Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
500 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
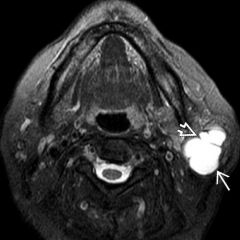
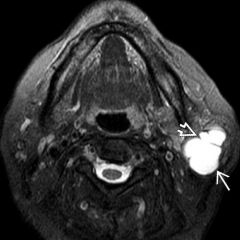
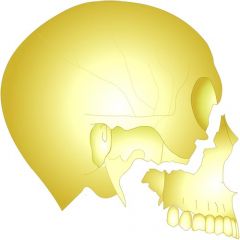
DD lateraler Knieschmerz / iliotibialband friction syndrome
|
Iliotibialband friction syndrome
Large joint effusion distending lateral synovial recess Lateral meniscus tear Lateral meniscus cyst LCL injury |
|
|
|
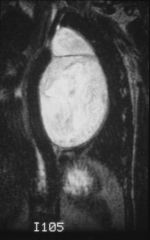
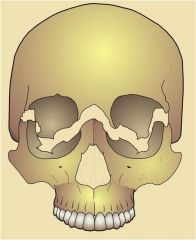
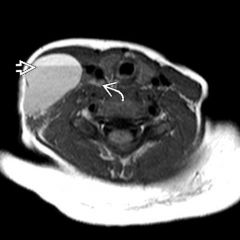
Was ist der natürliche Verlauf eines Hygroms?
|
enlarge
remain reduce change into chronic subduralhematoma (erneute einblutung) ! |
|
|
|
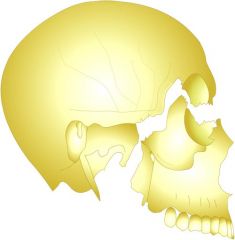
anterior knee pain DD
|
patellar tendonitits (jumpers knee)
osgood schlatter disease (partial avulsion of the tibia tubercle)Sinding-Larsen-Johansson Disease: - Osteochondrosis of the inferior pole of the patella |
|
|

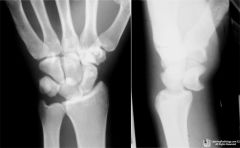
Was ist das für eine Fraktur?
|
Triquetrum Fraktur
|
|
|
|
Triquetral fractures may be associated with of the wrist
|
transcaphoid perilunate dislocations
|
|
|
Was ist das?
|
lunatum dislokation
|
|
|
|
When does the perilunate dislocation ocuur?
|
Occurs when the lunate maintains normal position with respect to the distal radius while all other carpal bones are dislocated posteriorly
|
|
|

Was ist das?
|
perilunate dislocation
|
|
|
|
Perilunate Dislocation is associated with
|
commonly associated with a scaphoid waist fracture auch mit triquetrum fx. capitatum und radial styloid fx.
|
|
|
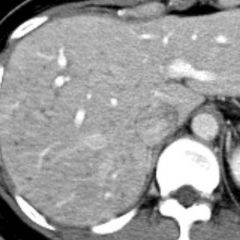
Was ist das?
|
Budd chiari syndrome
|
|
|

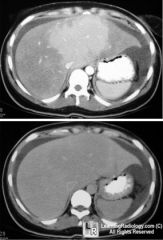
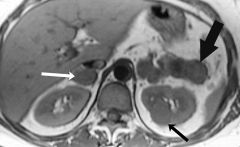
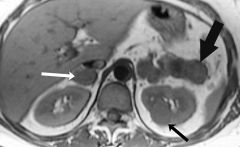
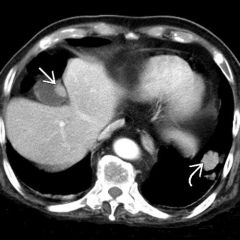
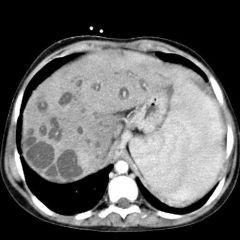
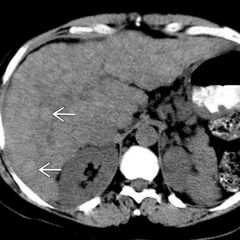
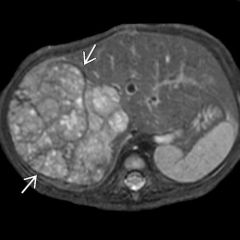
Was ist das?
|
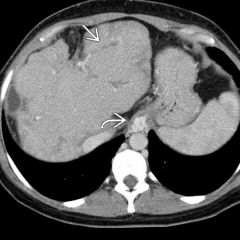
Schistosoma. Axial CT shows signs of portal hypertension, including large varices (white curved) and splenomegaly. Note the extraordinarily widened hepatic fissures deeply dividing the segments of the liver along the portal vein branches. This is a characteristic feature of hepatic schistosomiasis & a distinguishing feature from more common forms of cirrhosis. The appearance of the liver has been described as that of a tortoise shell.
|
|
|
|
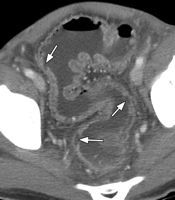
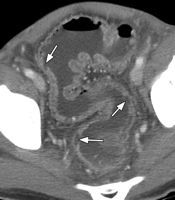
Was sind die Ursachen für eine Mucocele der Appendix?
|
muzinöses Cystadenom
cystadenocarcinoma mucosale Hyperplasie Mukus retentionszyste |
|
|
|
Zu was führt die Ruptur einer Mucocelel der Appendix?
|
pseudomyxoma peritonei
|
|
|
|
Kolonlymphoma most common site?
|
Coecum, lymphombefall des Colons ist selten
|
|
|
|
was ist das budd chiari syndrome
|
chronic hepatic venous occlussive disease, nodular liver comtour from regenerative nodules
|
|
|
|
Wie stellen sich regenerative nodules im T1 dar?
|
hyperintense
|
|
|
|
Häufigste primärkarzinome mit lebermetastsen'
|
Brust kolorektal, Lung
|
|
|
|
Wie sieht confluent hepatic fibrosis aus?
|
wedge shaped hypodense region on ct that extends from the hilum
|
|
|
|
Was ist eine Choledochus anomomaly?
Welche Typen der Choledochus anomaly gibt es? |

Choledochus cyst
1 - 5 |
|
|
|
Choledochus Zyste typ 2
|
common bile duct diverticulum
|
|
|
|
Choledochus Zyste typ 3
|
choledochocele
|
|
|
|
Choledochus Zyste typ 4
|
extrahepatic ductal dilatation
|
|
|
|
Choledochus Zyste typ 5
|
Caroli disease, intrahepatic ductal dilatation
|
|
|
|
Type 1 choledochal cyst
|
most common
cystic or fusiform diatation of the common bile duct |
|
|
|
most common cystic pancreas lesion in children
|
pseudocyst from blunt trauma or pancreatitis
|
|
|
|
most common locations of gi duplication cysts?
|
ileum und esophagus
|
|
|
|
most common cystic ovarian lesions girls younger than 17
|
cystic ovarian teratoma
|
|
|
|
was sind mesenteric cysts?
|
lymphangioma im mesenterium
|
|
|
|
oesophagusvarizen klassifikation
|
uphill downhill
|
|
|
|
Ursache und Charakteristika uphill varizen
|
portale hypertension, häufiger, im distalen oesophagus, gi bleeding,
azygos in vena cava |
|
|
|
downhill varizen
|
bei superior vena cava syndrom im proximalen oesophagus
|
|
|
|
varizen vs. reflux esophagitis
|
reflux sieht gleich aus: thickened tortuous folds, remain fixed in appearance
|
|
|
|
Typen von oesophaguskarzinom
|
infiltrating, polypoid, ulcerative, varicoid
varicoid least common sieht aus wie varizen! dont change appearance |
|
|
|
esophagus lymphoma is
|
rare, when it does meist from contigous spread from gastric cardia or fundus
|
|
|
|
Typisch für achalasie
|
birds peak
|
|
|
|
achalasie definition
|
erkrankung des myenteric plexus results in failure of relaxation of distal sphincter. fehlende peristaltik
|
|
|
|
Ursache achalasie
|
primary degeneration of myenteric plexus
secondary: chagas, fungal, tumor |
|
|
|
scleroderma is a
|
a collagen vascular disease in which smooth cell muscle becomes fibrotic
|
|
|
|
Scleroderma affects ... of the esophagus resulting in
|
distal two thirds, dysmotility and dilatation
|
|
|
|
achalasie vs. scleroderma
|
birds peak vs. dilatation des sphinkters
|
|
|
|
tapered
|
kaegelfärmig, konisch
|
|
|
|
was sind die charakteristika der COP?
|
intraalveolärer Prozess, steroide, lower lobes, patchy and peribronchial consolidations können auch peripher sein
|
|
|
|
BAC presents as
|
ground glass nodule 60%, diffuse or patchy consolidations/ ground glass 40%, pseudocavitation possible,
welll differentiated |
|
|
|
was ist die chronic eosinophilic pneumonia?
|
idiopathic processnalveolar and interstitial infiltration of inflammatory cells, homogene periphere consolidations, sometimes patchy und upper lobe, crazy paving possible, steroids nützen schnell
|
|
|
|
lipoid pneumonia characteristics
|
lower lobe, kann crazy paving haben, consolidations, chronic process fibrose, necrosis, sogar cavitatons
|
|
|
|
was sind die charakteristika der COP?
|
intraalveolärer Prozess, steroide, lower lobes, patchy and peribronchial consolidations können auch peripher sein
|
|
|
|
BAC presents as
|
ground glass nodule 60%, diffuse or patchy consolidations/ ground glass 40%, pseudocavitation possible,
welll differentiated |
|
|
|
was ist die chronic eosinophilic pneumonia?
|
idiopathic processnalveolar and interstitial infiltration of inflammatory cells, homogene periphere consolidations, sometimes patchy und upper lobe, crazy paving possible, steroids nützen schnell
|
|
|
|
woraus entstehen hepatic cysts?
|
development defect of biliary ducts
|
|
|
|
epatic abscess entsteht meist aus
|
pyogen, ascendierende cholangitis, hematogen oder direkt extension
|
|
|
|
pyogenic abscesses are often
|
multilocular
|
|
|
|
amebic abscesses are often
|
unilocular sonst gleich wie pyogenic (randenhancement)
tendency to rupture |
|
|
|
echinococcal infection can be
|
very large with rimlike calcification, daughter cysts
|
|
|
|
mycotic abscesses are often
|
multiple and small
|
|
|
|
peripheral cholangiocarcinoma are
|
hypodense and enhance late 10min, have capsular retraction due to fibrosis, biliary ductal dilatation peripherally to tumor common
|
|
|
|
biliary cystadenoma are
|
uncommon multilocular well defined masses middle aged women, cyst wall may enhance malignant transformation may occur
|
|
|
|
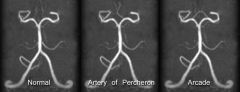
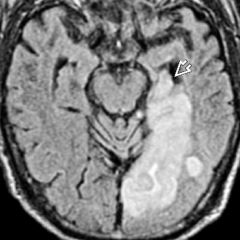
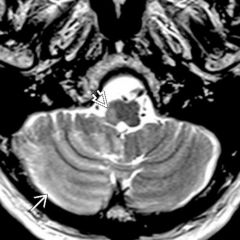
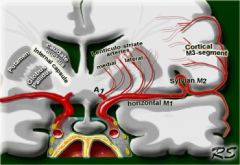
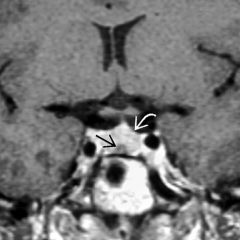
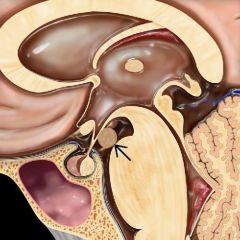
Wie sieht die percheron Arterie aus'
|
|
|
|
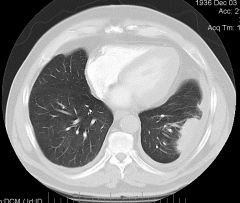
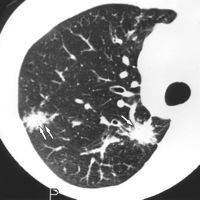
Was ist das?
|
round atelectasis
|
|
|
|
ab wieviel mm sollte ein colonpolyp entfernt werden?
|
10mm
Risiko >20mm 50% >10mm 10% |
|
|
|
Wie gross darf eine rectocele sein?
|
2cm
|
|
|
|
Diverticula are
|
herniations of mucosa and submucosa through the colonic wall.
|
|
|
|
Giant diverticula are most common in the
|
sigmoid up to 25%
|
|
|
|
Aphtoid ulcers are nonspecific finding found in
|
Crohn’s disease
Yersinia Tb Amoebic colitis Ischaemic colitis Behcets disease HIV |
|
|
|
What is the hallmark of IBD?
|
Wall thickening Crohn average 11mm, UC 7mm
|
|
|
|
Wie kommt es zu toxic megacolon?
|
In severe acute colitis, transmural inflammation may result in fulminate colitis with degeneration of the underlying muscle wall leading to colonic dilatation
|
|
|
|
Image characteristics toxic megacolon
|
The colon is dilated, and thick walled, with thickening and effacement of haustral folds, resulting in so called 'thumb-printing'
|
|
|
|
Apthoid ulceration is a non specific finding and may be found in many disorders including:
|
Crohn’s disease
Yersinia Tb Amoebic colitis Ischaemic colitis Behcets disease HIV |
|
|
|
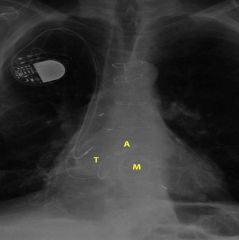
Was ist ein Shaldon katheter?
Wie hoch muss er liegen? |

