Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
116 Cards in this Set
- Front
- Back
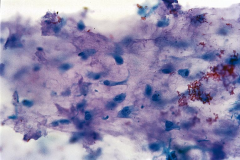
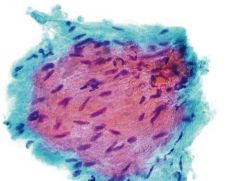
Respiratory sample
|
Creola body
ciliated cells with lots of vacs mimics adenoca asthma BENIGN |
|

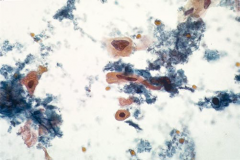
Respiratory sample
|
Curshman spiral
Inspissated mucous |
|
Respiratory sample
|
Ciliocytopthoria
Just the cilia. Mimics organisms. ASSOCIATED WITH VIRUSES |
|
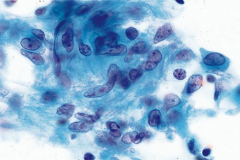
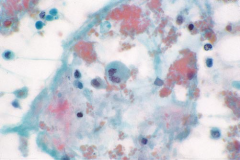
Respiratory sample. what is this? what stain?
|
PCP
Pap stain (fuzzy exudates) |
|
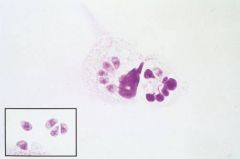
|
PCP Diff quik stain outlines cyst forms and trophs in macrophages
|
|
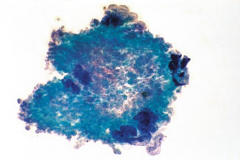
stain?
|
GMS
PCP cyst form |
|
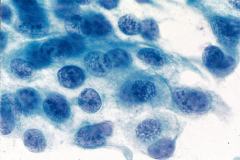
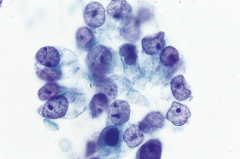
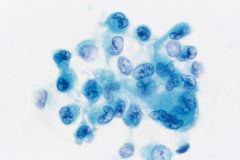
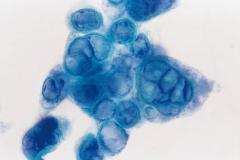
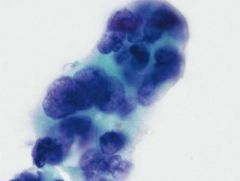
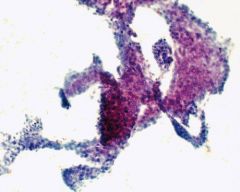
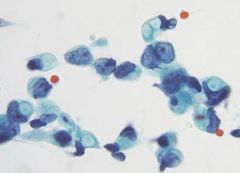
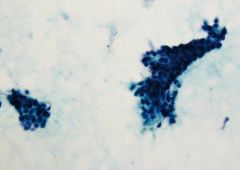
FNA lung mass
|
Benign mesos, contaminant
Flat cohesive sheets Round nuclei, small neucleoli WINDOWS |
|
|

Alternaria
contaminant snowshoe conidia with horiz & vertical lines Septate |
|
|
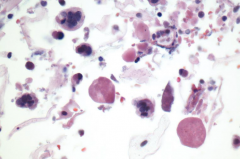
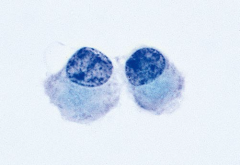
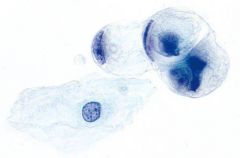
Measles virus infection causes pneumonia with giant multinucleated epithelial cells that have eosinophilic intranuclear and intracytoplasmic inclusions. These
cells are pathognomonic. |
|
|
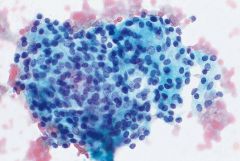
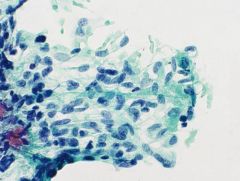
TB
The nodular aggregate of epithelioid histiocytes, which defines the granuloma, has a syncytial appearance because individual cell borders are indistinct. Note the curved and elongated, boomerang shape of some of the histiocytic nuclei. Interspersed lymphocytes can also be seen. |
|
|
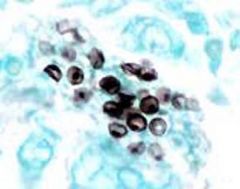
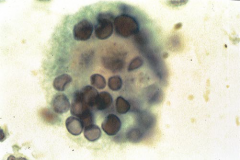
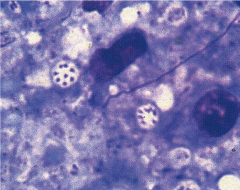
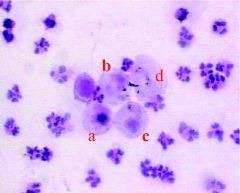
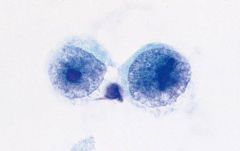
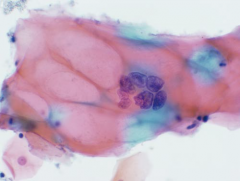
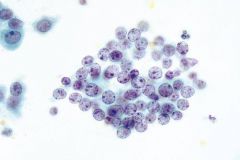
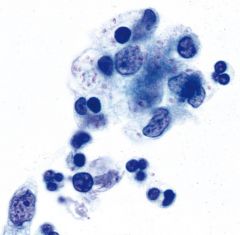
