![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
417 Cards in this Set
- Front
- Back
|
Which one of the following conditions is most likely to result in secondary dysmenorrhoea? Adenomyosis Polycystic ovary syndrome Hypothyroidism Premature ovarian failure Bacterial vaginosis |
Adenomyosis |
|
|
Adenomyosis describes the |
extension of endometrial tissue into the uterine myometrium |
|
|
Primary dysmenorrhoea def |
is physiological affects up to 50% women usu within 1-2 yrs of menarche thought to be assoc with too much prostaglandin production |
|
|
Primary dysmenorrhoea fxs |
pain typically starts just before or within a few hours of the period starting suprapubic cramping pains which may radiate to the back or down the thigh |
|
|
Primary dysmenorrhoea mgmt |
NSAID works in 80% (block PG prodxn) = 1st line COCs = 2nd line |
|
|
2o dysmenorrhoea - is it pathological or physiological |
pathological |
|
|
is 1o dysmenorrhoea pathological or physiological |
physiological |
|
|
Secondary dysmenorrhoea typically develops many years after |
menarche and is the result of an underlying pathology pain usually starts 3-4 days before the onset of the period |
|
|
Secondary dysmenorrhoea causes |
endometriosis adenomyosis pelvic inflammatory disease intrauterine devices copper coils ONLY not MIRENA fibroids |
|
|
A 15 year old girl presents with amenorrhoea, having never started her periods. Which element of her history would lead you to reassure her that there is no need to investigate yet? She has not developed breasts or axillary/pubic hair Family history of late menarche History of acne and scanty, dark facial hair She is sexually active Cyclical abdominal pain |
Family history of late menarche |
|
|
Primary amenorrhoea can be diagnosed in women: |
- above the age of 14 with no secondary sexual characteristics, or - above the age of 16 with secondary sexual characteristics |
|
|
Primary amenorrhoea is commonly constitutional and has a familial distribution; in these cases there is no anatomical or physiological abnormality and patients will generally start menstruating by age |
18yo |
|
|
1o amenorrhoea can occur with no abn/path in women who have a |
fhx of late menarche generally will start by age 18 |
|
|
Cyclical abdominal pain associated with amenorrhoea may suggest an anatomical abnormality such as an |
imperforate hymen |
|
|
Lack of breast or body hair development suggests this is true |
primary amenorrhoea and so warrants investigation |
|
|
Acne and facial hair may suggest |
virilisation, e.g. in polycystic ovarian syndrome |
|
|
In a woman who is sexually active, pregnancy may be a cause of |
amenorrhoea and should always be excluded |
|
|
Amenorrhoea may be divided into |
primary (failure to start menses by the age of 16 years) or secondary (cessation of established, regular menstruation for 6 months or longer) |
|
|
1o amenorrhoea def |
failure to start menses by the age of 16 years |
|
|
2o amenorrhoea def |
cessation of established, regular menstruation at least 6 months |
|
|
Causes of primary amenorrhoea |
Turner's syndrome testicular feminisation congenital adrenal hyperplasia congenital malformations of the genital tract |
|
|
Secondary amenorrhoea causes |
hypothalamic amenorrhoea (e.g. Stress, excessive exercise) polycystic ovarian syndrome (PCOS) hyperprolactinaemia premature ovarian failure thyrotoxicosis/hypothyroidism Sheehan's syndrome Asherman's syndrome (intrauterine adhesions) |
|
|
Initial investigations of Amenorrhoea |
exclude pregnancy with urinary or serum bHCG gonadotrophins: low levels indicate a hypothalamic cause where as raised levels suggest an ovarian problem (e.g. Premature ovarian failure) prolactin androgen levels: raised levels may be seen in PCOS oestradiol thyroid function tests |
|
|
summary of initial inV of amenorrhoea |
urine/serum bHCG gonadotrophins - FSH & LH prolactin androgen levels - (PCOS = UP testosterone) oestradiol TFTs |
|
|
gonadotrophin |
any of a group of hormones secreted by the pituitary which stimulate the activity of the gonads |
|
|
Progesterone is the dominant ovarian hormone secreted during the |
luteal (second) phase of the menstrual cycle |
|
|
Progesterone is the dominant ovarian hormone secreted during the luteal (second) phase of the menstrual cycle. Its main function is to |
prepare the uterus for implantation of an embryo, in the event that fertilisation occurs during that cycle. If pregnancy occurs, human chorionic gonadotropin (hCG) is released which maintains the corpus luteum, which in turn allows progesterone levels to remain raised. At approximately twelve weeks gestation, the placenta begins to produce progesterone in place of the corpus luteum. Progesterone levels decrease after delivery and during breastfeeding. |
|
|
Progesterone levels are low in women after menopause |
true |
|
|
In males almost all progesterone is converted to testosterone in the testes. |
true |
|
|
testosterone func |
development and maintenance of male sexual characteristics stimulates anabolic processes in non-sexual tissues |
|
|
In males, LH stimulates the Leydig cells in the testes to produce |
testosterone. A small amount of testosterone in males is produced by the adrenal glands |
|
|
In females, the majority of testosterone is produced by |
peripheral conversion of androgen precursor steroids to testosterone, with the remainder produced in the ovaries and adrenal glands. |
|
|
to confirm preg, what do you need to test |
bHCG serum/urine ONLY |
|
|
generally what hormone do you need to test for menopause |
usu. only FSH |
|
|
Oestradiol is the principal oestrogen in |
females who are ovulating and the dominant ovarian hormone during the follicular (first) phase of the menstrual cycle The concentration of oestradiol varies throughout the menstrual cycle. Oestradiol is released in parallel to follicular growth and is highest when the follicle matures (prior to ovulation). Oestradiol production gradually reduces if the oocyte released by the follicle is unfertilised. Laboratory testing routinely measures E2 forms of oestradiol, most of which is bound to sex hormone-binding globulin (SHBG). Oestradiol levels decrease significantly during menopause. |
|
|
In males, oestrogen is an essential part of the reproductive system, and is required for |
maturation of sperm Primary hypogonadism (impaired response to gonadotropins including LH and FSH) can result in increased testicular secretion of oestradiol and increased conversion of testosterone to oestradiol. Obesity may also increase oestrogen levels in males. 3 An increase in the ratio of oestrogen to androgens in males is associated with gynaecomastia (the development of breast tissue). |
|
|
MEDLAB NZ provides details on lab https://cdr.medlabcentral.co.nz/handbook/ |
tests look under collection guide other sites lab plus nz lab tests |
|
|
ruby is a |
german rubella aka german measles |
|
|
Roseola infantum |
starts as high fever when fever goes, rash starts on face and/OR body +- runny nose, irritability, tiredness mainly in infancy (rare in adults) saliva via person to person transmission |
|
|
Roseola is a disease caused by |
human herpes virus type 6B (HHV-6B) and possibly type 7 (HHV-7) |
|
|
Roseola infantum key fx |
fever followed later by rash |
|
|
Roseola infantum also known as |
exanthem subitum, occasionally sixth disease |
|
|
Roseola infantum fxs |
high fever: lasting a few days, followed by a maculopapular rash febrile convulsions occur in around 10-15% diarrhoea and cough are also commonly seen |
|
|
Other possible consequences of HHV6 infection |
aseptic meningitis hepatitis |
|
|
A 24-year-old heroin addict is admitted following an overdose. He is drowsy and has a respiratory rate of 6 / min. Which of the following arterial blood gas results (taken on room air) are most consistent with this? |
pH = 7.31; pCO2 = 7.4 kPa; pO2 = 8.1 kPa This patient is likely to have developed a respiratory acidosis secondary to hypoventilation. |
|
|
opioid OD will cause what changes on ABG |
respiratory acidosis secondary to hypoventilation. E.G. pH = 7.31; pCO2 = 7.4 kPa; pO2 = 8.1 kPa |
|
|
Respiratory acidosis may be caused by a number of conditions |
COPD decompensation in other respiratory conditions e.g. life-threatening asthma / pulmonary oedema sedative drugs: benzodiazepines, opiate overdose |
|
|
A 19-year-old female presents complaining of visual disturbance. Examination reveals a bitemporal hemianopia with predominately the lower quadrants being affected. What is the most likely lesion? |
Craniopharyngioma |
|
|
A 17 year old girl presents with a history of amenorrhoea, having never started her period. On further questioning she has developed secondary sexual characteristics, such as growth of breast tissue and pubic hair. She also complains of pelvic pain and some bloating.Which of the following is likely to be the cause? |
Imperforate hymen |
|
|
An imperforate hymen would |
block passage of menses, causing amenorrhoea without affecting development of secondary characteristics such as pubic hair and breast development. This can cause a build up of menstrual blood in the vagina (haematocolpos), causing pelvic pain and bloating through a pressure effect. |
|
|
IMPERFORATE hymen effect |
amenorrhoea no effect on d/t of 2o sex. characteristics build up of menstrual blood in the vag (haematocolpos) causes: - pelvic pain - bloating due to pressure effect |
|
|
Chemotherapy at a young age has the potential to damage the |
hypothalamic-pituitary-ovarian axis |
|
|
while Turner's syndrome can cause |
premature ovarian failure |
|
|
Excessive exercise and/or rapid loss of body weight can also cause |
a reduction in oestrogen secretion |
|
|
You are fast-bleeped to the respiratory ward to review a 70-year-old man with known chronic obstructive pulmonary disease (COPD) who has become 'unresponsive'. On arrival you note the following:Airwayoropharyngeal airway already in-situBreathingrespiratory rate 6/minoxygen saturations 99% on 15 l/min oxygenCirculationheart rate 96/minblood pressure 88/60 mmHgAnother doctor has already taken arterial blood gases (on 15 l/min oxygen):pH7.15pCO214.5 kPapO217.1 kPaBicarbonate34.5 mmol/lBase excess+10.6 mmol/lWhat do the arterial blood gases show? |
Acute-on-chronic respiratory acidosis with a partial metabolic compensation |
|
|
Overgrowth of which one of the following organisms is most likely to cause bacterial vaginosis? |
predominately Gardnerella vaginalis (anaerobe) This leads to a consequent fall in lactic acid producing aerobic lactobacilli resulting in a raised vaginal pH. |
|
|
is bacterial vaginosis and STI |
no, but seen mainly in sexually active women |
|
|
fxs of bacterial vaginosis (BV) |
vaginal discharge: 'fishy', offensive asymptomatic in 50% |
|
|
Amsel's criteria for diagnosis of BV - 3 of the following 4 points should be present |
thin, white homogenous discharge clue cells on microscopy: stippled vaginal epithelial cells vaginal pH > 4.5 positive whiff test (addition of potassium hydroxide results in fishy odour) |
|
|
MGMT OF BV |
ORAL metronidazole |
|
|
Bacterial vaginosis in pregnancy |
increased risk of: - preterm labour, - low birth weight and chorioamnionitis, late miscarriage it was previously taught that oral metronidazole should be avoided in the first trimester and topical clindamycin used instead. Recent guidelines however recommend that oral metronidazole is used throughout pregnancy. The BNF still advises against the use of high dose metronidazole regimes |
|
|
A 65 year old gentleman with known multiple myeloma presents with abdominal pain, polydipsia and confusion. Some blood results are shown below. px has hypercalcemia, hypernatremia What is the most important initial management of his symptoms? |
IV 0.9% saline he has polydipsia, and is likely to be dehydrated he is also sxmatic |
|
|
Hypercalcaemia: management |
initial = normal saline (rehydration) next +- bisphosphonates other options - calcitonin (quicker effect to bis) - steroids in sarcoidosis |
|
|
organic vs non organic cause of dis/illness |
organic cause relates to a cause assoc with physical or physiological change to some tissue or organ of the body non organic cause = psyc cause |
|
|
A conversion disorder causes patients to |
suffer from neurological symptoms, such as numbness, blindness, paralysis, or fits without a definable organic cause thought that sxs arise in response to stressful situations affecting the pxs mental health |
|
|
A 18-year-old sprinter who is currently preparing for a national athletics meeting asks to see the team doctor due to an unusual sensation in his legs. He describes a numb sensation below his knee. On examination the patient there is apparent sensory loss below the right knee in a non-dermatomal distribution. The team doctor suspects a non-organic cause of his symptoms. This is an example of a: |
Conversion disorder |
|
|
Somatisation disorder fxs |
multiple physical SYMPTOMS present for at least 2 years patient refuses to accept reassurance or negative test results |
|
|
Hypochondrial disorder fxs |
persistent belief in the presence of an underlying serious DISEASE, e.g. cancer patient again refuses to accept reassurance or negative test results |
|
|
diffference b/w munchausen syndrome and malingering |
munchausen = making up sxs for psych gain of playing a sick role
malingering = making up or exaggerating sxs for material GAIN |
|
|
Dissociative disorder |
separating certain memories from normal consciousness includes psyc sxs |
|
|
Dissociative disorder vs dissociative identity disorder (DID) |
dissociative identity disorder (DID) is the new term for multiple personality disorder as is the most severe form of dissociative disorder |
|
|
A 35-year-old female who has recently being diagnosed with Grave's disease presents for review 3 months after starting a 'block and replace' regime with carbimazole and thyroxine. She is concerned about developing thyroid eye disease. What is the best way that her risk of developing thyroid eye disease can be reduced? |
Stop smoking |
|
|
most important modifiable risk factor for the development of thyroid eye disease is |
STOP SMOKING |
|
|
A 45-year-old woman who is being treated for Hodgkin's lymphoma with ABVD chemotherapy is reviewed on the haematology ward. She has been admitted by her GP with a fever of 38.9ºC. Her blood count from two days ago was as follows: low Hb, WBC, neutrophils and lymphocytes elevated platelets Blood pressure is 102/66 mmHg and the heart rate is 96/min. Respiratory examination is unremarkable. You insert an intravenous cannula and take bloods including cultures. What is the most appropriate next step in management? |
Start intravenous piperacillin with tazobactam (Tazocin) dx = Neutropenic sepsis |
|
|
Neutropenic sepsis is a common complication of |
CHEMO for cancer |
|
|
Neutropenic sepsis def |
neutrophil count of < 0.5 * 109 in px getting anticancer chemo and one of the following: - high fever >38 or - other signs/sxs of clinically sig. sepsis |
|
|
in chemo cancer pxs suspected of having neutropenic sepsis - what can be given as prophylaxis |
fluoroquinolone |
|
|
Neutropenic sepsis mgmt |
Empirical Abx STAT (dont wait for WBC) =piperacillin with tazobactam (Tazocin) next specialist help no response = +- meropenem +- vanc still no response = inV fungal infxns +- G-CSF |
|
|
whats the initial mgmt of neutropenic sepsis |
Empirical Abx STAT (dont wait for WBC) = piperacillin with tazobactam (Tazocin) |
|
|
You are counselling a 24-year-old woman who has just found out she is pregnant. She currently smokes 20 cigarettes/day. Which one of the following is most associated with smoking during pregnancy? Neonatal abstinence syndrome Microcephaly Pre-eclampsia Increased risk of pre-term labour Postnatal restricted growth |
Increased risk of pre-term labour |
|
|
Pregnancy and drugs Smoking increases the risk of |
miscarriage pre-term labour stillbirth IUGR sudden unexpected death in infancy |
|
|
Alcohol in preg increases the risk of |
FAS learning difficulties characteristic facies:smooth philtrum, thin vermilion, small palpebral fissures IUGR & postnatal restricted growth microcephaly Binge drinking is a major risk factor for FAS |
|
|
Cannabis in preg increases the risk of |
Similar to smoking risks due to tobacco content |
|
|
Cocaine in preg increases the risk of |
Maternal risks = HTN incl preeclampsia = placental abruption Fetal risk = prematurity = neonatal abstinence syndrome |
|
|
Heroin in preg increases the risk of |
= neonatal abstinence sydrome |
|
|
Which one of the following patients should not automatically beprescribed a statin in the absence of any contraindication? |
A 47-year-old man with well controlled diabetes mellitus type 2 with a 10-year cardiovascular risk of 9% |
|
|
should you give a statin to this px A 51-year-old man who had a myocardial infarction 4 years ago and is now asymptomatic |
yes |
|
|
should you give a statin to this px A 57-year-old female smoker with a 10-year cardiovascular risk of 23% |
yes |
|
|
should you give a statin to this px A 53-year-old man with intermittent claudication |
yes |
|
|
should you give a statin to this px A 62-year-old man who had a transient ischaemic attack 10 months ago |
yes |
|
|
statin moa |
inhibit the action of HMG-CoA reductase, the rate-limiting enzyme in hepatic cholesterol synthesis |
|
|
Who should receive a statin? |
all people with established cardiovascular disease (stroke, TIA, ischaemic heart disease, peripheral arterial disease) |
|
|
Who should receive a statin? |
NICE recommend anyone with a 10-year cardiovascular risk >= 10% |
|
|
Who should receive a statin? |
patients with type 2 diabetes mellitus should now be assessed using QRISK2 like other patients are, to determine whether they should be started on statins |
|
|
what does most of cholesterol synthesis take place in us |
at night as this is when the majority of cholesterol synthesis takes place thus statin should be taken at night too This is especially true for simvastatin which has a shorter half-life than other statins |
|
|
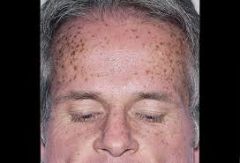
A 52-year-old woman presents with pruritus and lethargy. She has recently put on weight and is complaining about dry skin |
Hypothyroidism |
|
|
A 57-year-old woman presents with pruritus. She states she has been gaining weight despite eating less and complains of constant nausea. On examination she is pale |
Chronic kidney disease |
|
|
A 59-year-old man complains of pruritus and lethargy. On examination he has spoon shaped nails and a smooth tongue |
Iron deficiency anaemia |
|
|
main characteristics of the most important causes of pruritus |
liver dis iron def anaemia polycythemia chronic kidney dis lymphoma Other causes: hyper- and hypothyroidism diabetes pregnancy 'senile' pruritus urticaria skin disorders: eczema, scabies, psoriasis, pityriasis rosea |
|
|
Liver disease fxs |
History of alcohol excess Stigmata of chronic liver disease: spider naevi, bruising, palmar erythema, gynaecomastia etc Evidence of decompensation: ascites, jaundice, encephalopathy |
|
|
Iron deficiency anaemia fxs |
Pallor Other signs: koilonychia, atrophic glossitis, post-cricoid webs, angular stomatitis |
|
|
Polycythaemia fxs |
Pruritus particularly after warm bath 'Ruddy complexion' Gout Peptic ulcer disease |
|
|
Chronic kidney disease fxs |
Lethargy & pallor Oedema & weight gain Hypertension |
|
|
Lymphoma fxs fxs |
Night sweats Lymphadenopathy Splenomegaly, hepatomegaly Fatigue |
|
|
elicit the triceps reflex by placing arm across her chest and striking the triceps tendon with a tendon hammer. Which nerve (and its nerve root) are you testing? |
Radial nerve C7 |
|
|
radial nerve info |
The radial nerve innervates the triceps muscle. It is primarily derived from the C7 nerve root.The radial nerve is the motor supply to the extensor compartments of the upper arm. The triceps muscle is the chief extensor of the forearm. Its name derives from its three heads of origin; the long, lateral and medial heads. It attaches into the olecranon of the ulna.It is these components which form the triceps reflex arc. |
|
|
Musculocutaneous nerve (C5-C7) |
MOTOR Elbow flexion (supplies biceps brachii) and supination SENSORY Lateral part of the forearm Typical mechanism of injury & notes Isolated injury rare - usually injured as part of brachial plexus injury |
|
|
Axillary nerve (C5,C6) |
MOTOR Shoulder abduction (deltoid muscle) SENSORY Inferior region of the deltoid muscle Typical mechanism of injury & notes Humeral neck fracture/dislocation Results in flattened deltoid |
|
|
DOES musculocutaneous or axillary nerve injury lead to flat deltoid |
AXILLARY NERVE |
|
|
Radial nerve (C5-C8) |
MOTOR Extension (forearm, wrist, fingers, thumb) SENSORY Small area between the dorsal aspect of the 1st and 2nd metacarpals Typical mechanism of injury & notes Humeral midshaft fracture Palsy results in wrist drop |
|
|
Median nerve (C6, C8, T1) |
MOTOR LOAF mus Features depend on the site of the lesion: - wrist: paralysis of thenar muscles, opponens pollicis - elbow: loss of pronation of forearm and weak wrist flexion SENSORY Palmar aspect of lateral 3½ fingers Typical mechanism of injury & notes Wrist lesion → carpal tunnel syndrome |
|
|
*LOAF muscles |
Lateral two lumbricals Opponens pollis Abductor pollis brevis Flexor pollis brevis |
|
|
Ulnar nerve (C8, T1) |
MOTOR Intrinsic hand muscles except LOAF* Wrist flexion SENSORY Medial 1½ fingers Typical mechanism of injury & notes Medial epicondyle fracture Damage may result in a 'claw hand' |
|
|
Long thoracic nerve (C5-C7) |
MOTOR serratus anterior SENSORY = NON Typical mechanism of injury & notes Often during sport e.g. following a blow to the ribs. Also possible complication of mastectomy Damage results in a winged scapula |
|
|
Erb-Duchenne palsy ('waiter's tip') PALSY |
damage to C5, C6 arm hangs by the side and is internally rotated, elbow extended DAVID HAS ERBS |
|

