Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
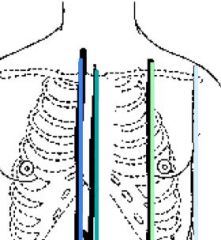
Name the landmark lines for the anterior chest
|
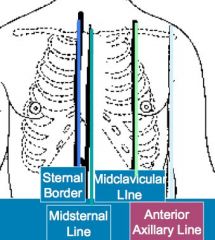
RSB or LSB
MSL RMCL or LMCL RAAL or LAAL |
|
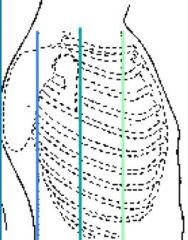
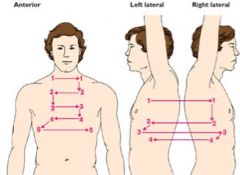
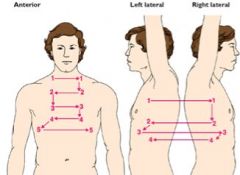
Name the landmark lines for the lateral chest
|
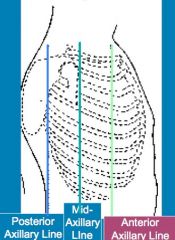
PAL
MAL AAL |
|
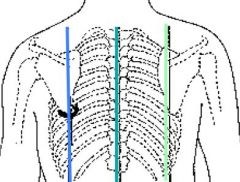
Name the landmark lines for the posterior chest
|
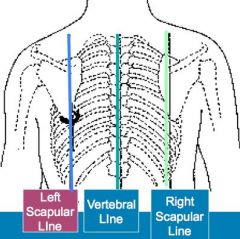
No abbreviations
|
|
|
What are the borders of the thoracic cage?
|
The thoracic cage is defined by the sternum, 12 pairs of ribs, and 12 thoracic vertebrae. The diaphragm forms the floor of the thoracic cavity. The intercostal space is named for the rib above it.
|
|
|
What are the Anterior Thoracic landmarks?
|
• Suprasternal Notch – U-shaped depression just above the sternum.
• Sternum – Three parts – manubrium, body, xiphoid process • Angle of Louis – Manubriosternal angle/sternal angle - the articulation of the manubrium and the body of the sternum; continuous with the 2nd rib; level of the tracheal bifurcation, upper border of the atria of the heart; lies above the fourth thoracic vertebra. • Costal Angle – The angle of the lower costal margins; meet at the xiphoid process; should be 90° or less. |
|
|
What are the Posterior Thoracic Landmarks?
|
• Vertebra Prominens – Most prominent bony spur protruding at the base of the neck; spinous process of C7; one right below it will be T1
• Spinous Processes – Count down these to locate the level of thoracic vertebrae and the ribs branching off of them • Inferior Border of the Scapula – The lower tip is usually at the 8th or 9th rib • Twelfth Rib – Palpate midway between the spine and the person’s side to identify its free tip |
|
|
What is the Pleurae and Costodiaphragmatic Recess?
|
• The thin, slippery Pleurae form an envelope between the lungs and the chest wall. The Visceral pleura lines the outside of the lungs, and the Parietal pleura lines the inside of the chest wall and diaphragm.
• The Costodiaphragmatic Recess is a space of the pleurae that extends about 3cm below the level of the lungs. It can abnormally fill with fluid or air and compromise lung expansion. |
|
|
Explain details about the Trachea
|
• The Trachea lies anterior to the esophagus and is 10-11 cm long in an adult. The tracheal bifurcation is at the level of T4 or T5 posteriorly, at the level of the Angle of Louis or 2nd ICS anteriorly, and high in the axilla laterally. The right main bronchus is shorter, wider, and more vertical than the left. This makes it easier for a foreign body to lodge in the right bronchus.
|
|
|
What is the Bronchial Tree?
|
• The Tree and the Bronchi transport gases between the environment and the lung parenchyma. They constitute dead space and do not allow for gas exchange, however they are lined with goblet cells and cilia to trap particles from the air and transport them out of the respiratory system.
|
|
|
What is an Acinus?
|
• An Acinus is the functional respiratory unit; consists of the bronchioles, alveolar ducts, alveolar sacs, and the alveoli.
|
|
|
4 Main Mechanics of Respiration:
|
• Supply oxygen to the body for energy production
• Remove CO2 as the waste product of energy reactions • Maintain homeostasis of the acid-base balance system of arterial blood • Maintain heat exchange |
|
|
What is Hypercapnia, Hypoxemia, and Surfactant?
