Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
123 Cards in this Set
- Front
- Back
|
Describe the Gram negative bacteria in terms of
Cocci (2) Coccoid Rods (4) Oxidase + (2) Rods Lactose Fermenting (5) Rods Non Fermenting Lactose (4) |

|
|
|
Describ Gram Positive Rods in terms of
Catalase + Cocci (3) Catalase - (4) Rods (bacillia) (4) Branching Filaments (2) |

|
|
|
1. Name the THREE closed organ systems (3)
2. Infections associated with (2) 3. These systems normally (2) |
1. Bone & Joints
Vascular CNS 2. ↑Morbidity & ↑Mortality 3. Sterile & No normal biota |
|
|
Describe the
1. Blood-Brain-Barrier (2) 2. Blood-CSF Barrier (2) 3. Brain-CSF Barrier |
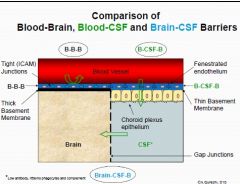
1. Tight Junctions & Thick Basement Membrane
2. Fenestrated Endothelium & Thin Basement Membrane 3. Gap Junctions |
|
|
Define
1. Empyema 2. Abscess 3. Meningitis 4. Encephalitis 5. Myelitis 6. Meningoencephalitis |
1 Epidural/Subdural abscess
2. Localised pockets of infection 3. Infection of CNS coverings 4. Infection of Brain parenchyma 5. Infection of Spinal Cord 6. ALL 3 |
|
|
CSF
1. Lacks 2. Delay in therapy |
1. Immune Response
2. ↑ Morbidity & ↑ Mortality |
|
|
Most important Epidemiological concern
|
1. AGE
|
|
|
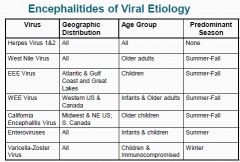
Describe the GEOGRAPHIC, AGE & SEASONALITY for the following
1. Herpes Virus 1 & 2 2. West Nile Virus 3. EEE Virus 4. WEE Virus 5. California Encephalitis Virus 6. Enetrovirus 7. Varciella-Zoster Virus |
|
|
|
Most Common Site for Entry, Replication & Spread
|
1. HEMATOGENOUS
|
|
|
Most Common Site for Entry,
Replication & Spread Hematogenous 1. Respiratory 2. Insect Bite 3. Transplacental 4. Neural (2) Direct Innoculation 5. Via trauma (wound) 6. Direct Innoculation in Immunodefecient (3) |
1. Meningoccoci
2. West Nile Virus 3. Rubella 4. Rabies & HHV 1-3 5. Staph aureus 6. Nocardia, Aspergillus & Candida |
|
|
What is the source of infection for the following Bacteria
1. Corynebacterium 2. Enterobacteria 3. Fusibaterium 4. Peptococcus 5. Pseudomonas 6. Streptococci 7. Strep Viridans 8. Staph aureus |
1. Lungs
2. Urinary Tract 3. Lungs 4. Lungs 5. Urinary Tract 6. Lungs 7. Heart 8. Wounds & Heart |
|
|
CNS Syndromes name the general cause of
1. Acute Meningitis (2) 2. Chronic Meningitis (2) 3. Acute Brain Abscess 4. Chronic Brain Abscess (3) 5. Encephalitis 6. Myelitis |
1. Viral & Bacterial
2. Fungal & Tubercle bacilli 3. Poly microbial 4. Tubercle bacilli, fungi & protozoa 5. Viral 6. Viral |
|
|
Classic Symptoms Seen w/ Meningitis, specifically the inflammation (4)
|
More HNNP
Headache Nuchal Rigidity Nausea & Vomiting Photophobia |
|
|
FIVE indicators for Meningism
|
1. CANNOT Chin to Chest
2. CANNOT Knees to Nose 3. Tripod sign 4. Kerning sign (hamstring spasm) 5. Brudzinski's (Legs retracted, when neck lifted) |
|
|
How do you diagnose Meningitis
1. Site 2. 3 ways |
CSF
1. Chemical & Cultural Analysis 2. Culture 3. PCR |
|
|
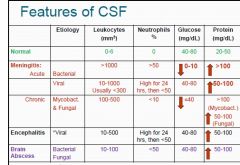
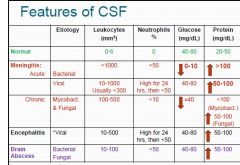
Describe the Leukocytes, Neutrophils, Glucose & Protein seen
1. Normal 2. Acute Bacterial Meningitis 3. Acute Viral Meningitis 4. Chronic Mycobacterial & Fungal 5. Encephalitis 6. Brain Abscess |
|
|
|
Diangnostic CNS imaging, describe what is seen with
1. Japanese B virus 2. Nipah Virus 3. Human Herpes virus -1 |
1. Grey Matter involvement
2. MULTIPLE, SMALL, WHITE matter lesions 3. Hemmorhages w/ encephalitis |
|
|
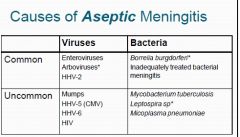
