![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
154 Cards in this Set
- Front
- Back
|
Midline back pain |
Assess for musculoligamentous injury, disc herniation, vertebral collapse, spinal cord metastases, and, rarely, epidural abscess |
|
|
Back pain off the midline |
Assess for muscle strain, sacroiliitis, trochanteric bursitis, sciatica, and hip arthritis; also for renal conditions like pyelonephritis or stones. |
|
|
Sciatica |
Radicular gluteal and posterior leg pain in the S1 distribution that increases with cough or Valsalva |
|
|
Spinal stenosis |
Leg pain that resolves with rest and/or lumbar forward flexion |
|
|
Bowel or bladder dysfunction (usually urinary retention with overflow incontinence), especially if there is saddle anesthesia or perineal numbness. |
Cauda equina syndrome from S2-4 mideline disc or tumor |
|
|
Key warning signs for serious underlying systemic disease |
In cases of low back pain plus another indicator, there is a 10% probability of serious systemic disease. |
|
|
Radicular Neck Pain |
Arises from spinal nerve compression, most commonly C7 followed by C6. Unlike low back pain, it is usually caused by foraminal impingement from degenerative joint changes (70% to 75%) rather than disc herniation (20% to 25%). |
|
|
Monoarticular Pain |
Pain in one joint
Suggests injury, monoarticular arthritis, possible tendinitis, or bursitis. |
|
|
Trochanteric bursitis |
Lateral hip pain near the greater trochanter |
|
|
Migratory pattern of spread of joint pain |
Rheumatic fever Gonococcal arthritis |
|
|
Polyarticualr: Progressive additive pattern with symmetric involvement of joint pain |
Rheumatoid arthritis
Inflammatory arthritides are more common in women |
|
|
Extra-ocular joint pain |
Involving bones, muscles, and tissues around the joint such as the tendons, bursae or even overlying skin
Occurs in: Bursitis Tendinitis Inflammation of tendon sheaths (tenosynovitis) Sprains from stretching or tearing of ligaments |
|
|
Severe pain of rapid onset in a red, swollen joint |
Acute septic arthritis Gout
In children, consider osteomyelitis in bone contiguous to a joint |
|
|
Fever, chills, warmth, redness with joint pain |
Septic arthritis
Also, gout or possible rheumatic fever |
|
|
Pain, swelling, loss of active motion, or "locking" of joints |
Articular joint pain |
|
|
Loss of active but not passive motion and tenderness outside the joint |
Nonarticular joint pain |
|
|
Degenerative joint disease |
Stiffness and limited motion after inactivity, sometimes called gelling, occurs in degenerative joint disease but usually lasts only a few minutes |
|
|
Rheumatoid arthritis |
Stiffness lasting 30 minutes or more; also occurs in fibromyalgia and Polymyalgia rheumatica (PMR)
Also present in other inflammatory arthritides
Process: Chronic inflammation of synovial membranes with secondary erosion of adjacent cartilage and bone, and damage to ligaments and tendons
Common Locations: Hands (PIP and MCP joints), Feet (Metatarsophalangeal joints), wrists, knees, elbows, ankles
Pattern of Spread: Symmetrically additive: progresses to other joints while persisting in the intial ones
Onset: Usually insidious
Progression and Duration: Often chronic, with remissions and exacerbations
Swelling: Frequent swelling of synovial tissue in joints or tendon sheaths; also subcutaneous nodules
Redness, Warmth, & Tenderness: Tender, often warm, but seldom red
Stiffness: Prominent, often for an hour or more in the mornings, also after inactivity
Limitations of Motion: Often develops
Generalized Symptoms: Weakness, fatigue, weight loss, and low fever are common
|
|
|
Joint Pain and Systemic Disorders: Systemic lupus erythematosus |
Butterfly rash on the cheeks |
|
|
Joint Pain and Systemic Disorders: Psoriatic arthirtis |
DIP joint pain
Scaly rash and pitted nails of psoriasis |
|
|
Joint Pain and Systemic Disorders: Gonococcal arthritis |
A few papules, pustules, or vesicles on reddened bases, located on the distal extremities
Preceding sore throat
Symptoms of urethritis |
|
|
Joint Pain and Systemic Disorders: Lyme disease |
An expanding erythematous patch early in an illness
Lyme disease with CNS involvement: Mental status change, facial or other weakness, stiff neck |
|
|
Joint Pain and Systemic Disorders: Serum sickness, drug reaction |
Hives |
|
|
Joint Pain and Systemic Disorders: Reiter's syndrome |
Erosions or scaling on the penis and crusted, scaling papules on the soles and palms
Red, burning, and itchy eyes
Symptoms of urethritis
Includes arthritis, urethritis, and uveitis |
|
|
Joint Pain and Systemic Disorders: Arthritis rubella |
Maculopapular rash of rubella |
|
|
Joint Pain and Systemic Disorders: Hypertrophic osteoarthropathy |
Clubbing of the fingernails |
|
|
Joint Pain and Systemic Disorders: Behcet's syndrome |
Red, burning, and itchy eyes |
|
|
Joint Pain and Systemic Disorders: Acute rheumatic fever |
Preceding sore throat |
|
|
Joint Pain and Systemic Disorders: Arthritis with ulcerative colitis, regional enteritis, scleroderma |
Diarrhea, abdominal pain, cramping |
|
|
Symmetry of involvement of joints: Acute involvement of only one joint |
