![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
158 Cards in this Set
- Front
- Back
|
What does Sternheimer-Malbin stain contain? |
Crystal-violet
Safranin |
|
|
What are the most common supravital stain? |
Sternheimer-Malbin and toluidine blue |
|
|
When can Sternheimer-Malbin stain not be used? |
Strongly alkaline urines, causes the stain to precipitate |
|
|
How does acetic acid help in microscopic examination of the urine? |
Lyses RBCs Makes nuclear pattern more prominent (WBCs & epithelial cells) |
|
|
What does Sudan III & Oil Red O help to ID? |
neutral fat or triglyceride |
|
|
Will Sudan III & Oil Red O stain cholesterol, and why? |
No cholesterol is not neutral |
|
|
What does the Prussian Blue Reaction help to ID? |
Visualizationof hemosiderin, free floating or in epithelial cells andcasts, |
|
|
What does Hansel Stain help to ID? |
Eosinophils |
|
|
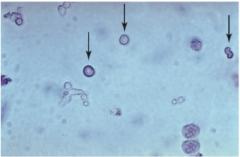
RBC -from top (disk) -from side (hourglass) |
|
|
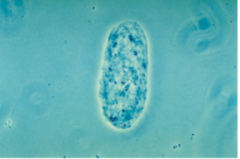
Dysmorphic and crenated red blood cells. A singleghost red blood cell is located at top of view. Phase contrast, 400×. |
|
|
What chemicals/stains help in the ID of RBCs? |
-acetic acid -toluidine blue stain - Sternheimer-Malbin stain |
|
|
What are the lookalikes for RBCs |
-WBC -Yeast -Monohydrate calcium oxalate crystals -small oildroplets -air bubbles |
|
|
What is the clinical sig for high RBCs in the urine? |
-Kidney or urinary tract disorders -Hypertension -Cancer -Trama -Strenuous exercise -Smoking -Anticoag drugs with induced toxic reactions |
|
|
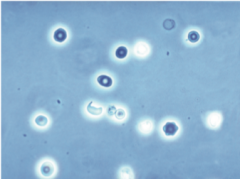
What is the most common granulocytic leukocytes present in urine? |
Neutrophils |
|
|
What happens when neutrophils are in the urine for to long? |
-their lobed nuclei fuse --They remember a mononuclear cell |
|
|
Several white blood cells with characteristic cyto-plasmic granules and lobed nuclei surrounding a squamous epithe-lial cell. Budding yeast cells are also present. |
|

|
WBCs with vacuoles (blebs) |
|
|
What are glitter cells, and how do they from? |
-Large swollen WBCs, brownian movement of therefractile cytoplasmic granules -Common in hypotonic urine |
|
|
What are myelin filaments and how are they distinguished? |
As WBCs degrade and the cell wall breaks down |
|
|
Are WBCs normal in the urine, why? |
Yes small numbers
They are motile and can enter the urinary tract |
|
|
Using WBCs how can one distinguish upper and lower UTIs? |
Lower- Increased WBCs, without cellular casts, protein present Upper- Cellular casts, coarsely granular casts, protein present |
|
|
What physical characteristic is associated with WBCs in the urine? |
-Cloudiness -Large gray-white sediment material -Worse infection = foul smell |
|
|
What WBCs has no leukocyte esterase? |
Lymphocytes |
|
|
What are the lookalikes for WBCs? |
-Renal tubular epithelial cells -RBCs |
|
|
What chemicals/stains help to ID WBCs? |
-acetic acid -toluidine blue stain -Sternheimer-Malbin stain |
|
|
What is the clinical sig of increased WBCs? |
-All renal diseases -Inflammatory conditions - |
|
|
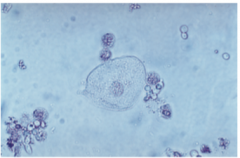
What do squamous epithelial cells look like and what are the clinical significances? |
-Large thin cells with flagstone boarders -Large amount of cytoplasm --Poor collection technique (not clean catch) |
|
|
What do transitional epithelial cells look like and what are the clinical significances? |
-Shape carries with site -Moderate amount go cytoplasm -"Firm" boarder appearance --Infection of inflammation of ureters, renal peeves, or male urethra -Can occur after cauterization or cystoscopy |
|
|
What do renal collecting duct (small and large) epithelial cells look like and what are the clinical significances? |
-Scant cytoplasm for both -Small duct - polygonal or cuboidal cells, with flat edges --Shock, sepsis -Large duct- Columnar --Trauma |
|
|
What do renal collecting duct (distal & proximal) epithelial cells look like and what are the clinical significances? |
-Distal- oval to round -Proximal- Large oblong with indistinct cell membrane. Larger than distal tubulars cells --BOTH -Toxic events (heavy metals etc), poisons, drugs |
|
|
Squamous epithelial cells: |
|