ASEPTIC (acute) Meningitis, name
1. Common viruses (3) 2. Uncommon Viruses (4) 3. Common Bacteria (2) 4. Uncommon Bacteria (3) |
|
|
|
Vrial Infections of CNS
1. Most common pathway 2. Via Olfactory Nerve (2) 3. Intra-axonal neuronal route |
1. Hematogenous
2. HHV 1 & 2 3. Rabies |
|
|
1. Name THREE Picornaviruses involved in Vrial Meningitis
2. Gram stain 3. CSF findings |
1. Echovirus, Coxsackie & Poliovirus
2. NO bacteria 3. refer to table |
|
|
Picornaviridae
1. SES 2. Nucleic ACid 3. Class 4. Resistant to (3) |
1. Small, Naked, Icosahedral
2.(+)ssRNA 3.Class IVa 4. pH 3-9, detergents & heat |
|
|
Pneumonic for Picornaviruses
|
PERCH on a PIC
Polio Echo Rhino (not entero) Coxsackie HAV |
|
|
Which Picornoviruse can causes
1. Aseptic Meningitis Enteroviruses, 2. ALL except 3. Spread via 4. Most are 5. Responsible for 90% of (MOST COMMON) |
1. Polio, Echo & Coxsackie
2. Rhino 3. Fecal-Oral 4. CYTOLYTIC (permenant loss) 5. Viral meningitis (MOST COMMON) |
|
|
Name FIVE dieases caused by ENTEROVIRUS
|
Hand-Foot & Mouth disease
Herpangina Myocarditis Pleurodynia Acute Hemorrhagic Conjunctivitis |
|
|
Enterovirus
1. MOST susceptible 2. Resevior 3. Symptoms 4. TEMPERATE seasonality (transmission) 5. TROPICAL seasonality (transmission) |
1. INFANTS & CHILDREN
2. Humans 3. Asymptomatic 4. Summer to Fall (water) 5. Year round (fecal-oral) |
|
|
Poliovirus
1. Transmission 2. Direct contact via (2) 3. Initial Symptoms (3) 4. Followed by (KEY) 5. Clinical Syndrome 6. D/T 7. Dangerous because |
1. Fecal-Oral
2. Infected Stool & Throat Secretions 3. Headache, Fever & Nuchal Rigidity 4. WEAKNESS in ONE or MORE extremeties 5. Acute Flaccid Paralysis 6. Infection of ANTERIOR HORN of GREY matter 7. Cytolytic (permenant damage) |
|
|
Poliovirus PATHOGENESIS
SEVEN STEPS 1. Site of Primary Replication KEY |
Infects Enterocyte → Transverse Basement Membrane→GALT (peyer's patches)→Primary Replication→Viremie Peripheral Tissue→Enters Periheral Neurons→Retrograde Axonal Transport → CNS
|
|
|
Poliovirus
1. Outcomes (4) |
1. Inapperent infections (95%) (virus in RES)
2. Abortive Polio (flu like) 3. Polio encephalitis -RARE 4. Aseptic meningitis (non-paralytic polio) |
|
|
Poliovirus vs, Other Enteroviral meningits.
Differentiate |
1. Serology/isolation of virus
|
|
|
Paralytic Polio
1. Occurs in % 2. Restricted d/t Barriers (4) 3. If breached, spinal (3) 4. Bulbar (4) |
1. <2%
2. Limited replication in Neurons, insufficient Retrograde Transport, IFNα/β 3. Flaccid paralysis, lysis of Anterio Horn Cells 4. CN IX, X, medullay/respiratory centers, DEATH |
|
|
Polio, name the key traits
1.LIVE Oral (4) 2. Inactivated (3) |
1. SABIN -stable at room temp, MgCl2 & produces secretory antibodies (sIgA in gut)
2. SALK-injected IM, NO ABs produced |
|
|
Septic vs. Aseptic
|
1. Septic- BACTERIAL
2. Aseptic-VIRAL |
|
|
Septic Meningitis more
|
1. Severe, HIGH mortality & Age dependent
|
|
|
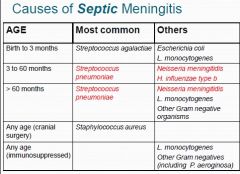
Name the causes of Septic Meningitis, Most common & other
1. Neonate (1 & 3) 2. Children < 5years (1 & 2) 3. >60 months (1 & 3) 4. Any age d/t cranial surgery 5. Any age d/t immunosupressed (2) |
|
|
|
Again, describe the levels of leukocytes, Neutrophils, Glucose & Protein for
1. Normal 2. Acute Bacterial Meningitis 3. Acute Viral Meningitis 4. Chronic Mycobacteria & Fungal 5. Encephalitis 6. Brain Abscess |
|
|
|
Pneumone for the folliwng Gram Positive Cocci
1. Staph 2. Strep (2) |
1. On the office's STAPH retreat, there was NO StRES