in der V.cava superior
|
|
|
|
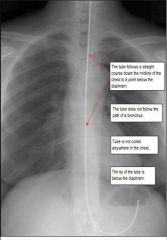
Korrekter Verlauf Magensonde?
|
|
|
|
|
Lage IABP
|

Lage: Spitze 2-3cm nach Abgang der A. subclavia
|
|
|

Was ist das?
|
Intraaortale Ballonpumpe IABP
|
|
|
|
Was heisst IABP
|
Intraaortale Ballonpumpe IABP
|
|
|
|
Herzklappen Lage
|
|
|
|

Welche klappe ist das?
|
mitralklappe
|
|
|

Wie heisst das?
|
Girdlestone
|
|
|
|
Causes of adrenal gland calcifications
|
hemorrhage as a child
Tb or granulomatous disease Neuroblastomas (80% verkalkt) Carcinoma (30% verkalkt) Phaeochromocytoma (10%) |
|
|
|
Small unilateral adrenal masses
|
>3cm
Adenomas Phaeochromocytomas Metastases Tb Myelolipomas |
|
|
|
large unilateral adrenal masses
|
Adrenocorticales karzinom
Phaeochromocytom Ganglioneuroma/ Neuroblastoma Myelolipoma Metastases Abscess |
|
|
|
Cystic adrenal masses
|
revious Hemorrhage
True cysts Mesothalial inclusion Cyst vascular cystic spaces (endothelial lining) lymphangioma paracystic cyst hydatid cyst |
|
|
|
Verteilung Inguinalhernien beim Kind
|
rechts 60%
links 25% beidseits 15% |
|
|
|
Myelolipoma of nnr
|
selten, meist kleiner 5cm kann bis 30cm gross werden.
60 jahre alt Fett und bone marrow elements, kann verkalken 30%, necrosis, |
|
|
|
primary tumors giving rise to nnr metastases are
|
lung breast melanoma kidney, thyroid colon
|
|
|
|
NNR Metastases in T1 und T2
|
T1 hypointens im vergleich zu leber , T2 leicht hyperintens
contain no fat therefore no dropout in out of phase imaging |
|
|
|
lymphoma of nnr
|
primary selten m >60
secondary continous spread from retroperitoneal disease, non hodgkin lymphom, oft bilateral |
|
|
|
wash out adenoma absolute and ratio
|
Has an absolute washout of >60% or relative washout of >40%, it is nearly always an adenoma (specificity 96-100%)
|
|
|
|
Was muss man machen bevor man einen grossen NNR Tumor biopsiert?
|
Before performing a biopsy, the patient must be fully blocked if phaeochromocytoma is metabolically active.
|
|
|
|
Wie gross darf der Böhler Winkel sein?
|
30°
|
|
|
|
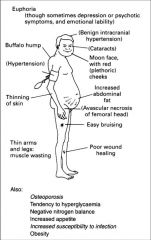
Cushing syndrome klinik
|
|
|
|
|
We kommt es zu Cushing?
|
Excess cortisol secretion due to adrenal hyperplasia in 70% ACTH up
Adrenal adenoma in 20% Adrenal carcinoma in 10% |
|
|
|
Was ist wichtig zu unterscheiden beim Cushing (ursachen)
|
ACTH dependent from independent
|
|
|
|
acth dependent cushing charakteristika
|
adrenal hyperplasia secondary to an elevated ACTH production, usually from a pituitary tumour (70%). In adrenal hyperplasia the adrenal shape is preserved but the limbs of the gland measure more than 1 cm.
|
|
|
|
Ursachen ACTH dependent cushing anders als pituitary?
Woher kommt das ektope ACTH? |
Sources of ectopic ACTH include:
Bronchial carcinoid Pancreatic Islet cell tumour Thymic carcinoid Medullary carcinoma of the thyroid Phaeochromocytoma Small cell lung cancer |
|
|
|
ACTH independent cushing Ursachen
|
The raised cortisol is due to a primary adrenal adenoma or carcinoma in 90% of cases. Other rare causes include primary pigmented nodular adrenal dysplasia or macronodular hyperplasia
|
|
|
|
hyperaldosteronismus conn Ursachen
|
adenoma, selten carcinoma
bilaterale adrenal hyperplasie |
|
|
|
Conn klinik
|
hyperaldosteronismus
It causes hypertension, muscular weakness, and tetany due to hypokalaemia. |
|
|
|
conn zona?
|
glomerulosa
|
|
|
|
conn imaging?
|
adenoma are small <2 cm hypodens <10HU, fast kein enhancement, im mr hypo- or isointense to liver on T2W images
|
|
|
|
was ist die addison disease?
|
primary adrenal insufficiency and occurs when more than 90% of the adrenal cortex is destroyed.
60-70% the cause is an idiopathic auto-immune disorder and the adrenals are atrophic |
|
|
|
other causes of addison?
|
Other causes include:
Granulomatous disease: sarcoidosis or tuberculosis Fungal infections: histoplasmosis, blastomycosis, coccidioidomycosis Adrenal haemorrhage Bilateral metastatic disease (rarely) |
|
|
|
Phaeochromocytom imaging characteristics
|
MR. t1 hypo- iso intense zu leber, T2 hyperintense. inhomogene km anreicherung (necrosis, calcification,
kein signal verlust in in- out of phase imaging ct arteriell deutlich enhancement, venös wie leber inhomogen |
|
|
|
phaeochromocytom charakteristika/klinik
|
selten, 40-60j, bis 2% der ursache hypertension, ca.5cm gross, non specific symptoms including: palpitations, headache, sweating and hypertension
|
|
|
|
Von wo kommt das phaeochromocytom?
|
paraganglion cells within the autonomic nervous system.
|
|
|
|
phaeochromocytom patho definition
|
Kapsel, messen 5-6cm. Rechts doppelt so häufig, Verkalkung in 12%, with haemorrhage in 35% and necrosis in 20-30%.
|
|
|
|
Diagnose klinisch Phaeochromocytom
|
urinary catecholamines and vanillylmandelic acid (VMA) and the diagnosis should be established prior to biopsy.
|
|
|
|
% Regel Phaeochromocytom
|
Phaeochromocytomas arise in the neuroectodermal tissue of the adrenal medulla in 90% of cases and are usually hyperfunctioning. 10% are multiple, 10% associated with neuroectodermal syndromes, and in 25% of sporadic cases there are germ line mutations. 10% are non-functioning and 10% are malignant, especially in tumours greater than 6 cm.
|
|
|
|
Phaeochromocytom extraadrenal sites
|
Extra-adrenal sites:
Sympathetic nerve chain - 46% Organ of Zuckerkandl - 29% Aortic and carotid chemoreceptors - 3% Bladder - 10% Chest - 10% Head and neck - 2-4% |
|
|
|
phaeochromocytoma extraadrenal associated with
|
Tuberose sclerosis
Neurofibromatosis – type 1 von Hippel Lindau disease Carney’s syndrome – pulmonary chondroma /gastric leiomyosarcoma /phaeochromocytoma Multiple endocrine neoplasia 11A (50%) 11B (90%) |
|
|
|
carney syndrome
|
pulmonary chondroma /gastric leiomyosarcoma /phaeochromocytoma
|
|
|
|
adreno cortical carcinoma charakteristika
|
2 peaks <5y und 40-50y
selten, kann nicht von phaeochromocytom unterschieden werden , vor biopsie ausschliessen gefässinvasion |
|
|
|
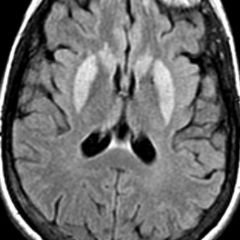
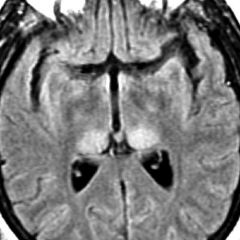
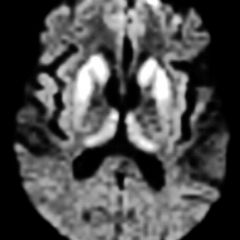
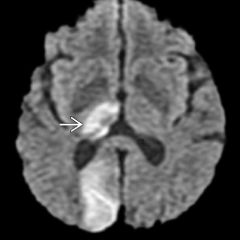
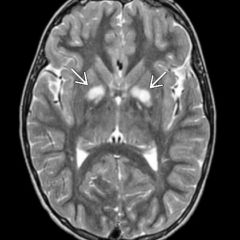
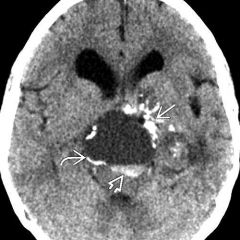
Was ist die percheron artery?
|
which a single dominant thalamoperforating artery supplies the bilateral medial thalami with variable contribution to the rostral midbrain
|
|
|

