Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
49 Cards in this Set
- Front
- Back
|
What are the tracts of the medial motor pathways? |
- Anterior Corticospinal Tract
- Vestibulospinal Tract - Reticulospinal Tract - Tectospinal Tract |
|
|
What is the function of the Lateral Vestibulospinal Tract?
|
- Maintain upright posture and balance
- Excites neurons innervating extensor (anti-gravity) muscles mainly in trunk and lower limbs |
|
|
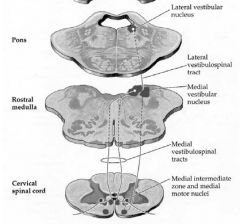
Where does the Lateral Vestibulospinal Tract arise?
|
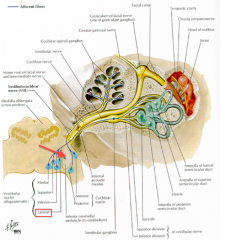
Lateral Vestibular Nucleus (Pons)
|
|
|
What do the axons of the Lateral Vestibulospinal Tract project to?
|
Ipsilaterally to all levels of spinal cord (trunk and lower limbs)
|
|
|
The descending axons of the Lateral Vestibulospinal Tract excite what?
|
Alpha- and gamma- lower motor neurons (LMNs) that innervate extensor muscles of trunk and lower limbs (may be direct or indirect, via interneurons)
|
|
|
What modifies the Lateral Vestibulospinal Tract?
|
- Input to lateral vestibular nucleus from cerebellum (floccular and nodular lobes)
- Sensory receptors in utricle, saccule, and semicircular canals via CN VIII |
|
|
What happens if there are lesions to the Vestibular N. or Vestibular Nucleus?
|
Stumbling and/or falling towards the side of the lesion
|
|

What is this dog using to stay balanced and maintain upright posture? What would happen if one of these pathways was cut on one side
|

- Lateral Vestibulospinal Tract is activating the antigravity muscles to maintain posture
- If one side is lesioned, fall to the side of the lesion (because opposite side is unopposed) |
|
|
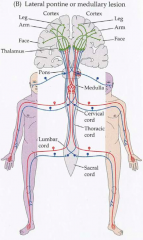
What can cause Lateral Medullary Syndrome?
|
Occlusion to vertebral a. or PICA
|
|
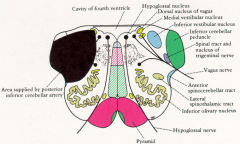
What are the symptoms of Lateral Medullary Syndrome?
|
- Dysphagia, dysarthria, decreased gag reflex (ipsilateral)
- Loss of pain and temp from face (ipsilateral) - Vertigo, nausea, vomiting, nystagmus (ipsilateral) - Loss of pain and temp. sensation from body (contralateral) |
|
|
What causes the dysphagia (difficulty swallowing), dysarthria (difficult articulation of speech), and decreased gag reflex in the Lateral Medullary Syndrome? Which side?
|
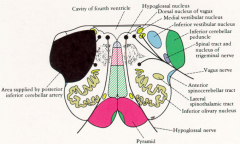
Lesion to nucleus ambiguus - CN XI and X - ipsilateral to lesion
|
|
|
What causes loss of pain and temperature from face in the Lateral Medullary Syndrome? Which side
|
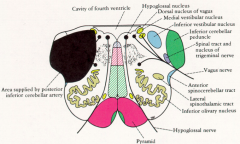
Lesion to spinal tract of V - descends ipsilaterally to spinal nucleus of V - ipsilateral to lesion
|
|
|
What causes the vertigo, nausea, vomiting, and nystagmus in the Lateral Medullary Syndrome? Which side?
|
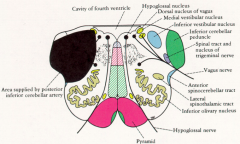
Lesion to Vestibular nuclei - ipsilateral to lesion
|
|
|
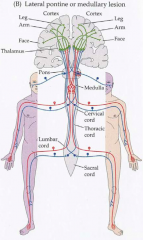
What causes the loss of pain and temperature sensation from body in the Lateral Medullary Syndrome? Which side?
|
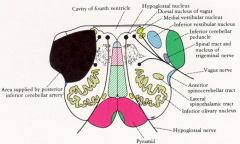
Lesion to anterolateral system (spinothalamic tract) which decussates in spinal cord - contralateral to lesion
|
|
|
If you see a checkerboard pattern of loss of pain and temperature in the face and body, what is the cause? Which side is ipsilatera/contralateral?