Trauma, septic arthritis, or gout |
|
|
Joint deformities or malalignment of bones or joints |
Dupuytren's contracture Bowlegs (Genu varum) Knock-knees (Genu valgum) |
|
|
Subcutaneous nodules of muscle tissue |
Rheumatoid arthritis Rheumatic fever |
|
|
Serous effusion of muscle tissue |
Trauma |
|
|
Crepitus over inflamed joints or over the inflamed tendon sheaths |
Osteoarthritis Tenosynovitis |
|
|
Decreased range of motion |
Arthritis Inflammation of tissues around a joint Fibrosis in or around a joint Bony fixation (ankylosis) |
|
|
Ligamentous laxity of the ACL |
Knee trauma |
|
|
Muscle atrophy or weakness |
Rheumatoid arthritis |
|
|
Signs of Inflammation and Arthritis: Palpable bogginess or doughiness of the synovial membrane |
Synovitis
Often accompanied by effusion |
|
|
Signs of Inflammation and Arthritis: Palpable joint fluid |
Effusion |
|
|
Signs of Inflammation and Arthritis: Tenderness over the tendon sheaths |
Tendinitis |
|
|
Signs of Inflammation and Arthritis: Increased warmth |
Arthritis Tendinitis Bursitis Osteomyelitis |
|
|
Signs of Inflammation and Arthritis: Diffuse tenderness and warmth over a thickened synovium |
Arthritis Infection |
|
|
Signs of Inflammation and Arthritis: Focal tenderness |
Injury |
|
|
Signs of Inflammation and Arthritis: Redness over a tender joint |
Septic or gouty arthritis Possibly Rheumatoid arthritis |
|
|
Scoliosis |
May cause elevation of one shoulder
Lateral and rotatory curvature of the spine to bring the head back to midline
Often becomes evident during adolescence, before symptoms appear
Deformity of the thorax on forward being, especially differences in height of the scapulae |
|
|
Anterior Dislocation of the Shoulder |
Rounded lateral aspect of the shoulder appears flattened |
|
|
Rotator Cuff Tear |
Atrophy of the supraspinatus and infraspinatus with increased prominence of scapular spine can appear within 2 to 3 weeks |
|
|
Swelling of the Joint Capsule |
A significant amount of synovial fluid is needed before the glenohumeral joint capsule appears distended. Swelling of the acromioclavicular joint is easier to identify since it is more superficial |
|
|
Sprains, tears and tendon rupture of the rotator cuff |
Tenderness over the SITS muscle insertions and inability to abduct the arm above shoulder level
Commonly the supraspinatus |
|
|
Synovitis of the glenohumeral joint |
Tenderness and effusion
If synovitis is minimal, it cannot be detected on palpation |
|
|
Moderate to large effusion of capsule and synovial membrane of rotator cuff |
Margins of the capsule and synovial membrane are palpable |
|
|
Restricted ROM of shoulder |
Bursitis Capsulitis Rotator cuff tears or sprains Tendinitis |
|
|
Diffuse swelling of the wrist and hand |
Arthritis or infection
Local swelling suggests a ganglion |
|
|
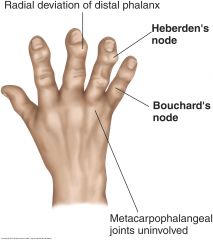
Osteoarthritis of wrists, hands, or fingers |
Look for Heberden's nodes at the DIP joints - usually hard and painless, they affect the middle-aged or elderly; often associated with arthritic changes in other joints. Flexion and deviation deformities may develop
Bouchard's nodes at the PIP joints are less common. The MCP joints are spared |
|
|
Rheumatoid arthritis of the wrists, hands, or fingers |
Symmetric deformity in the PIP, MCP and wrist joints, and ulnar deviation
Swelling and/or tenderness if bilateral and of several weeks' duration
MCPs are often boggy or tender, but are rarely involved in osteoarthritis
PIP changes are seen |
|
|
Occurs in median nerve compression from carpal tunnel syndrome |
Thenar atrophy |
|
|
Ulnar nerve compression |
Hypothenar atrophy |
|
|
Dupuytren's contractures |
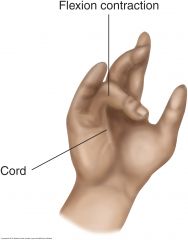
Flexion contractures in the ring, fifth, and third fingers arise from thickening of the palmar fascia
First sign s a thickened nodule overlying the flexor tendon of the ring finger and possibly the little finger near the distal palmar crease. Subsequently, the skin in this area puckers, and a thickened fibrotic cord develops between palm and finger. Finger extension is limited, but flexion is usually normal. Flexion contracture of the fingers may gradually ensue.
|
|
|
Colles' fracture |
Tenderness over the distal radius occurs from a fall, especially in patients with osteoporosis. Any tenderness or bony step-offs are suspicious for fracture |
|
|
de Quervain's tenosynovitis and Gonococcal tenosynovitis |
Tenderness over the extensor and abductor tendons of the thumb at the radial styloid
Ask patient to grasp thumb against the palm and then move wrist toward the midline in ulnar deviation; pain will occur with inflammation of the abductor pollicis longus and extensor pollicis brevis tendons and tendon sheaths
More common in women |
|
|
Scaphoid fracture |
Tenderness over the "snuffbox"
The most common injury of the carpal bones
Poor blood supply puts the scaphoid bone at risk for avascular necrosis |
|
|
Pain with pressure the carpals, metacarpals, and phalanges |
Synovitis in the MCPs |
|
|
Carpometacarpal arthritis |
Pain at the base of the thumb |
|
|
Heberden’s nodes |