Klumpke injury |
C8, T1 damage |
|
|
A 45-year-old man presents with a painful swelling on the posterior aspect of his elbow. There is no history of trauma. On examination an erythematous tender swelling is noted. What is the most likely diagnosis? |
Olecranon bursitis |
|
|
Olecranon bursitis |
Swelling over the posterior aspect of the elbow. There may be associated pain, warmth and erythema. It typically affects middle-aged male patients. |
|
|
The causes of clubbing may be divided into cardiac, respiratory and other |
Cardiac causes cyanotic congenital heart disease (Fallot's, TGA) bacterial endocarditis atrial myxoma Respiratory causes lung cancer pyogenic conditions: cystic fibrosis, bronchiectasis, abscess, empyema tuberculosis asbestosis, mesothelioma fibrosing alveolitis Other causes Crohn's, to a lesser extent UC cirrhosis, primary biliary cirrhosis Graves' disease (thyroid acropachy) rare: Whipple's disease |
|
|
A 3-year-old child is brought to surgery as her mother has noticed that she is 'cross-eyed'. The corneal light reflection test confirms this. What is the most appropriate management? |
Refer to ophthalmology |
|
|
Refer children with a squint immediately to |
ophthalmology |
|
|
squint aka |
strabismus |
|
|
Squint (strabismus) is characterised by |
misalignment of the visual axes IE CROSS EYED Squints may be divided into concomitant (common) and paralytic (rare) |
|
|
Squints may be divided into |
oncomitant (common) and paralytic (rare) |
|
|
Concomitant SQUINT |
Due to imbalance in extraocular muscles Convergent is more common than divergent |
|
|
Paralytic SQUINT |
Due to paralysis of extraocular muscles |
|
|
SQUINT DX |
made by the corneal light reflection test - holding a light source 30cm from the child's face to see if the light reflects symmetrically on the pupils |
|
|
The cover test is used to identify the nature of the squint |
ask the child to focus on a object cover one eye observe movement of uncovered eye cover other eye and repeat test |
|
|
SQUINT MGMT |
eye patches may help prevent amblyopia referral to secondary care is appropriate |
|
|
A 27-year-old man presents with a nocturnal cough and a feeling of wheeziness when he plays football. He is a non-smoker and generally fit and well. He has no pets and works as an accountant. There is no history of asthma or any other respiratory problems as a child. Respiratory examination today is unremarkable.According to British Thoracic Society (BTS) guidelines, what is the most appropriate next step to investigate the possibility of asthma? Give him a trial of a salbutamol inhaler Arrange spirometry Prescribe a peak flow meter and ask him to keep a diary |
Arrange spirometry |
|
|
The British Thoracic Society (BTS) recommend reversibility testing for adults and children with asthma |
reversibility testing for all adult patients with suspected asthma, regardless of the probability children, tests of reversibility are generally only used when there is a low or intermediate probability of asthma. |
|
|
BTS recommend classifying pxs as either |
a high, intermediate or low probability of asthma based on the presence or absence of certain symptoms: |
|
|
for adults dx of asthma |
hx then exam then spirometry (or PEF if not available) next +- reversibility testing |
|
|
Features which make a diagnosis of asthma more likely |
More than one of the following symptoms: wheeze, breathlessness, chest tightness and cough, particularly if: -symptoms worse at night and in the early morning -symptoms in response to exercise, allergen exposure and cold air -symptoms after taking aspirin or beta blockers History of atopic disorder Family history of asthma and/or atopic disorder Widespread wheeze heard on auscultation of the chest Otherwise unexplained low FEV1 or PEF (historical or serial readings) Otherwise unexplained peripheral blood eosinophilia |
|
|
Features which make a diagnosis of asthma less likely |
Prominent dizziness, light-headedness, peripheral tingling Chronic productive cough in the absence of wheeze or breathlessness Repeatedly normal physical examination of chest when symptomatic Voice disturbance Symptoms with colds only Significant smoking history (ie > 20 pack-years) Cardiac disease Normal PEF or spirometry when symptomatic |
|
|
if px has many of the fxs which make a diagnosis of asthma more likely = |
high prob of asthma = start trial of tx aka reversability testing - if good response = +ve revers. testing - if poor response = further inV intermediate prob = further inV + reversibility testing low prob = further InV +- resp specialist referral |
|
|
whats the most important initial asthma tx? |
Patients should start treatment at the step most appropriate to the initial severity of their asthma |
|
|
indications for asthmatic using inhaled steroids |
exacerbations of asthma in the last two years using inhaled β2 agonists three times a week or more symptomatic three times a week or more waking one night a week |
|
|
in terms of dx asthma adult pxs if px is low, intermediate, high risk what should you do |
low = further InV +- resp spec. referral intermediate = further inV + reversibility testing high = reversibility testing |
|
|
so for dx of asthma px you need to first take a history and exam so you can |
risk stratify ie low, intermed, high after you risk stratify - follow the dx process |
|
|
in terms of reversibility what is considered sig |
> 400 ml improvement in FEV1 is considered significant - in a px before and after inhaled salbutamon with dx uncertain and airflow obstrxn - if they dont respond to inhaled salbutamol, and then you give ICS or oral prednisolone |
|