|
- Lateral Medullary Syndrome
- Face - ipsilateral - Body - contralateral |
|
|
What are the three functions of the Medial Vestibulospinal Tract?
|
- Adjusts head position in response to changes in posture
- Coordinates eye movements with each other - Coordinates eye movements to compensate for head movements (VOR) |
|
|
Where does the Medial Vestibulospinal Tract arise?
|
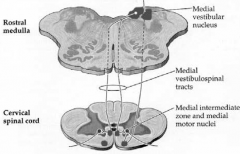
Medial Vestibular Nucleus (rostral medulla)
|
|
|
What do the axons of the Medial Vestibulospinal Tract project to?
|
- Project bilaterally (both ipsilateral and contralateral) to ventral horn of the cervical spinal cord and to LMNs associated with the spinal accessory nerve; within the medial longitudinal fasciculus (MLF)
- Project superiorly in the MLF to the nuclei of CNs III, IV, and VI - coordinates eye movements w/ each other and w/ head movements |
|
|
The descending axons of the Medial Vestibulospinal Tract inhibit what?
|
Inhibit α-LMNs and γ-LMNs controlling neck and axial muscles
|
|
|
What modifies the Medial Vestibulospinal Tract?
|
Sensory information from the medial vestibular nuclei modulates activity of this pathway to adjust head position in response to changes in posture
|
|
|
Which clinical conditions/processes can affect the Medial Vestibulospinal Tract?
|
- Internuclear Ophthalmoplegia (INO)
- Vestibulo-ocular Reflex (VOR) - Doll's Eyes Maneuver |
|
|
What is lesioned in an Internuclear Ophthalmoplegia (INO)?
|
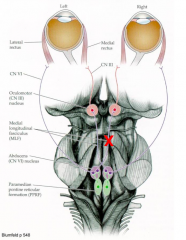
Lesion of the Medial Longitudinal Fasciculus (MLF)
|
|
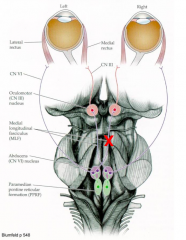
What are the symptoms of a lesion to the medial longitudinal fasciculus (MLF) on one side, between the nuclei of CN VII and III? Name of this disordre?
|

- On attempted horizontal gaze, eye on side of lesion cannot fully adduct (look medially)
- Eye on opposite side of lesion exhibits nystagmus to side eyes are trying to look - Left MLF injury --> left INO (left eye can't adduct / medial rectus not working) * Internuclear Ophthalmoplegia * |
|

What is the explanation for the symptoms of an Internuclear Ophthalmopolegia (INO)?
|
Input to medial rectus m. is interrupted by interruption of signal between abducens nucleus and contralateral oculomotor nucleus
|
|
|
What are some potential causes of Internuclear Ophthalmopolegia (INO)?
|
- Multiple Sclerosis (loss of myelination)
- Pontine infarcts - Tumor - Trauma |
|
|
What is the purpose of the Vestibulo-Ocular Reflex (VOR)?
|
Maintain vision on stationary object while the head or body is moving
|
|
|
What is the afferent component for the Vestibulo-Ocular Reflex (VOR)? Efferent?
|
- Afferent: neck proprioceptors and CN VIII
- Efferent: Medial Vestibulospinal Tract to abducens nucleus and via MLF to oculomotor nucleus |
|
|
What happens if the Vestibulo-Ocular Reflex (VOR) is normal?
|
If brainstem vestibular connections are intact, head movements result in conjugate eye movements that are equal and opposite to the side of the head movement
|
|
|
If your Vestibulo-Ocular Reflex (VOR) is abnormal, what does this mean?
|
- Eye movement goes with the head movement
- Brainstem dysfunction - Medial Vestibulospinal Tract is not intact |
|
|
What is the Doll's Eye Maneuver used for? What must you rule out before doing it?
|
- For brainstem evaluation in a comatose patient
- Cervical spinal injury must be ruled out before attempting this maneuver!!! |
|
|
What do you do in the Doll's Eye Maneuver?
|
- Turn head in one direction should cause eyes to turn in opposite direction
- Indicates pathways connecting vestibular nuclei in medulla to extraocular nuclei in pons and midbrain are functioning and brainstem is intact - Absence of response indicates brainstem dysfunction (interruption of MLF) |
|
|
What is the function of the Corticotectal Tract and the Tectospinal Tract?
|
- Facilitate reflexive turning movements of eyes and head
- Also facilitate upward gaze - Helps you move your eyes and head to something that caught your attention (e.g., pitcher sees baseball player trying to steal base and turns to look at him) |
|
|
Where do the Corticotectal fibers arise? Project to?