PCP
The Giemsa stain outlines the cysts as negative images, and stains the intracystic bodies or trophozoites. Each cyst, as seen here, contains eight intracystic bodies. |
|
|
Wegener's granulomatosis
Neutrophils, giant cells, necrotic collagen Necrosis Granulomatous inflammation granular background debris consisting of necrotic collagen without acute inflammation is characteristic Vasculitis |
|
|
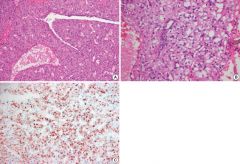
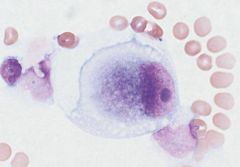
Pulmonary alveolar proteinosis (PAP) is a rare disease
characterized by an accumulation of a lipid-rich material within alveoli. The characteristic findings include an opaque, milky gross appearance; large, acellular, eosinophilic, blobs that are positive for periodic acid-Schiff; and pulmonary macrophages filled with material that is positive for periodic acid-Schiff. |
|
|
Smears from a pulmonary hamartoma show fragments of myxoid material, chondroid material, or both. Chondrocytes in lacunae, which are green with Papanicolaou’s stain, but unstained on H&E.
• benign glandular cells • immature fibromyxoid matrix and bland spindle cells • mature cartilage with chondrocytes in lacunae • adipocytes HMGI(Y) gene on chromosome 6p21. |
|
|
Patient under 40y
Peripheral discrete nodule Bland spindle cells storiform pattern |
Inflammatory myofibroblastic tumor
Unpredictable behavior ALK gene translocations |
|
|
Why do we separate out small cell carcinoma?
|
Usually metastatic at presentation, and treated with chemo.
Surgery for others |
|
|
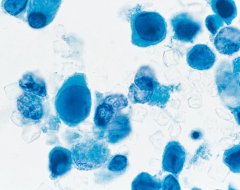
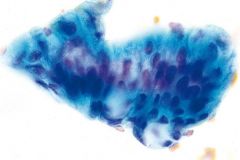
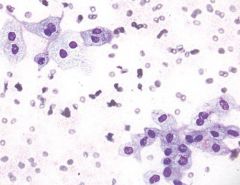
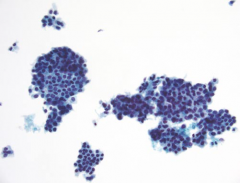
SCC, well-diff
• abundant dyshesive cells • polymorphic cell shapes: polygonal, rounded, elongated (fiber-like), tadpole shaped • dense cytoplasmic orangeophilia (Papanicolaou stain) • pyknotic nuclei • frequent anucleate cells abundant granular debris |
|
|
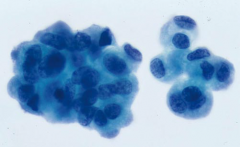
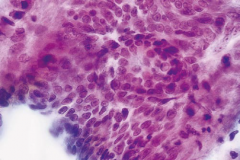
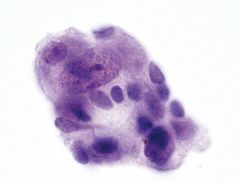
SCC, poorly differentiated
• large, cohesive clusters of elongated cells • rare to absent keratinization • large nuclei • coarse chromatin texture (“Idaho potato”) • ± prominent nucleoli |
|
|
Where are adenocarcinomas of the lung usually located? What molecular test?