Hard dorsolateral nodules on the DIP joints are common is osteoarthritis
|
|
|
Restricted ROM of Wrist |
Arthritis Tenosynovitis Dupuytren's contracture |
|
|
Carpal Tunnel Syndrome |
Often related to repetitive motion with wrists flexed (as in keyboard use or mail-sorting), pregnancy, rheumatoid arthritis, diabetes, or hypothyroidism
Decreased sensation in the median nerve distributions of the hand |
|
|
Decreased grip strength |
Positive sign for weakness of finger flexors and/or intrinsic muscles of the hand
May also result from pain from degenerative joint changes |
|
|
Thumb Abduction |
Ask patient to raise thumb straight up as you apply downward resistance
Weakness is a positive test
Weak thumb abduction, diagrams that confirm sensory symptoms in the hand, and decreased sensation roughly double the likelihood of carpal tunnel disease |
|
|
Tinel's sign |
For median nerve compression
Tap lightly over the course of the median nerve in the carpal tunnel
Aching and numbness in the median nerve distribution is a positive test
Does not reliably predict positive electrodiagnosis of carpal tunnel disease |
|
|
Phalen's sign |
For median nerve compression
Ask patient to hold wrists in flexion for 60 seconds or press the backs of both hands together to form right angles
Numbness and tingling in the median nerve distribution within 60 seconds is a positive test
Does not reliably predict positive electrodiagnosis of carpal tunnel disease |
|
|
Torticollis |
Lateral deviation and rotation of the head from contraction of the sternocleidomastoid muscle |
|
|
Tenderness of the spinous process of each vertabra |
Fracture or dislocation if preceded by trauma Underlying infection Arthritis |
|
|
Tenderness of facet joints (between the cervical vertebrae about 1 inch lateral) |
Arthritis, especially at the facet joints between C5 and C6 |
|
|
Spondylolisthesis |
Step-offs of vertebra or forward slippage of one vertebra, which may compress the spinal cord
Vertebral tenderness is suspicious for fracture or infection |
|
|
Tenderness over the sacroiliac joint |
Sacroiliitis Ankylosing spondylitis |
|
|
Pain on percussion of the spine |
Osteoporosis Infection Malignancy |
|
|
Thoracic kyphosis |
Occurs with aging
In children, a correctable structural deformity should be pursued |
|
|
Unequal shoulder heights |
Scoliosis
Sprengel's deformity of the scapula, from attachment of an extra bone or band between the upper scapula and C7
"Winging" of the scapula, from loss of innervation of the serratus anterior muscle by the long thoracic nerve
Contralateral weakness of the trapezius |
|
|
Unequal heights of the iliac crests or pelvic tilt |
Unequal lengths of the legs and disappear when a block is placed under the shorter limb
Scoliosis and hip abduction or adduction
"Listing" of the trunk to one side is seen with a herniated lumbar disc |
|
|
Spina bifida can be overlooked by: |
Birthmarks Port-wine stains Hairy patches Lipomas |
|
|
Neurofibromatosis |
Cafe-au-lait spots Skin tags Fibrous tumors |
|
|
Spasms on paravertebral muscles |
Occurs in degenerative and inflammatory processes of muscles, overuse, prolonged contraction from abnormal posture, or anxiety |
|
|
Sciatic nerve tenderness |
Herniated disc or mass lesion impinging on the contributing nerve roots
Nerve is difficult to palpate in most patients |
|
|
Herniated intervertebral discs |
Most common at L5-S1 or L4-L5
May produce tenderness of the spinous processes, the intervertebral joints, the paravertebral muscles, the sacrosciatic notch, and the sciatic nerve |
|
|
Rheumatoid arthritis of the spine |
Tenderness of the intervertebral joints
Tenderness at C1-C2 suggests possible risk for subluxation and high cervical cord compression and needs prompt additional assessment |
|
|
Kidney infection |
Tenderness in the costovertebral angles
Rather than a musculoskeletal problem |
|
|
Limitations in ROM of neck |
Stiffness from arthritis Pain from trauma Overuse Muscle spasm such as torticollis |
|
|
Persistence of lumbar lordosis |
Muscle spasm Ankylosing spondylitis |
|
|
Decreased spinal mobility |
Osteoarthritis Ankylosing spondylitis |
|
|
Flexion deformity of the hip |