|
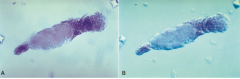
Both are epithelial cells A, Brightfield, Sedi-Stain, 200×. B, Phase contrast,200×. |
|
|
What are the most common epithelialcells in the urine? |
Squamous Epithelial Cells |
|

|
Two transitional (urothelial) epithelial cells. A, Phase contrast, 400×. B, Interference contrast, 400×. |
|
|
Four transitional (urothelial) epithelial cells. Phasecontrast, 400×. |
|
|
Convoluted tubular epithelial cells |
|

|
Renal collecting duct epithelial cells |
|
|
A, Fragment of renal collecting duct epithelial cells. Brightfield, 400×. B, Fragment of renal collecting duct epithelial cells in“spindle” form, indicative of regeneration of the tubular epithelium after injury. Interference contrast, 400×. |
|
|
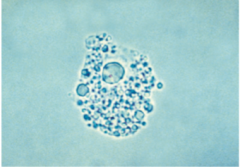
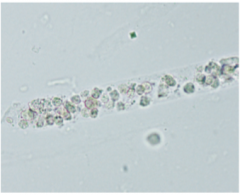
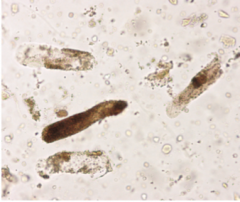
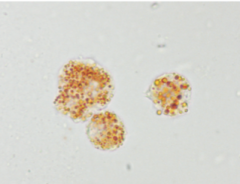
What are oval fat bodies? |
Renaltubular cells that are engorged with absorbed fat fromthe tubular lumen or are degenerating their own intracel-lular lipids |
|
|
Oval fat bodies |
|
|
What is the core matrix of casts made up of? |
uromodulin |
|
|
What is uromodulin? |
Makes up casts Glycoprotein |
|
|
What are casts cylindrical? |
They are formed within the tubules |
|
|
Three hyaline casts and several mucous threads.Phase contrast, 100×. |
|

|
Three hyaline casts. The cast with a tapered end isfrequently called a cylindroid. Phase contrast, 100×. |
|

|
Convoluted hyaline cast, initially formed in a tubuleand later compressed in a tubule of larger diameter. Phase contrast,200×. |
|

|
Two broad, granular to waxy casts. A, Brightfield, 100×. B, Interference contrast, 100×. |
|
|
What are cylindroid and how are they distinguished? |
Casts are well formed at one end but aretapered or have a tail at the other end |
|
|
Coarsely granular going to waxy cast. Brightfield,100×. |
|
|
One intact finely granular/waxy cast and two brokenpieces of a cast. Brightfield, 100×. |
|
|
What factors of the urine increase cast formation? |
-acid pH -increasedsolute concentration -urine stasis, and increased plasmaproteins (particularly albumin) |
|
|
What two exceptions would not indicate a disorder if a large amount of casts are observed? |
-Strenuous exercise (marathon running) -Diuretic therapies. |
|
|
What other things can affect formed elements in the urine? |
-physical exercise -emotional stress |
|
|
What are Hyaline casts? |
-Composed primarily of a homoge-neous uromodulin protein matrix |
|
|
What is the most common cast? |
Hyaline casts |
|
|
How can you ID Hyaline casts? |
They appear colorless in unstained urine sediment, withrounded ends and in various shapes and sizes -Phase contrast and interface contact microscopy |
|
|
3 hyaline casts and mucousthreads |
|
|
Hyaline cast. Note the appearance of the fibrillarprotein matrix and the presence of fine granulation. Phase contrast, |
|
|
When are waxy cast more common and what is another name for them? |
-Chronic renal failure or acute renal failure -Renal failure casts |
|
|
What are RBC casts? |
Casts with RBCs inside, can be packed with RBCs or sparse -Present as hyaline cast with RBCs inside |
|
|
Red blood cell cast. |
|
|
Cast, part granular and part waxy. Note the difference in cast diameter at one end compared with the other. This indicatesinitial cast formation in a narrow tubular lumen followed by stasis in a tubule with a wider lumen and further cast formation. A, Brightfield,Sedi-Stain, 200×. B, Interference contrast, 200×. |
|