|
Peripheral
EGFR |
|
|
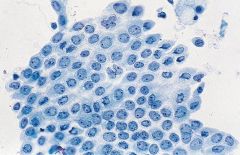
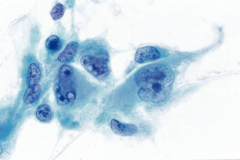
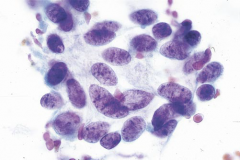
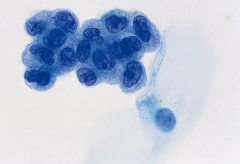
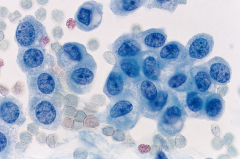
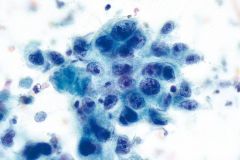
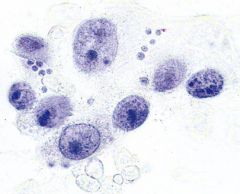
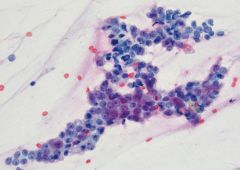
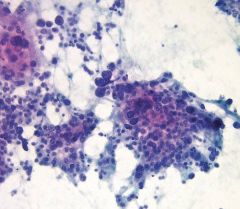
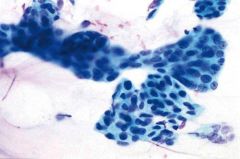
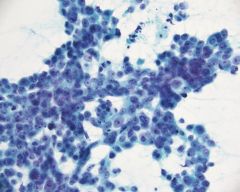
Adeno of the lung
The glandular differentiation can be easily appreciated. Cells are columnar, with polarized nuclei and single prominent nucleoli. |
|
|
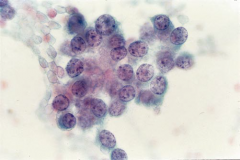
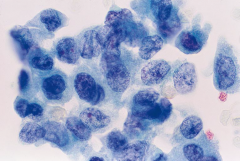
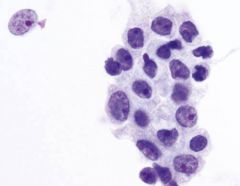
Mucinous BAC
(looks like papillary thyroid) uniform cells with pale, optically clear nuclei and inconspicuous nucleoli. Grooves and nuclear pseudoinclusions are often present |
|
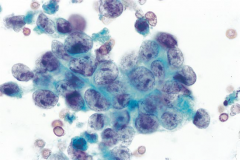
Peripheral mass
|
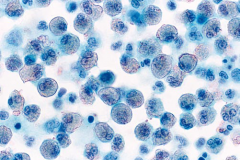
Large cell neuroendocrine carcinoma
• syncytial clusters and dispersed cells Palisading, MOLDING, ROSETTES MITOSES, NECROSIS • irregular nuclei • striking chromatin clearing • prominent, often multiple nucleoli • ill-defined, feathery cytoplasm |
|
|
Subtypes of Large cell carcinoma?