|
• Hypercapnia is the increase of CO2 that stimulates us to breathe
• Hypoxemia is a decrease in O2 in the blood that can stimulate us to breathe, but is less effective than hypercapnia • Surfactant is the complex lipid substance neeed to sustained inflation of the alveoli |
|
|
What are the anterior surface landmarks of the thorax?
|
• Anterior Chest: Suprasternal notch, sternum, manubriosternal angle (Angle of Louis)(2nd Rib), costal angle (should be <90°), tracheal bifurcation (2nd rib or intercostal space), clavicle (top of lung is 3-4 cm above the clavicle)
|
|
|
What are the posterior surface landmarks of the thorax?
|
• Posterior Chest: Vertebra prominens, superior border of scapula (around 2nd rib), inferior border of scapula (7th or 8th rib), 10th rib (lower level of lung with normal respiration), 12th rib (lower level of lung during deep inspiration), tracheal bifurcation (2nd rib or intercostal space); to locate T10, palpate floating rib in and move up to 11th rib, make a ‘v’ with your hands and you will be right around T10
|
|
|
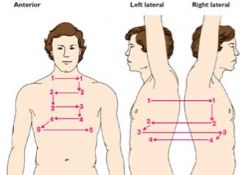
What are the borders of the lungs?
|
• Lung Border Summary: Anterior – Above clavicle and down to the 6th rib; Lateral – High in axilla and down to the 8th rib; Posterior – T1 to T10 or T12; Lower borders are easy to remember as 6, 8, 10, and 12.
|
|
|
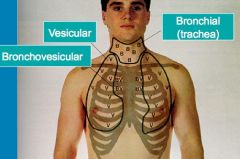
What are three normal breath sounds in their expected region?
|
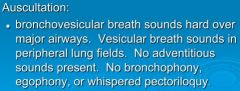
• Bronchial – Normal over the trachea; loud with harsh sounds, tubular; I<E (inspiration is shorter than expiration)
• Bronchovesicular – Normal over major airways; quieter sound heard over sternum and scapulae; I=E • Vesicular – Normal in peripheral lung fields; I>E |
|
|
What are the three normal voiced sounds of the lungs?
|
• Bronchophony – Client voicing ‘99’ at each point of ascultation; should sound soft, muffled, and indistinct; fluid in the lungs would carry the sound and make it clearer
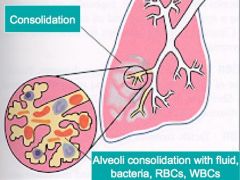
• Egophony - Client voicing ‘eeee’ at each point of ascultation; should hear an ‘aaaa’ (ay) sound; hearing an ‘eeee’ sound indicates consolodation (fluid, bacteria, RBC’s, WBC’s) • Whispered Pectoriloquy – Client whispering ‘1, 2, 3’ at each point of ascultation; normal sound will be faint and muffled; hearing the whispers clearly transmitted indicates consolodation • Documentation for ‘normal’ evaluation – “No bronchophony or egophony” |
|
|
What are four adventitious sounds that are always abnormal?
|
Crackles (rales): Discontinuous sounds due to fluid in alveoli or alveoli popping open after being compressed; always allow a person to move around/cough, etc. after waking up first thing – some alveoli may have closed while client was sleeping, but will clear up after some deeper breathing – could lead to a false diagnosis
Wheezes: Continuous, high pitched sounds d/t obstructed air flow; typically heard with asthma Rhonchi: Continuous, low pitch type of wheeze; snoring sound; from mucous or fluid in the airway Stridor: From an upper airway obstruction; indicates a medical emergency will soon be happening; ex. Choking on foreign body |
|
|
What are five questions to ask while performing auscultation?
|
• Where did I hear it?
• What did I hear? • How did it compare to the opposite lung? • Did it go away with coughing? (Especially with crackes and wheezes) • Where in the respiratory cycle did I hear it? Inspiration/Expiration or Both? |
|
|
What are the expected normal findings of a thorax exam?
|
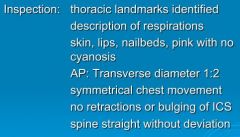
General inspection should show a normal LOC, VS, SpO2; no obvious signs of illness; moderate, rhythmic, symmetrical, unlabored respirations (Eupnea with 12-20 respirations per minute, around 1 breath for every 4 heartbeats); no pallor or cyanosis; anterior angle of costal margins at or <90 °; no retractions in the ICS (intercostal spaces); spine is straight with no scoliosis, kyphosis, “spine straight with no deviation”; AP to transverse shape/configuration is roughly 1:2 (not including infants)
|
|
|
What are the general signs of respiratory distress?
|
General signs of respiratory distress include: Hypertrophy of the neck muscles, nasal flaring (esp. in babies), ICS retractions, pursed lips on expiration, tripod position, barrel chest with 1:1 configuration and costal margins >90° (from long-standing COPD)
|
|
|
What are the 12 subjective areas we ask our patients for a respiratory assessment?
|
• Any hx of chronic cough?