is this infective exacerbation of COPD or is it LV failure |
Left ventricular failure |
|
|
pul edema fxs on CXR |
bat's wing appearance alveolar oedema interstitial oedem aleft pleural effusion upper lobe diversion |
|
|
pul edema is most commonly cause by |
Left ventricular failure |
|
|
A 25 -year-old female presents to her GP with heavy painful bleeding during menstruation. She does not wish to have contraception. Which of the following is most suitable? |
Naproxen |
|
|
Tranexamic acid would be effective for |
menorrhagia but not help the dysmenorrhoea. |
|
|
The intrauterine system is of course a very effective treatment for |
menorrhagia and is often used as first line treatment for this condition |
|
|
Norethisterone is useful for helping combat flooding for short periods of time |
true |
|
|
whats the first line tx for menorrhagia |
intrauterine system (Mirena) should be considered first-line |
|
|
2-month-old girl is brought to surgery with poor feeding and vomiting. Mother reports that her urine has a strong smell. A urinary tract infection is suspected. What is the most appropriate management? |
Refer immediately to hospital |
|
|
InV of UTI in infants/children |
urine sample - clean catch preferable |
|
|
mgmt of UTI in infants <3months |
should be referred immediately to a paediatrician |
|
|
mgmt of UTI in infants > 3 months upper UTI |
admit
if not admitted start oral abx (cephs/augmentum) |
|
|
mgmt of UTI in infants> 3 months lower UTI |
outpx tx with abx trimethoprim, nitrofurantoin, cephalosporin or amoxicillin |
|
|
antibiotic prophylaxis is not given after the first UTI but should be considered with recurrent UTIs |
true |
|
|
A 4-week-old child is brought to clinic with a red rash on her scalp associated with yellow flakes. What is the most likely diagnosis? |
Seborrhoeic dermatitis |
|
|
Seborrhoeic dermatitis is a relatively common skin disorder |
seen in children |
|
|
Seborrhoeic dermatitiscommon skin disorder seen in children. It typically affects the |
scalp ('Cradle cap'), nappy area, face and limb flexures. |
|
|
Seborrhoeic dermatitis in children whats one of the first signs of this |
Cradle cap is an early sign which may develop in the first few weeks of life. It is characterised by an erythematous rash with coarse yellow scales. |
|
|
Seborrhoeic dermatitis in children mgmt |
depends on severity mild-moderate: baby shampoo and baby oils severe: mild topical steroids e.g. 1% hydrocortisone |
|
|
Seborrhoeic dermatitis in children tends to resolve spontaneously by around 8 months of age |
true |
|
|
A 46-year-old woman presents to surgery complaining of a dry mouth and dry eyes for the past 6 months. She has also generalised arthralgia and is more tired than normal. Which one of the following autoantibodies is most associated with primary Sjogren's syndrome? anti-RNP Anti-Ro Anti-smooth muscle Anti-centromere Anti-Sm |
Anti-Ro |
|
|
Sjogren's syndrome def |
autoimmune disorder affecting exocrine glands resulting in dry mucosal surfaces |
|
|
Sjogren's syndrome |
It may be primary (PSS) or secondary to rheumatoid arthritis or other connective tissue disorders, where it usually develops around 10 years after the initial onset. Sjogren's syndrome is much more common in females (ratio 9:1). There is a marked increased risk of lymphoid malignancy (40-60 fold) |
|
|
Sjogren's syndrome sig increases the risk of |
lymphoid malig 40-60x |
|
|
inV for sjogrens syndrome |
RF +ve in nearly 100% pxs ANA +ve 70% anti-RO 70% anti-La 30% Schirmer's test: filter paper near conjunctival sac to measure tear formation histology: focal lymphocytic infiltration also: hypergammaglobulinaemia, low C4 |
|
|
mgmt of sjogrens syndrome |
artificial saliva and tears pilocarpine may stimulate saliva production |
|
|
A newly qualified staff nurse at the local hospital undergoes vaccination against hepatitis B. The following results are obtained three months after completion of the primary course: Anti-HBs10 - 100 mIU/ml What is the most appropriate course of action? |
Give one further dose of hepatitis B vaccine |
|
|
px given hep b immunisation: Anti-HBs level (mIU/ml)> 100 |
Indicates adequate response, no further testing required. Should still receive booster at 5 years |
|
|
px given hep b immunisation: Anti-HBs level (mIU/ml)10 - 100 |
Suboptimal response - one additional vaccine dose should be given. If immunocompetent no further testing is required |
|
|
px given hep b immunisation: Anti-HBs level (mIU/ml) < 10 |
Non-responder. Test for current or past infection. Give further vaccine course (i.e. 3 doses again) with testing following. If still fails to respond then HBIG would be required for protection if exposed to the virus |
|
|
Management of chronic hepatitis B in nz |
Peginterferon alfa first line |
|
|
Complications of hepatitis B infection |
chronic hepatitis (5-10%) fulminant liver failure (1%) hepatocellular carcinoma glomerulonephritis polyarteritis nodosa cryoglobulinaemia |
|
|
The features of hepatitis B include fever, jaundice and elevated liver transaminases. |
true |
|
|
Meig's syndrome is a triad of |
ascites, pleural effusion and benign ovarian tumor (fibroma,Brenner tumour and occasionally granulosa cell tumour) |
|
|
Pleural effusion |
Exudate (> 30g/L protein) Transudate (< 30g/L protein) |
|
|
Pleural effusion Exudate (> 30g/L protein) causes |
infection: pneumonia, TB, subphrenic abscess connective tissue disease: RA, SLE neoplasia: lung cancer, mesothelioma, metastases pancreatitis pulmonary embolism Dressler's syndrome yellow nail syndrome |
|
|
Pleural effusion Transudate (< 30g/L protein) |
heart failure hypoalbuminaemia (liver disease, nephrotic syndrome, malabsorption) hypothyroidism Meigs' syndrome |
|
|
A 52-year-old female presents with weakness and pins and needles in her right hand. On examination she has wasting of the thenar eminence associated with sensory loss to the palmar aspect of lateral (radial) three fingers. Which nerve is likely to be affected? |
Median nerve |
|
|
Anterior interosseous nerve (branch of median nerve) |
leaves just below the elbow results in loss of pronation of forearm and weakness of long flexors of thumb and index finger |
|
|
Patterns of damage of median nerve |
Damage at wrist e.g. carpal tunnel syndrome paralysis and wasting of thenar eminence muscles sensory loss to palmar aspect of lateral (radial) 3 1/2 fingers Damage at elbow, as above plus: unable to pronate forearm weak wrist flexion ulnar deviation of wrist Anterior interosseous nerve (branch of median nerve) leaves just below the elbow results in loss of pronation of forearm and weakness of long flexors of thumb and index finger |
|