|
Basaloid carcinoma (NOT peripheral)
Lymphoepithelioma-like carcinoma Clear cell carcinoma Large cell neuroendocrine LCC with rhabdoid phenotype |
|
CD31positive lung mass
|
Epithelioid angiosarcoma
Mimics LCC CD31, CD34+ (30%+ cytokeratins...) |
|
|
Male, 30s, tumor resembles fetal lung
|
Pulmonary blastoma
-Biphasic neoplasm - Spindled component (myxoid, chondroid, osteoid, rhabdo) -Epithelial (tubules with piano key appearance) (Tumors of just the epithelioid portion called FETAL ADENOCA) |
|
|
Most specific neuroendocrine marker?
|
chromogranin A
|
|
|
Carcinoids (typical & atypical) vs SmCC/LCNEC?
|
MITOTIC RATE
<10/10hpf and lack of necrosis |
|
|
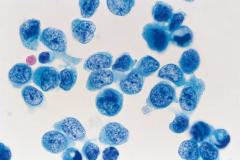
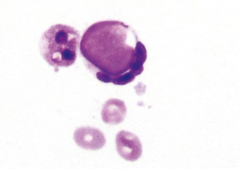
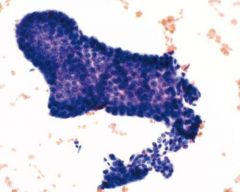
typical carcinoid
80% are POSITIVE for keratins! 30% are POSITIVE for TTF1! • loosely cohesive groups and single cells • rosette-like structures • round, plasmacytoid, or elongated cells • uniform nuclei with “salt and pepper” chromatin • ample granular cytoplasm • branching capillaries • mitoses uncommon • no necrosis RBCs |
|
|
Atypical carcinoid
All the features of typical carcinoid can be seen, but greater pleomorphism, slight nuclear enlargement, an increased number of mitoses, and focal necrosis are important distinguishing elements. |
|
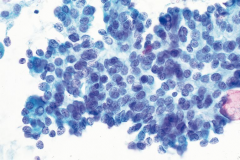
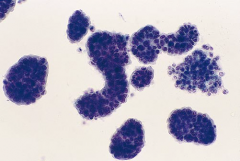
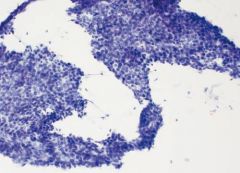
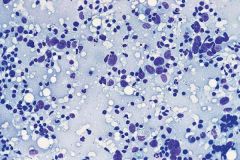
Central mass
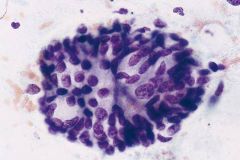
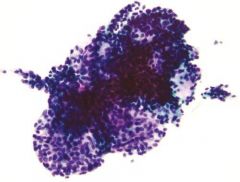
|
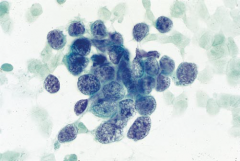
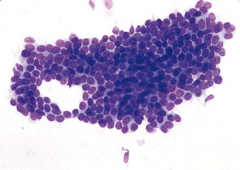
Small cell carcinoma
90% CENTRAL • small cells (twice the size of lymphocytes) • evenly dispersed, powdery chromatin • nuclear molding • small to indistinct nucleoli • paranuclear blue bodies • mitoses • background of nuclear debris and crush artifact |
|
HMB45+
|
Clear cell sugar tumor (PEComa)
HMB45+/MelanA+; keratin - Benign extremely rare and can occur in persons of all ages, most of whom are asymptomatic. It is usually a peripheral mass and ranges from 1 to 7 cm in greatest diameter. |
|
|
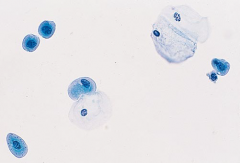
Normal voided urine
Umbrellas and squames |
|
|
Melamed Wolinska bodies
Seen in degenerated urothelial cells |
|
|
Even the small basal urothelial cells, because of their
scant cytoplasm and dark nuclei, are also occasionally mistaken for carcinoma cells. These cells are rare in voided urine but common in catheterized specimens and usually tightly clustered. Higher magnification reveals predominantly round, regular nuclear contours. |
|
|
Ileal loop specimen
Most cells in ileal loop specimens are degenerated intestinal cells that resemble macrophages |
|
|
Michaelis Gutman bodies
PAS, CALCIUM, IRON POSITIVE Malakoplakia (chronic granulomatous disease) Histiocytic inclusions |
|
|
6 features of HG urothelial ca?