Was ist das?
|
toxic megacolon
|
|
|
Was ist das?
|
Pseudomembranous colitis
|
|
|
Was ist das?
|

galaxy sign, sarcoidosis
|
|
|
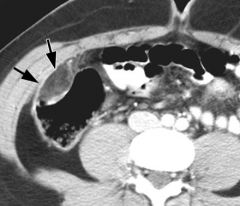
Was ist das? Was sieht man?
|
ulcerative colitis. The wall of the sigmoid is thickened, and hyperemic mesenteric arteries appear as bright dots next to the outer wall of the colon. This indicates active disease.
|
|
|

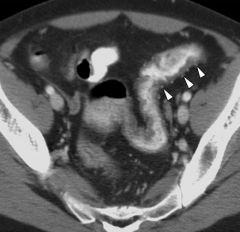
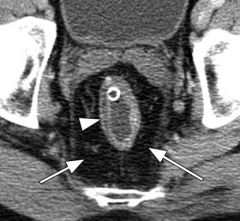
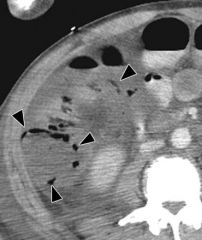
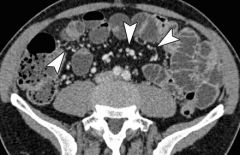
Was ist das? Beschreiben
|
Crohn disease (granulomatous ileocolitis) shows thickening of the ileocecal tip (arrows) and marked thickening of the terminal ileum (arrowheads). The ileocecal valve is stenosed, as demonstrated by succus in the lumen and prestenotic dilatation.
|
|
|
Was ist das? Beschrieb
|
chronic ulcerative colitis. Thickened rectal wall demonstrates the fat halo sign (arrowhead). Perirectal fat (arrows) is increased.
|
|
|
Was ist das? Wie heisst das? Beschrieb?
|
ulcerative colitis and bloody diarrhea demonstrates the double halo, or target, sign with inner (mucosa, arrow) and outer (muscularis propria, arrowhead) rings of high attenuation separated by a ring of low attenuation, which represents submucosa with edema. Little if any pericolonic stranding is seen.
|
|
|

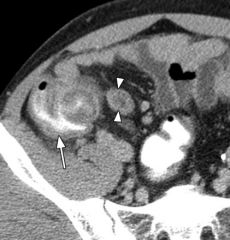
Was ist das? Beschreiben...
|
Crohn ileocolitis shows thickening of terminal ileum and cecum (white arrows) with fibrofatty proliferation (arrowheads) in right lower quadrant. One enlarged lymph node (black arrow) is also depicted.
|
|
|

Was sieht man? DD
|
fistula formation due to tuberculous colitis. Descending colon appears slightly thickened, and a fistulous tract (white arrows) is shown to extend from the colon to an abscess (black arrow) in the left psoas muscle and through the left paraspinal muscles into the subcutaneous tissue of the back, where another abscess (arrowheads) has formed.
|
|
|

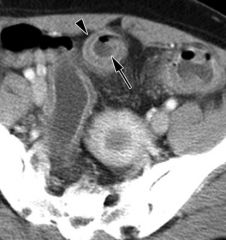
Was ist das? Beschreiben
|
31-year-old man with amebiasis who had a history of diarrhea and recent travel to North Africa. (a) Cecal wall is thickened (arrow), but terminal ileum (arrowheads) is not involved. (b) Hepatic flexure (arrows) also demonstrates marked thickening, but descending colon (arrowhead) appears normal.
|
|
|

Was ist das?
|
pseudomembranous colitis who was undergoing antibiotic treatment for sepsis. Extensive wall thickening throughout the colon is evident. The accordion sign (arrows) is seen in the transverse colon, and ascites (arrowheads) is also noted.
|
|
|

was ist das? DD, beschreiben
|
transplantation patient with neutropenic colitis shows marked wall thickening in ascending colon (arrow) associated with pericolonic stranding and ascites (arrowheads).
|
|
|

was ist das? beschreiben
|
ischemic colitis due to arrhythmia shows ascites and marked thickening of sigmoid colon associated with multiple large nodular defects, which are the CT analog of thumbprinting (arrows) on radiographs. Note that rectal wall (arrowheads) is normal.
|
|
|

was ist das? Speziell?
|
ischemic colitis after blunt abdominal trauma to right flank demonstrates marked thickening of hepatic flexure and right colon, with abrupt transition (arrows) between abnormal and normal wall in the transverse colon.
|
|
|
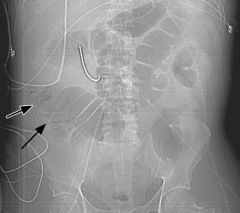
was sieht man? diagnose?
|
ischemic colitis (a) Anteroposterior CT scout view shows air (arrows) in wall of right colon and small- and large-bowel dilatation. (b) Transverse CT image demonstrates air (arrowheads) in wall of right colon, with lack of wall enhancement and pericolonic stranding indicative of infarction.
|
|
|
was ist das? Diagnose?
|
25-year-old man with epiploic appendagitis and right upper quadrant pain shows ovoid fatty mass with enhancing rim (arrows) and increased attenuation. Colonic wall is not thickened.
|
|
|

Diagnose?
|
67-year-old woman with acute right upper quadrant pain due to omental infarction shows ill-defined, ovoid, fatty mass (arrows) of increased attenuation centered in the greater omentum.
|
|
|
was ist das'
|
swyer james syndrom
|
|
|
|
What is the classic triad of choledochal cysts?
|
palpable right upper quadrant mass, jaundice and pain (most first decade of life) Type 1 most common
|
|
|
|
Churg-Strauss syndrome is a
|
rare condition seen almost exclusively in patients with asthma and characterized by the presence of systemic vasculitis, extravascular granulomatous inflammation, and eosinophilia.
|
|
|

|
1. Hypersensitivity pneumonitis: ill defined centrilobular nodules.
2. Miliary TB: random nodules of the same size. 3. Sarcoidosis: nodules with perilymphatic distribution, along fissures, adenopathy. 4. Hypersensitivity pneumonitis: centrilobular nodules, notice sparing of the subpleural area. 5. Sarcoidosis: nodules with perilymphatic distribution, along fissures, adenopathy. 6. TB: Tree-in-bud appearance in a patient with active TB. 7. Langerhans cell histiocytosis: early nodular stage before the typical cysts appear. 8. Respiratory bronchiolitis: ill defined centrilobular nodules of ground-glass opacity. |
|
|
|
Wie werden die Vaskulitiden eingeteilt?
|
Large und small vessel
|
|
|
|
Welche Vaskulitiden gehören zu den large vessel disease?
|
Takayasu und Behcet
|
|
|
|
Wie werden die small vessel vaskulitiden weiter unterteilt?
|
-ANCA associated
- collagen vascular associated - Goodpasture syndrome |
|
|
|
Welche Erkrankungen gehören zu den ANCA associated Vaskulitiden?
|
Wegener granulomatosis
Churg-Strauss syndrome (CSS) Microscopic polyangiitis |
|
|
|
Welche Erkrankungen gehören zu den collagen vascular associated Vaskulitiden?
|
SLE, RA
|
|
|
|
Charakteristika Behcet
|
Chronic systemic vasculitis
Männer “Old Silk Route” Japan, China to the Mediterranean (Turkey and Iran) Thoracic involvement 8% Pulmonary vasculitis PA aneurysms (30% mortality) Thrombosis Infarction Hemorrhage A-V shunts |
|
|
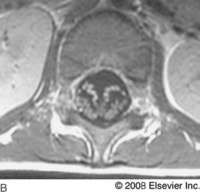
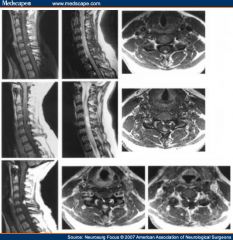
Modic?
|
Modic 1 hypointense on T1-weighted imaging (T1WI) and hyperintense on T2-weighted imaging (T2WI) represents marrow edema and inflammation.
|
|
|
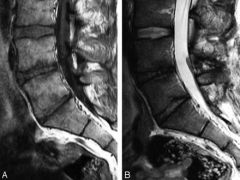
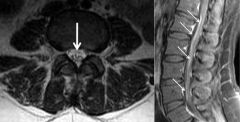
Modic?
|
Modic 3, hypointense on both T1 und T2, represents subchondral bone sclerosis
|
|
|
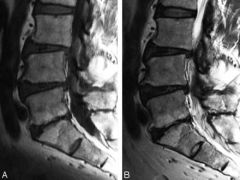
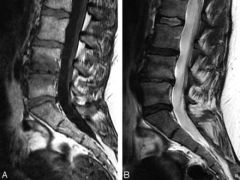
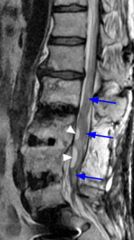
Modic?
|
Modic 2 hyperintense on T1WI (A) and isointense or hyperintense on T2WI (B).
conversion of normal red hemopoietic bone marrow into yellow fatty marrow as a result of marrow ischemia |
|
|
|
Demographie und algemeine Pathologie Wegener
|
selten um 50J Male=female, children possible
|
|
|
|
Patho Wegener Upper Airway
|
Knorpeldestruktion, Saddle nose, chronic nose obstruction und discharge, subglottic stricture, otitis media durch eustachian tube obstruction
|
|
|
|
Patho Wegener Lunge
|

" necrosis und hemorrhage"
Lung Most commonly affected (94%) Multiple bilateral nodules or masses Cavitation common (30%-50%) Occasionally solitary mass or nodule All patients progress Less common Diffuse alveolar hemorrhage |
|
|
|
Wegener im CT
|
feeding vessels, Cavitation (nodules grösser 2cm), subpleural predominant, CT HALO sign
|
|
|
|
Differential Multiple Vessel Associated
Nodules |
Metastatic Disease: squamous
multifocal infection: Tb, bacterial septic emboli Vasculitis |
|
|

|
Contrast-enhanced scan shows a multilocular cyst with septations and mural calcifications (straight arrow) in the left hepatic lobe. There is duct dilatation and extension of the cyst into the left hepatic and common bile ducts
|
|
|
|
Conditions associated with medullary nephrocalcinosis
|
practically, medullary sponge kidney, renal tubular acidosis (RTA) (Type 1, distal), and hyperparathyroidism (or other hypercalcemic states)
|
|
|

