![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
91 Cards in this Set
- Front
- Back
|
the cerebrum, including the frontal lobs forms from the . . |
telencephalon |
|
|
embryologically the basal ganglia (thalumus, hypothalumus and pituitary) forms from the |
diencephalon |
|
|
What are the 4 types of vascular malformation? |
AVM, cavinoma, DVA, capillary telangectasia. |
|
|
What is a Braxton-Hicks contraction? |
Benign sporadic uterine contractions that start around 6/40 but are usually only felt late in the pregnancy. |
|
|
What is the embryonic period? |
6-10 weeks
|
|
|
Why perform first trimester US? |
identification of position, early foetal demise, anembryonic gestation, prediction of abnormalities based on secondary cireria - eg abnormal yolk sac.
|
|
|
What is the gestational sac called once it is implanted in the decidualized endometrium? |
intradecidual sac |
|
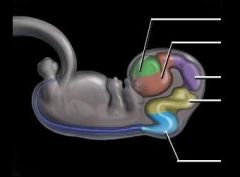
label this diagram |
Telencephalon Diencephalon Mesencephalon Metencephalon Myelencephalon |
|
lable this diagram |
Chorionic cavity Decidua basalis Decidua capsularis Decidua parietalis |
|
|
When is the heartbeat visible on ultrasound? |
5 weeks |
|
|
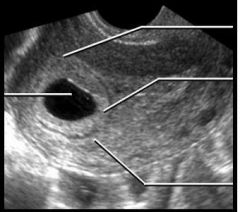
What is the double decidual sign |
Visualization of the 3 layers of the decidua confirming an intrauterine pregnancy. |
|
|
What CRL would you expect with a bHCG of 1000 and 10,000 repsectively?
|
5 mm at 1,000 & 10 mm at 10,000
|
|
|
When does an embryo become a foetus? |
10 weeks gestation |
|
|
When does a blastocyst become an embryo |
When the amniotic sac is formed (around day 10) |
|
|
At how many weeks is it abnormal not to see an embryo within the amnion and how large would you expect the amniotic sac to be? |
7 weeks. 23 mm. |
|
|
Most common mass seen in the first trimester of pregnancy |
Corpus luteum cyst (secretes progesterone) |
|
|
What is the characteristic appearance of a dermoid cyst? |
cystic mass with focal calcification and a fluid/fluid level. |
|
|
What is the typical appearance of a uterine fribroid? |
Solid, slighty hypoechoic mass +/- areas of calcification. Rarely cystic avascular areas related to necrosis.
Not to be confused with a focal myometrial contraction which will go away. |
|
What is this echogenic band called |
Synechiae. Also known as Ashermans syndrome or uterine adhesions. |
|
|
What is the most common ovarian tumour in the reproductive age-group? |
Ovarian teratoma. |
|
|
What is struma ovarii? |
Ovarian teratoma of the monodermal type which is composed of > 50% thyroid tissue (or the tumour is functionally active) |
|
What is this? |
Theca Lutein cyste (non vascular septa make ovarian cancer less likely) |
|
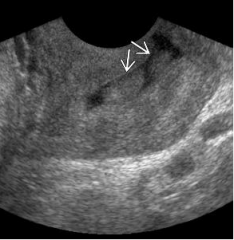
what is this adnexal structure with homogeneous low-level eches? |
Endometrioma (chocolate cyst) |
|
What is this structure with fine lace-like septations? |
Corpus luteum cyst. |
|
|
What is alpha fetoprotein? |
Most abundant protein in foetal blood (analogous to albumin). Produced by the yolk sac and liver. |
|
|
When is alpha fetoprotein elevated? |
OBST: omphalocele neural tube defectes
ONC: hepatocellular carcinoma, liver mets, germ cell tumours (not seminoma) |
|
|
What is Dandy-Walker malformation? |
Absence / hypoplasia of the cerebellar vermis. |
|
|
Earliest sign of corpus callosum agenesis |
Absent cavum septum pellucidum (CSP) |
|