No Ovobiocin- Saprophyticus is Resistant; Epidermidis is Sensitive. 2. OVeRPaS Optochin-Viridans is Resistant; Pneumoniae is Sensitive 3. B-BRAS Bacitracin-group B strep are Resistant; group A strep are Sensitive |
|
|
Bacterial Infection of CNS How is most likely to be infected by
1. Hematogenous 2. Middle Ear 3. Direct induction (rare) |
1. MOST COMMON
2. Children, 3. Adults via Trauma & Surgery |
|
|
More than 75% of Bacterial Meningitis is caused by what bacteria
|
Strep. pneumoniae, N. meningitidis, & H. influenzae
|
|
|
For the 3 MOST common causes of Bacterial infection, what is the
1. most improtant Virulence factor 2. Which have pili & endotoxin 3. Which have IgA proteases |
1. CAPSULE
2. Neisseria meningitidis & Haemophilus influenza 3. Strep pneumoniae, Neisseria meningitidis & Haemophilus influenza |
|
|
Neisseria meningitidis (1st Aid)
1. Ferment (2) 2. Key Virulence Factors (4) 3. Transmission (2) 4, Causes (3) |
1. Glucose & Maltose
2. Capsule, IgA protease, pilli & endotoxin 3. Respiratory & Oral 4. Meningitis, Meningococcemia & Waterhouse-friderchsen Syndrome |
|
|
N. meningitidis
1. Type of Bacteria (3) 2. Transmission 3. AGE 4. 50 % of Survivors 5. clinical Signs |
1. Gram negative, Maltose fermenting, Cocci
2. Respiratory 3. <5yrs 4. Neurological Deficits 5. Rash, Sepsis, Fever &Nuchal Rigidity |
|
|
N. Meningitidis diagnosis pneumonic
2. the cultures have |
Trust Neisseria to Look
Pleased eating Choclate belonging to Martin Thayer Tumbler Test- Rash Latex Agglutination PCR Chocolate Agar - Blood/CSf Modified Martin-Thayer -Nasoppahryngeal 2. 5-10% CO2 |
|
|
N. meningitdis DIAGNOSIS. Name WHAT is being tested
1. Tumbler Test 2. CSF tap 3. Choclate Agar (2) 4. Modified Martin-Thayer Agar 5. Latex Agglutination 6. PCR 5. Rapid techniques (2) |
1. Rash
2. Protein, Glucose & WBC count 3. Blood or CSF 4. Nasopharyngeal swab 5. Rapid techniques (2) |
|
|
1. Name the Vaccine for N. meningitidis
2. Composed of Groups (4) Most common? 3. Protection is (2) 4. Vaccination is not effective vs. 5. Does not protect vs. |
1. Trivalent
2. A, C, Y (most common) & W135 3. Group Specific & 3 years 4. Infants <2years old 5. Carriage of Organism |
|
|
0. ALL strep are (2)
1. What does Taxos A mean? 2. What bacteria is Taxos A resistant? (e.g) 3. Susceptible? (e.g) 4. What is Taxos P 5. Resistant? (e.g) 6. Susceptible? (e.g) |
0. Catalase -ve & Chains
1.Differentiates β Hemolytic Strep. based on BACITRACIN Resistance/ Susceptibile 2. Group B β Hemolytic Strep (S. agalactiae) 3. Group A β hemolytic Strep (pyogenes) 4. Differentiates α Hemolytic Strep based on OPTOCHIN Sensitivity/ Resistance 5. α Hemolytic Strep NON-Pneumoniae (Viridans) 6. α Hemolytic Strep. Pneumoniae |
|
|
Strep. agalactiae
1. Describe (6) |
1. Gram +ve, Cocci in Chains, Catalase -ve, β hemolytic & Taxos A resistant,
|
|
|
Group B Strep agalactiae
AGE 1. Most common 2. Also (2) |
1. Neonates Septic Mennigitis
2. Children & Adults |
|
|
Group B Strep agalactiae
1. Biota of 2. 60% of mortality in babies? IMPORTANT risk factor? 3. Neonate symptoms (4) 4. Children & Adult (2) |
1. 40% of Female Genitalia
2. Babies who develop meningitis in FIRST WEEK of life. (PREMATURE birth) 3. Lethargy, Fever, Sepsis & RESPIRATORY distress 4. PEUPERAL Fever @ DELIVERY & soft tissue infections |
|
|
Strep. pneumoniae
1. Describe characterestics (5) |
1. Gram +ve, Catalase -ve, lancet shapedCocci in Chanis, α Hemolytic & Taxos P sensitive
|
|
|
Strep. pneumoniae