As the opposite hip is flexed (with the thigh against the chest), the effected hip does not allow full hip extension, and the affected thigh appears flexed
May be masked by an increase, rather than flattening, in lumber lordosis and an anterior pelvic tilt
|
|
|
Hip osteoarthritis |
Restricted abduction |
|
|
Restrictions of internal and external rotation |
Sensitive indicators of hip disease such as arthritis |
|
|
Problems with patellar tracking, for example in patients with shallower grooves, especially women |
Can lead to arthritis, anterior knee pain, and patellar dislocation
|
|
|
In women, quadriceps contraction... |

Tends to have a more lateral pull that alters patellar tracking, contributing to anterior knee pain
|
|
|
Stumbling or "giving way" of the knee during heel strike |
Quadriceps weakness Abnormal patellar tracking |
|
|
Genu varum |
Bowlegs |
|
|
Genu valgum |
Knock-knees |
|
|
Flexion contracture (inability to extend fully) |
Seen in limb paralysis or hamstring tightness |
|
|
Swelling over the patella |
Prepatellar bursitis |
|
|
Swelling over the tibial tubercle |
Infrapatellar or Anserine (more medial) bursitis |
|
|
Osteoarthritis of the knee |
Likely when there are tender bony ridges along the joint margins, genu varum deformity, and stifness lasting 30 minutes or less' crepitus with flexion and extension may also be present
|
|
|
Medial meniscus tear with point tenderness is more common... |