Medullary nephrocalinosis secondary to medullary sponge kidney is a radiologic diagnosis which is made when
|

calcifications located in the papillary region are associated with dilatation of the terminal portions of the collecting ducts. Multiple pyramids in both kidneys are usually involved
|
|
|
|
Type 1 (distal) RTA is a tubular defect which prevents
|
hydrogen ion secretion. As a result, urinary wasting of calcium occurs.
All tubules involved resulting in massive calcium deposition. |
|
|
|
Milzlazeration Grade I
|
< 1 cm depth
No active bleeding or vessel involvement |
|
|
|
Milzlazeration Grade II
|
1-3 cm
Active bleeding but no vessel involvement |
|
|
|
Milzlazeration Grade III
|
> 3 cm depth
Active bleeding and trabecular vessel involvement |
|
|
|
Milzlazeration Grade IV
|
Major devascularization (> 25% parenchyma)
Active bleeding with segmental or hilar vessel involvement |
|
|
|
Milzlazeration Grade V
|
Shattered spleen with complete devascularization
Active bleeding with hilar vessel involvement |
|
|
|
Milzhämatom Einteilung Grad I
|
Subcapsular hematoma < 10% of surface area
Intact capsule without active bleeding or expanding hematoma |
|
|
|
Milzhämatom Einteilung Grad II
|
Subcapsular hematoma 10-50% of surface area; parenchymal hematoma < 5 cm in diameter
Intact capsule without active bleeding or expanding hematoma |
|
|
|
Milzhämatom Einteilung Grad III
|
Subcapsular hematoma > 50% surface area, subcapsular rupture, or rupture of capsule; parenchymal hemorrhage > 5 cm diameter
Capsule may or may not be intact; active bleeding, expanding hematoma |
|
|
|
Milzhämatom Einteilung Grad IV
|
Parenchymal rupture
Capsular disruption and active bleeding with hemoperitoneum |
|
|
|
Milzhämatom Einteilung Grad Wieviele und Unterschied zu Lazeration?
|
4 lazeration 5
|
|
|
|
Bosniak 1
|
uncomplicated simple benign cysts as shown by sonography or CT.
|
|
|
|
Bosniak 2
|
minimally complicated cysts, including those with a few thin septations, high density cysts, cysts with thin fine peripheral calcifications, and infected cysts. These unenhancing lesions are treated conservatively, with follow-up CT or sonography at 3, 6, and 12 months.
|
|
|
|
Bosniak 3
|
more complicated masses including those with thick, irregular, or numerous septations, central or thick peripheral calcifications, nonenhancing nodularity, a thick wall or multiple loculations. Surgical exploration of these lesions is recommended unless contraindicated.
|
|
|
|
Bosniak 4
|
clearly malignant masses with enhancing solid elements. Surgical resection is indicated. Remember that some cystic renal cell carcinomas may be composed entirely of homogeneous water density material. Here, the only clues to the true nature of the lesion may be in slight thickening of the wall, and contrast enhancement. Ultrasound, however, is usually more revealing than CT in these cases.
|
|
|
|
wann tritt der wilms tumor auf?
|
peak 3 jahre - 8 Jahre
|
|
|
|
Wie ist die Prognose des Wilms Tumor?
|
90% heilen unter chemotherapie
|
|
|
|
Wohin metastasiert der wilms tumor?
|
lungs, bone, liver, and brain.
|
|
|
|
was ist das 123 Zeichen
|
bilateral hilar und right paratracheal nodal enlargement Sarcoidosis
|
|
|
|
Sarcoidosis Stage 0
|
Normal chest radiography
|
|
|
|
Sarcoidosis Stage 1
|
nur lymphadenopathy
|
|
|
|
Sarcoidosis Stage 2
|
nodal enlargement und parenchymal disease
|
|
|
|
Sarcoidosis Stage 3
|
parenchymal disease only
|
|
|
|
Sarcoidosis Stage 4
|
end stage pulmonary fibrosis
|
|
|
|
Was hilft im CT TCC von RCC zu unterscheiden?
|
RCC hypervaskulär, TCC hypovaskulär
|
|
|
|
womit sind multiple AML assoziert?
|
Tuberöse sklerose
|
|
|
|
Was sind die Charakteristika der Tuberösen Sklerose?
|
autosomal dominant neurocutaneous disorder, is also characterized by mental retardation, epilepsy, renal cysts, and hamartomas of the skin, brain, heart, and lungs.
|
|
|
|
Multilocular cystic nephroma altersverteilung
|
bimodale Alterverteilung boys younger than 5y older women 5 - 6th decade
|
|
|
|
Multicystic nephroma charakteristika
|
capsule und multiple cysten, capsule und cystenwände enhancen, typisch herniert ins Nierenbecken, schwierig von zystischem RCC und Wilms tumor zu unterscheiden (bosniak iii oder iv)
|
|
|
|
Was ist die Zöliakie Sprue?
|
autoimmune krankheit mit hypersensitivity to wheat gluten, malabsorption und hypersecretion,
erhöhtes Krebsrisiko lymphom und adenokarzinom, dg confirmed duodenal biopsy |
|
|

Sprue Zöliakie findings:
|
small bowel dilatation, reversal of jejunal und ileal fold patterns, transient intususception
|
|
|
|
Was ist eine medullary sponge kidney?
|
tubular ektasie, medullary nephrocalcinosis; when calcifications located in the papillary region are associated with dilatation of the terminal portions of the collecting ducts.
|
|
|
|
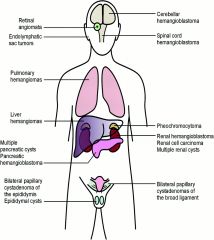
was ist die von Hippel Lindau disease?
|
autosomal dominant vererbte Erkrankung mit Zysten in zahlreichen Organen assoziert mit vielen Neoplasien (siehe andere Karte)
|
|
|
|
von Hippel Lindau disease assoziert mit
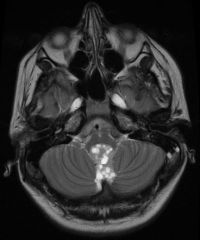
|
cysts und neoplasien
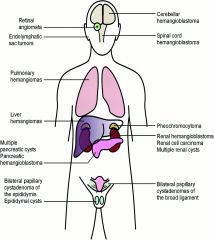
CNS hemangioblastomas, retinal angiomas, multiple renal cysts, renal cell carcinoma (RCC), pancreatic cysts, pancreatic cystadenocarcinomas, pancreatic islet cell tumors, pheochromocytomas, and epididymal cystadenomas. Solid renal tumors occur in 25% of patients and are bilateral and multiple in up to 60% of them. |
|
|
|
von Hippel Lindau disease trias
|
triad of retinal angiomatosis, cerebellar hemangioblastoma, and cysts of various organs
|
|
|
|
Tuberöse Sklerose Def
|
autosomal dominant
trias seizures, adenoma sebaceum, mental retardation |
|
|
|
Tuberöse Sklerose Niere
|
multiple AML, auch Zysten v.a. bei Kindern
|
|
|
|
Wo kommen hamartome bei tuberöser Sklerose vor?
|
retina, cortical tubers, subependymal, pulmonary lymphangiomyomatosis, cardiac rhabdomyoma, angiofribroma
|
|
|
|
Was ist die multicystic dysplastic kidney?
|
cystische Nierenerkrankung mit nichtfunktionalem zystischem Cortex, kann calcify, auch fokale form, nonenhancing cystic mass mit multiplen septen
|
|
|
|
was ist die pyeloureteritis cystica?
|
benigne erkrankung assoziert mit chronic urinary tract infection/irritation, urothelial metaplasie
|
|
|
|
Korrekte Lage Pulmonaliskatheter
|
nicht mehr als 3cm von der Mittellinie entfernt, in der A.pulmonalis
|
|
|
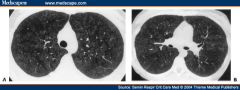
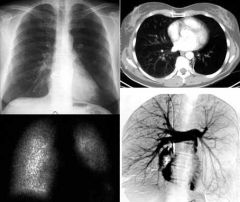
Was sieht man beim Goodpasture syndrome?
|
Goodpasture's syndrome. (A) Computed tomographic (CT) image at the level of the aortic arch shows centrilobular ground-glass opacities throughout the upper lobes due to diffuse pulmonary hemorrhage. (B) CT image at the level of the right main pulmonary artery shows ground-glass opacities in the lower lobes. The patient was a 35-year-old woman.
|
|
|
|
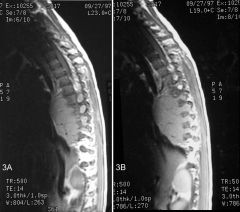
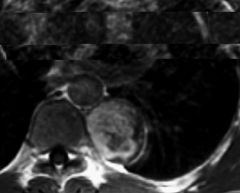
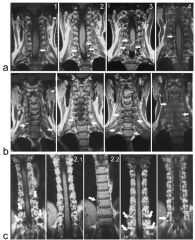
T1-weighted magnetic resonance images of a ganglioneuroma. The sagittal views demonstrate a well-defined, solid mass located slightly anterior to the midthoracic vertebral bodies. Ganglioneuroma. The mass is extending into the neural foramina, with widening of the neural foramina. The flow void within the lesion represents vascularity.
|
|
|
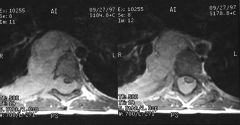
was ist das?
|
T1-weighted postcontrast axial images of a ganglioneuroma demonstrate homogeneous enhancement of the lesion. The lesion is extending from the right paraspinal region into the epidural space through the neural foramina causing cord compression.
|
|
|

Was ist das?
|
This axial noncontrast-enhanced computed tomography image of a ganglioneuroblastoma demonstrates a large, left heterogeneous paraspinal lesion with speckled calcifications that are predominantly peripheral.
This coronal T2-weighted image demonstrates a well-defined, lobulated mass with fibrous septations. The mass is extending into the neural foramina and is causing cord compression in the midthoracic region. The mass is also displacing the aorta to the right. |
|
|
|
neuroblastoma
Axial nonenhanced T1-weighted MRI shows a hypointense mass in the retroperitoneum originating from the left adrenal gland. The mass displaces the left kidney in an anterolateral direction, it extends through the neuroforamen into the spinal canal, and it displaces the spinal cord to the right. The exact site of origin of large masses can be difficult to determine. Sympathetic-chain primaries supposedly invade the spinal canal with greater frequency than do adrenal primaries. |
|
|

|
neuroblastoma
Axial T2-weighted MRI in the same patient as in the previous image again demonstrates extradural extension into the spinal canal. The tumor appears hyperintense. Spinal cord displacement is better demonstrated on T2-weighted images than on other images. |
|
|

Was ist ein staghorn calculus?
|
Upper urinary tract stones that involve the renal pelvis and extend into at least 2 calyces are classified as staghorn calculi
|
|
|
Was ist das? Charakteristika?
|
Multilocular cystic nephroma
young boys bis 10y, women um 30y unilateral, complex cystic mass enhancing septations that extend into the renal pelvis often Bosniak 3 oder 4 ( nephrectomy) hemorrhage und calcifications uncommon |
|
|
|
was sind biliary hamartomas? Synonym?
|
von Meyenburg Komplexe, Biliary hamartomas are composed of small disorganised clusters of dilated cystic bile ducts
|
|
|