|
1. Large nuclei
2. Scant cytoplasm 3. Coarse chromatin 4. Irregular nuclear contours 5. Single cells 6. Hyperchromasia Need all Can have all BUT coarse chromatin in stones |
|
|
Polyomavirus (JC, BK (papovaviruses))
Glassy nuclear inclusions Decoy cells (have smooth outlines) no clin sig |
|
|
High grade uroth ca
Numerous isolated malignant cells have enlarged, dark nuclei and an increased nuclear-to-cytoplasmic ratio. |
|
|
Low-grade uroth ca
Homogeneous cytoplasm, an increased nuclear-to-cytoplasmic ratio, and irregular nuclear outlines are associated with low-grade lesions, but are not specific. |
|
|
Benign stone atypia
|
|
|
Benign
|
|
|
malignant - HGUC
|
|
|
Schistosoma haemotobium
Nile River Valley Causes SCC bladder egg has terminal spine |
|
|
Adenoca of the bladder is rare and associated with what?
|
Bladder exstrophy & urachal remnants
|
|
|
FISH for uroth ca?
|
9- (deletion p16. Earliest!)
3+ 7+ 17+ |
|
|
Mesothelial cell markers
|
Calretinin
CA125 CD44 CK5/6 D240 WT1 |
|
pleural effusion
|
Causes of eosinophilic
#1: pneumothorax! vs idiopathic drug, parasite, infarction, |
|
|
DDx lymphocytic pleural effusion
|
Malignancy
Tb CABG |
|
Pleural effusion
|
Rheumatoid pleuritis
Abundant granular material in irregular clumps Macrophages, can be spindly Lack of mesos |
|
Pleural effusion
|
Lupus cell!
a neutrophil or macrophage that contains an ingested cytoplasmic particle called a hematoxylin body, that pushes the nucleus to one side |
|
|
#1 malignant pleural effusion in males? females?
Peritoneal? |
Pleural: M: LUNG, lymphoma; F: BREAST, lung
Peritoneal: M: lymphoma, GI; F: OV, breast |
|
|
Malignant mesothelioma
Many large groups, knobby edges Round central nuclei OFTEN HAVE A NORMAL N:C RATIO |
|
What virus is associated with this?
|
Primary effusion lymphoma
HHV8, often co-infected with EBV Seen in HIV pts. Poor px. Rare subtype DLBCL. CD45+ |
|
pleural fluid
|
Metastatic breast ca
Cannonball appearance |
|
Peritoneal washing
|
Endometriosis
|
|

Peritoneal washing
|
Reactive mesothelial cell in response to chemo
Very large |
|
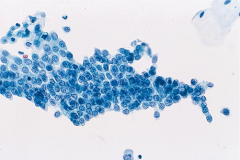
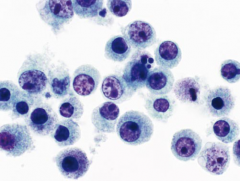
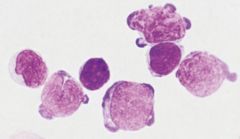
Plasma cells in CSF are associated with:
|
• viral meningitis (e.g., enterovirus, human immunodeficiency
virus [HIV]) • Lyme disease (IMAGE) • tuberculosis • cysticercosis • syphilis • multiple sclerosis |
