![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
76 Cards in this Set
- Front
- Back
|
note: how is blood sample collected |
•Patient’s blood is collected in aviolet topped tube containing EDTA (acts as an anticoagulant to prevent bloodfrom clotting) |
|
|
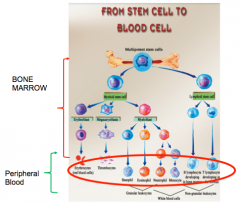
concept: what is seen on the CBC is just the tip of hte iceberg wrt cell types and development |
|
|
|
Normal reference range |
±2 SD wrt the reference population |
|
|
Pediatric CBC: some notable points 1. neut vs. lymp balance |
early childhood: Lymphs (60%) > Neut (30%) |
|
|
peds CBC: wbc levels in children |
are HIGHER |
|
|
peds CBC: HGB and MCV at birth |
–Veryhigh Hb andMCV at birth; dropping off quickly and then comparatively lower Hb andMCV Note:noraml HGB for baby is 180-200Babieslive in a relatively hypoxic environment |
|
|
the differential: 1. interpreting the numbers 2. abnormal cells that will be listed |
•The absolute values add up to theWBC number•The % values all add up to 100%.•abnormal white blood cells willalso be listed –Blasts -Myeloids = immature white cells beyond theblast stage (promyelocytes, myelocytes,metamyelocytes) –Abnormal or variant lymphocytes:these can be benign or malignant --->Atypical lymphocytes in mononucleosisand viral illness --->Lymphoproliferative neoplasms that “peripheralize”: CLLd |
|
|
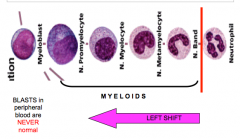
review: degrees of white cell maturation and the left shift |
|
|
|
review: significance of BLASTS in the peripheral blood? |
this is NEVER normal |
|
|
approach to cytopenia: 3 basic principles |
1. a cell count is low: where is the problem? 2. consider other cell counts. is this an isolated abnormality? 3. consider the patient: how urgently do tests need to be done? |
|
|
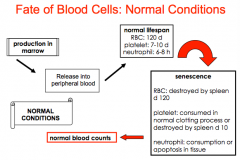
notes: 1. lifespan of RBC, PLT, Neut 2. consumption processes for each |
|
|
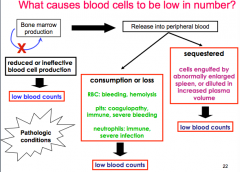
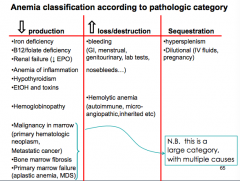
approach to low cell count by pathologic category 1. 3 categories? 2. examples of processes in each category |
|
|
|
approach to cytopenia: central vs. peripheral |
|
|
|
key question in making the distinction between central and peripheral: |
are other cell lines down? the more cell lines affected, the more likely the problem is one of marrow production |
|
|
features of bone marrow problem on CBC |
1. more likely to manifest as pancytopenia 2. seeing immature cells in the blood increases likelihood as primary bone marrow problem |
|
|
principle 3: consider the patient. how urgent is the situation? |
|
|
|
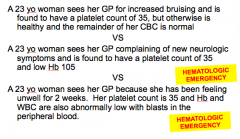
examples of patient factors... |
|
|
|
threshold for anemia in M/F |
<130 g/L in males <120 g/L in females |
|
|
anemia: signs and sx depend on... 4 |
severity, rapidity of onset, age of patient, comorbidities |
|
|
Sx and signs of anemia |
•in general:–fatigue–SOB & tachypnea–tachycardia–decreased exercise tolerance–dizzy or lightheaded–worsening of pre-existing ischemicstate all 2º to decreased O2 delivery ± dec. circulating blood volume |
|
|
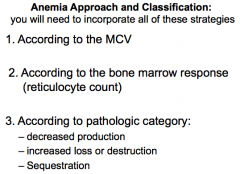
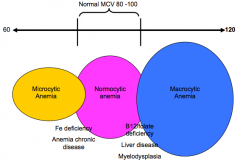
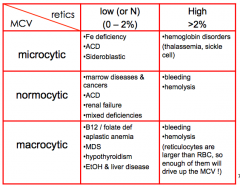
3 ways to classify anemia ? NB |
|
|
|
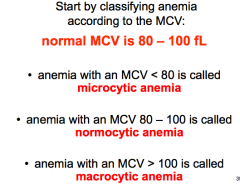
1. according to the MCV values for microcytic, normocytic, and macrocytic |