Was ist das ?
Characteristics? |
medullary carcinoma, rare tumor calyceal transitional epithelium, highly aggressive, young blacks sickle cell , prognosis very poor, centrally located kidney shape preserved
|
|
|
|
bone lesions with high t1 signal
|
intraooseous lipoma, hemangioma, bone infarct, paget's disease
|
|
|
|
bone lesions with low signal on t2
|
Sclerosis/calcification/matrix
some fibrous lesions primary lymophoma of the bone |
|
|
|
Was heisst stag horn
|

hirsch horn
|
|
|

Was ist das?
|
posterior ribs lytic expansile appearance, anterior ribs most often sclerotis in appearance.
Thoracic spine here also involved |
|
|
Was ist das
|
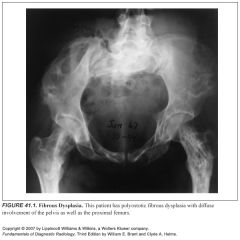
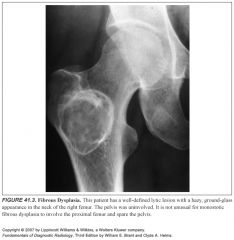
polyostotic fibrous dysplasia
when pelvis involved always femur same side also involved |
|
|
|
Was ist das maffucci syndrome?
|

malignant transformation more common than in ollier disease
|
|
|
|
Was ist die ollier disease?
|

nonhereditary disease with multiple enchondromas, often stable at puberty, risk chondrosarcoma 25%. hand foot deformities, multiple radiolucent expansile masses
tendency for unilaterality |
|
|
|
Wo kommt die fibröse dysplasie am häufigsten vor?
|
monostotic 85 %: femur most common, tibia ribs
polyostotic peak 8y: femur 90% tibia 80% pelvis 80% craniofacial |
|
|
|
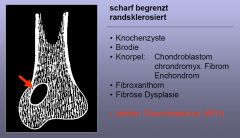
Discriminator fibröse dysplasie?
|
no periosteal reaction
ground glass can be misleading as it can be pure lytic |
|
|
|
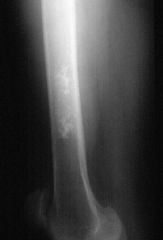
Enchondroma discriminator?
|
1. calcification present (except phalanges)
2. painless ( no periostitis) |
|
|
|
a lytic lesion in the phalanges is most commonly a
|
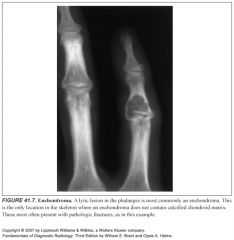
|
|
|
|
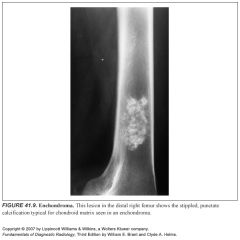
Enchondroma
chondroid calcifications rings and arcs scalloped endosteum cortex expansion but no cortical breakthrough unless fractured |
|
|
|
an was muss man auch denken wenn man an fibröse dysplasie denkt?
|

adamantinoma
rare tumor 90% tibia, jaw, 20 - 50y, sharply lytic lesion with marginal sclerosis, eccentric or central diaphysis, multilocular satellite foci in fibula, slightly expansile |
|
|
was ist das mc cune albright syndrome
|

polyostotic unilateral half body fibrous dysplasia, endocrine abnormalities, cafe au lait spots predominantly girls
|
|
|

Was ist cherubism?
|

symmetrical fibrous dysplasia of mandible and maxilla, familiär
|
|
|
|
Discrminator eosinophiles granulom
|
younger than 30, korrekter name heute langerhans cell histiocytose
|
|
|
|
Wofür steht langerhans cell histiocytosis?
|
abnormal proliferation of Histiocytes
3 Formen: letterer-Siwe: acute disseminated form 10% Hand-Schüller-Christian: chronic disseminated form 20% EG: only bone involvement 70% |
|
|
|
Was ist die DD von bony sequestrum?
|
EG, osteomyelitis, lymphom, fibrosarcoma
|
|
|
|
Was ist ein Sequestrum?
|
A sequestrum is usually a complication of osteomyelitis and represents devascularisation of a portion of bone with necrosis and resorption of surrounding bone leaving a 'floating' piece.
|
|
|
|
Wo kommt das eosinophile granulom am häufigsten vor?
|
Skull und mandibula
floating tooth solitary or multiple punched out lytic lesions with or without sclerotic rim double contour Greater involvement of the inner than the outer table. button sequestrum geographic skull |
|
|
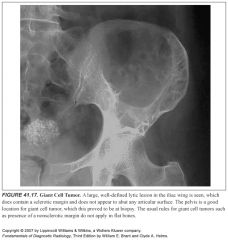
Discriminators Giant cell tumor
|
1. Epiphyses closed
2. Abuts the articular surface in long bones 3. well defined with a nonsclerotic margin 4. eccentric |
|
|

Was ist das?
|
Rx features Giant cell Tumor
lytic subarticular lesion expansile narrow transition, no sclerotic margin may be locally aggressive pathologic fracture 30% |
|
|

Giant cell tu Charakteristika (nicht Rx)
|
selten, epiphyse with metaphyseal extension
age: after epiphyseal closure 50 % around knee 10% are malignant (local spread, metastases) |
|
|
|
Nonossifying Fibroma discriminators
|
younger 30
painless (no perisotitis) cortically based |
|
|
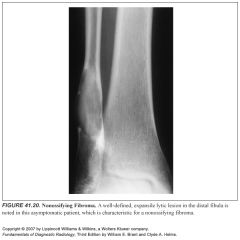
Unterschied NOF und FCD?
|

histologisch dasselbe, radiolucent lesion with or without sclerotic border, fcd cortex, nof medullary involvement
well demracated peripheral osseous shell, close to growth plate posteromedial 90% Tibia und Fibula |
|
|

Was ist das?
Rx Charakteristika |

Osteoblastoma
Spine posterior elements, long bones expansile lytic or slerotic >2cm(giant osteoid osteoma) similar to abc, central calcification, malignang osteoblastoma may destroy cortex and mimic osteosarcoma |
|
|
|
Discriminator Osteoblastoma
|
mentioned when ABC is mentioned (specially in the posterior elements of the spine)
|
|
|
|
Discriminator metastatic disease and multiple myeloma
|
older than 40y (35y)
|
|
|
|
Discriminator Aneurysmal Bone Cyst
|
1. Expansile
2. younger than 30y |
|
|
|
Discriminator solitary bone cyst
|
1. central
2. younger than 30y |
|
|
|
Discriminator Infection
|
always mention
|
|
|
|
Discriminator Chondroblastoma
|
1. younger 30
2. Epiphyseal |
|
|
|
Discriminator Chondromyxoid
|
no calcified matrix
|
|
|
|
lytic expansile metastases are often from
|
thyroid and renal cell carcinoma
|
|
|
|
like metastasis plasmacytomas often have a ..... appearance
|
completely benign
|
|
|
|
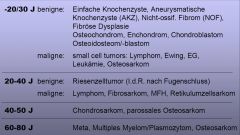
Lesions in patients younger than 30y
|
Eosinophilic granuloma
Aneurysmal bone cyst Nonossifying Fibroma Chondroblastoma Solitary bone cyst |
|
|
|
Lesions with no pain or periostitis
|
Fibrous dysplasia
Enchondroma Nonossyfing fibroma solitary bone cyst |
|
|
|
Automatics younger than 30y
|
Infection
eosinophilic granuloma |
|
|
|
Automatics older than 40y
|
infection
metastatic disease multiple myeloma |
|
|

Epiphyseal Lesions
|
infection
Giant cell Tumor Chondroblastoma Geode |
|
|

Differential for Rib lesions
|
Fibrous dysplasia
Aneurysmal bone cyst metastatic disease and myeloma enchondroma and eosinophilic granuloma |
|
|
|
Certain bones in the body can be considered "epiphyseal equivalents" for purposes of differential diagnosis. These include
|
the patella, the calcaneus, and most apophyses. the classic epiphyseal entities such as chondroblastoma, giant cell tumors and aneurysmal bone cysts.
|
|
|
|
With a long lesion in a long bone, think of
|
fibrous dysplasia.
|
|
|
|
Differential Diagnosis of Multiple Lucent Bone Lesions
|
Mnemonic = FOGMACHINES --> FEMHI
Fibrous Dysplasia Metastasis / Myeloma Hyperparathyroidism (brown tumors) / Hemangioma Infection Eosinophilic Granuloma / Enchondroma |
|
|
|
Multiple myeloma Characteristics allg.
|

most common primary bone tumor
95% >40y plasmacytentumor distribution wie red marrow: vertebral bodies, axial skeleton (skull, spine, ribs, pelvis) |
|
|
|
Staging multiples myelom Ia und b
|
Ia limited disease or plasmacytoma
Ib mild diffuse disease with <5 lesions |
|
|
|
Staging multiples myelom IIa, b
III a , b |
IIa, b moderate diffuse disease 5 - 20 focal lesions
IIIa und b severe diffuse disease >20 lesions |
|
|
|
Klinik Multiples myelom
und Komplikationen |
IgA und G peak
Bence jones Protein im Urin bone pain anemia Pathologic fractures Amyloidosis most Plasmacytomas progress to multiple myeloma |
|
|
|
Wie sieht das Plasmacytom aus?
Wo kommt es häufig vor? |

large und expansile
vertebral body, pelvis, femur |
|
|
|
Multiples myelom hat 2 common radiologic appearances, welche
|
multiple well defined punched out lesions 80% und
generalized osteopenia |
|
|
|
common lytic
|
kidney, lung, thyroid, breast
|
|
|
|
common sclerotic metastases
|
prostate, breast
|
|
|
|
Bone metastases Häufigkeit
Kinder |
Neuroblastoma
leukemia, lymphoma medulloblastoma sarcomas Wilms tumor |
|
|
|
Other rare sclerotic
|
hodgkin lymphoma
carcinoid medulloblastoma neuroblastoma TCC |
|
|
|
Was ist ein simple bone cyst?
|

common benign fluid filled lesion of childhood of unknown cause
10 - 20y, 50% present with pathologic fractures and pain most resolve with bone maturity |
|
|

Simple bone cyst Rx features
|

central (intramedullary) metadiaphyseal
respects physis expansile lesion fluid filled cavities fallen fragment sign pathognomonic no periosteal reaction unless fractured |
|
|

Was ist das?
Häufige Location? |

Aneurysmal bone cyst
posterior elements of spine metaphysis of long bones pelvis Wie ist die Definition? |
expansile nonneoplastic lesion containing thinwalled bloddfilled cystic cavities, age 5 - 20y
rapid progression with acute pain |
|

Rx features aneurysmal bone cyst
|

eccentric in location, expansile, thin maintained cortex, no periosteal reaction unless fractured
respects epiphyseal plate large lesions may appear aggressive fluid fluid levels in cystic components |
|
|
|
DD fluid fluid levels
|
ABC
simple bone cyst teleangiectatic osteosarcoma und andere |
|
|
|
Was ist pathognomonisch für Hyperparathyroidism?
|

bone resorption subperiosteal
radial aspect of middle phalanges |
|
|
|
Wo findetman brown tumors am häufigsten?
|
pelvis, jaw, femur
loss of lamina dura, soft tissue calcification, chondrocalcinosis, compl. fractures |
|
|
|
welche Knochen haben die Tendenz sich wie Epiphysen zuverhalten (bei DD)
|
Apophyses, carpal bones, tarsal bones und patella
|
|
|

Was ist ein Chondroblastom wo kommt es vor?
|

seltener Tumor in the epiphysis of immature skeleton, lobulated geographic lucency
around knee und humerus Th curretage |
|
|