|
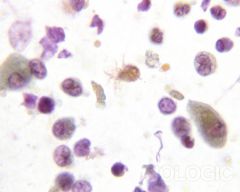
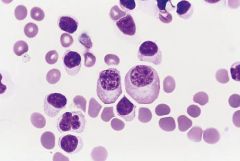
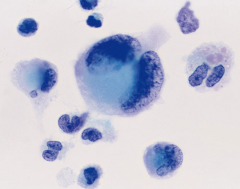
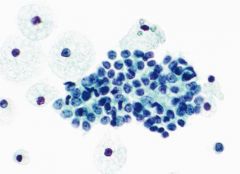
Macrophages in CSF are associated with:
|
• meningitis
• subarachnoid hemorrhage (IMAGE) • intraventricular hemorrhage • cerebral infarction • post-treatment inflammation • multiple sclerosis |
|
|
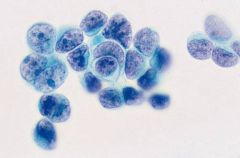
Neutrophils in CSF are associated with:
|
• peripheral blood contamination
• acute bacterial meningitis • CMV radiculopathy • Toxoplasma meningoencephalitis • viral meningitis (early stage) |
|
|
Eosinophils in CSF are associated with:
|
• parasites
• Coccidioides immitis • ventriculoperitoneal shunts • Rocky Mountain spotted fever cysticercosis |
|
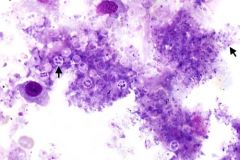
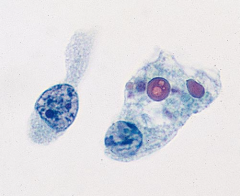
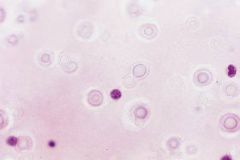
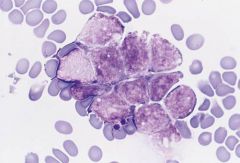
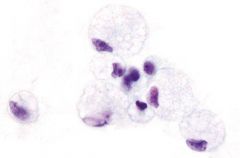
CSF
recurring attacks of fever, headache, and neck stiffness. Symptoms appear suddenly, last for 5 to 7 days, resolve spontaneously, but recur days or years later. |
Mollaret meningitis, form of aseptic meningitis
(aka idiopathic recurrent meningitis) “Mollaret cells,” monocytes with deep nuclear clefts that impart a footprint-like appearance to the nucleus, are seen within the first 24 hours of the onset of symptoms. They are characteristic of but not specific for MM; they can be seen in other diseases like sarcoidosis and Behçet disease |
|
|
In CSF, when do T cells predominate? B cells?
|
T cells - viral meningitis
B cells - Lyme |
|
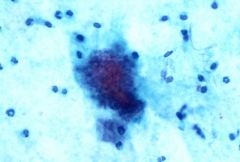
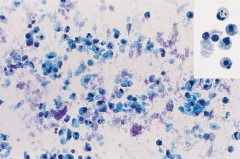
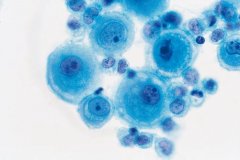
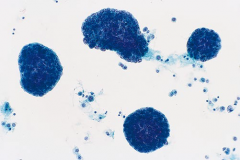
CSF, Pap stain
|
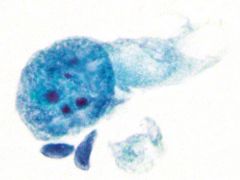
Cryptococcus
• round yeast forms • variable size: 5 to 15 μm diameter • pink or purple (Papanicolaou stain) • asymmetric, narrow-based budding • mucin-positive capsule • refractile artifact |
|
|
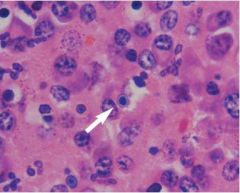
Toxoplasmosis
Neutrophils, monos, tachyzoites |
|

|
Cysticercosis
Taenia solium Numerous thin walled cysts in the brain 20-70% eos |
|
|
#1 cause of eosinophilic meningitis in Asia?
|
Angiostrongyliasis
Nematode (roundworm) Does not show discrete lesions on imaging (vs cysticercosis) |
|
|
CSF Ameba?