1. Normal Biota 20% of? 75% of? 2. Most COMMON cause 3. AGE 4. Neurological Sequale seen in 5. Symptoms (2) 6. Elderly |
1.20% - Adults & 75% < Children
2. BACTERIAL meningitis 3. 5 Years old < Anyone 4. 50% 5. Sinusitis, Middle ear infection (direct innoculation) 6. May follow Pneumoniae |
|
|
Strep pneuomoniae
1. Role of Hydrogen Peroxide (3) 2. Pneumolysin (4) |
1. No catalase → Hydrogen Peroxide Accumulate → Enhance Apoptosis
2. Pneumolysin → Pore Forming Toxin → Neuro Toxin → Cellular Apoptosis |
|
|
Strep pneumonia
0. Transmission 1. Invasion NOT via 2. invasion via 3. PATHOGENESIS (5 steps) |
0. Respiratory Droplets
1. Hematogenous 2. NASOPHARYNX 3. Tetoic & Lipoteichoic Acid bind → GANGLIOSIDE on Neurons →OLFACTORY → RETROGRADE Transport → Brain |
|
|
H. influenzae
1. Describe (4) |
1. Grame -ve, Coccoid Rods (pleomorphic), fastidous (requires CO2) & Encapsulated
|
|
|
H. infeulnzae
1. Age 2. Agar (2) 3. Spread via (2) 4. Vs. other Bacterial Meningitis 5. Vaccine made for |
1. 4 MONTHS to 3 years
2. Chocolate Agar V-NAD+ & X -Hematin) & Blood Agar w/ S. aurues (growws on Streak) 3. BLOOD & RT 4. GRETEST Risk for PERMENANT neuroligical damage 5. type B capsular PS |
|
|
Name the Gram -ve RODS that
1. FERMENT Lactose FAST (3) 2. FERMENT Lactose SLOW (2) Do Not Ferment LACTOSE 3. Oxidase -ve (3) 4. Oxidase +ve |
1. Klebsiella, E.coli & Enterobacter
2. Citrobacter & Serratia 3. Shigella, Salmonella & Protues 4. PseudOmOnas |
|
|
E. coli K1
1. Describe (6)) 2. Neonate menengitis |
1. Gram -ve, Rod, Encapsulated, Fast Lactose fermenter, Facultative Anaerobe & Flagella
2. 2nd most common cause |
|
|
E. coli K1
0. KEY TEST 1. During pregnancy? Increase in mortality? 2. Spread via? |
0. Pink on MaConkey's Agar & Blue-Black colonies w/ Metalic Sheen on Eosin -Methylene Blue Agar
1. Increased Colonization & 8% mortality 2. Nasopharynx to meninges |
|
|
E. coli K1 SYMPTOMS w/ Meningitis
1. <1 month old (5) 2. 4-18 months old (3) 3. Older children & Adults (6) |
<1 month - VAILS
Vommiting, lack of APPETITE, Irritability, Lethargy, Seizures 4-18months- FFR FEVER, tense FRONTALES & nuchal RIGIDIDTY 3. CONFUSION & HEADACHE Lethargy Vommiting, Seizures (also in infants,) Fever (also in kids) |
|
|
E. coli K1 capsule significant in Meningitis d/t/
1. Cross 2. Protects from (2) |
1. Blood Brain Barrier
2. Vacule Maturation & Fusion w/ Lysososome |
|
|
Klebsiella pneumoniae
1. Describe (4) 2. Similar to |
1. Gram -ve, Rod, THICK capsule Fast Lactose fermenter, Facultative Anaerobe
2. E. coli K1 (cept Flagella) |
|
|
K. pneumonia
1. Age Symptoms & Time 2. Early onset (2) 3. Second to? 4. Late Onset (2) 5. Second to |
1. Neonates/Infants. COCKROACH infested areas
2. <3 days- Too LITTLE (leukopenia & neutropenia) 3. GBS 4. 8- 28 days - Too MUCH (leukocytosis & Neutrophilia) 5. Staph |
|
|
K. pneumoniae
1 Culture from (3) 2. Sputum colour 3. Symptoms (6) 4. Positve for |
1. Blood. CSF & Urine
2. Lethargy, Fever, POOR FEEDING, little CRY, SCLEREMA (shrunked waxy skin) & Rasin Color Sputum 4. C-Reactive Protein |
|
|
L. monocytogenes
1. Describe (5) 2. Produces what exotoxins (4) 3. Transmission |
1. Gram +ve, Rods, NON-spore forming, Aerobic,& Motile
2. Internalin A & B, Hemolysins (Listeriolysin O & 2 phospholypase Cs) & ActA 3. Fecal-ORal & Transplacental |
|
|
L. monocytogenes Meningitis. Describe Function of
1. Internalin A & B 2. Listeriolysin O 3. 2phospholypase C 4. ActA |
1. Cell ATTACHMENT moleuce, triggering entry