Was ist das?
|
Chondromyxoid fibroma
very rare, resemble nof mention when nof is mentioned, no calcified matrix |
|
|
|
Was ist der Unterschied zwischen Apophyse und Epiphyse?
|
Epiphyse dienen dem Längenwachstum, Apophysen dienen als ligamentäre attachments
|
|
|
|
Welche Subtypen des Osteosarkoms gibt es?
|
teleangiectatic
multicentric juxtacorticale -parosteal und periosteal |
|
|
|
Definition Osteosarkom
|
second most common malignant tumor of connective tissue that produces osteoid matrix and variable amounts of cartilage matrix and fibrous tissue
|
|
|

Wann kommt dieser Tumor vor?
Rx features |

Osteosarcoma
10y - 30y poorly defined, intramedullary, metaphyseal mass that extends through cortex, matrix ossär, cartilaginous und fibrör aggressive periosteal reaction skin lesions und mets |
|
|

Location Osteosarcoma
|
Tubular bones 80%
- around knee 75% - Humerus other bones 20% flat bones, vertebral bodies |
|
|

Was ist das characteristics?
|
teleangiectatic osteosarcoma, aggressive, worse prognosis
purely, large lytic lesion cystic cavities filled with blood / necrosis (fluid fluid levels) may mimic abc |
|
|
|
Was ist das multicentrische Osteosarkom?
|
gleichzeitig OS an mehreren Stellen, metaphyseal und symmetrisch, nur bei children 5y - 10y sehr schlechte prognose
|
|
|
Was ist das?
|

Parosteales OS
low grade OS older age group (20y - 50y) location similar to normal os Rx. features 80% distal femur attached to cortex only at origin central calcification vs myositis ossifican mit ringförmiger ossification |
|
|
|
wie ist die Überlebensrate der verschiedenen Typen OS?
|
parosteal 80%, Periosteal 50%, conventional 20%, teleangiectatic 20%
|
|
|
|
Was heisst ALMA?
|
Alter
Lokalisation Morphologie Ausdehnung |
|
|
|
Charakteristika Lodwick 1a
|
|
|
|
|
Charakteristika Lodwick 1b
|

|
|
|
|
Übersicht Lodwick 1ABC
|
|
|
|
|
Altersverteilung Knochentumore
|
|
|
|
|
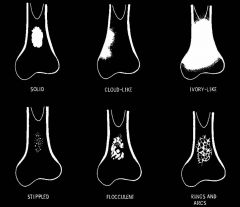
Welche matrixtypen gibt es bei chondraler und ossärer Matrix?
|
|
|
|
|
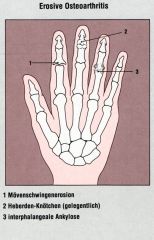
Erosive Arthrose Verteilung
|
|
|
|
|
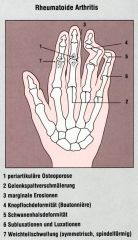
Verteilung Frühform RA
|
PIP‘s, MCP‘s, pankarpal
|
|
|
|
Frühform RA Verteilung
|
|
|
|
|
RA Spätform
|
|
|
|
|
Definition CPPD
|
Kalzium-Pyrophosphosphat-Krankheit: Ablagerung von CPPD Kristallen in und um Gelenke
|
|
|
|
Definition Pseudogicht
|
Pseudogicht: Form der klinischen Manifestation der CPPD
|
|
|
|
Definiton Pyrophosphat-Arthropathie
|
Pyrophosphat-Arthropathie: Ausdruck der Gelenksdestruktion im Rahmen der CPPD Deposition
|
|
|

Ursachen
|

CPPD, Gicht, Hyperparathyreodismus, Hämochromatose, M. Wilson
|
|
|

|
Weichteile Normal
Subluxationen Keine Mineralisation Regelrecht Kalzifikationen TFC Gelenkspalt Homogene Gelenkspaltverschälerung MCP; radiokarpal und zwischen Capitatum und Lunatum Erosionen Nein, aber Zysten Knochenpro-liferation Osteophyten am MCP, subchondrale Sklerose Navikulare, Capitatum, und Lunatum Verteilung MCP‘s, Radiokarpal, Capitatum-Lunatum |
|
|
|
Weichteile Fusiforme Fingerschwellung – 1°, 2° und 4° Finger
Subluxationen Keine Mineralisation Regelrecht Kalzifikationen Keine Gelenkspalt Homogene Gelenkspaltverschälerung 2°- 4° MCP; Destruktion 4° PIP, 1° IP, 2° DIP Erosionen Ja (gross; ‚pencil in a cup‘ IP) Knochenproliferation Periostale Knochenneubildung Verteilung MCP‘s, PIP‘s, DIP‘s im Strahl |
|
|
|
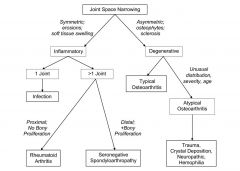
Flowchart Ossäre Läsion
|
|
|
|

Was ist das?
|

posteriore Luxation
|
|
|

Was ist das?
|
Erosive Arthrose
|
|
|
|
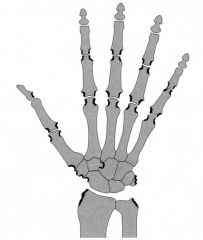
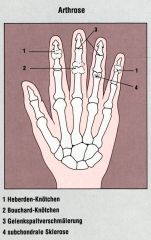
Arthrose Hand Verteilung
|
|
|
|
|
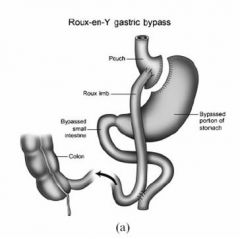
Wie sieht ein Roux en y aus?
|
|
|
|
|
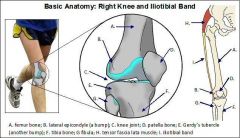
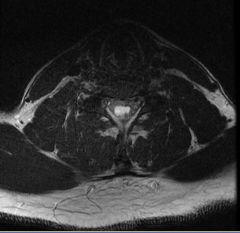
Was ist das iliotibial band syndrome?
|
|
|
|
|
kann bei endokriner orbitopathie nur ein muskel betroffen sein?
|
ja in 5 % meist superior rectus
|
|
|
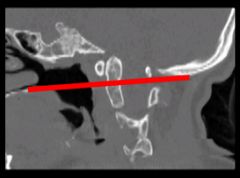
Wie heisst das ?
|
basilar invagination
|
|
|
|
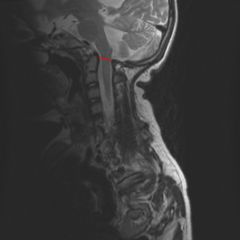
Wie sieht die Chiari 1 malformation aus?
|

|
|
|
|
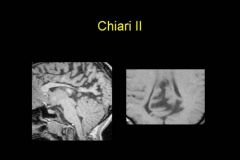
Wie sieht die Chiari II Malformation aus?
|
|
|
|
|
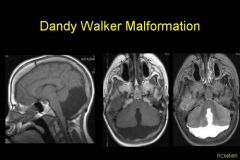
Wie sieht dandy walker aus?
|
|
|
|
|
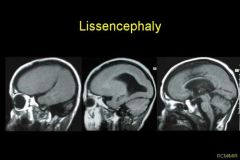
Wie sieht die lissencephaly aus?
was ist die lissencephaly? |

smooth brain surface, fehlende gyrierung
my be secondary to cmv infectionin utero |
|
|
|
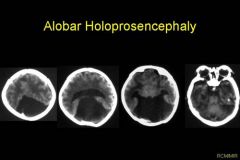
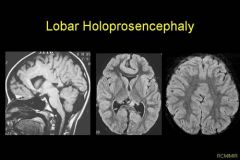
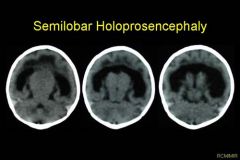
wie werden die holoprosencephaly eingeteilt?
|
alobar, lobar, semilobar
|
|
|
|
Was ist die holoprosencephaly?
|
failure of primitive brain to cleave into left and right hemispheres
|
|
|
|
wie sieht die alobar holoprosencephaly aus?
|
|
|
|
|
wie sieht die lobar holoprosencephaly aus?
|
|
|
|
|
Wie sieht die semilobar holoprosencephaly aus'
|
|
|
|
|
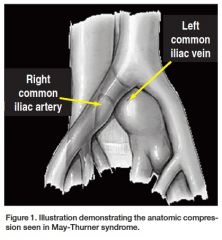
Was ist das May Thurner Syndrom?
|
|
|
|
|
Was heisst MELAS?
|
Mitochondrial encephalopathy with lactic acidosis and stroke
|
|
|
|
Was heisst PRES?
|
Posterior reversible encephalopathy syndrome
|
|
|
|
Was heisst ADEM?
|
Acute disseminated encephalomyelitis
|
|
|
|
Was heisst CADASIL?
|
Cerebral autosomal-dominant arteriopathy with subcortical infarction and leukoencephalopathy
|
|
|
|
Was heisst PML?
|
Progressive multifocal Leukoencephalopathy
|
|
|
Diagnose?
|
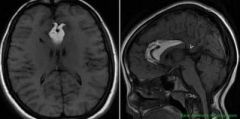
Empty sella
|
|
|
Dg?
|
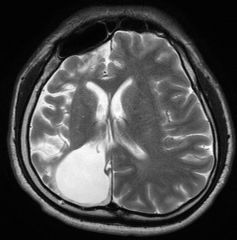
Cortical heterotopie
|
|
|
Diagnose?
|
Lissencephalie
|
|
|
Diagnose?
|
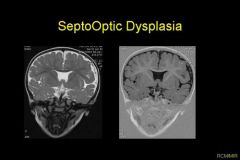
Septooptic dysplasie
|
|
|
Diagnose?
|
polymicrogyrie
|
|
|
Dg?
|
interhemispheric lipoma
|
|
|
dg? aka
|
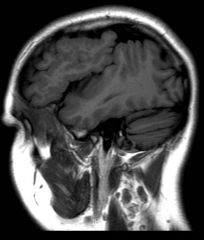
dyke davidoff
cerebral hemiatrophy compensatory skull thickening |
|
|
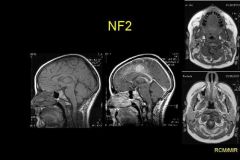
Dg?
|
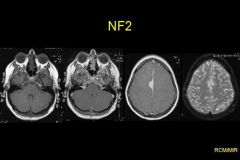
Ependymoma
Misme multiple inherited acoustic schwannoma (bilateral), meningioma, ependymoma, NF 2 |
|
|
DG?
|
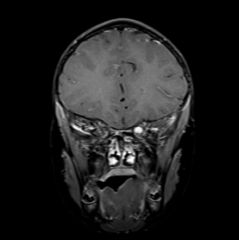
acoustic schwannoma
NF 2 auch cranial trigeminus |
|
|
Dg?
|
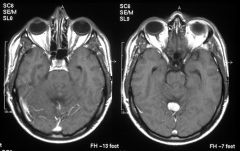
von Hippel Lindau syndrome
|
|
|
Dg?
|
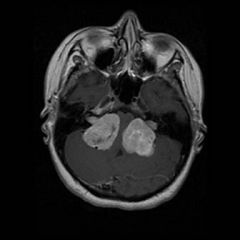
hemangioblastoma bei VHL
|
|
|
|
Manifestationen VHl Disease
|
|
|
|
Dg?
|
NF 2
|
|
|
dg?
|
optic nerve glioma
NF ? |
NF 1
|
|