|
Naegleria fowleri
Primary amebic meningoencephalitis must be distinguished from an amebic brain abscess caused by Entamoeba histolytica. Amebae are not seen in the CSF with the latter infection. |
|
|
Primary CNS lymphoma
EBV+ in immunocompromised patients |
|
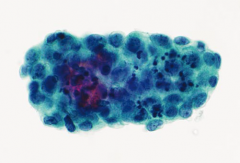
Cerebellar mass, kid
|
Medulloblastoma
MOLDING Small round blue cells Pineoblastomas look exactly like this. These tumors are in kids, and located in the pineal gland. |
|
csf
|
GBM
|
|
csf adolescent with 4th ventricle mass
|
ependymoma
round eccentric nuclei |
|
Infant
|
Atypical Teratoid/Rhabdoid Tumor (ATRT)
rhabdoid cells: medium-sized to large-sized cells with a round, eccentrically placed nucleus, and a prominent nucleolus. The cytoplasm is homogeneous and may contain a large, poorly defined, dense, inclusion-like structure that pushes aside the nucleus |
|
Child, 4th ventricle mass
|
Choroid plexus papilloma
Tumor cells are arranged in large, three-dimensional clusters of uniform cuboidal cells with a round or oval nucleus **Choroid plexus carcinomas are rare and exclusively in children** |
|
CNS, pineal mass
|
Germinoma
Any germ cell tumor can occur in the pineal/suprasellar region. Germinomas are the most common, occurring more often in males, and in young adults |
|
esophageal brushing
|
HSV
|
|
esophageal specimen
|
radiation change
Cellular and nuclear enlargement, multinucleation, and vacuolization of cytoplasm and nuclei are characteristic |
|
esophagus
|
Low grade dysplasia in background of Barrett's
|
|
esophagus
|
adenoca
Features favoring ca over HGD: More cells & more atypia (quantitative rather than qualitative) tumor diathesis |
|
Esophageal mass
|
Leiomyoma
|
|
gastric brushing
|
signet ring cell carcinoma
(in contrast to goblet cells, nuclei are hyperchromatic and angulated) |
|
duodenal brushing
|
well-differentiated endocrine (carcinoid) tumor
|
|
Gastric FNA
|
GIST
ckit+ (DOT-LIKE CYTOPLASMIC) |
|
Duodenum
|
Microsporidium
obligate intracellular spore-forming protozoon AIDS Bright red on Pap; 1-3um |
|
Duodenum
|
Cryptosporidium
2-5um HIV luminal surface |
|
Ampullary brushing
|
Adenoma
A crowded group of glandular cells with mucin depletion and an increased nuclear-to-cytoplasmic ratio is present. A gland opening is apparent. Despite the crowding, the arrangement is orderly. The nuclei are enlarged and elongated but significant atypia is absent |
|
Colon
|
TA
A cohesive group of stratified but orderly glandular cells with elongated nuclei is seen. Despite the increased nuclear-to-cytoplasmic ratio and hyperchromasia, significant atypia is absent |
|
Nipple discharge
|
Benign
Histiocytes/ foam cells |
|
Ductal lavage
|
Benign ductal cells with MYOEPS
|
|
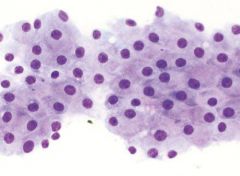
Breast
|
Apocrine metaplasia
Large, flat sheets of apocrine cells have distinct cytoplasmic borders, a centrally located nucleus, and a prominent nucleolus. Abundant granular cytoplasm is gray-purple |
|
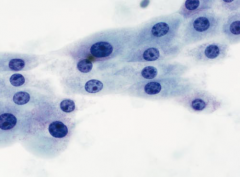
Breast
|
Benign ductal cells
Note the interspersed myoepithelial cells, which stand out like sesame seeds on a bun |
|
Breast
|
DCIS / suspicious for malignancy
The cells are loosely cohesive with marked nuclear pleomorphism, nucleoli, and a dirty background. Such specimens cannot be distinguished from invasive carcinoma |
|
Breast
|
Fibroadenoma
Hypercellular with folded sheets and many ANTLER-HORN CLUSTERS May have stripped nuclei |
|
breast
|
FA
|
|
breast
|
FA!