One particular mole is noted due to the irregular border. It is 6 * 4 mm in size. What is the most appropriate action? |
Refer under the two-week rule to dermatology |
|
|
Malignant melanoma: prognostic factors |
The invasion depth of a tumour (Breslow depth) is the single most important factor in determining prognosis of patients with malignant melanoma |
|
|
The invasion depth of a tumour (Breslow depth) |
true |
|
|
whatsthe single most important factor in determining prognosis of patients with malignant melanoma |
invasion depth of a tumour (Breslow depth) |
|
|
Breslow Thickness < 1 mm |
Approximate 5 year survival 95-100% |
|
|
Breslow Thickness 1 - 2 mm |
Approximate 5 year survival80-96% |
|
|
Breslow Thickness2.1 - 4 mm |
Approximate 5 year survival60-75% |
|
|
Breslow Thickness> 4 mm |
Approximate 5 year survival50% |
|
|
A 78 year old lady with known type 2 diabetes presents with a 1 week history of polydipsia, feeling generally unwell and drowsy. On examination she looks very dehydrated and is difficult to rouse. She appears confused when she does talk to you.Admission bloods show: Na+149 mmol/lK+5.2 mmol/lUrea22.1 mmol/lCreatinine254 µmol/lHer blood glucose is 36 mmol/L. What's the most important first management step? |
Rehydrate with 0.9% Saline |
|
|
DM2 px with polydipsia, generally unwell and drowsy, dehydrated, confused, hypernatremic develops renal failure, sig raised serum glucose dx and mgmt |
HONK first mgmt step = REHYDRATE with 0.9 % saline |
|
|
HONK is |
hyperosmolar non-ketotic |
|
|
HONK is characterised by: |
1.) Severe hyperglaycaemia 2.) Dehydration and renal failure 3.) Mild/absent ketonuria |
|
|
HONK has a mortality of |
50% |
|
|
This partly because of its' insidious onset but also because many cases occur in newly diagnosed type 2 diabetics. The mortality of HONK occurs from complications of the hyperosmolar state namely; |
rhabdomyolysis, venous thromboembolism, lactic acidosis, hypertriglyceridaemia, renal failure, stroke and cerebral oedema. |
|
|
precipitants of HONK. Precipitants include: |
New diagnosis of type 2 diabetes Infection High dose steroids Myocardial infarction Vomiting Stroke Thromboembolism Poor treatment compliance |
|
|
The central management of HONK is |
supportive care and slow metabolic resolution |
|
|
avoid rapid fluid r/t in HONK pxs why |
rapid osmolar shifts can cause cerebral oedema. |
|
|
mgmt of HONK |
fluid resus with 0.9% Saline next insulin sliding scale |
|
|
Hyperosmolar hyperglycaemic state (HHS) is confirmed by: |
Dehydration Osmolality >320mosmol/kg Hyperglycaemia >30 mmol/L with pH >7.3, bicarbonate >15mmolL and no significant ketonenaemia <3mmol/L |
|