2. Helps escape phagosome (only translated in Vacuole) 3. Break the cell membrane 4. Resshuffles cell-membrane via ACTI |
|
|
L. monocytogenes
0. AGE 1. DIAGNOSIS (4) 2. Epi (3) 3. Resevoir (3) 4. KEY Clinical Vignette 5. Tranmission |
0. Neonates or Children/Adults
1. RODS in MACROPHAGES or NEUTROPHILS & CSF- looks like β Strep, but CATALASE + & TUMBLE 2. Delly, Dairy or Soil/Water/Decaying vegtationm 3.Hjuman intestine (2-12%) 4. SPONTANEOUS ABORTIONS 5. Delivery |
|
|
Treponema pallidum Meningitis
0. Lay man term 1. Describe 2. Is a |
0. Syphillus
1. Gram Negative, Spirochetes 2. STI |
|
|
T. pallidum
0. Age 1. initially 2. tertiary stage (3) 3. KEY charactersic 4. Part of Pathogenic Mechanism 5. Route |
0. Sexually Active
1. Big Pox 2. Neuorospyhillus after 10 years, no longer infections 3. GUMMAS (many tissues) 4. Delayed Hypersensitivity 5. Meninigovascular route |
|
|
T. pallidum
1. Diagnosis (4) 2. Symptoms |
1. Spinal fluid, Elevated WBC & Protein & VLDRL POSTIVE
2. FRANK PSYCHOSIS, GUMAS & SHUFFLING Gait (tabes dorsalis) bowed bones) |
|
|
L. interrogans
1. Describe (2) 2. Transmission (2) 3. Resevori 4. Found in 5. Sensitive to (3) 6. Likely patients (4) |
1. Gram -ve, Spirochete, LONG doubling time
2. Fecal-Oral 3. Animals 4. ALL bodies of water 5. Acid pH, Drying & Soap 6. Swere Workers, Miners, Veternarians & Meat Packers |
|
|
L. interrogans
1. Incubation 2. 1st Phase (3) 3. 2nd Phase (3) 4. WHEN does it enter CNS |
1. 5 days to 4 weeks
2. Bacterema, w/ infleunza like symptoms & fever 3. 3+ weeks, Headache w/ aseptic meningitis & HEMODYNAMIC collapse (sometimes) 4. 1st phase |
|
|
Boreilla burgdorferi
1. Pneumonic 2. describe (2) 3. Transmitted via |
BAKE a key LYME pie
Bell's Palsy Arthritis Kardiak Block Erythema Migrans 2. LARGE spirochetes, gram -ve 3. TICK BITE |
|
|
B. burgdorferi
1. Stage 1 (3) 2. Stage 2 (3) 3. Srage 3 (3) |
1. Eythema Chronicum Migrans, Meningeal Irrritation & Flue-like symptoms
2. Spirochetemia, Bell's Palsy & AV nodal block 3. FRANK encephallities, Chronic monoarthritis & Migratory poly arthritis |
|
|
B. burgdorferi
1. Diagnosis (2) |
1. Loose Irregular Spirals, Silver or IF Stain
2. Western Blot w/ ELISA |
|
|
Fungal Infections of CNS
1. Dessiminate? From? (2) 2. Infection created/ 3. Can cause 4. Early Vascular invasion causes 5. Secondary symptoms include (3) |
1. Hematogenously from Respiratory Infections
2. Multiple w/in brain 3. Abscesses 4. Meningoencephalitis 5. Secondary Thrombosis, Cerebral Infarction & Hemorrhages |
|
|
Which fungal infection has
1. Pseudohyphae 2. Yeat @ room temp 3. Name THREE other fungi that infect CNS |
1. Candida albicans
2. Aspergillus fumigatus 3. Histoplasma capsultatum, Cryptococcus neoformans & gatti |
|
|
Diagnosis
1. Candida (3) 2. Cryptococcua (2) 3. Histoplasma 4. Aspergillus (2) |
1. froms Granulomatus rxn, yeast form, w/ PSEUDOHYPAHE on SILVER STAIN
2. India Ink & MUCICARMINE showing capsules w/ halo 3. CT scan 4. Acute Septate branching Hpyhae on SILVEr stain |
|
|
Cryptococcus neoformans
1. Affects 2. CLINICAL vignette 3. Most improtant fungal infection in AIDS patients, afer 4.Tranmission 5. Disease of 6. Key characterestic |
1. IMMUNOCOMPROMISED
2. PIGEON excretea 3. Pneumocystis jirovecii 4. Respiratory 5. Respartory tract 6. HUGE CAPSULE |
|
|
Cryptococcus gattii
1. Effects 2. Associated w/ (3) 3. Kills who (2) Time frame? 4. Key symptom 5. 75% disease 6. 10% disease |
1. IMMUNOCOMPETENT