• Any shortness of breath? • Any chest pain with breathing? • Any past hx of illness associated with the lungs? Any hx of lung CA? • Any hx of smoking? • Any hx of environmental exposure to things such as farming chemicals, working in heavy outdoor traffic, etc.? • Have you ever had a TB test or chest x-rays? What were the results? • Are you current on childhood immunizations? • Do you take any medications? • Any personal or family hx of heart disease or heart problems? • Do you have any allergies? • Don’t forget COLDSPA!! |
|
|
What six things do we check upon inspection of the thorax?
|
• Perform identification of landmarks, structures, and reference lines
• Include a description of skin including the lips and nails • Include the thoracic configuration and ratio (ex. AP=1:2) • Look at the angle of rib insertion anteriorly an posteriorly (ex. Anterior – horizontal, Posterior – sloped) • Assess the ICS – note any bulging or retractions) • Give a description of the spine |
|
|
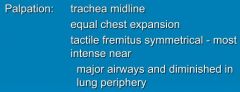
What are the four areas of palpation assessment that we do for the thorax?
|
• Perform a tracheal assessment (midline?)
• Check for symmetrical chest expansion using bilateral hand placement technique • Assess skin turgor, lesions, moisture, and texture • Assess tactile (vocal) fremitus on the anterior, posterior, and lateral chest (“99” palpation techniques) |
|
|
What are three general guidelines when percussing the thorax?
|
• Be specific as to sound elicited and location heard. Describe lung borders, techniques, and findings
• Use percussed resonance starting at the apicies and comparing side to side as you work down • Abnormal findings must be at least 2-3 cm wide |
|
|
What four sound qualities are possible when percussing a thorax?
|
• Resonance – The sound heard over “healthy adult lungs,” sounds hollow, low-pitched, and clear
• Hyperresonance – Lower-pitched booming sound found when too much air is present, as in emphysema or pneumothorax; can be normal in small children as they do not have as much adipose tissue overlaying their chest cavity • Dullness – A soft, muffled thud heard with abnormal density that would be present with pneumonia, pleural effusion, atelectasis, or tumor. Also heard over bone • Diaphragmatic Excursion – Use percussion to determine equal movement of the diaphragm upon expiration and inspiration |
|
|
What are the sounds heard upon auscultation in 'normal' lungs and how do you document it?
|
Vesicular, Bronchovesicular, Bronchial, Broncophony, Whispered Pectoriloquy, Egophony
• Documentation for ‘normal’ evaluation – “No bronchophony or egophony” |
|
|
What is the pattern to assess areas of tactile fremitus?
|

|
|
|
What is the lateral pattern for tactile fremitus?
|
|
|
|
What is the pattern for assessing percussion on the anterior and lateral aspects of the thorax?
|
|
|
|
What is the pattern for assessing percussion in the posterior position?
|
|
|
|
Where are the areas to auscultate lung sounds on the anterior chest?
|
|
|
|
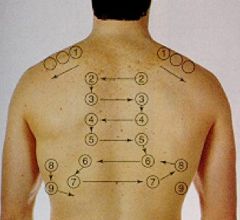
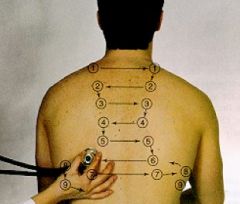
Where are the areas to auscultate breath sounds on the posterior chest?
|

|
|
|
What is the pattern for auscultating breath sounds on the anterior and lateral chest?
|
|
|
|
What is the pattern for auscultation of breath sounds on the posterior chest?
|
|
|
|
What are some reasons for diminished breath sounds?
|
-obesity
-foreign body -hyperinflated lung (emphysemia) -air or fluid in the pleural space -not moving enough air - |
|
|
What are the normal findings for auscultation?
|
|
|
|
What are the normal findings for inspection?
|
|
|
|
What are the normal findings for palpation?
|
|
|
|
What are the normal findings with percussion?
|

|
|

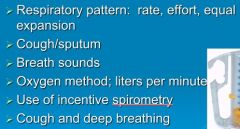
Components of a respiratory assessment in the clinical setting
|
|
|

Components of charting by exception in the clinical setting
|
|
|
What would be the typical documentation for this disease process?