dx |
Left lower lobe collapse left lower lobe collapses medially and posteriorly behind the heart. The classic result is a triangular opacity giving the heart an unusually straight border. |
|
|
When assessing a patient with suspected chronic obstructive pulmonary disease, which one of the following is least relevant? |
Peak expiratory flow |
|
|
Peak expiratory flow is of no value in the diagnosis of |
COPD |
|
|
COPD dx |
clinical - SOB, CHRONIC COUGH, regular sputum prodxn SPIROMETRY CXR FBC (exclude 2o polycythemia) BMI |
|
|
A 64-year-old man with a history of Parkinson's disease is reviewed in clinic and a decision has been made to start him on cabergoline. Which one of the following adverse effects is most strongly associated with this drug? |
Pulmonary fibrosis |
|
|
Parkinson's disease: management |
delay treatment until the onset of disabling symptoms and then to introduce a dopamine receptor agonist. If the patient is elderly, levodopa is sometimes used as an initial treatment. |
|
|
Parkinson's disease: management
Dopamine receptor agonists |
Bromocriptine, ropinirole, cabergoline, apomorphine,pergolide |
|
|
ergot-derived dopamine receptor agonists (bromocriptine, cabergoline, pergolide*) have been associated with |
pulmonary, retroperitoneal and cardiac fibrosis The Committee on Safety of Medicines advice that an echocardiogram, ESR, creatinine and chest x-ray should be obtained prior to treatment and patients should be closely monitored |
|
|
Dopamine receptor agonists AE |
pulmonary, retroperitoneal and cardiac fibrosis impulse control disorders and excessive daytime somnolence hallucinations in elderly nasal congestion and postural hypotension |
|
|
Levodopa |
is dopamine analog usually combined with a decarboxylase inhibitor (e.g. carbidopa or benserazide) to prevent peripheral metabolism of levodopa to dopamine |
|
|
Levodopa AE |
dyskinesia (involuntary writhing movements), 'on-off' effect, dry mouth, anorexia, palpitations, postural hypotension, psychosis, drowsiness |
|
|
MAO-B (Monoamine Oxidase-B) inhibitors |
e.g. Selegiline inhibits the breakdown of dopamine secreted by the dopaminergic neurons |
|
|
Amantadine |
mechanism is not fully understood, probably increases dopamine release and inhibits its uptake at dopaminergic synapses |
|
|
Amantadine AE |
include ataxia, slurred speech, confusion, dizziness and livedo reticularis |
|
|
COMT (Catechol-O-Methyl Transferase) inhibitors |
e.g. Entacapone, tolcapone COMT is an enzyme involved in the breakdown of dopamine, and hence may be used as an adjunct to levodopa therapy used in conjunction with levodopa in patients with established PD |
|
|
Antimuscarinics |
block cholinergic receptors now used more to treat drug-induced parkinsonism rather than idiopathic Parkinson's disease help tremor and rigidity e.g. procyclidine, benzotropine, trihexyphenidyl (benzhexol) |
|
|
if a px had a drug induced parkinsonism what would you give them |
?antimuscarinic |
|
|
You are called to see a 25-year-old 10 week pregnant lady in the Emergency Department complaining of abdominal pain and heavy vaginal bleeding. Her observations are normal and she is afebrile, on ultrasound a fetal heart rate is still present and the uterus is the size expected. On examination her cervical os is closed. How would you classify her miscarriage? |
Threatened |
|
miscarriage MTIICR MyTIICRuel |
missed = no bleeding & empty sac threatened = bleeding & closed c. os inevitable = open c. os incomplete = preg. tissue partially expelled complete = all preg tissue expelled recurrent = >= 3 consec miscarriages <22 wees |
|
|
CREST syndrome is a subtype of |
Limited cutaneous systemic sclerosis |
|

Please look at the hands of this 50-year-old lady. She complains of tight, stiff fingers that turn white in the cold. DX |
Limited cutaneous systemic sclerosis |
|
|
Limited cutaneous systemic sclerosis remember a subtype of this is |
CREST syndrome |
|
|
Systemic sclerosis is a condition of |
unknown cause characterised by hardened, sclerotic skin and other connective tissues |
|
|
There are three patterns of disease: |
Limited cutaneous systemic sclerosis Diffuse cutaneous systemic sclerosis Scleroderma (without internal organ involvement) |
|
|
Limited cutaneous systemic sclerosis |
Raynaud's may be first sign scleroderma affects face and distal limbs predominately associated with anti-centromere antibodies a subtype of limited systemic sclerosis is: CREST syndrome: Calcinosis, Raynaud's phenomenon, oEsophageal dysmotility, Sclerodactyly, Telangiectasia |
|
|
Diffuse cutaneous systemic sclerosis |
scleroderma affects trunk and proximal limbs predominately associated with scl-70 antibodies hypertension, lung fibrosis and renal involvement seen poor prognosis |
|
|
Scleroderma (without internal organ involvement) |
tightening and fibrosis of skin may be manifest as plaques (morphoea) or linear |
|

scleroderma |

scleroderma |
|
|
Systemic sclerosis InV of antibodies |
ANA positive in 90% RF positive in 30% anti-scl-70 antibodies associated with diffuse cutaneous systemic sclerosis anti-centromere antibodies associated with limited cutaneous systemic sclerosis |
|
|
breakdown CREST |
systemic sclerosis is the umbrella dis - one type (of the 3 types) of this is: Limited cutaneous systemic sclerosis one subtype of this is: - CREST syndrome |
|
|
Slipped upper femoral epiphysis SUUUUUU FAT |
typically an overweight adolescent boy with knee / hip problems |
|
|
You review a 47-year-old woman who was diagnosed with breast cancer two years ago. She has been 'off her legs' since yesterday and cannot walk more than a few steps. What is the most common and early feature of spinal cord compression? Constipation Reduced sensation in the perianal area Back pain Urinary hesitancy Leg weakness |
Back pain |
|
|
Spinal cord compression - whats the EARLIEST AND MOST COMMON SX |
BACK PAIN |
|
|
Spinal cord compression affects what proportion of met cancer pxs |
5% It is more common in patients with lung, breast and prostate cancer |
|
|
Spinal cord compression fxs |
back pain +- worse on lying down and coughing lower limb weakness sensory changes: sensory loss and numbness neurological signs depend on the level of the lesion. |
|
|
Spinal cord compression fxs neurological signs depend on the level of the lesion |
lesion above L1 = usu. UMN lesion below L1 = usu LMN signs in legs and perianal numbness Tendon reflexes tend to be increased below the level of the lesion and absent at the level of the lesion |
|
|
Spinal cord compression mgmt |
high-dose oral dexamethasone urgent oncological assessment for consideration of radiotherapy or surgery |
|
|
You review a 42-year-old woman six weeks following a renal transplant for focal segmental glomerulosclerosis. Following the procedure she was discharged on a combination of tacrolimus, mycophenolate, and prednisolone. She has now presented with a five day history of feeling generally unwell with anorexia, fatigue and arthralgia. On examination her sclera are jaundiced and she has widespread lymphadenopathy with hepatomegaly. What is the most likely diagnosis? |
Cytomegalovirus |
|
|
Cytomegalovirus is the most common and important viral infection in |
solid organ transplant recipients |
|
|
A woman who is 8 weeks pregnant presents with abdominal pain and vaginal bleeding. On examination she is tender in the right iliac fossa and suprapubic region. Speculum examination shows an open cervical os. Ultrasound confirms an intrauterine pregnancy. |
This lady is likely to be having an inevitable miscarriage. |
|
|
A woman who is 33 weeks pregnant presents with vaginal bleeding, which she describes as being like a period. She also has constant, lower abdominal pain. On assessment her blood pressure is 90/60 mmHg and pulse is 110/min |
Placental abruption |
|
|
Placental praevia would not usually present with abdominal pain. |
true |
|
|
A woman who is 22 weeks pregnant presents with abdominal pain on the right side of her abdomen. On examination she has abdominal tenderness on the right side and urine dipstick is normal. White blood cells are raised at 18.5 * 109/l |
Appendicitis nb Ovarian torsion should be considered but would not normally be associated with such a leucocytosis. |
|
|
whatis the single most important cause of abdominal pain to exclude in early pregnancy |
ectopic preg |
|
|
ectopic preg Risk factors (anything slowing the ovum's passage to the uterus) |
damage to tubes (salpingitis, surgery) previous ectopic IVF (3% of pregnancies are ectopic) |
|
|
A typical history is a female with a history of 6-8 weeks amenorrhoea who presents with lower abdominal pain and later develops vaginal bleeding describes |
ectopic preg |
|
|
Abdominal pain early in pregnancy - causes |
ectopic preg miscarriage |
|
|
Abdominal pain later in pregnancy - causes |
labour placental abruption symphysis pubis dysf pre-eclampsia/HELLP syndrome uterine rupture |
|
|
abdo pain at any point in preg - cause |
appendicities UTI |
|
|
labour fxs |
Regular tightening of the abdomen which may be painful in the later stages |
|
|
placental abruption separation of placenta from the uterine wall, resulting in maternal haemorrhage into the intervening space |
shock out of keeping with visible loss pain constant tender, tense uterus normal lie and presentation fetal heart: absent/distressed coagulation problems beware pre-eclampsia, DIC, anuria |
|
|
Symphysis pubis dysfunction |
Ligament laxity increases in response to hormonal changes of pregnancy Pain over the pubic symphysis with radiation to the groins and the medial aspects of the thighs. A waddling gait may be seen |
|
|
Pre-eclampsia/HELLP syndrome |
Associated with hypertension, proteinuria. Patients with HELLP also have haemolysis, elevated liver enzymes and a low platelet count. The pain is typically epigastric or in the RUQ |
|
|
Uterine rupture |
Ruptures usually occur during labour but occur in third trimester Risk factors: previous caesarean section Presents with maternal shock, abdominal pain and vaginal bleeding to varying degree |
|
|
key FX FOR UTERINE RUPTURE remember it has the usu. abo pain, mum shock, and bleeding |
PREVIOUS C SXN
LATE IN PREG. |
|
|
UTI during preg is assoc with |
increased risk of pre-term delivery and IUGR 4% incidence |
|
|
whats themost common non-obstetric surgical emergency in preg |
appendicitis Higher morbidity and mortality in pregnancy |
|
|
An 80-year-old gentleman on a care of the elderly ward has developed diarrhoea. Stool samples have isolatedClostridium difficile. The patient has been moved to a side room and is being barrier nursed. Which is the most likely medication contributing to his diarrhoea? Clindamycin Gentamicin Vancomycin Clarithromycin Rifampicin |
Clindamycin |
|
|
Clostridium difficile is a gram positive, spore forming anaerobic bacterium which can cause |
colitis in susceptible individuals. |
|
|
Although any antibiotic can contribute to Clostridium difficile diarrhoea, which ones are the main culprits |
broad spectrum antibiotics (for example clindamycin, cephalosporins, penicillins and fluoroquinolones) |
|
|
broad spectrum antibiotics (for example clindamycin, cephalosporins, penicillins and fluoroquinolones) are the main contributing medications disrupting the normal bowel flora, and enabling |
clostridium difficile overgrowth |
|
|
define broad spec antibiotics |
acts against both gram +ve and -ve bact |
|
|
empirically def |
(i.e., based on the experience of the practitioner), prior to the formal identification of the causative bacteria, when there is a wide range of possible illnesses and a potentially serious illness would result if treatment is delayed |
|
|
broad spectrum antibiotics for example |
clindamycin, cephalosporins, penicillins and fluoroquinolones |
|
|
Vancomycin is frequently used in the treatment of clostridium difficile diarrhoea, along with metronidazole. |
true give orally |
|
|
Proton pump inhibitors (for example omeprazole, lansoprazole) are another group of medications thought to contribute to clostridium difficile diarrhoea. |
true |
|
|
c. diffproduces an exotoxin which causes intestinal damage leading to a syndrome called |
pseudomembranous colitis |
|
|
whats the most common cause of c diff assoc with antibiotic use |
Second and third generation cephalosporins are now the leading cause of Clostridium difficile. |
|
|
dx of c diff |
stool sample = detecting Clostridium difficile toxin (CDT) |
|
|
first line tx for c diff |
oral metronidazole for 10-14 days unresponsive = try oral vanc if life threatening you can use both = IV met and oral van |
|
|
A 53-year-old man presents complaining of an itchy scalp and dandruff. On examination he is noted to have eczema on his scalp, behind his ears and around his nose. He has tried 'Head and Shoulders' and 'Neutrogen T-gel' but with poor results. Which one of the following is the most appropriate treatment for his scalp? |