2. EUCALYPTUS TREeS, seeds, soil or foliage 3. Children & Elders w/in 1 week 4. Blindness via OPTIC neuropathy 5. Pulmonary 6. Meningitis |
|
|
Protozoan Meningitits
1. 4 Protozoa 2. Diagnosis 3. Diagnosis for Sappina diploida |
1. Naegra floweri, Acontha moeba, Balamanthia manidillus & Sappina diploida
2. CSF microscopy 3. Brain Biopdy w/ PCR |
|
|
Encephallitis
1. Normally 2. EXCEPT (23) 3. Fungal (2) 4. Parasitic (3) |
1. VIRAL
2. Leigonella pneumophillia, Borelia burgdorferi & Treponema pallidum 3. C. neoformans & gattii 4. Plasmodium falciparum & Trypanosomes |
|
|
Encephalitis
1. More sever than 2. Symptoms (5) |
1. Meningitis
2. Headache, Fever, Altered consciousness, Seizures, & Behavioral/Speech disurbanes |
|
|
Togaviridae
1. Envelope 2. Structure 3. Class 4. Capsid 5. Arboviruses (2) |
1. Envelope
2. +ss Linear 3. Class IVb (buds at plasma membrane) 4. Icosahedral 5. EEE & WEE |
|
|
Flaviviradae
1. Envelope 2. Structure 3. Class 4. Capsid 5. Arboviruses (5) |
1. Envelope
2. (+) ss Linear 3. Class IVa (buds @ cytoplasmic membrane & exocytosis) 4. Icoashedral 5. Yellow Fever, Dengue, St. Louis Encephalitis, Japenese B encephalitis Virus & West Nile Virus |
|
|
Bunyaviridae
1. Envelope 2. Structure 3. Class 4. Capsid 5. Arboviruses (4) |
1. Envelope
2. (-)ss circular 3 segments 3 Class Vb (smallest segment half '+' & half 'v') 4. Helical 5. California Encephalitis, Sandfly/Rift Valley Fever, Crimean-Congo Hemorrhagic Fever & La Crosse Vrius |
|
|
Rhabdoviridae
Togaviridae 1. Envelope 2. Structure 3. Class 4. Capsid 5. Medical Improtance |
1. Envelope
2. (-) ss Linear RNA 3. Class Va 4. HELICAL 5. Rabies |
|
|
Polyomavirus
1. Envelope 2. Structure 3. Class 4.Medical Improtance |
1. Naked
2. (-) ds ciruclar DNA 3. Class I 4. JC virus |
|
|
Parmyxoviridae
1. Envelope 2. Structure 3. Class 4. Capsid 5. Medical Improtance (4) |
1. Envelope
2. (-) ss linear Nonsegmented RNA 3. Class Va 4. Helical 5. PaRaMyxo Parainfluenza, barking PIG syndrome (nipah virus) RSV, Rubeola (Measles) & Mumps |
|
|
Venezualen EE
1. Family 2. Srpead via (2) 3. Inital Symptoms 4. D/t 5. Raprdid progression d/t 6. Symptoms (3) 7 50% time (2). 8. Death |
1. Togaviridae
2. Culex & Aedes mosquitoes 3. Prodrome 4. Viral replication 5. Spread via microvasculatur brain (axon-dendrites) 6. Nuchal rigidity, CONFUSION, SOMNOLENCE, 7. Sezures & COMA 8. NO DEATHS in humans (80% horses) |
|
|
Eastern EE
0. Family 1. Zoonotic (2) 2. Mortality rate 3. Symptoms similar to 4. Epi |
0. Toga
1. Aedes & Culiesta 2. HIGHEST 3. VEE 4. North Americal |
|
|
Western EE
1. Family 2. Zoonotic (2) 3. Epi 4. Fatality 5. Death in 6. 30% of CNS sequale |
1. Toga
2. Culex & Culiseta 3. Rural USA 4. 3-4% 5. 1-2 days 6. Children |
|
|
Togaviradea & Flaviviradea
Match the Virus w/ the: 1. Culex (4) 2. Aedes (3) 3. Culiseta (2) |
1. VE, WE, SL & JB
2. VE, EE & WNV 3. WE & EE |
|
|
Equine Encephalitides
1. Involvment 2. Damage mediated byvia (2) 3. Causing (2) 4. Vascular inflammation w/ |
1. Defuse CNS
2. Neutrophils & Macrophages 3. FOCAL NECROSIS & SPORRy demyelination 4. ENDOTHELIAL proliferation & small vessel thrombosis |
|
|
EEE vs. WEE
EEE 1. Mosquito (2) 2. Entering Brain Parenchyma 3. Effects (2) WEE 4. Mosquito 5. Brian via 6. Cell death by? Effects (2) |
1. Aedes & Culiseta
2. Large # of ACTIVE virus 3. PERIKARYON & DENDRITES 4. Culex & Culiseta 5. Large # of IMMMUNOLOGICALLY active CELLs 6. Apoptosis in GLIAL & INFLAMMATORY cells |
|
|
TOGAviridae vs. Flaviviradea
TOGA 1. Class 2. Replication 3. Virus buds & leaves Flavi 4. Class 5. Replication 6 Buds & leaves |