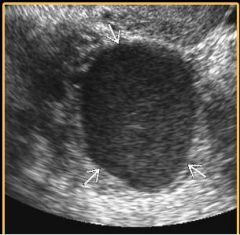
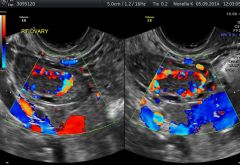
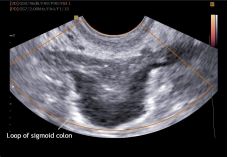
Describe this lesion arising in the left adnexa and list differentials |
Transvaginal technique. Solid mass with slightly heterogeneous echogenicity arising in the left adnexa which appears separate from the adjecent uterus.
DDx : choriocarcinoma (gestational or ovarian), Other malignant germ cell tumours or tumour of sex cord / stromal origin. |
|
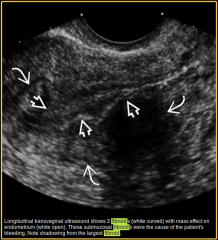
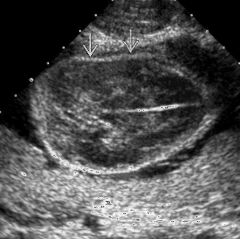
Desribe these 3 lesion |
3 well demarcated masses arising from the myometrium of the uterus and impinging on the overlying endometrium. All the lesions are hypoechoic to myometrium. The largest lesion is causing shadowing.
Appearances consistent with submucosal fibroids. |
|
|
What are the 4 catagories of fibroids by location? |
Submucosal (in contact with the endometrium) Mural Subserosal Pedunculated (separate to the uterus, but joined to it by a stalk. |
|
|
What is adenomyosis? |
Presence of heterotopic endometrial tissue within the myometrium. |
|
|
What are the ultrasound imaging characteristics of adenomhyosis? |
- Multiple find foci of attenuation give a "rain shower" appearance. - Myometrial cysts. - Heterotopic endometrial tissue within the myometrium. - Loss of the normal myo-endometrial junction. |
|
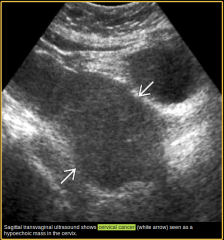
Describe this lesion |
There is a hypoechoic mass arising from and partially replacing the cervix.
Dx cervical cancer. DDx cervical fibroid. |
|
|
What are come complications of an IUD |
Pain during intercourse (usually due to malpositioning) uterine perforation. An IUD that has perforated the uterus can go on to perforate other pelvic organs. Infection |
|
|
What is the upper limit of normal for endometrial thickness in a postmenopausal woman? |
5 mm |
|
|
What is the upper limit of normal in premenopausal women? |
No reliable threashold. Reported between 8 mm and 16 mm depending on time in cycle. |
|
|
What is most important about endometrial hyperplasia |
It may progress to endometrial cancer. |
|
|
Common neoplasms of the uterus |
endometrial polyps, leiomyoma (fibroids), endometrial carcinoma, leiomyosarcoma. |
|
|
Endometrial polyps are caused by |
A monocolonal proliferation of stromal cells probably due to a rearrangement at 6p21. |
|
|
Ultrasound appearance of a uterine polyp |
Isoechoic with surrounding myometrium |
|
|
Uterine polyp microscopy |
proliferation of stromal cells with dilated glands and lined by colmnar epithelium. |
|

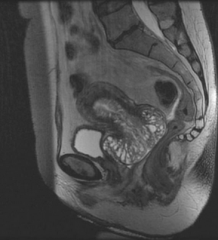
Describe these findings and give diagnosis. |
There is incomplete fusion of the fundal myometrium with a cleft separating the symmetrical divergent horns.
Bicornuate uterus (heart shaped uterus) |
|
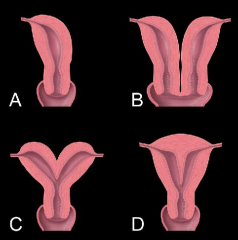
Name these Mullerian duct malformations. |
A. Unicornate uterus B. Uterus didelphys C. Bicornuate uterus D. Septate uterus |
|
|
is septate or bicornuate more associated with misscarriage? |
setpate because the septum is unable to maintain the placenta. |
|
|
What is an arcute uterus? |
Smooth broad convex fundal indentation with normal external contour. |
|
|
Leiomyoma histology and macropathology |
Whorled bundles of smooth muscle.
Pale grey will circumscribed spherical mass. |
|
|
From where do leiomyosarcomas arise? |
The mesenchymal cells of the myometrium. |
|
|
Define: mesenchymal |
Mesodermal tissue that forms connective tissue, blood and smooth muscles. |
|
|
What are the germ layers? |
Endoderm, mesoderm, ectoderm. |
|
|
Define: endoderm. |
The innermost of the 3 primary germ layers.
Forms most organs, specifically: stomach, the colon, the liver, the pancreas, the urinary bladder, the epithelial parts of trachea, the lungs, the pharynx, the thyroid, the parathyroid, and the intestines. |
|
|
Define: ectoderm. |
Outermost of the 3 primary germ cell layers.
Forms the neural tube, neural crest and surface ectoderm. The surface ectoderm goes on to differentiate into skin, nails, hair and lens of the eye. |
|
describe the lesion in the cervix and offer a differential. |
There are two polypoid lesions extending into the cervical canal. They are isoechoic with the neibouring cervical parenchyma. Doppler imaging is likely to reveal a single supplying artery.
Dx Cervical polyp.
DDx Polypoid leiomyoma, descending uterine polyp, blood clot. |
|