Dg?
|
tibial pseudoarthrosis
NF ? |
1
|
|
Dg?
|
mediastinal schwannoma
|
|
|

Dg?
|
Schwannoma
|
|
|
Was ist das?
|
hemangioblastoma
|
|
|

Was ist das?
Mit was ist das assoziert? |
VHL
|
|
|

Dg?
|
spinal ependymoma
|
|
|
Dg?
|
Astrocytoma spine
|
|
|

Dg?
|
Astrocytoma spine km
|
|
|

Dg?
|
acute localised myelitis
|
|
|
Was ist das?
|
pseudomeningocele
|
|
|
Was ist das?
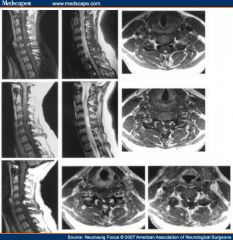
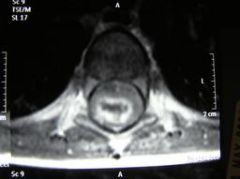
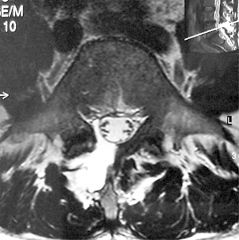
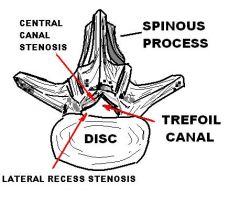
|
trefoil spinal stenosis
|
|
|
Dg?
|
Guillain Barre
|
|
|
Dg?
|
Guilain Barre
|
|
|
Dg?
|
arachnoiditis
with intradural cysts |
|
|

DG?
|
lipomyelomeingocele
|
|
|

DG?
|
tethered cord
|
|
|

Dg?
|
CIPD
chronic inflammatory demyelinating disease |
|
|

DG?
|
Pott disease
|
|
|
Dg?
|
Diastematomyelia
|
|
|

Dg?
|
Hydrosyringomyelie
|
|
|
Dg?
|
Hydrosyringomyelie axial
|
|
|
Dg?
|
Optic nerve glioma
assoziert mit |
NF 1
|
|
Dg
|
Von Hippel lindau disease
|
|
|
Dg?
|
NF 2
|
|
|
Dg?
|
hemangioblastoma
|
|
|

DG?
|
Hemangioblastoma spine VHL
|
|
|

DG?
|
Neurofibroma whole spine
|
|
|

Dg?
|
Ependymoma
|
|
|
Dg?
|
spinal neurofibromatosis
|
|
|
Dg?
|
VHL
Phaeochromocytomas usw. |
|
|
DG?
|
cortical heterotopie
|
|
|
|
RIVA=englisch
|
LAD (left=CX und RIVA)
|
|
|
|
RIVP= englisch
|
PDA=posterior descendent artery
right |
|
|
|
Was ist ein Askin Tumor?
|
form of primitive neuroectodermal tumor (PNET). It arises in the soft tissues of the thorax.
|
|
|

Was ist das?
|
Askin Tumor
Children and young adults chest wall pain. mass with or without rib destruction. Rib destruction is less common than in Ewing sarcoma. +- pleural effusion. metastasizes to lung and bone are common. |
|
|
Assoziert mit?
|
COPD
Definition? |
Saber sheath trachea is a trachea in which the coronal dimension is less than or equal to 2/3 of the sagittal dimension. The extrathoracic trachea is normal
|
|

Was ist das?
|
Tracheopathia osteochondroplastica, rare
cartilaginous or osseous submucosal mural nodules no treatment |
|
|

Dg? Warum?
|
lower lobe predominant emphysema, combination with cirrhosis or bullae
in nonsmokers, symptoms or signs rarely develop before age 55 |
|
|

Was ist das?
|
aortic transsection
intimal flap am aortic isthmus nach autounfall und wandhematoma |
|
|
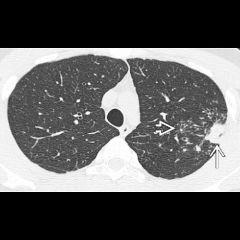
beschreiben und Diagnose
|
Axial NECT shows upper lobe nodular opacity straight arrow and surrounding bronchogenic spread with centrilobular nodules and tree-in-bud opacities open arrow.
Mycoplasma Pneumonie |
|
|
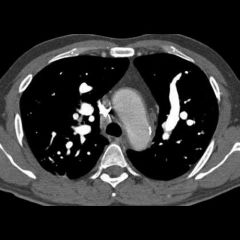
Was ist das beschreiben und diagnose
|
Axial CECT images (#1-3) show circumferential thickening of the aortic wall straight arrow. Enlarged tortuous pulmonary arteries curved arrow and prominent ectatic collaterals (open arrow, #1) are also seen.
Takayasu arteritis |
|
|

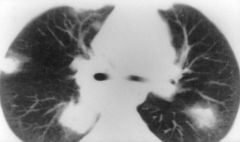
Was ist das?
|
talcosis
progressive massive fibrosis könnte auch silicosis und sarcoidosis sein wichtig ist pmf |
|
|

Wie heisst das Zeichen?
WIe die Diagnose? |
Cord sign
cortical vein thrombosis |
|
|
|
Wie ist die Verteilung der Läsionen bei neurosarcoid?
|
|
|
|
Was ist das ?
|
creutzfeld jakob classic variant
nucleus caudatus, putamen gray matter (auch asymmetric) |
|
|
Was ist die DG?
|
CJD variant
pulvinar t2 und flair hyperintensity |
|
|
Was ist das?
|
hockey stick sign
cjd beide |
|
|
Dg?
|
PCA infarction
|
|
|
Dg?
|
PCA infarction
|
|
|

Was ist das?
|
PICA infarction
Was ist das Wallenberg syndrom? |
Horner syndrome, ataxia, and contralateral hemisensory
|
|
Stromgebiet?
|
Medulla und Kleinhirnhemisphere PICA (AICA ist hier nicht hell!)
|
|
|
Was ist das?
|
SCA infarction, notice limitation to the midline!
|
|
|
|
Aus wem kommen die mediale lenticulostriatae aus wo die laterale?
|
|
|
|
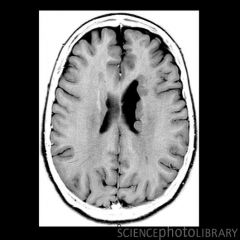
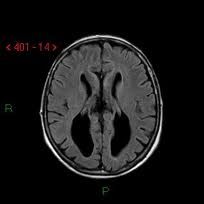
Was ist das?
|
normal pressure hydrocephalus
Wieso' |
dilatierte ventricle und silvii fissur gleich stark dilatiert, 4th fast normal |
|
|
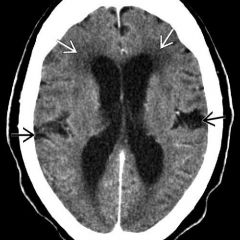
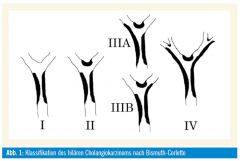
Wie werden die Cholangiokarzinome eingeteilt?
|
|
|
|
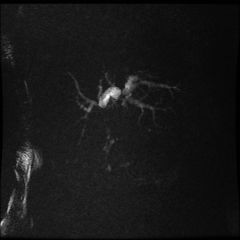
Was ist hier typisch für was?
|
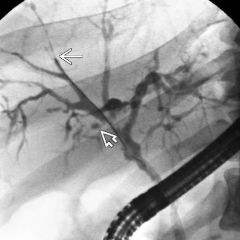
Klatskin tumor bei Cholangiokarzinom keine Verbindung zwischen den dilatierten Gallengänen im Hilus / Gabelung
|
|
|
|
Wo sollte der Nabelvenenkatheter liegen
|
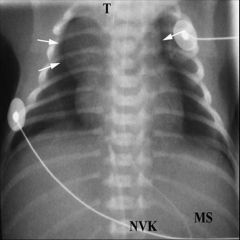
Übergang rechter Vorhof VCI
|
|
|

Wo sollte der Nabelarterienkatheter liegen?
|

Katheterspitze nicht auf Höhe der abgehenden Gefässe (Thrombosegefahr)
Katheterposition: high lines: Spitze in der thorakalen A.desc. (Th8-10) low lines: Spitze unterhalb L3 Spitze nicht zwischen Th10-L3 |
|
|

Was ist das beschreiben...
|
feingranuläres Muster HMK I
|
|
|

Was ist das beschreiben...
|
Zwerchfell und Herzkontur knapp abgenzbar
Deutliches Air-bronchogramm HMK 2 |
|
|
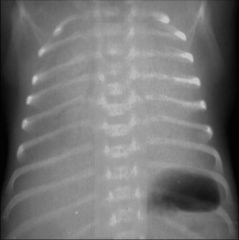
Was ist das beschreiben...
|
HMK III white lung
|
|
|
|
Was ist das?
|

|
|
|
|
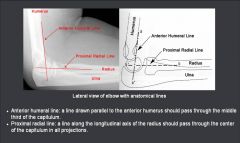
Wie heissen die Linien am Ellbogen?
|
|
|
|
|
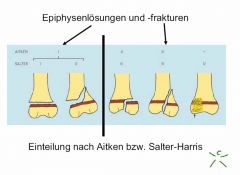
Einteilung Aitken und Salter Harris
|
|
|
|

Was ist hier typisch für was
|
Barrett Oesophagus macht typischerweise low or mid esophageal strictures
|
|
|

Was ist das?
|
Spontaneous omental infarcts almost always occur near the ascending colon and usually resolve without complication
|
|
|
Was ist typisch?
|
Melanome sind die häufigsten Metastasen der Gallenblase und sind bekannt dafür gerne dorthin zu metastasieren.
|
|
|
Dg?
|

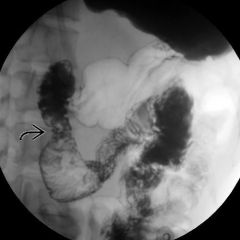
Anular pancreas
Pfeile zeigen normales pankreasgewebe um das duodenum |
|
|
|
Gross dilation of pancreatic duct, plus intraductal tumor are classic findings of
|
intraductal pancreatic mucinous tumor (IPMT)
|
|
|

beschreiben und DG.
|
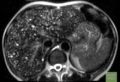
Budd chiari
moderate ascites liver enhances heterogeneously with the peripheral segments appearing low in density and diminished in size. The deep right lobe and caudate enhance normally and are relatively hypertrophied. The hepatic veins are small and do not enhance, causing them to simulate dilated intrahepatic bile ducts. |
|
|
|
Axial CECT shows a small liver with deep scars and lobular contour, typical of cirrhosis due to PSC. Note the irregular dilation of intrahepatic ducts and esophageal varices
|
|
|
Was sieht man?
|
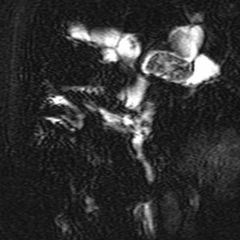
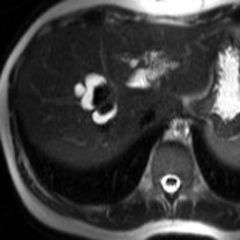
caroli disease
cystic dilation of many intrahepatic ducts, many of which contain calculi. The dilated ducts are evident as bright "cystic " lesions straight arrow. Within the most dilated ducts, low signal stones are evident |
|
|
|
Was ist das Bouveret syndrome?
|
Bouveret syndrome
Gallstone eroded into duodenum |
|
|