After trauma
|
|
|
MCL tenderness after injury... |
Suspicious for an MCL tear
LCL injuries are less frequent |
|
|
Tenderness over the patellar tendon or inability to extend the knee suggests... |
A partial or complete tear of the patellar tendon |
|
|
Pain and crepitus of the knee suggest... |
Roughening of the patellar undersurface that articulates with the femur
|
|
|
Pain with compression and with patellar movement during quadriceps contraction suggests... |
Chondromalacia Degenerative patella (the patellofemoral syndrome) |
|
|
Swelling above and adjacent to the patella suggests... |
Synovial thickening or effusion in the knee joint |
|
|
Thickening, bogginess, or warmth around the knee indicates... |
Synovitis Nontender effusions from osteoarthritis |
|
|
Prepatellar bursitis |
"Housemaid's knee"
Arises from excessive kneeling |
|
|
Anserine bursitis |
From running Valgus knee deformity Fibromyalgias Osteoarthritis |
|
|
Popliteal or "Baker's" cyst |
From distension of the gastrocnemius semimembranosus bursa from underlying arthritis or trauma |
|
|
Positive bulge sign consistent with an effusion |
A fluid wave or bulge on the medial side between the patella and the femur |
|
|
Large effusion of the knee joint |
Suprapatellar compression ejects fluid into the spaces adjacent to the patella
A palpable fluid wave signifies a positive "balloon sign"
A returning fluid wave into the suprapatellar pouch confirms an effusion
A palpable patellar click with compression may also occur, but yields more false positives |
|
|
Ruptured Achilles tendon |
Defect in the muscles (gastrocnemius and soleus) with tenderness and swelling |
|
|
Achilles tendinitis |
Tenderness and thickening of the tendon above the calcaneus, sometimes with a protuberant posterolateral bony process of the calcaneus |
|
|
Test the integrity of the Achilles tendon: Ruptured Achilles tendon |
Absence of plantar flexion Sudden severe pain "like a gunshot wound" An ecchymosis from the calf into the heel A flat-footed gait with absence of "toe-off" |
|
|
Medial Meniscus and Lateral Meniscus: McMurray Test |
Tear of the posterior portion of the medial meniscus: A click or pop along the medial joint with valgus stress, external rotation, and leg extension
The tear may displace meniscal tissue, causing "locking" on full knee extension |
|
|
Medial Collateral Ligament (MCL): Abduction (or Valgus) Stress Test |
Pair or a gap in the medial joint line points to ligamentous laxity and a partial tear of the MCL
Most injuries are on the medial side |
|
|
Lateral Collateral Ligament (LCL): Adduction (or Varus) Stress Test |
Pain or a gap in the lateral joint line points to ligamentous laxity and a partial tear of the LCL |
|
|
Osteoarthritis (degenerative joint disease) |
Process: Degeneration and progressive loss of cartilage within the joints, damage to underlying bone, and formation of new bone at the margins of the cartilage
Common Locations: Knees, hips, hands (DIP and sometimes PIP joints), cervical and lumbar spine, and wrists (first carpometacarpal joint); also joints previously injured or diseased
Pattern of Spread: Additive; however, only one joint may be involved
Onset: Usually insidious
Progression & Duration: Slowly progressive, with temporary exacerbations after periods of overuse
Swelling: Small effusions in the joints may be present, especially in the knees; also bony enlargement
Redness, Warmth, and Tenderness: Possibly tender, seldom warm, and rarely red