|
|
|
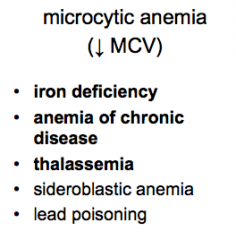
NB: 1. DDx for Microcytic anemia (top 3 of 5) |
|
|
|
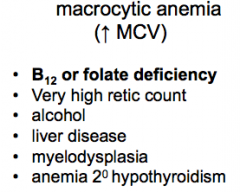
NB: DDx for macrocytic anemia (6) |
|
|
|
for everything else, there's normocytic anemia (most other causes. therefore its a large DDx) note that MCV is not an absolute rule.. |
|
|
|
strategy 2: classify by the reticulocyte response which test should be ordered along with the retic count? |
|
|
|
background: appropriate bone marrow response to anemia |
|
|
|
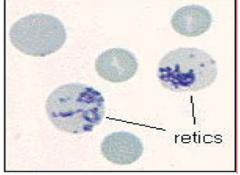
this is what a reticulocyte looks like |
|
|
|
what is a normal reticulocyte count? |
1% |
|
|
what is the rule of thumb for retic count in anemia? |
2% |
|
|
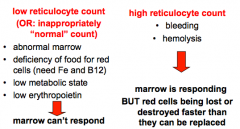
anemia classification according to the retic response: 1. LOW retic count (or inappropriately normal): list causes 2.High retic count (responding appropriately): list causes. |
|
|
|
approach to anemia by pathologic category examples of causes of increased loss or destruction |
bleeding and hemolysis |
|
|
approach to anemia by pathologic category causes of sequestration and dilution |
dilutional anemia: pregnancy, large IV boluses sequestration: not a common cause for anemia |
|
|
decreased production |
is a BIG category |
|
|
best way to assess iron stores |
get a serum ferritin note that patients who are Fe deficient are not always microcytic, this is more of an end stage feature... |
|
|
Iron deficiency anemia causes (7) 1. kids 2. females of reproductive age 3. some others (diet, GI, etc) |
note that iron def anemia is NOT a diagnosis |
|
|
Hemolysis note: immune vs. non immune which tests should be ordered? |
•Tests to order: –Blood film, reticulocyte count –LDH, bilirubin, unconjugatedbilirubin –haptoglobin (mops up free heme?) –DAT (direct antiglobulin test) |
|
|
Broad approach to pathologic categories |
|
|
|
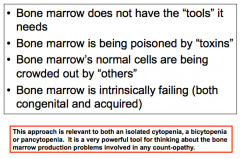
approach to decreased bone marrow production? 4 NB |
|
|
|
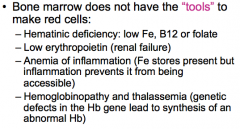
4 examples of bone marrow not having "tools" it needs to make red cells |
|
|
|
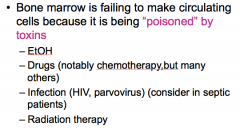
example of toxic (or inflammatory??) insult to bone marrow (4) |
|
|
|
example of bone marrow failing because it is being crowded out by others 4 |
|
|
|
What are primary bone marrow failure syndromes? 3 |
|
|
|
suspected bone marrow failure: what is next step after non-invasive tests? |
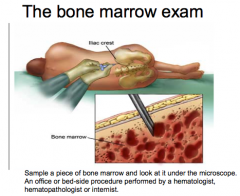
Bone marrow exam! |
|
|
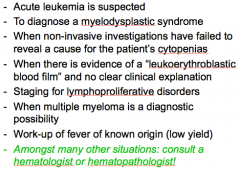
when to consider doing a bone marrow exam? |
|
|
|
Anemia of inflammation: what are the effects leading to anemia? |
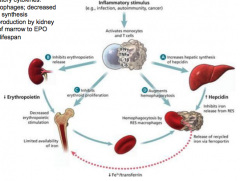
increased inflammatory cytokines lead to: 1. trapping of iron in macrophages, decreased availability for RBC synthesis 2. decreases EPO production by the kidney 3. blunt response of marrow to EPO 4. shortens RBC lifespan |
|
|
anemia of inflammation: making the diagnosis |
1. dx of exclusion 2. can be multiple causes 3. find AND treat reversible causes of anemia, rule out serious causes |
|
|
2 reasons for blasts in the peripheral blood |
1. hematologic neoplasm in the marrow 2. stressed out marrow |
|
|
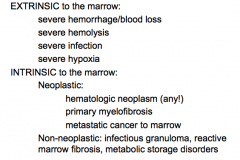
