral strain ◦ Named for position of basi-sphenoid in relation to the basi-occiput. **Right Lateral strain: sphenoid base is sheared right in relation to the occiput **Left Lateral strain: sphenoid base is sheared left in relation to the occiput |
|
|
◦ The sphenoid and occiput have been forced together.
◦ May be caused by severe blow or by fever or metabolic problem. ◦ Little or no motion at the SBS. ◦ Classically described as a “bowling ball” head or a “bag of worms”. |
SBS Compression
|
|
|
Entrapment of which Cranial nerve causes Bell's Palsy?
|
CN VII
|
|
|
Which cranial bone is related to nerve entrapment causing Tinnitus and vertigo?
Also a cause of TMJ |
Temporal Bone
|
|
|
***Major trauma***
◦ Involvement in a motor vehicle accident ◦ Fall from a height ◦ Physical assault **Minor trauma*** ◦ Osteoporosis ◦ Metabolic bone disease ◦ Malignancy and infection What is the significance of these "Red-flag" situations in a patient presenting with low-back pain? |
There may be a vertebral fracture!
GET IMAGING |
|
|
You have a patient presenting with low back pain. Pain worsens when supine; and he often has severe nighttime pain while lying in bed.
What are you thinking? |
"Red-Flag"
Possible Spinal Infection |
|
|
A male patient presents with low back pain. He complains of bilateral sciatica pain, SADDLE ANESTHESIA and BLADDER AND BOWEL INCOMPETENCE.
|
Cauda Equina Syndrome
(lesion that compresses nerve roots of cauda equina) |
|
|
You are seeing a patient with pain in the Multifidus Triangle (sacroiliac, posterior thigh and/or inguinal region)
-he also has bilateral UPL5 tender points He thinks he might have an inguinal hernia. What else might you think he has? |
Iliolumbar ligament syndrome
(Mimics Inguinal Hernia) |
|
|
The sciatic nerve arises from the ___ nerve roots
|
L4-S3
|
|
|
Compression by which muscle often results in sciatic nerve irritation?
|
Piriformis!
(normally exits below the piriformis but may actually pierce the piriformis in 10% population) |
|
|
Which side does the pelvis shift in a patient with a right iliopsoas spasm?
|
Pelvis will shift to the left
(OPPOSITE SIDE) |
|
|
A man presents to you with sciatic pain that doesn't go past his knee. He just got back from a long drive from Florida to WV. What are you thinking?
|
Iliopsoas Syndrome
|
|
|
Piriformis spasm often occurs on the _____ side of Iliopsoas spasm in a patient presenting with Iliopsoas syndrome
|
Opposite side
|
|
|
Where is the key lesion in Iliopsoas Syndrome?
|
Type 2 @ L1-2
|
|
|
be sure, now....
|
|
|
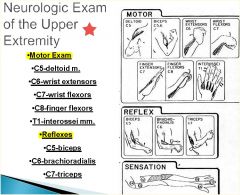
How would you test the MOTOR function of:
-C5 -C6 -C7 -C8 -T1 How would you check the REFLEXES of: -C5 -C6 -C7 |
|
|
|
What type of tumor must your rule out as the source of arm pain or parathesia?
|
Pancoast Tumor
|
|
|
What is the most common cause of cervical strain and sprain?
|
Whiplash
|
|
|
You believe your patient has Thoracic Outlet syndrome.
The costoclavicular compression test will tell you if the nerve root is being compressed between the ____ and ____ |
Clavicle and 1st Rib
**Rib 1 could be elevated** -consider Rib one ME and thrusts |
|
|
You believe your patient has Thoracic Outlet syndrome.
You preform the Scalene Compression Test (Adson's Maneuver) which is (+) -Positive test = diminished pulse and/or reproduction or exacerbation of symptoms Where is the compression occuring? |
Anterior and Middle Scalene mm.
|
|
|
You believe your patient has Thoracic Outlet syndrome.
What test could you do to rule out compression by the pectoralis minor muscle or tendon |
Pectoralis Compression Test
|
|
|
What are some of the things that may diminish recovery from whiplash due to a worse prognosis?
|
- Older age
◦ Female ◦ Initial pain in neck ◦ Increasing lag time between injury date and presentation for treatment ◦ Higher initial pain intensity ◦ Lawyer involvement ◦ Injury during work |
|
|
- Facial or sinus pain
- Headache - Ear pain - Sensory disturbances ◦ Tinnitus/hearing loss ◦ Dizziness ◦ Visual disturbances ◦ Tongue pain -Back pain -Extremity pain These are all symptoms associated with what cervical spine injury? |
Whiplash
|
|
|
At time of whiplash injury,
___% asymptomatic @ 3 months ___% recovered @ 24 months |
56%
82% |
|
|
Reduced cervical ROM at
3 months is a good predictor of pain and disability at 2 years This applies to patients with ____ |
Whiplash
|
|
|
No matter what modality you use to treat trigger points, an essential modality is _______
|
home stretches
|
|
|
A patient comes to your office with motor weakness in anterior tibialis, and is walking on their toes. They have an absent patellar reflex. They have a foot drop and can't invert the foot, what is your diagnosis?
|
L4 Radiculopathy
|
|
|
patient comes in with difficulty extending their toes, and sensation on middle of foot what do they have?
|
L5 radiculopathy
|
|
|
Pt comes in and cannot evert the foot and has sensation on the outer foot. They have no achilles' reflex what do they have?
|
S1 radiculopathy
|
|
|
What type of muscle contraction is occurring when a patient contracts muscles against your resistance in a Muscle Energy technique?
|
Isometric Contraction
"static contraction of a muscle without any visible movement in the angle of the joint" |