Describe this cervical lesion and offer a differential |
There is a well circumscribed, anechoic, unilocular cyst-like entity arising from the cervical epithelium.
No definite decidual reaction. I would enquire about the beta-hCG.
Dx Nabothian cyst DDx cervical gestation, adenoma malignum, SCC of cervix with central necrosis, |
|
|
The equivalent cystic lesion to a Nabothian cyst in the vagina is called |
Gartner duct cyst |
|
What is this? |
Adenoma malignum.
Rare variant of cervical adenocarcinomas (3%). On imaging contains multiple small cysts. |
|
|
What are the two histiologic types of cervical cancer? |
Squamous cell carcinoma (85%) Adenocarcinoma (worse prognosis) |
|
|
What is Asherman syndrome? |
Multiple endometrial adhesions. |
|

Identify pathology |
hypospadias |
|

Identify pathology |
hydrosalpinx |
|

Identify pathology |
Osteogenesis imperfecta |
|

Identify pathology |
Osteogenesis imperfecta |
|

Identify pathology |
Acrania |
|

Identify pathology |
Adenomyosis |
|

|
Absent end diastolic flow |
|

|
Anembryonic pregnancy |
|

|
Atypical ovarian mass |
|

|
Cleft palate |
|
|
Corpus luteum |
|
|
Exophytic corpus luteum |
|
|
CPAM (Congenital Pulmonary Airway Malformation) |
|

|
Extensive cystic hygroma |
|

|
Duodenal atresia |
|
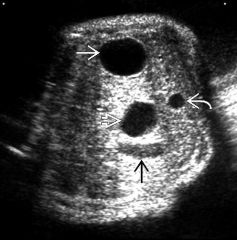
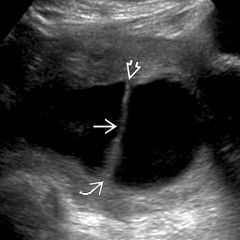
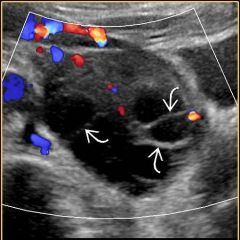
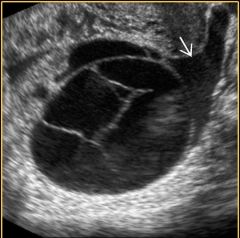
Identify pathology and label anatomy designated by white curved and black arrows |
Duodenal atresia. white curved: umbilical vein black arrow: gall bladder |
|
|
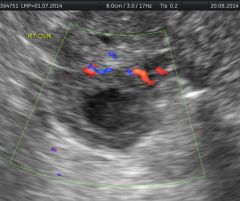
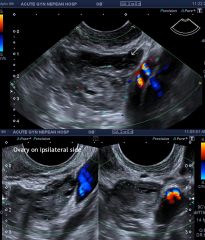
Ectopic pregnancy |
|

|
Endometrial carcinoma |
|

|
Endometrial polyp |
|

|
Endometriosis |
|
|
Endometriosis |
|

|
gastroschesis |
|

|
hydrosalpinx |
|

|
hydrosalpinx |
|

|
ovarian hyperstimulation |
|

|
hypospadias |
|

|
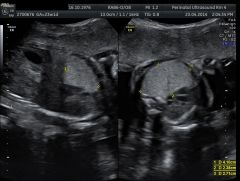
Large head. Turned out to be trisomy 18. |
|
|
osteogenesis imperfecta |
|

|
osteogenesis imperfecta |
|

|
osteogenesis imperfecta |
|

|
placenta previa |
|

middle aged lady presents with intermenstral PV bleeding. |
retained products of conception |
|

|
Uterine rupture. |