examples of 1. extrinsic stressors to bone marrow 2. intrinsic stressors of bone marrow (neoplastic vs. non-neoplastic) |
|
|
|
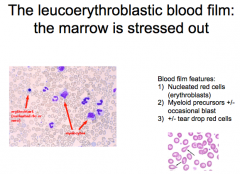
features of "stressed marrow" blood film |
|
|
|
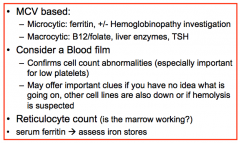
Initial investigations in Anemia workup? |
|
|
|
Anemia Summary Chart causes of 1. microcytic 2. normo 3. macrocytic vs. Low retic or High Retic |
|
|
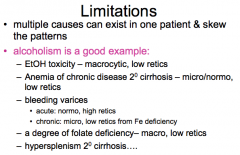
Limitations and variations |
d |
|
|
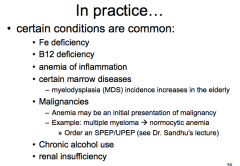
causes of anemia that are more common |
|
|
|
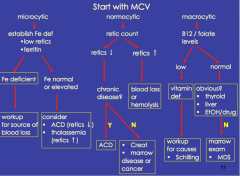
anemia algorithm |
|
|
|
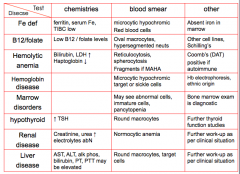
unique features of anemia causes.. a)fe def b) B12 c) hemolytic d) HGB disease e) marrow disorders f) hypothyroid g) renal disease h) liver disease 1. chemistries 2. Blood smear 3. other.. |
|
|
|
Normal range for neutrophil count |
|
|
|
how is neutropenia define? |
1.5 x 10^9 /L note that Ashkenazi Jews, black people have lower counts |
|
|
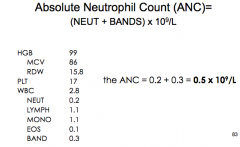
what is the ANC |
|
|
|
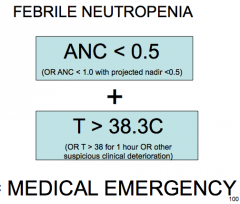
ANC: how low is too low |
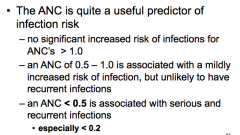
<0.5 = badness |
|
|
neutropenic infections: potential organisms? |
1. gram pos and gram neg, often from organisms not usually pathogenetic 2. fungus (aspergillus and candida) 3. protozoa (toxoplasmosis) |
|
|
what history is important to get in neutropenic patient? |
|
|
|
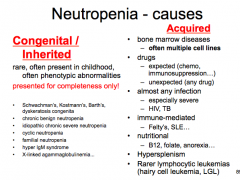
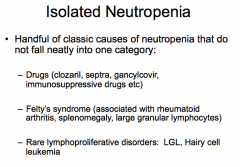
approach to neutropenia: Congenital RARE vs Acquired causes |
|
|
|
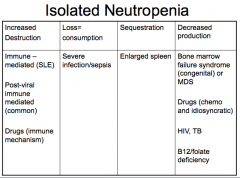
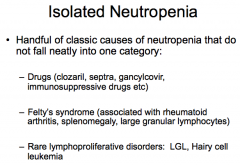
Approach to Neutropenia via pathologic categories |
|
|
|
d |
|
|
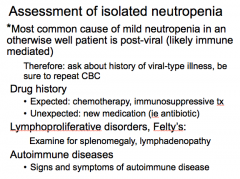
what is the most common cause of neutropenia in an otherwise well patient? |
*Mostcommon cause of mild neutropenia in an otherwise well patient is post-viral(likely immune mediated) Therefore: ask about history ofviral-type illness, be sure to repeatCBC |
|
|
|
|
|
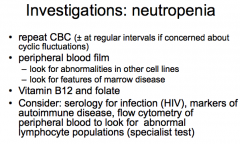
Investigations to consider in neutropenia |
|
|
|
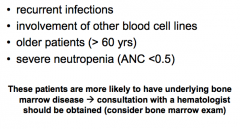
Warning signs for neutropenia that suggest underlying bone marrow disease 4 |
|
|
|
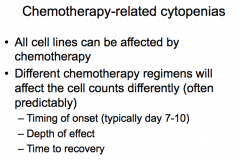
basic description of CHemo related cytopenia |
|
|
|
which cancer has VERY myelosuppressive chemo regimens |
Chemotherapy for acute leukemia isone of the most potent and myelosuppressive regimens --platelet and neutrophil countsapproach zero Other regimens (iebreast cancer, lymphoma) --milder effect and shorter lastingeffect --canstill cause significant morbidity and mortality --can lead to delays inadministering next cycle of chemotherapy if cell counts have not adequatelyrecovered |
|
|
Dx criteria for Febrile Neutropenia |
` |
|
|
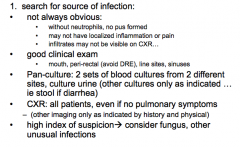
Febrile neutropenia: searching for source of infection (investigations |
|
|
|
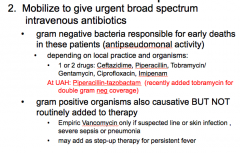
Tx of febrile neutropenia |
|
|
|
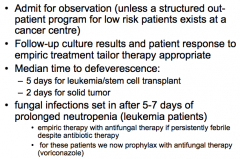
febrile neutropenia: 1. admit 2. follow up cultures 3. time to defeverescence 3. when do fungal infections set in? |
|
|
|
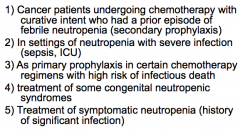
indications for G-CSF 5 (will shorten duration of chemo-associated neutropenia) |
|