1. Class IVb
2. Early & Late Proteins 3. Buds @ Plasma membrane 4. Class IVa 5. Polyprotein, which is cleaved into many 6. Buds @ Cytoplasmic vessicle & Exits via Excoytosis |
|
|
St. Louis Viral Encephalitis
1. Transmitted 2. epi 3. Overt infection d/u 4. ENTERS brain via (2) |
1. Culex
2. Argintina 3. Replication at neural sites, Viremia & Age 4. BBB (astrocyte comples) & Choroid Plexu (fenestrated endothelium) |
|
|
St. Louis Encephalitis
1. 1-20% mortality in 2. Non-specific symptoms (2) 3. 20% develop what Sequelae 4. MOST COMMON encephalitis with (2) |
1. ELDERLY
2. Mailaise & FEVER 3. Irritability, Memory Loss, Movement Disorders & Motor Deficitis 4. SEIZURES & COMA |
|
|
Japanese B Encephalitis virus
1. Mosquito 2. Epi 3. Incubation 4. Viral prodrome 5. KEY symptoms 6. Hight death rate Porportional to |
1. Culex
2. Rural Asia 3. 4-14days 4. 2nd weel 5. TREMOR 6. Low CSF/IgM ration |
|
|
West Nile Encephalitis Virus
1. Mosquito 2.Resevoir 3. 3-15% 4. Prodrome w/ (2) 5. Symptoms (6) 6. Possible comligation |
1. Aedes
2. Wild birds 3. FATAL 4. MACULOPAPULAR rash on TRUNK & EXTREMETIES 5. HIGH fever, Headach, Nuchal rigidity, Stupor, TREMOR & SEZURE 6. 2-3 Weeks after infection, Guillene-Barre Syndrome |
|
|
Lysavirus
0. layman Name 1. Family 2. Five proteins? 3. Fxn of Most Improtant |
0. Rabies
1. Rhabdoviridae 2. G (most improtant) L, M, N & P 3. Attaches to Ach receptors @ NMJ |
|
|
O antigen
K antigen H antigen |
O -Somatic (cell wall)
K- Capsule H - Flagella |
|
|
Rabies
1. Enters via 2. Tropism (2) 3. Spreads from Brain to (3) 4. Virus shed in |
1. Endocytosis
2. Nerve & Salvary Glands (axons to CNS) 3. Salvary Glands, Kidney & Conjunctival Cells 4. TEARS |
|
|
Rabies
1. Epi Zoonotic 2. Susceptible via bite from 3. Respiratory from |
1. HIGHEST in Asia
2. Warm Blooded Animals 3. Bats |
|
|
RABIES
0. Irreversible stage 1. Incubation 2. Non specific symptoms @ Bite Site (2) 3. Progressive symptoms include (5) 4. Paralytic (2) 5. Death w/in |
0. Progressive stage
1. 20days to YEAR (d/t SoInnoculation) 2. Tingling pain & Weakness 3. Insomia, Confusion, Agitation, Hypersalvation & Dysphagiea 4. Disoreintation & Stupor 5. <7 days |
|
|
Rabies
1. Diagnosis (3) 2. Teatment Vaccination (prophylactic) 3. 1st dose (time & site) 4. 4 doses (time & site) 5. Booster doses (time & site) 6. |
1. Rt-PCR -saliva
FA & ELISA - Serum & CSF Negir Bodies & Babes nodules -Brain tissu 2. Wash wounds with SOAP & WATER 3. Site of Infection, 0 days & Ig (HRIG) 4. Deltoid & 1, 3, 7 & 14 5. Deltoid & 0 & 3 |
|
|
Human Rabies Immunio Globin
1. Not be administered to |
1. Previously vaccinated
|
|
|
Nipah virus
0. Disease 1. Family 2. Epi 3. Spreads via (4) 4. Only symptom |
0. Barking Pig Syndrome
1. Paramyxoviidae 2. Bangladesh & Mylasia 3. BAT feces/urine/saliva & Fruit juices 4. Encephalitis |
|
|
Rubeola (Measles) Virus
0. MORE SEVER IN 1. Family 2. Causes 3. More common in 4. Clinical Vignette 5. Reappear 6. Fulimant Course 7. Chronic Course 8. Viral RNA (not Virus) found in |
0. MALNOURISHED CHILDREN
1. Paramyxoviridae 2. SSPE (Subacute Sclerosing Pan Encephalitis) 3. Boys 4. Child becomes AGGRESSIVE in school 5. SLOW, FATAL after 10 years 6. 10%-Death in 3 months 7. Death in 4-10 years 8. Found in Brain biopsy |
|
|
Togaviradea (Rubella)
1. key Characterestic |
1. Carries on Ribosome
|
|
|
Myelits
1 Describe 2. May lead to 3. Symptoms (3) 4. Followed by 5. Leading cause 6. Leading cause before VACCINATION |