Stiffness: Frequent but brief (usually 5-10 min), in the morning and after inactivity
Limitation of Motion: Often develops
Generalized Symptoms: Usually absent |
|
|
Gouty Arthritis: Acute Gout |
Process: An inflammatory reaction to microcrystals of monosodium urate
Common Locations: Base of the big toe (the first metatarsophalangeal joint), the instep or dorsa of feet, the ankles, knees and elbows
Pattern of Spread: Early attacks usually confined to one joint
Onset: Sudden; often at night; often after injury, surgery, fasting, or excessive food or alcohol intake. Gradual development of chronicity with repeated attacks
Progression and Duration: Occasional isolated attacks lasting days up to 2 weeks; they may get more frequent and severe, with persisting symptoms
Swelling: Present within and around the involved joint
Redness, Warmth, and Tenderness: Exquisitely tender, hot and red
Stiffness: Not evident
Limitation of Motion: Motion is limited primarily by pain
Generalized Symptoms: Fever may be present. Consider also septic arthritis |
|
|
Gouty Arthritis: Chronic Tophaceous Gout |
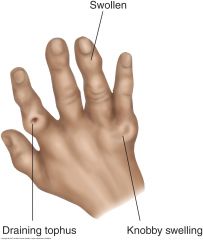
Can mimic rheumatoid arthritis and osteoarthritis
Process: Multiple local accumulations of sodium urate in the joints (discharge white chalklike urates) and other tissues (tophi), with or without inflammation
Common Locations: Feet, ankles, wrists, fingers, and elbows
Pattern of Spread: Additive, not so symmetric as rheumatoid arthritis
Onset: Gradual development of chronicity with repeated attacks
Progression and Duration: Chronic symptoms with acute exacerbations
Swelling: Present as tophi in joints, bursae, and subcutaneous tissues. Check ears and extensor surfaces for tophi
Redness, Warmth, & Tenderness: Tenderness, warmth, and redness may be present during exacerbations
Generalized Symptoms: Possibly fever; patient may also develop symptoms of renal failure and renal stones |
|
|
Polymyalgia Rheumatica |
Process: A disease of unclear etiology in people older than 50, especially women; overlaps with giant cell arteritis
Common Locations: Muscles of the hip and shoulder girdles and neck; symmetric
Onset: Insidious or abrupt, even appearing overnight
Progression and Duration: Chronic but ultimately self-limiting
Swelling: Swelling and edema may be present over dorsum of hands, wrists, feet
Redness, Warmth, and Tenderness: Muscles often tender, but not warm or red
Stiffness: Prominent, especially in the morning
Limitation of Motion: Pain restricts movement, especially in shoulders
Generalized Symptoms: Malaise, depression, anorexia, weight loss, and fever, but no true weakness |
|
|
Fibromyalgia Syndrome |
Process: Widespread musculoskeletal pain and tender points. Mechanism may involve aberrant pain signaling and amplification
Common Locations: "All over," but especially in the neck, shoulders, hands, low back and knees
Pattern of Spread: Shifts unpredictably or worsens in response to immobility, excessive use, or exposure to cold
Onset: Variable
Progression and Duration: Chronic, with "ups and downs"
Swelling: None
Redness, Warmth and Tenderness: Multiple specific and symmetric tender "trigger points," often not recognized until examination
Stiffness: Present, especially in the morning
Limitation of Motion: Absent, though stiffness is greater at the extremes of movement
Generalized Symptoms: A disturbance of sleep, usually associated with morning fatigue; overlaps with depression |
|
|
Olecranon Bursitis |