topical ketoconazole |
|
|
Seborrhoeic dermatitis in adults aka dandruff mgmt - 1st line |
over the counter preparations containing zinc pyrithione ('Head & Shoulders') and tar ('Neutrogena T/Gel') are first-line |
|
|
Seborrhoeic dermatitis in adultsaka dandruff mgmt - 2nd line |
Topical ketoconazole nb selenium sulphide and topical corticosteroid may also be useful |
|
|
Seborrhoeic dermatitis in adults |
is a chronic dermatitis thought to be caused by an inflammatory reaction related to a proliferation of a normal skin inhabitant, a fungus called Malassezia furfur (formerly known as Pityrosporum ovale) |
|
|
Seborrhoeic dermatitis thought to be caused by |
malassezie furfur = fungus |
|
|
Seborrhoeic dermatitis in adults fxs |
eczematous lesions on the sebum-rich areas: scalp (may cause dandruff), periorbital, auricular and nasolabial folds otitis externa and blepharitis may develop |
|
|
Seborrhoeic dermatitis in adults Associated conditions include |
HIV Parkinson's disease |
|
|
Face and body management |
topical antifungals: e.g. Ketoconazole topical steroids: best used for short periods difficult to treat - recurrences are common |
|
|
You see a 6 week-old baby boy for his routine baby check. You are unable to palpate the right testicle on examination, though the left is present. What should you do? |
Watch and wait |
|
|
Undescended testicles is a common finding on |
examination of the newborn |
|
|
Undescended testicles is a common finding on examination of the newborn so what should you do if you dont find it |
Try to 'milk' the testis down the inguinal canal - if it can be brought in to the scrotum it is retractile rather than undescended |
|
|
undescended testis is common in newborn examination, it will usu. descend by |
6 months of age so arrange r/v towards end of their first year |
|
|
if px has undescended still by 1yo - whats the mgmt |
orchidopexy |
|
|
Bilateral impalpable testes at birth should raise suspicions of problems such as |
congenital adrenal hyperplasia and urgent paediatric review should be sought. |
|
|
Undescended testis fxs |
occurs in around 2-4% of term male infants., but is much more common if the baby is preterm. Around 25% of cases are bilateral |
|
|
Complications of undescended testis |
infertility torsion testicular cancer psychological |
|
|
Management of undescended testis |
orchidopexy: referral should be considered from around 6 months of age. Surgical practices vary although the majority of procedures are performed at around 1 year of age |
|

dx |
Lentigo maligna The asymmetrical nature of the lesion would however point away from a diagnosis of solar lentigo |
|

Lentigo maligna |

Lentigo maligna |
|

Dermatofibroma |

Dermatofibroma |
|

Dermatofibroma |

downlaod |
|
Solar lentigo |

Solar lentigo |
|

Solar lentigo |

Solar lentigo |
|

Solar lentigo |

Solar lentigo |
|

Bowen's disease |

Bowen's disease |
|

Bowen's disease |

Bowen's disease |
|

Bowen's disease |

Bowen's disease |
|
|
Lentigo maligna |
Lentigo maligna is a type of melanoma in-situ. It typically progresses slowly but may at some stage become invasive causing lentigo maligna melanoma. |
|
|
A 66-year-old woman presents to her GP with a 2 month history of abdominal bloating, early satiety, urinary urgency and symptoms of both constipation and diarrhoea. She has never experienced this before and has no past medical history. Her only family history is of breast cancer, of which both her mother and sister died. Abdominal examination is unremarkable. What is the next step in her management? |
Measure CA-125 |
|
|
The National Institute for Health and Care Excellence (NICE) recommends that women with symptoms of ovarian cancer, especially if over 50 years, should have tests in primary care. NICE defines symptoms as: |
persistent abdominal distension (bloating) early satiety or loss of appetite pelvic/abdominal pain increased urinary frequency and/or urgency |
|
|
if px has abdo bloating, early satiety, urinary urgency and constipation and diarrhoea with fhx of breast cancer of mother and sister abdo exam normal - what next step in mgmt |
Measure CA-125 |
|
|
so if px has sxs suggestive of ovary cancer + fhx, but exam normal, next |
Measure CA-125 if this is elevated next do: - US abdo & pelvis next if suggestive of ovarian cancer: - 2 week wait referral to gynaecology should be made |
|
|
so if px has sxs suggestive of ovary cancer + fhx, but exam shows ascites and palpable mass mgmt |
2 week wait referral to gynaecology should be made |
|
|
Ovarian cancer is the fifth |
most common malignancy in females. |
|
|
Around 90% of ovarian cancers are |
epithelial in origin. |
|
|
Ovarian cancer prognosis |
generally poor due to late dx |
|
|
Ovarian cancer risk factors |
fhx: mutations of the BRCA1 or the BRCA2 gene many ovulations: early menarche, late menopause, nulliparity |
|
|
Ovarian cancer Clinical features are notoriously vague |
abdominal distension and bloating abdominal and pelvic pain urinary symptoms e.g. Urgency early satiety diarrhoea |
|
|
ovarian cancer dx |
Diagnosis is difficult and usually involves diagnostic laparotomy |
|
|
A 19-year-old man presents with a compound fracture of his leg following a fall from scaffolding. Examination reveals soiling of the wound with mud. He is sure he has had five previous tetanus vaccinations. What is the most appropriate course of action to prevent the development of tetanus? |
Clean wound + intramuscular human tetanus immunoglobulin |
|
|
px has compound #, gets dirty, they've had tetanus vaccine in past - mgmt |
Clean wound + intramuscular human tetanus immunoglobulin +- Abx |
|
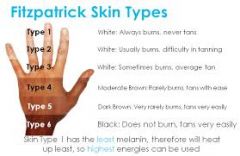
fitzpatrick skin type classfication |
goes form white to darker |
|
|
A 17 year old male presents with a new skin condition which his mum noticed when they were on holiday in Spain. On examination, he has skin type V, with multiple small patches of depigmentation to the upper back. The patches appear mildly flaky but they are asymptomatic. He is usually well, and has never had this condition before. Which of the following is the most likely diagnosis? |
Pityriasis versicolor |
|

Pityriasis versicolor |

Pityriasis versicolor |
|

Pityriasis versicolor |

Pityriasis versicolor |
|

Guttate psoriasis |

Guttate psoriasis |
|

Guttate psoriasis |

Guttate psoriasis |
|

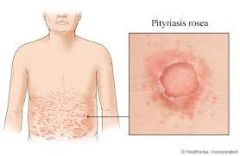
pityriasis rosea |

pityriasis rosea |
|

pityriasis rosea |

pityriasis rosea |
|

pityriasis rosea |
pityriasis rosea |
|
|
Pityriasis versicolor, also called |
tinea versicolor, is a superficial cutaneous fungal infection caused by Malassezia furfur (formerly termed Pityrosporum ovale) |
|
|
Pityriasis versicolor mgmt |
topical antifungal if extensive disease or failure to respond to topical treatment then consider oral itraconazole |
|
|
CURB65 what are the values |
ALL 1 POINT Blood pressure less than 90 mmHg systolic or diastolic blood pressure 60 mmHg or less |
|
|
A 37 year old women presents to you in general practice. She has a one year history of right wrist pain. The pain is exacerbated by flexion and she rates it as 7 on the pain score. She has trialled pain medication with no great success. On examination there is no evidence of synovitis. A small effusion is present in the right wrist. Onycholysis is noted. There is purple plaques present over the extensor surfaces of the elbows bilaterally. What is the clinical diagnosis? |
Psoriatic arthritis |
|
|
Psoriatic arthritis strong associations with |
psoriasis. remember it affects DIP and has sausage fingers |
|
|
Psoriatic arthropathy MGMT |
tx same as RA BUT BETTER PROGNOSIS |
|
|
a preg post term occurs when |
42 weeks Postmaturity is the condition of a baby that has not yet been born after 42 weeks of gestation, two weeks beyond the normal 40 |
|