|
- Retina
- Visual cortex - Inferior parietal lobes - Project to Superior Colliculus |
|
|
Where do the Tectospinal fibers arise? Project to?
|
- Superior Colliculus
- Decussate in dorsal tegmentum - Terminate in contrlateral cervical spinal cord (CN XI nucleus - SCM) - Other fibers project to the pontine paramedian reticular formation (PRRF) and then via the medial longitudinal fasciculus (MLF) to control extraocular muscles for upward gaze |
|
|
Which clinical concern affects the Corticotectal Tract and Tectospinal Tract?
|
Parinaud's Syndrome / Dorsal Midbrain Syndrome / Collicular Syndrome
|
|
|
What is lesioned in Parinaud's Syndrome / Dorsal Midbrain Syndrome / Collicular Syndrome?
|
- Superior Colliculus or Posterior Commissure of Midbrain
- Leads to a lesion of the Corticotectal Tract / Tectospinal Tract (control movements of eye, head, and upward gaze) |
|
|
What are the implications of a lesion to the superior colliculus or posterior commissure of the midbrain?
|
- Impaired vertical / upward gaze
- Large, irregular pupils w/ light-near dissociation (pupils do not constrict w/ light but do constrict w/ accommodation) - Eyelid abnormalities (retraction or ptosis) - Convergence - retraction nystagmus (attempted upward gaze --> eyes oscillate between convergence and retraction) |
|
|
If a patient can not gaze upward, what is this a sign of?
|
- Parinaud's Syndrome / Dorsal Midbrain Syndrome / Collicular Syndrome
- Superior Colliculus or Posterior Commissure of Midbrain lesion - Leads to a lesion of the Corticotectal Tract / Tectospinal Tract (control movements of eye, head, and upward gaze) |
|
|
What are some common causes of Parinaud's Syndrome / Dorsal Midbrain Syndrome / Collicular Syndrome?
|
- Hydrocephalus resulting from aqueductal stenosis
- Pineal gland tumors |
|
|
What is the reticular formation composed of?
|
Scattered groups of neuron cell bodies and fibers that extend throughout the brain
|
|
|
What are the functions of the Reticulospinal Tracts?
|
- Help maintain upright posture by influencing voluntary and reflexive movements
- Inhibit (LRST) or exciting (MRST) motor neurons innervating axial musculature - Convey autonomic information from higher levels to influence respiration, circulation, sweating, shivering, pupil dilation, and sphincter muscles of GI and urinary tracts |
|
|
What is the other name for the Lateral Reticulospinal Tract? Function?
|
- Medullary Reticulospinal Tract
- M for Medulla = Mellows = Inhibits extensor spinal reflex actively by inhibiting spinal motor neurons (Also, ascending fibers project to intralaminar and thalamic nuclei to play a role in arousal and sleep) |
|
|
What is the other name for the Medial Reticulospinal Tract? Function?
|
- Pontine Reticulospinal Tract
- P for Pontine = Pump up! = Excites spinal motor neurons that innervate axial muscles and leg extensors |
|
|
What is the pathway of the Lateral (Medullary) Reticulospinal Tract (LRST)?
|
- Axons (crossed and uncrossed) descend bilaterally through lateral funiculus to all spinal cord levels
- Also, ascending fibers of LRST project to intralaminar and and thalamic nuclei (arousal and sleep) |
|
|
What is the pathway of the Medial (Pontine) Reticulospinal Tract (LRST)?
|
Axons descend ipsilaterally in the anterior funiculus to all spinal cord levels
|
|
|
Which clinical condition affects the Medial and Lateral Reticulospinal Tracts?
|
Decerebrate Posturing / Decerebrate Rigidity
|
|
|
What are the symptoms of Decerebrate Posturing / Decerebrate Rigidity?
|
- Increased muscle tone
- Extension of upper and lower limbs with arms adducted and medially rotated - Arched back - Feet extended - Toes curled |
|
|
What is the explanation for the symptoms of Decerebrate Posturing / Decerebrate Rigidity?
|
- Transection of brain between superior and inferior colliculi in midbrain
- Removes excitatory cortical input to INHIBITORY LRST (medulla) - Ascending input to MRST (pons) is still intact - Facilitory influence of MRST is now unopposed by inhibitory influence of LRST - Leads to facilitation of extensor motor neurons |
|
|
What is Locked-In Syndrome?
|
Patient is aware and awake but cannot move or communicate verbally due to complete paralysis of nearly all voluntary muscles in body except for eyes
|