Swelling and inflammation of the olecranon bursa may results from trauma, gout, or rheumatoid arthritis. The swelling is superficial to the olecranon process and may reach 6 cm in diameter. Consider aspiration for both diagnosis and symptomatic relief
|
|
|
Rheumatoid Nodules |

Subcutaneous nodules may develop at pressure points along the extensor surface of the ulna in patients with rheumatoid arthritis or acute rheumatic fever. They are firm and nontender. They are not attached to the overlying skin but may be attached to the underlying periosteum. They can develop in the area of the olecranon bursa, but often occur more distally
|
|
|
Arthritis of the Elbow |

Synovial inflammation or fluid is felt best in the grooves between the olecranon process and the epicondyles on either side. Palpate for a boggy, soft, or fluctuant swelling and for tenderness. Causes include rheumatoid arthritis, gout and pseudogout, osteoarthritis, and trauma. Patients report pain, stiffness, and restricted motion
|
|
|
Epicondylitis |

Lateral epicondylitis (tennis elbow) follows repatitive extension of the wrist or pronation-supination of the forearm. Pain and tenderness develop 1 cm distal to the lateral epicondyle and possibly in the extensor muscles close to it. When the patient tries to extend the wrist against resistance, pain increases
Medial epicondylitis (pitcher's, golfer's, or Little League elbow) follows repetitive wrist flexion, as in throwing. Tenderness is maximal just lateral and distal to the medial epicondyle. Wrist flexion against resistance increases the pain
|
|
|
Acute Rheumatoid Arthritis |
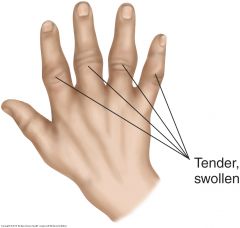
Tender, painful, stiff joints in rheumatoid arthritis, usually with symmetric involvement on both sides of the body. The PIP, MCP and wrist joints are the most frequently affected. Note the fusiform or spindle-shaped swelling of the PIP joints in acute disease
|
|
|
Chronic Rheumatoid Arthritis |
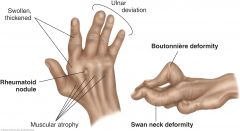
In chronic disease, note the swelling and thickening of the MCP and PIP joints. ROM becomes limited, and fingers may deviate toward the ulnar side. The interosseous muscles atrophy. The fingers may show "swan neck" deformities (hyperextension of the PIP joints with fixed flexion of the DIP joints). Less common is a boutonniere deformity (persistent with flexion of the PIP joint with hyperextension of the DIP joint). Rheumatoid nodules are seen in the acute or the chronic stage
|
|
|
Trigger Finger |

Caused by a painless nodule in a flexor tendon in the palm, near the metacarpal head. The nodule is too big to enter easily into the tendon sheath during extension of the fingers from a flexed position. With extra effort or assistance, the finger extends and flexes with a palpable and audible snap as the nodule pops into the tendon sheath. Watch, listen, and palpate the nodule as the patient flexes and extends the fingers.
|
|
|
Thenar Atrophy |
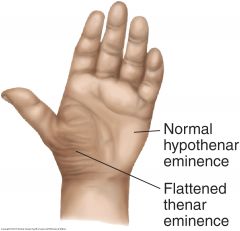
Suggests a median nerve disorder such as carpal tunnel syndrome. Hypothenar atrophy suggests an ulnar nerve disorder.
|
|
|
Ganglion |

Ganglia are cystic, round, usually nontender swellings along tendon sheaths or joint capsules, frequently at the dorsum of the wrist. The cyst contains synovial fluid arising from erosion or tearing of the joint capsule or tendon sheath and trapped in the cystic cavity. Flexion of the wrist makes ganglia more prominent; extension tends to obscure them. Ganglia may also develop on the hands, wrists, ankles, and feet. They can disappear spontaneously.
|
|
|
Abnormalities of the Feet: Acute Gouty Arthritis |
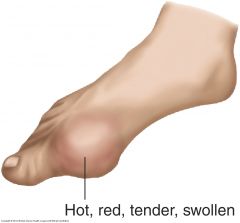
The metatarsophalangeal joint of the great toe is the initial site of attack in 50% of the episodes of acute gouty arthritis. It is characterized by a very painful and tender, hot, dusky red swelling that extends beyond the margin of the joint. It is easily mistaken for a cellulitis. The ankle, tarsal joints, and knee are also commonly involved. |
|
|
Abnormalities of the Feet: Flat Feet |
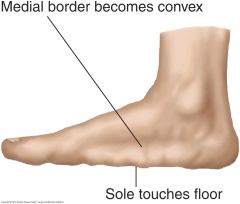
Signs of flat feet may be apparent only when the patient stands, or they may become permanent. The longitudinal arch flattens so that the sole approaches or touches the floor. The normal concavity on the medial side of the foot becomes convex. Tenderness may be present from the medial malleolus down along the medial-plantar surface of the foot. Swelling may develop anterior to the malleoli. “Flat foot” may be a normal variant or arise from posterior tibial tendon dysfunction, seen in obesity, diabetes, and prior foot injury. Inspect the shoes for excess wear on the inner sides of the soles and heels. |
|
|
Abnormalities of the Feet: Hallux Valgus |

Lateral deviation of the great toe and enlargement of the head of the first metatarsal on its medial side, forming a bursa or bunion. This bursa may become inflamed. Women are 10 times more likely to be affected than men. |
|
|
Abnormalities of the Feet: Morton's Neuroma |

Look for tenderness over the plantar surface between the third and fourth metatarsal heads, from perineural fibrosis of the common digital nerve due to repetitive nerve irritation (not a true neuroma). Check for pain radiating to the toes when you press on the plantar interspace and squeeze the metatarsals with your other hand. Symptoms include hyperesthesia, numbness, aching, and burning from the metatarsal heads into the third and fourth toes. |
|
|
Neer's Impingement |