|
Red blood cell cast. This cast is packed with intactred blood cells. A, Brightfield, 200×. B, Interference contrast, 400×. |
|
|
A pigmented granular cast or blood cast. The gran-ules and pigmentation originate from hemoglobin and red bloodcell degeneration. Brightfield, 200×. |
|
|
White blood cell cast |
|
|
What are WBC casts? |
WBC casts consist of leuko-cytes embedded in a hyaline cast matrix |
|
|
What do WBC casts indicate? |
Infection or inflammation |
|
|
Degeneration of cellular casts may cause them to be IDed as? |
Granular Casts |
|
|
Finely granular and coarsely granular casts. Pigmen-tation from hemoglobin degradation. |
|

|
A fatty cast. Note the globules and their character-istic refractility. Brightfield, 400×. |
|
|
What technique or chemicals can help to ID fatty casts? |
Sudan III or Oil Red O Polarized light |
|

|
Fatty cast. Note the high refractility of the fat globule inclusions in the matrix of the cast. A, Phase contrast, 400×. B, Polar-izing microscopy, 400×. The highly refractile fat globules apparent in A do not exhibit a Maltese cross pattern, identifying them as neutralfat; those with a Maltese cross pattern are cholesterol. |
|
|
Cast with sulfamethoxazole crystal inclusions.Brightfield, 200×. |
|
|
What kinds of injury are associated with fatty casts? |
Crush injury |
|
|
Define pigment cast? |
usually of ahyaline matrix with distinct coloration, are characterizedby incorporation of the pigment within the casts |
|
|
What is a key identifier for hyaline casts? |
Mucous threads |
|
|
What is a lookalike for waxy casts? |
Various fibers -Cotton, diaper |
|
|
What is a lookalike for casts? |
Crystals such as amorphous urates and phosphatescan aggregate together or along a mucous thread tosimulate a cast. |
|
|
What formed elements increase as urine cools to room temp or in a refrigerator? |
Crystals |
|
|
Regardless of the crystal type, crystal formation withinthe nephrons can cause? |
tubular damage |
|
|
What 3 factors influence crystal formation? |
-Concentration of solute in urine -Urine pH -Flow of urine through tubules |
|
|
Clinically significant crystal are more typical in what type of urine? |
Acidic |
|
|
Amorphous urate are more common in what pH range? |
5.7-7.0 |
|
|
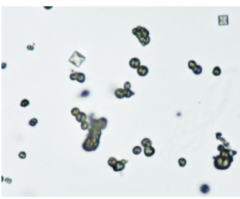
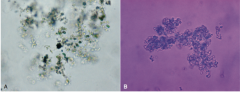
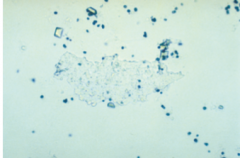
Describe the appearance of amorphous urate crystals? |
Small Yellow-brown -apparence like sand |
|
|
Are amorphous urate crystals polarizing? |
Yes |
|
|
Amorphous urates |
|
|
What tests are useful for the ID for Amorphous urates? |
-Solubilized in alkaline conditions -Will dissolve when heated (~60C) |
|
|
Do amorphous urates have any clinical sig? |
No |
|
|
Describe acid urates and and what chemicals do they contain? |
sodium, potas-sium, and ammonium salts Yellow-brown balls or spheres |
|
|
What pH are acid urates common in? |
Neutral to acidic |
|
|
What are acid urates misidentified as? |
leucine crystals |
|
|
How can acid urates be IDed? |
-Dissolve at ~60C -Can be converted to uric acid crystals with glacial acetic acid |
|
|
Do acid urates and clinical significance? |
No |
|
|
Acid urate crystals. Brightfield, 200×. |
|
|
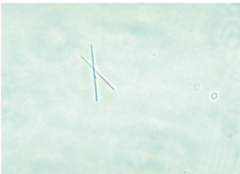
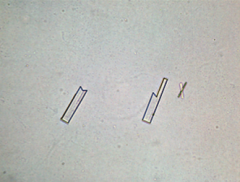
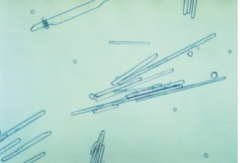
How are Monosodium Urate crystals distinct from uric acid salt? |
monosodium appear colorless to light yellow-low slender, pencil-like prisms. |
|
|
Monosodium urate crystals. Brightfield, 200×. |
|
|
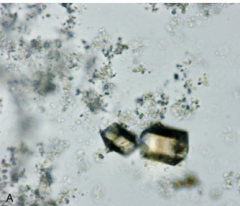
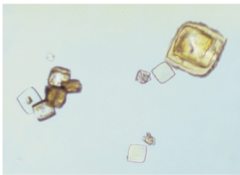
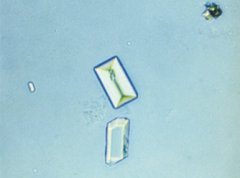
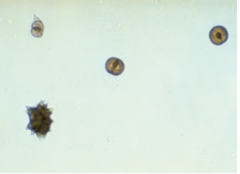
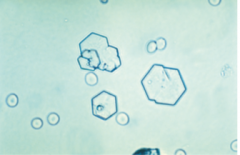
What is the common shape of uric acid crystals? |
rhombic or diamond shape, cubes, barrels, or banks in clusters. |
|