A 60-year-old man asks you to have a look at a 'sore' on his right ear. It has been present for around 6 months and is not painful. What is the most likely diagnosis? |
Actinic keratosis |
|
|
Actinic, or solar, keratoses (AK) is a common |
premalignant skin lesion that develops as a consequence of chronic sun exposure |
|
|
actinic keratoses fxs |
small, crusty or scaly, lesions may be pink, red, brown or the same colour as the skin typically on sun-exposed areas e.g. temples of head multiple lesions may be present |
|
|
Actinic keratosesManagement options include |
prevention - sun avoidance/cream fluorouracil cream: typically a 2 to 3 week course. The skin will become red and inflamed - sometimes topical hydrocortisone is given following fluorouracil to help settle the inflammation topical diclofenac: may be used for mild AKs. Moderate efficacy but much fewer side-effects topical imiquimod: trials have shown good efficacy cryotherapy curettage and cautery |
|
|
Which one of the following statements regarding hepatitis A is false? |
It is a DNA virus |
|
|
true facts about hep A |
Has an incubation period of 2-4 weeks Doesn't cause chronic hepatitis May cause hepatosplenomegaly A vaccine is available RNA picornavirus |
|
|
are there any complications of hep A |
RARE NO HEP CANCER |
|
|
A 33-year-old woman visits her general practitioner complaining of inability to conceive after two years of trying with a regular partner. She has a body mass index of 28 kg/m² and an existing diagnosis of polycystic ovarian syndrome. Which of the following drugs is most likely to help restore normal ovulation in this case? |
Metformin |
|
|
first line tx for PCOS pxs struggling to conceive |
lose weight |
|
|
if PCOS px fails to lose weight for trying to conceive - next tx |
metformin nb Thyroxine might help a hypothyroid patient conceive |
|

dx |
Black hairy tongue Black hairy tongue is relatively common condition which results from defective desquamation of the filiform papillae. Despite the name the tongue may be brown, green, pink or another colour. Predisposing factors poor oral hygiene antibiotics head and neck radiation HIV intravenous drug use The tongue should be swabbed to exclude Candida Management tongue scraping topical antifungals if Candida |
|
|
first line tx for tinea pedis aka athletes foot |
topical imidazole, undecenoate, or terbinafine first-line |
|
|
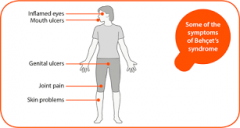
A 27-year-old woman presents with painful genital ulceration. She has had recurrent attacks for the past four years. Oral aciclovir has had little effect on the duration of her symptoms. She has also noticed for the past year almost weekly attacks of mouth ulcers which again are slow to heal. Her only past medical history of note is being treated for thrombophlebitis two years ago. What is the most likely diagnosis? |
Behcet's syndrome |
|
|
Behcet's syndrome |
|
|
Behcet's syndrome is a complex multisystem disorder associated with presumed |
autoimmune mediated inflammation of the arteries and veins actual cause unknown |
|
|
Behcet's syndrome classic triad |
oral ulcers, genital ulcers and anterior uveitis +- thrombophlebitis |
|
|
Behcet's syndrome epi |
tends to affect young men 30% +ve fhx associated with HLA B5* and MICA6 allele |
|
|
Behcet's syndrome fxs |
classically: 1) oral ulcers 2) genital ulcers 3) anterior uveitis thrombophlebitis arthritis neurological involvement (e.g. aseptic meningitis) GI: abdo pain, diarrhoea, colitis erythema nodosum, DVT |
|
|
Behcet's syndrome dx |
no definitive test diagnosis based on clinical findings positive pathergy test is suggestive (puncture site following needle prick becomes inflamed with small pustule forming) |
|
|
What is the most common identified trigger of anaphylaxis in children? |
food |
|
|
A woman presents to her GP complaining of bleeding after sexual intercourse. What is the most common identifiable cause of postcoital bleeding? |
Cervical ectropion |
|
|
Cervical ectropion is the most common identifiable cause of postcoital bleeding |
true |
|
|
Cervical ectropion |
(or cervical eversion) is a condition in which the central (endocervical) columnar epithelium protrudes out through the external os of the cervix and onto the vaginal portion of the cervix, undergoes squamous metaplasia, and transforms to stratified squamous epithelium. |
|
|
Postcoital bleeding causes |
no identifiable pathology is found in around 50% of cases cervical ectropion is the most common identifiable causes, causing around 33% of cases. This is more common in women on the combined oral contraceptive pill cervicitis e.g. secondary to Chlamydia cervical cancer polyps trauma |
|
|
A 42-year-old woman is admitted to hospital with pyrexia and a productive cough. Around 10 days ago she developed symptoms consistent with a flu-like illness. For around 4-5 days she was in bed with myalgia, fever and lethargy. Initially there was an improvement in her condition but over the past three days she has developed a cough productive of thick pink-yellow sputum. On examination there are scattered crackles in the right base. A chest x-ray confirms pneumonia. Which one of the following organisms is more common in patients who have recently had influenza? |
Staphylococcus aureus |
|
|
There is a high incidence of Staphylococcus aureus pneumonia in patients following |
influenza |
|
|
whats the most common cause of CAP |
strep pneumonia 80% |
|
|
if a px with a flu then gets CAP whats the likely cause |
STAPH AUREUS |
|
|
herpes labialis |
(also called cold sores, fever blisters, herpes simplex labialis, recurrent herpes labialis, or orolabial herpes) : is a type ofherpes simplex occurring on the lip, i.e. an infection caused by herpes simplex virus (HSV). An outbreak typically causes small blisters or sores on or around the mouth. |
|
|
Characteristic features of pneumococcal pneumonia |
rapid onset high fever pleuritic chest pain herpes labialis |
|
|
low or moderate severity CAP mgmt |
oral amoxicillin outpx +macrolide if admitted |
|
|
high severity CAP |
intravenous co-amoxiclav + clarithromycin OR cefuroxime + clarithromycin OR cefotaxime + clarithromycin |
|
|
Skin disorders affecting the soles of the feet |
Verrucas Tinea pedis Corn and calluses Keratoderma Pitted keratolysis Palmoplantar pustulosis Juvenile plantar dermatosis |
|
|
What is the single most useful test for determining the cause of her hypercalcaemia? |
Parathyroid hormone |
|
|
The most common causes of hypercalcaemia are |
malignancy (bone metastases, myeloma, PTHrP from squamous cell lung cancer) and primary hyperparathyroidism |
|
|
other causes of hypercalcemia include |
sarcoidosis* vitamin D intoxication acromegaly thyrotoxicosis Milk-alkali syndrome drugs: thiazides, calcium containing antacids dehydration Addison's disease Paget's disease of the bone** |
|
|
A 21-year-old female presents for review. She is 14 weeks pregnant and has been seen by the midwives for her booking visit. There have been no pregnancy related problems to date. Tests taken revealed the following:Blood group:A Rhesus negative What is the most appropriate management regarding her rhesus status? |
Give first dose of anti-D at 28 weeks |
|
|
Rhesus negative woman rule |
anti-D at 28 + 34 weeks |
|
|
A 2-month-old girl is brought in by her mother. She was breastfed for the first two weeks of life before being switched to formula. For the past six weeks she has experienced a number of problems including regurgitation, vomiting, diarrhoea and eczema. Despite these problems she has kept to the 50th centile for weight. Clinical examination is unremarkable other than some dry skin on her torso. What is the most likely diagnosis? |
Cow's milk protein intolerance |
|
|
The emergence of symptoms following the introduction of formula is very suggestive of |
cow's milk protein intolerance. |
|
|
Cow's milk protein intolerance/allergy dx |
often clinical (e.g. improvement with cow's milk protein elimination). Investigations include: skin prick/patch testing total IgE and specific IgE (RAST) for cow's milk protein |
|
|
Cow's milk protein intolerance/allergy |
severe = peds referral Management if formula-fed extensive hydrolysed formula (eHF) milk is the first-line replacement formula for infants with mild-moderate symptomsamino acid-based formula (AAF) in infants with severe CMPA or if no response to eHFaround 10% of infants are also intolerant to soya milk Management if breast-fed continue breastfeedingeliminate cow's milk protein from maternal dietuse eHF milk when breastfeeding stops, until 12 months of age and at least for 6 months |
|
|
A primiparous 31 year-old women who is at 14 weeks gestation has a cardiac arrest. What is the most likely cause of cardiac arrest in early pregnancy? |
Ruptured ectopic pregnancy |
|
|
What is the most likely cause of cardiac arrest in early pregnancy? |
Ruptured ectopic pregnancy causing hypovolemia |
|
|
Ectopic pregnancy |
Implantation of a fertilized ovum outside the uterus results in an ectopic pregnancy |
|
|
Ectopic pregnancyRisk factors (anything slowing the ovum's passage to the uterus) |
damage to tubes (salpingitis, surgery) previous ectopic endometriosis IUCD progesterone only pill IVF (3% of pregnancies are ectopic) |
|
|
You review a 47-year-old man one year after he was diagnosed with prediabetes. Last year he had a HbA1c taken after being diagnosed as having hypertension. This was recorded as being 43 mmol/mol (6.1%). His most recent blood test is recorded as being 45 mmol/mol (6.3%) despite the patient reporting that he has changed his diet as instructed and exercising three times a week. His body mass index (BMI) today is 26.5 kg/m². Last year it was 27.5kg/m². What is the most appropriate course of action? |
Start metformin |
|
|
start metformin, even in pxs who are likely to get DM2 |
DESPITE lifestyle changes |
|
|
which one of the following variables is not required by the Modification of Diet in Renal Disease (MDRD) equation? |
Serum urea |
|
|
eGFR variables |
CAGE - Creatinine, Age, Gender, Ethnicity |
|
|
Serum creatinine may not provide an accurate estimate of renal function due to differences in muscle. |
For this reason formulas were develop to help estimate the glomerular filtration rate namely estimated GFR or eGFR |
|
|
The most commonly used formula is the Modification of Diet in Renal Disease (MDRD) equation, for measuring eGFR which uses the following variables: |
CAGE Factors which may affect the result pregnancy muscle mass (e.g. amputees, body-builders) eating red meat 12 hours prior to the sample being taken |
|
|
CKD may be classified according to GFR: |
its in other cards |
|
|
A 2-year-old girl develops a rash on her legs. The next day she is brought to surgery, by which time the rash has spread to the rest of her body. dx |