Note the prominent nuclear atypia with nucleoli. The tightness of the cluster and a background of single bipolar cells and stripped nuclei are important clues in avoiding an overdiagnosis of malignancy IDC has ISOLATED CELLS WITH INTACT CYTOPLASM |
|
Breast
|
Lactational change/ pregnancy
Numerous isolated epithelial cells or stripped nuclei Prominent nucleolus Wispy granular vacuolated cytoplasm Proteinaceous background |
|
Breast
|
Fat necrosis
Histiocytes with foamy vacuolated cytoplasm and oval nuclei |
|
Breast
|
Radiation change
pronounced nuclear enlargement but also concomitant cytomegaly. The nuclear to cytoplasmic ratio is maintained |
|
breast
|
cancer
in contrast to previous, the nuclei are irregular and the nuclear-to-cytoplasmic ratio is increased |
|
Male breast
|
Gynecomastia
Identical to FA |
|
Breast
|
"Papillary lesion"
Can't tell benign from malignant on cytology 3D sheets, usually bloody, usually central vs. FA: Papillary lesions are DYSHESIVE at edges |
|
Breast
|
Phyllodes tumor
Similar to FA but MORE cellular |
|
Breast
|
IDC / DCIS (can't tell on cytology)
HYPERCELLULAR isolated cells and poorly cohesive clusters of cells eccentric nucleus often protruding from the cytoplasm (i.e., “comet cells”) **ISOLATED CELLS |
|
Breast
|
COMET CELL!
IDC! |
|
breast
|
ILC
Sparsely cellular small to medium sized cells intracytoplasmic vacuoles Single filing Hyperchromatic kidney bean nucleus |
|
Breast in young patient
|
Medullary carcinoma
Well-circumscribed mass Numerous isolated cells Mitoses Abundant lymphs and plasma cells |
|
Breast
|
Mucinous / colloid carcinoma
Excellent prognosis Tightly cohesive 3D balls of cells Mucinous background BRANCHING CAPILLARIES |
|
Breast
|
Tubular carcinoma
Excellent prognosis Mimics FA Clusters of cells typically come to a sharp point (comma or cornucopia formations). By contrast, fibroadenomas (FAs) tend to have more rounded and less rigid outlines. The presence of angular epithelial groups, isolated epithelial cells, and nuclear atypia, warrants consideration of the diagnosis of TC |
|
Breast
|
Apocrine carcinoma
Rare subtype Granular cytoplasm Necrotic debris Protruding nuclei Variation in nuclear size but not much atypia |
|
Breast
|
Adenoid cystic carcinoma
Hyaline globules (also seen in collagenous spherulosis) |
|
|
Adenoid cystic board pearls
|
COLLAGEN IV stains background
p63 stains tumor cells. the only breast malignancy with myoepithelial cells! Excellent prognosis in breast, as opposed to poor px in salivary gland |
|

|
Ferruginous body
ASBESTOSIS |
|
|
Aspergillus fumigatus
Associated with CALCIUM OXALATE crytstals |
|
|
Characteristics of TB effusions
|
Yellow turbid fluid
Abundant lymphs (in clusters!) Few mesos UNCOMMON to see MNGCs |
|
|
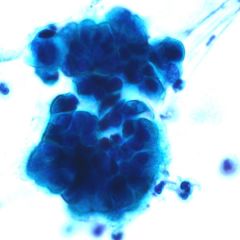
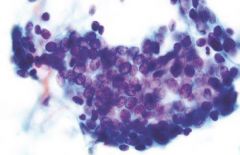
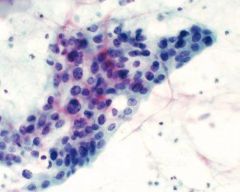
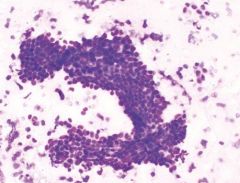
Central lung mass
|
Scc
Small cell ca |
|
|
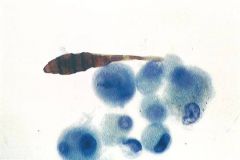
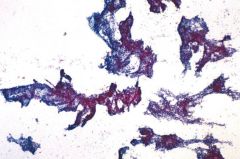
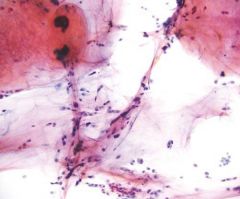
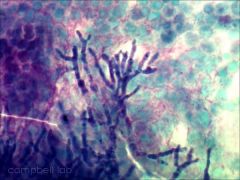
Herxheimer spirals
|
Marker of squamous diff
Long thin strands of keratin Benign or malignant |