|
Uric acid crystals (diamond-shaped) and a fewcalcium oxalate crystals. Note the darker coloration as the crystalslayer and thicken. Brightfield, 200×. |
|
|
Uric acid crystals. Single and cluster forms. Bright-field, 200×. |
|
|
Uric acid crystals. Less common barrel forms. Bright-field, 200×. |
|
|
Uric acid crystals. Barrel form. Brightfield, 200×. |
|
|
Uric acid crystals. These crystals can layer or lami-nate on top of one another. Brightfield, 100×. |
|
|
What pH can uric acid crystals survive at? |
Less than 5.7 |
|
|
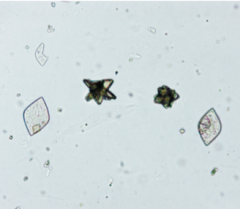
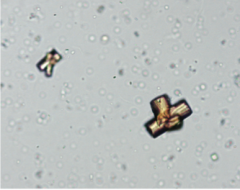
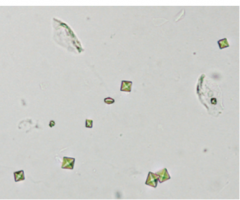
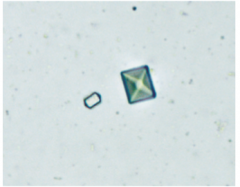
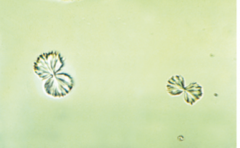
What shape are calcium oxalate? |
octahedral or pyramidform |
|
|
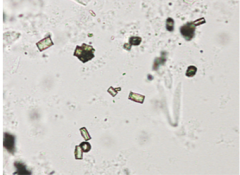
Calcium oxalate crystals. Octahedral (envelope)form of dihydrate crystals. Brightfield, 200×. |
|
|
Calcium oxalate crystals. An unusual barrel form anda typical dehydrate form. Brightfield, 400×. |
|
|
What pH does calcium oxalate crystals from? |
Any pH |
|
|
What foods aid in the formation of oxalate crystals? |
-Ascorbic acid -Oxalate precursor -Oxalic acid (cocoa, tea, coffee, and chocolate.) |
|
|
Increase number of calcium oxalate crystals are often involved with the ingestion of what? |
antifreeze ( ethylene glycol) |
|
|
What pH are Amorphous phosphates found in? |
Alkaline and neutral |
|
|
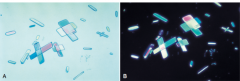
Amorphous phosphates. Note the lack of birefringence under polarizing microscopy. A, Brightfield microscopy, 400×. B, Polarizing microscopy with first-order red compensator, 400×. |
|
|
Triple phosphate crystals. Typical “coffin lid” form.Brightfield, 100×. |
|
|
Calcium phosphate crystals. Prisms are arrangedsingly and in rosette forms. Brightfield, 100×. |
|
|
What are amorphous phosphates soluble in? |
Acid and will NOT dissolve when heated |
|
|
Triple Phosphate are in what pH? |
Neutral |
|
|
Calcium phosphate crystals. Uncommon slenderneedles arranged in bundles or sheaves. Other crystals present inbackground include ammonium biurate, calcium carbonate, and asingle calcium oxalate. Brightfield, 400×. |
|
|
Calcium phosphate sheet or plate. Brightfield, 100×. |
|
|
Magnesium phosphate crystals. Brightfield, 400×. |
|
|
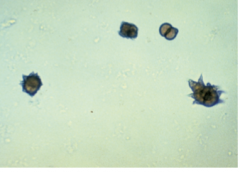
Ammonium biurate crystals. Spheres and a “thornyapple” form. Brightfield, 200×. |
|
|
Ammonium biurate crystals. Several “thorny apple”forms. Brightfield, 200×. |
|
|
Are magnesium phosphate birefringent ? |
weakly birefringentunder polarizing microscopy. |
|
|
How to Ammonium Biurate appear? |
Yellow-brown spheres or spiky |
|
|
Where are Ammonium Biurate most common? |
In prolonged storage specimens |
|
|
What is the significance of Ammonium Biurate? |
Dehydration |
|
|
How can Ammonium Biurate be IDed? |
-Strongly birefringent -Dissolve in acetic acid -Dissolve when heated to 60C |
|
|
How can you distinguish ammonium biurate and sulfonamide crystals? |
Basis of urine pH, sulfonamide confirmatory test, and the solubility characteristics of the crystals |
|