Erythema multiforme |
|
|
Erythema multiforme Features |
target lesions initially seen on the back of the hands / feet before spreading to the torso upper limbs are more commonly affected than the lower limbs pruritus is occasionally seen and is usually mild |
|
|
Erythema multiforme causes |
viruses: herpes simplex virus (the most common cause), Orf* idiopathic bacteria: Mycoplasma, Streptococcus drugs: penicillin, sulphonamides, carbamazepine, allopurinol, NSAIDs, oral contraceptive pill, nevirapine connective tissue disease e.g. Systemic lupus erythematosus sarcoidosis malignancy |
|
|
Polymorphic eruption of pregnancy is not associated with blistering |
Pemphigoid gestationis does have blisters |
|
|
Polymorphic eruption of pregnancy is not associated with blistering |
Pemphigoid gestationis does have blisters |
|
|
A 30-year-old female in her third trimester of pregnancy mentions during an antenatal appointment that she has noticed an itchy rash around her umbilicus. This is her second pregnancy and she had no similar problems in her first pregnancy. Examination reveals blistering lesions in the peri-umbilical region and on her arms. What is the likely diagnosis? |
Pemphigoid gestationis |
|
|
A 38 year old man presents with a sudden onset rash. He is otherwise well in himself and has no notable past medical history. You see from his notes he has had a recent tonsillitis for which he received amoxicillin. On examination, there are multiple papules on his trunk and proximal extremities. There is a fine scale on several of these lesions. What is the most likely diagnosis? |
Guttate psoriasis |
|
|
Polymorphic eruption of pregnancy is not associated with blistering |
Pemphigoid gestationis does have blisters |
|
|
A 30-year-old female in her third trimester of pregnancy mentions during an antenatal appointment that she has noticed an itchy rash around her umbilicus. This is her second pregnancy and she had no similar problems in her first pregnancy. Examination reveals blistering lesions in the peri-umbilical region and on her arms. What is the likely diagnosis? |
Pemphigoid gestationis |
|
|
A 38 year old man presents with a sudden onset rash. He is otherwise well in himself and has no notable past medical history. You see from his notes he has had a recent tonsillitis for which he received amoxicillin. On examination, there are multiple papules on his trunk and proximal extremities. There is a fine scale on several of these lesions. What is the most likely diagnosis? |
Guttate psoriasis |
|
|
It can occur as the first presentation of psoriasis or as an acute exacerbation of plaque psoriasis, particularly after acute streptococcal infection (usually of the throat) or viral infection.
Which condition is this |
Guttate psoriasis |
|
|
violaceous border suggests |
Pyoderma gangrenosum |
|
|
A 62-year-old female is referred to dermatology by her GP due to a lesion over her shin. It initially started as a small red papule which later became a deep, red, necrotic ulcer with a violaceous border. What is the likely diagnosis? |
Pyoderma gangrenosum |
|
|
The differential diagnosis of shin lesions includes the following conditions: |
erythema nodosum pretibial myxoedema pyoderma gangrenosum necrobiosis lipoidica diabeticorum |
|
|
The differential diagnosis of shin lesions includes the following conditions: |
erythema nodosum pretibial myxoedema pyoderma gangrenosum necrobiosis lipoidica diabeticorum |
|
|
On examination the lesions are consistent with erythema nodosum. You arrange some baseline investigations. What is the most appropriate management? |
No active treatment, arrange routine follow-up |
|
|
Erythema nodosum is inflammation of the |
Subcut fat
typically causes tender, erythematous, nodular lesions usually occurs over shins, may also occur elsewhere (e.g. forearms, thighs)
usually resolves within 6 weeks lesions heal without scarring |
|
|
Erythema nodosum causes |
infection: streptococci, TB, brucellosis systemic disease: sarcoidosis, inflammatory bowel disease, Behcet's malignancy/lymphoma drugs: penicillins, sulphonamides, combined oral contraceptive pill pregnancy |
|
|
A 19-year-old female who has just started work as a cleaner presents with a rash on her hands. On examination there is a generalised erythematous rash on the dorsum of both hands. There is no evidence of scaling or vesicles. What is the most likely diagnosis? |
Irritant contact dermatitis |
|
|
2 types of contact dermatitis |
Irritant and allergic |
|
|
2 types of contact dermatitis |
Irritant and allergic |
|
|
Irritant dermatitis |
The strong alkalis and acids found in cleaning solutions are common triggers of irritant contact dermatitis |
|
|
Allergic contact dermatitis |
often seen on the head following hair dyes. Presents as an acute weeping eczema which predominately affects the margins of the hairline rather than the hairy scalp itself. Topical treatment with a potent steroid is indicated |
|
|
Reactive arthritis skin manifestations |
skin:
circinate balanitis (painless vesicles on the coronal margin of the prepuce),
keratoderma blenorrhagica (waxy yellow/brown papules on palms and soles) |
|
|
A 45-year-old woman presents for review. She has noticed a number of patches of 'pale skin' on her hands over the past few weeks. The patient has tried using an emollient and topical hydrocortisone with no result. On examination you note a number of hypopigmented patches on the dorsum of both hands. Her past medical history includes thyrotoxicosis for which she takes carbimazole and thyroxine. What is the most likely causes of her symptoms? |
Vitiligo |
|
|
Reactive arthritis skin manifestations |
skin:
circinate balanitis (painless vesicles on the coronal margin of the prepuce),
keratoderma blenorrhagica (waxy yellow/brown papules on palms and soles) |
|
|
A 45-year-old woman presents for review. She has noticed a number of patches of 'pale skin' on her hands over the past few weeks. The patient has tried using an emollient and topical hydrocortisone with no result. On examination you note a number of hypopigmented patches on the dorsum of both hands. Her past medical history includes thyrotoxicosis for which she takes carbimazole and thyroxine. What is the most likely causes of her symptoms? |
Vitiligo |
|
|
Which one of the following medications is most likely to have exacerbated his psoriasis? |
Atenolol |
|
|
The following factors may exacerbate psoriasis: |
trauma alcohol drugs: beta blockers, lithium, antimalarials (chloroquine and hydroxychloroquine), NSAIDs and ACE inhibitors, infliximab
withdrawal of systemic steroids |
|
|
The following factors may exacerbate psoriasis: |
trauma alcohol
drugs: beta blockers, lithium, antimalarials (chloroquine and hydroxychloroquine), NSAIDs and ACE inhibitors, infliximab
withdrawal of systemic steroids |
|
|
The following factors may exacerbate psoriasis: |
trauma alcohol
drugs: beta blockers, lithium, antimalarials (chloroquine and hydroxychloroquine), NSAIDs and ACE inhibitors, infliximab
withdrawal of systemic steroids |
|
|
A diagnosis of pityriasis versicolor is suspected. Which one of the following is the most appropriate treatment? |
Topical ketoconazole |
|
|
Pityriasis versicolor, also called tinea versicolor, is a |
superficial cutaneous fungal infection caused by Malassezia furfur (formerly termed Pityrosporum ovale) |
|
|
Pityriasis versicolor, also called tinea versicolor, is a caused by a |
Fungis
Just remember its tinea versicolor
So tx is topical ketoconazole |
|
|
A 32 year old lady attends with a facial rash for several weeks. She has an erythematous rash which looks greasy and has a fine scale over her face affecting her cheeks, naso-labial folds, eye brows, nasal bridge and scalp. What is the most likely diagnosis? |
Seborrhoeic dermatitis |
|
|
Acne rosecea vs Seborrhoeic dermatitis |
involvement of the naso-labial folds differentiates it from acne rosacea which typically spares this area and tends to include telangiectasia and pustules. |
|
|
Acne rosecea vs Seborrhoeic dermatitis |
involvement of the naso-labial folds differentiates it from acne rosacea which typically spares this area and tends to include telangiectasia and pustules. |