Rotator Cuff Tear
Press scapula
Pain = positive test |
|
|
Hawkin's Impingement |
Rotator Cuff Tear
Flex shoulder, elbow at 90 degrees
Internal rotation of shoulder
Pain = positive test
|
|
|
Empty Can Test |
Rotator Cuff Tear
Elevate arms to 90 degrees
Internally rotate arms with thumbs down
Ask patient to resist downward pressure
Weakness = positive test
|
|
|
Drop Arm Test |
Rotator Cuff Tear
Abduct arm to 90 degrees
Ask patient to slowly lower arm
Patient can't hold arm up or control lowering = positive test |
|
|
Finkelstein's Test |

de Quervain's tenosynovitis
Patient grasps thumb against palm and moves wrist down
Pain = positive test |
|
|
Tinel's Sign |

Median Nerve Compression; Carpal Tunnel Syndrome
Tap lightly over median nerve in the carpal tunnel
Aching & numbness in the median nerve distribution = positive test |
|
|
Phalen's Sign |
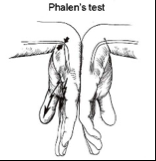
Median Nerve Compression; Carpal Tunnel Syndrome
Patient holds wrists in flexion with backs of hands together for 60 seconds
Numbness and tingling in the median nerve distribution = positive test |
|
|
Balloon Sign Bulge Sign |

Balloon sign = Major Effusion Bulge Sign = Minor Effusion
|
|
|
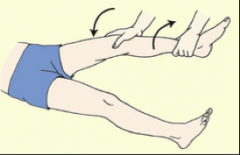
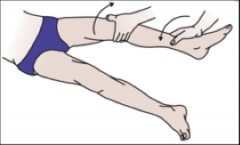
McMurray Test |
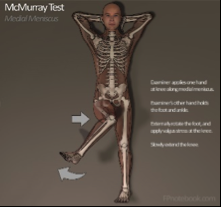
Meniscus Tear; Position on meniscus depends on stress applied
Grasp heel and flex knee Externally rotate heel Apply valgus stress to the knee Slowly extend lower leg in external rotation
A click or pop along medial joint = positive test |
|
|
Apley's Test |

Meniscus Tear
Patient in prone position Flex knee and push down on the foot to "grind" knee
Pain = positive test |
|
|
Abduction (valgus) stress test |
MCL tear
Slightly flex knee Push medially on knee and pull laterally on ankle Applies valgus stress and opens lateral medial side
Pain or a gap in the medial joint line = positive test |
|
|
Adduction (varus) Stress Test |
LCL tear
Slightly flex knee Push medially on knee and laterally on ankle Applies valgus stress on opens medial side
Pain or gap in the medial joint line = positive test |
|
|
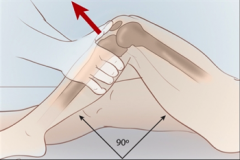
Anterior Drawer Test |
ACL tear
Flex hips and Flex knees to 90 degrees with feet flat Cup hands around knee with thumbs on medial and lateral joint lines Draw tibia forward and observe sliding forward
Forward jerk showing contours of upper tibia = positive test |
|
|
Lachman Test |
ACL Tear
Flex and externally rotate knee 15 degrees Grasp distal femur on lateral side and proximal tibia on medial side Pull tibia forward and push femur back
Significant forward excursion = positive test |
|
|
Posterior Drawer Test |

PCL Tear
Flex hips and flex knees to 90 degrees with feet flat on table Cup hands around knee with thumbs on medial and lateral joint lines Push tibia posteriorly and observe any sliding backward
Proximal tibia falls back = positive test |
|
|
Straight Leg Raise |
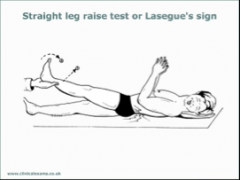
Radiculopathy
Determine whether a patient with low back pain has an underlying herniated disk
Sciatic pain = positive test |
|
|
Apprehension - Patella |

Subluxation and/or Dislocation
Try to push patella to each side
Pain and/or significant movement = positive test |