|
Bilirubin crystal. Brightfield, 400×. |
|

|
Calcium carbonate. A, Numerous single crystals. Brightfield, 400×. B, Aggregate of calcium carbonate crystals. Brightfield,400×. |
|
|
Calcium Carbonate ID |
-Tiny colorless granular - strongly birefringent 0Alkaline urine |
|
|
When do bilirubin crystals appear more? |
Refrigeration Acidic urine will dissolve in alkaline |
|
|
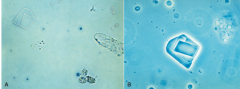
Cystine ID? |
colorless, hexagonal plates Acidic urine Dissolve in alkali or hydrochloric acid (<2pH) |
|
|
What disease are cystine associated with? |
congenital cystinosis or cystinuria |
|
|
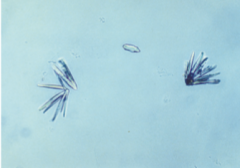
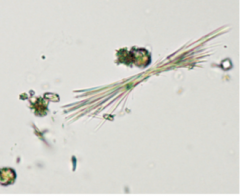
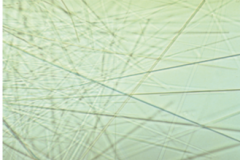
Tyrosine and Leucine ID? |
-Delicate needed colorless or yellow -Aggregate often -Acidic urine -Need refrigeration to be forced out of solution |
|
|
Cystine crystals. Brightfield, 400×. |
|
|
Tyrosine crystals. Brightfield, 400×. |
|
|
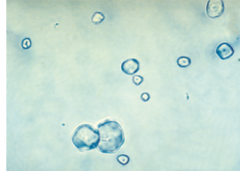
View of urine sediment with a cholesterol crystal, free-floating fat, and oval fat bodies. Brightfield, 200×. B, Cholesterolcrystal. Phase contrast, 400×. |
|
|
What disorder are Tyrosine and Leucine associated with? |
rare inherited metabolic disorders |
|
|
Cholesterol ID? |
-Clear, flat rectangular plated, with notched corners |
|
|
Diseases with cholesterol crystals? |
ephroticsyndrome and in conditions resulting in chyluria: therupture of lymphatic vessels into the renal tubules as aresult of tumors, filariasis, and so on. |
|
|
Ampicillin crystals. Brightfieqld 400X |
|