1. ACUTE inflammation of spinal cord
2. FLACCID paralysis 3. Headache, Fever & Irritation 4. WEAKNESS of ONE or MORE extremities 5. WEST NILE VIRUS 6. Poliovirus |
|
|
Name
A hole in the brain 1. w/ defined borders 2.w/ defined borders Vascular Inflammation of skin 3. w/ defined borders 4. w/o defined borders |
1. ABSCESS
2. EMPYEMA 3. ERYSIPELAS 4. VASCULITIS |
|
|
Brain Abscess & Empyema
1. Infection of (3) 2. At site abscess? d/t? 3. Infectious Agent |
1. Brain parenchyma, subdural & epidural
2. Dead Parenchyma d/t PRESSURE 3. Polymicrobial |
|
|
Brain Abscess & Empyema
1. Onset 2. Symptoms (3) 3. Clinical Vignette |
1. Rapid & associated w/ location
2. Headache, Generalized seizure & DROWSINESS → COMA 3. Abrupt change in behaviour |
|
|
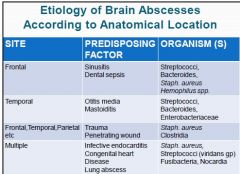
Describe the PREDISPOSING FACTORS & ORGANISMS for the following symptoms:
1. Frontal (2 & 4) 2. Temporal (2 & 3) 3. Frontal, Temporal, Parietal, etc. (2 & 2) 4. Multiple (4 & 4) |
|
|
|
Fungal Brain Abscess
1. Site of Entry (2) 2. Disseminated 3. What occurs early? Via 4. Name THREE important Fungi |
1. Lungs or Oropharynx
2. Hematogenously 3. Meningoencephalitis via Vascular Invasion 4. Aspegillus, Candida Albicans & Crytpoccous neoformans |
|
|
Name the defining characteresitc for the following fungi
1. Candida albcians 2. Aspergillus (2) 3. Cryptococcus neoformans |
1. PSEUDOHYPHAE
2. Monophasic: Always MOULD from, w/ ACUTE ANGLE septate 3. India Ink w/ Capsule & Muscarine stain |
|
|
Prion's Disease
1. Normal P^c 2. Abnormal P^Sc 3. Is 4. Nucleic Acid 5. Replicate w/o (2) 6. Resistant to (3) |
1. Glycoprotien w/ α helix
2. Glycoprotein w/ β -pleats 3. Abnormal isomer 4. ABSENT 5. Antibody or Inflammatory Response 6. 70% Alcohol, X-rays & UV light |
|
|
Transmissible Sponigform Encephalitis
1. Sensitive to (2) 2. Disease confined to 3. Inheritance 4. Seen in brain 5. Spongy appearance of cerebrum d/t (2) |
1. Autoclaving & Bleach
2. CNS 3. 15% 4. Myeloid plagues (modified protein aggreagates) 5. Vacuoles in cortex & Cerebeullum |
|
|
Name the FOUR methods of Transmissible Sponigform Encephalitis
|
Sporadic
Inherited Acquired (ingestion) Latrogenic (medical) |
|
|
Spread of Prions
1. Describe Sporadic (& examples) 2. Inherited (2) 3. Ingestion (acquired) (5) 4. Latrogenic (2) |
1. Rapdily progressive dementia (& CJD)
2. 10-15% via AD (Gerstmann-Straeussle-Scheinker syndrome) 3. Canabailism, incubation 20 yrs. invovles trunkal shaking & unsteady gait. Death w/in 3-24 years (KURU) 4. Via surgery or Organ transplant |
|
|
Transmissible Sponigform Encephalitis
1. MOST common Human PRION disease 2. Peak incidence 3. Symptoms a. Start b. Early symptoms (2) c. In 6 months d. Also involves (2) 4. Treatment |
1. CJD
2. 55-65 3aINSIDIOUS mental deterioration, b. Early Cerebellar & Visual problems c. SEVERE dementia d. Brain & LMN involvement 4. NONE |
|
|
FOUR Causes of CJD
|
1. Infected CORNEAL transplants
2. Unsterilized equipment 3. Piuitary Hormone injections from CADAVERS 4. Accidental cuts during surgery. autopsies |
|
|
Transmissible Sponigform Encephalitis d/t CJD
1. Known as 2. Diagnosis (3) |
1. Mad Cows Disease
2. Biopsy of Brain -Spongiform encepalopathy -Accumualtion of abnormally folded proteins 3. Sporadic disease 4. CSF no cells |
|
|
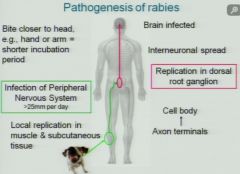
RABIES PATHOGENESIS
1. Shorter incubation period if 2. Local Replilcation in 3. Systemic Replication in 4. Travels from? To? 5. Rates of Infection Spread |
|