|
Pneumonia (consolodation) - Increased RR; guarding and lag on expansion on affected side; increased tactile fremitus, increased breath sounds on affected side (patent airway for both); increased clarity, bronchophony, egophony, whispered pectoriloquy present; crackles
|
|

What is the expected findings of this disease process? (Enlarged alveoli and alveoli wall deterioration)
|
Emphysema (COPD) - Increased anteroposterior diameter; barrel chest; use of accessory muscles; SOB; tachypnea; decreased tactile fremitus and chest expansion; hyperresonant; decreased diaphragmatic expansion; decreased breath sounds; muffled heart sounds; possible wheeze
|
|
What are the expected findings of this disease process?
|
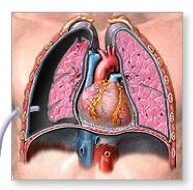
Pneumothorax - Mediastinum shifted from midline; unequal chest expansion; poss tachypnea, cyanosis, bulging in interspaces; tactile fremitus decreased or absent; decreased BP; tachycardia; hyperresonant; decreased diaphragmatic excursion; breath sounds decreased or absent; no adventitious sounds
|
|
|
What is atelectasis?
|
Collapse of part of lung, or the entire lung
|
|
|
Which of the following is true regarding the vertebra prominens? The vertebra prominens is:
1. the spinous process of C7. 2. usually not palpable in most individuals. 3. opposite the interior border of the scapula. 4. located next to the manubrium of the sternum. |
#1
|
|
|
When performing a respiratory assessment on a patient, the nurse notes a costal angle of approximately 90 degrees. This characteristic is:
1. seen in patients with kyphosis. 2. indicative of lung disease. 3. a normal finding in a healthy adult. 4. an expected finding in a patient with a barrel chest. |
#3 - #1 would have no effect, #4 is >90°
|
|
|
Which statement about the apices of the lungs is true? The apices of the lungs:
1. are at the level of the second rib anteriorly. 2. extend 3 to 4 cm above the inner third of the clavicles. 3. are located at the sixth rib anteriorly and the eighth rib laterally. 4. rest on the diaphragm at the fifth intercostal space in the midclavicular line. |
#2 - #3 and 4 are at the base
|
|
|
During an examination of the anterior thorax, the nurse recalls that the trachea bifurcates anteriorly at the:
1. costal angle. 2. sternal angle. 3. xiphoid process. 4. suprasternal notch. |
#2 - Angle of Louis
|
|
|
During an assessment, the nurse knows that expected assessment findings in the normal adult lung include the presence of:
1. adventitious sounds and limited chest expansion. 2. increased tactile fremitus and dull percussion tones. 3. muffled voice sounds and symmetrical tactile fremitus. 4. absent voice sounds and hyperresonant percussion tones. |
#3 - Consolodation, like pneumonia
|
|
|
The primary muscles of respiration include the:
1. diaphragm and intercostals. 2. sternomastoids and scaleni. 3. trapezius and rectus abdominis. 4. external obliques and pectoralis major. |
#1 - The others are used in labored respiration
|
|
|
When assessing tactile fremitus, the nurse recalls that it is normal to feel tactile fremitus most intensely over which location?
1. Between the scapulae 2. Third intercostal space, MCL 3. Fifth intercostal space, MAL 4. Over the lower lobes, posterior side |
#1 - At the level of the trachial bifurcation
|
|
|
The nurse is aware that tactile fremitus is produced by:
1. moisture in the alveoli. 2. air in the subcutaneous tissues. 3. sounds generated from the larynx. 4. blood flow through the pulmonary arteries. |
#3
|
|
|
During percussion, the nurse knows that a dull percussion note elicited over a lung lobe most likely results from:
1. shallow breathing. 2. normal lung tissue. 3. decreased adipose tissue. 4. increased density of lung tissue. |
#4
|
|
|
The most important technique when progressing from one auscultatory site on the thorax to another is:
1. side-to-side comparison. 2. top-to-bottom comparison. 3. posterior-to-anterior comparison. 4. interspace-by-interspace comparison. |
#1
|
|
|
When auscultating the chest in an adult, the nurse would:
1. instruct the patient to take deep, rapid breaths. 2. instruct the patient to breathe in and out through his or her nose. 3. use the diaphragm of the stethoscope held firmly against the chest. 4. use the bell of the stethoscope held lightly against the chest to avoid friction. |
#3
|
|
|
The nurse is assessing voice sounds during a respiratory assessment. Match the assessment with the correct technique:
1. The normal response is faint, muffled, and almost inaudible when the patient says “one, two, three” in a very soft voice. 2. Ask the person to say “ninety-nine” repeatedly while auscultating the chest wall. Normally, a sound will be heard but the examiner will not be able to distinguish exactly what is being said. 3. Listen to the chest while the patient says a long “ee-ee-ee” sound; hearing a long “aaaaaa” sound may be noted over areas of consolidation. B = Bronchophony E = Egophony W = Whispered pectoriloquy |
1. W
2. B 3. E |