|
Indinavir sulfate crystals. A, Brightfield, 200×.B, Polarizing microscopy with first-order red compensator, 200×. |
|
|
Sulfamethoxazole (Bactrim) crystals. Brightfield,400×. |
|
|
Radiographic contrast medium following retrogradeadministration; meglumine diatrizoate (Renografin). The crystalsappear in needle forms. Brightfield, 100×. |
|
|
Sulfadiazine crystals. Brightfield, 400×. (CourtesyPatrick C. Ward.) |
|
|
Intravenous radiographic contrast medium. A, Interference contrast microscopy, 100×. B, Polarizing microscopy, 100×. |
|
|
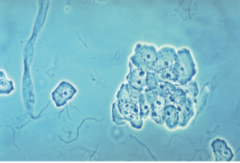
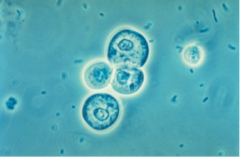
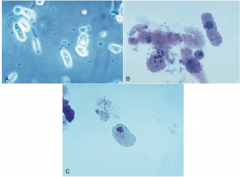
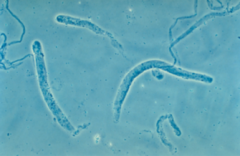
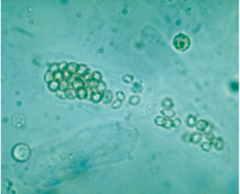
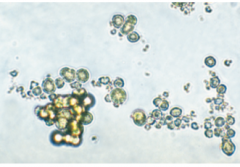
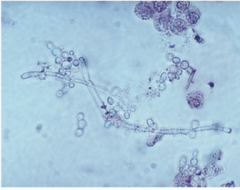
Budding yeast and pseudohyphae. Leukocytes arealso present singly and as a clump. Brightfield, Sedi-Stain, 400×. |
|

|
Pseudohyphae development by yeast. A, Interfer-ence contrast, 400×. B, Brightfield, 400×. |
|
|
Leukocytes with intracellular yeast. Interference con-trast, 400×. |
|
|
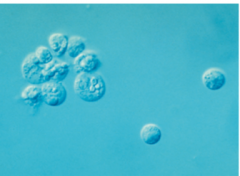
How are yeast IDed? |
-Will not dissolve in acid -Don't stain with supra vital stains - KOH preparation |
|

|
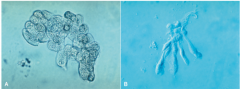
A trichomonad in urine sediment. Because of theirrapid flitting motion, only one of the flagella is visible in this view(arrow). Mucus, white blood cells, and other trichomonads arepresent but are not in focus at this focal plane. Phase contrast,400×. |
|

|
The slightly larger squamous epithelial cell with indistinct, shaggy cytoplasmic edges is a clue cell. The cell with well-definedcytoplasmic edges is a normal squamous epithelial cell. A, Brightfield, 200×. B, Phase contrast, 200×. |
|
|
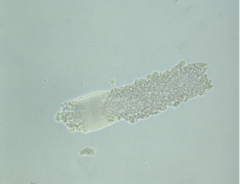
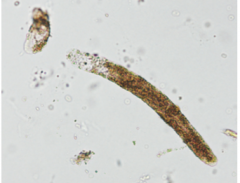
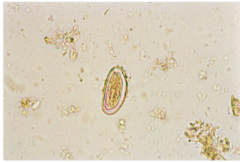
An Enterobius vermicularis egg, unstained wetmount. Note its oval shape with a slightly flattened side and thedeveloping larva within. |
|
|
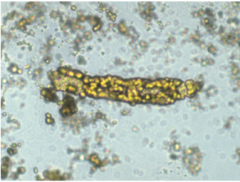
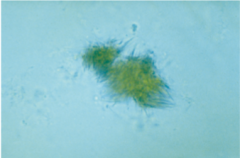
Three oval fat bodies stained with Sudan III stain.Note the characteristic orange-red staining of neutral fat globules.Brightfield, 400×. |
|

|
Mucus. A, Several mucous threads and two hyalinecasts. Phase contrast, 100×. B, A mass of mucus surrounding a fiber(contaminant). Brightfield, 400×. |
|
|
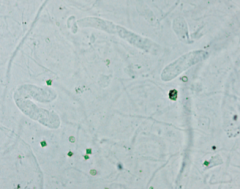
Starch granules. Brightfield, 400× |
|

|
Starch granules. A, Demonstration of a Maltesecross pattern using polarizing microscopy, 400×. B, Polarizingmicroscopy with first-order red compensator, 400×. |
|
|
How to ID starch granules? |
-Not perfectly round -Indented center -Maltese cross pattern (polarized), the edgesof the Maltese pattern are less define |
|
|
How does starch end up in samples? |
Gloves most likely |