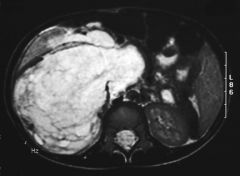
Was ist das?
|
size, exophytic extension, and foci of necrosis are characteristic features of a gastric stromal tumor (GIST).
|
|
|
Dg weshalb
|
heterogeneously hypervascular. Hepatic adenomas are often seen with a foci of fat, necrosis, or hemorrhage. few intrahepatic processes are hyperintense on T1WI, except for hemorrhage and fat.
|
|
|

Wie erkennt man einen arterioportalen shunt?
|

arteriel hell wedge shaped
portalvenös isodens dilatierte arterien im hilus |
|
|
Was ist das?
|
mucinous cystic pancreas tumourmost common cystic neoplasm, usually occurring in middle-aged women in the body-tail segment. The mass may have peripheral calcification.
|
|
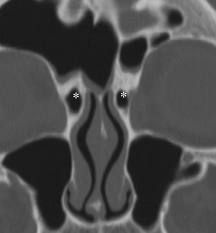
|

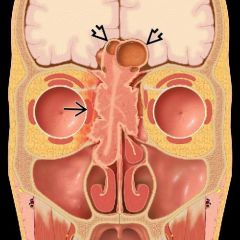
Was ist das?
|
agger nasi cells
most anterior ethmoid cells frequently pneumatize adjacent bones like frontal bone , maxilla, middle turbinate |
|
|

Was sind onodi cells?
|
most posterior ethmoid cells that surround optic canal and optic nerve
|
|
|

Was sind haller cells?
|
posterior ethmoid cells invading the medial orbit floor can obstruct ostia, can be source of infection
|
|
|
Was sind nasofrontal ducts?
|
frontal sinus drains directly into frontal recess of nasal cavity
|
|
|

was ist die fossa pterygopalatina?
|

pyramidal space between upper pterygoid process and posterior wall ox maxillary antrum
|
|
|
|
Connections der fossa pterygopalatina?
|
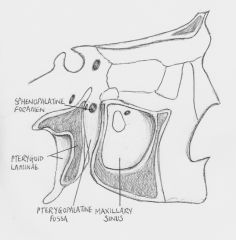
foramen rotundum to middle cranial fossa
sphenopalatine foramen to posterior nasal cavity pterygoid (vidian canal) inferior and lateral to foramen rotundum |
|
|
|
Bedeutung und connection pterygoid canal? (vidian)
|

pterygopalatine fossa and foramen lacerum
(from below) |
|
|
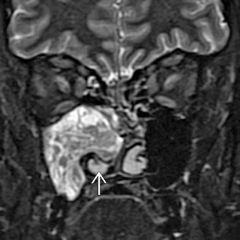
Was ist das?
|
Inverted papilloma
associated with? |
HPV and malignancy
|
|

Was ist das?
|
Esthesioneuroblastoma
fromolfactory epithelial cells extends through cribriform plate |
|
|
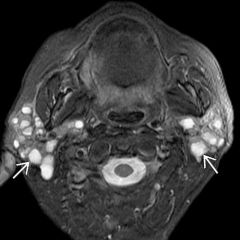
Was ist das?
findings und bei wem? |
Sjögren, autoimmune disease, sicca complex, women
|
|
|
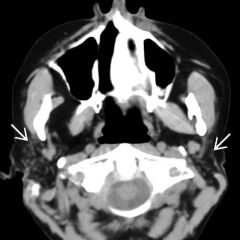
Unterschied zwischen acute und chronic sjögren?
|

multiple small cysts vs. atrophy
(cystic degeneration) microcysts and fatty replacement |
|
|
|
Was ist eine Ranula?
|
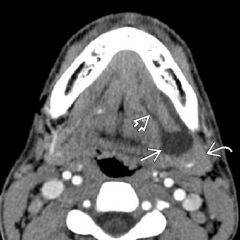
retention cyst from sublingual glands in floor of mouth
|
|
|
|
Was ist eine BLC?
assoziert mit? |

benign lymphoepithelial cyst
HIV, bilateral parotid cysts, can be indistiguishable from sjögren DD warthin tumor |
|
|
|
was ist ein Warthin tumor?
|
cystic tumor benign, bilateral 10%, accumulation of pertechnetate, intermediate signal mass with cystic areas
|
|
|
|
was ist ein Warthin tumor?
|
cystic tumor benign, bilateral 10%, accumulation of pertechnetate, intermediate signal mass with cystic areas
|
|
|
|
Was ist der häufigste maligne Parotis Tumor?
|

Mucoepidermoid carcinoma
dicke enhancende wand |
|
|
|
Was ist der häufigste benigne Parotis Tumor?
|
Pleomorphic adenoma=benignmixed tumor
calcification in a parotid mass is very suggestive of |
|
|
|
Wie sieht ein adenoidcystic carcinoma aus'
|
homogenously enhancing, keine Zysten, 2.häufigster maligner Parotis tumor
|
|
|
|
Woraus besteht die tripod fracture?
|
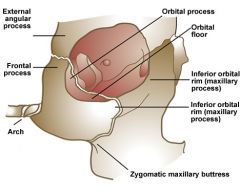
1.laterale orbita wand
2.Orbitaboden 3.arch zygomatic 4zygomaticomaxillary suture/posterolateral wall of maxillary antrum |
|
|
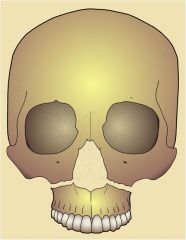
Was ist das?
Wo läuft sie durch? |
separating the caudal maxilla from the midface. The fracture involves all walls of the maxillary sinus and the nasal septum. pterygoid plates are fractured as with all le fort fractures
|
|
|
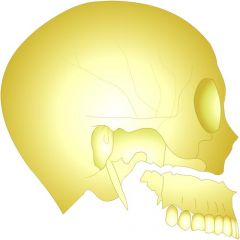
Wo läuft die le fort II durch?
|
pyramidal fracture involving the nasoethmoid region and the orbital floor. The anterior and posterolateral wall of the maxillary sinus are involved
|
|
|
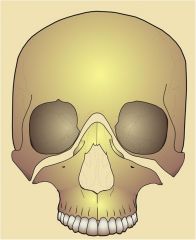
Wie kann man die le fort 3 beschreiben?
|
the medial and lateral orbital walls, most cranial
|
|
|
|
intraconal vs. extraconal
|
intraconal= innerhalb der racti muskeln,
extraconal = ausserhalb |
|
|
Was ist das für eine Erkrankung, warum?
|
Caroli disease, central dot ist pathognomonisch
|
|
|
Was ist das?
|
Desmoid tumor
bei Gardner syndrome encasement of vessels, histologisch benigne |
|
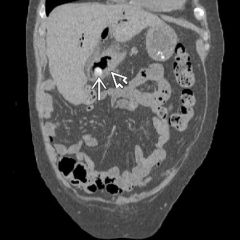
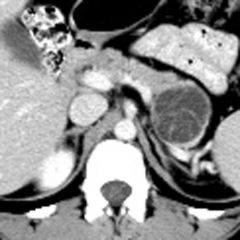
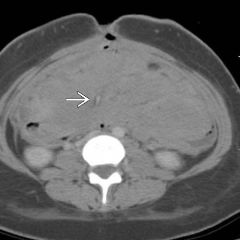
|

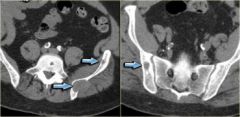
DG?
|

Mucocele of the appendix with characteristic eggshell calcification
|
|
|
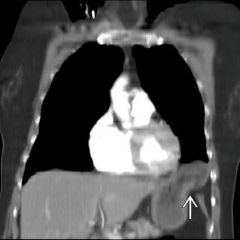
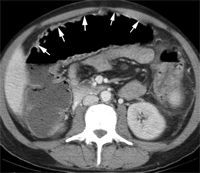
Wie heissen die beiden Zeichen bei traumatic diaphragmatic rupture?
|
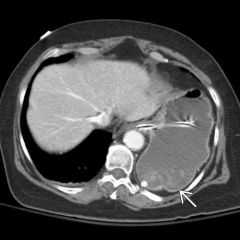
collar sign=einkerbung des magens bei durchtritt durchs zwerchfell
fallen viscus sign magen bzw. dünndarm an hinterer Thoraxwand angrenzend |
|
|

Was ist das? Wieso?
|

typisches late enhancement und fibrose mit einziehungen
|
|
|
Was ist das?
|
radiation colitis
bowel wall edema with hyperenhancement of the mucosa and serosa, as well as low attenuation in the wall of the bowel |
|
|

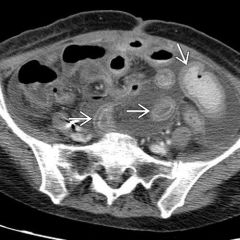
Was ist das beschreiben?
|

Coeliac/Sprue
Intussusception mit intraluminalem Fett Umkehrung der folds jejunal/ileal |
|
|
|
was ist das ogilvie syndrome?
|

colonic pseudoobstruction
dilatiertes colon ohne sichtbare obstruktion meist coecum und ascendens mehr betroffen. obstipation, postoperative |
|
|
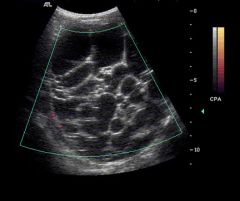
Was isnd das für liver nodules?
|

Liver cirrhosis with regenerative nodules. low attenuation lymph nodes = sarcoidosis
|
|
|
Was sieht man'
|
microabscesses
usually candida bei immunsupprimierten bsp lymphoma oder chemo |
|
|

Was sieht man?
|

massive submucosal edema that is limited to the wall of the ascending colon and cecum, typical of typhlitis or neutropenic colitis.
characteristics? |
Luminal narrowing and wall thickening of the cecum and ascending colon are characteristic of typhlitis. Typhlitis is due to polymicrobial infiltration of the colonic wall.
|
|
|
Welches sind die normalerweise ermittelten Metaboliten der MR Spektroskopie?
|
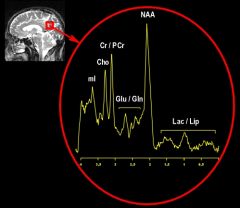
N-acetylaspartate, creatine, choline, lactate
|
|
|
|
was ist die colpocephaly
|
Colpocephaly refers to an abnormal appearance of the ventricular system of the brain in which there is asymmetric dilatation of its lateral ventricle occipital horns, but with normal caliber frontal horns.
|
|
|
|
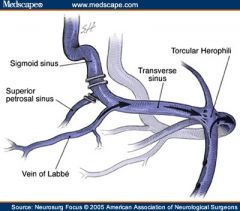
was ist der torcular?
|
|
|
|
|
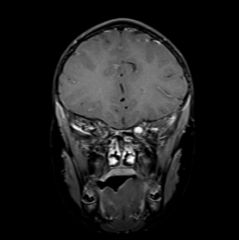
What are the most common lesions of nf1?
|
nf1 spots: high t2 weighted lesins in the globus pallidus, cerebellum, brainstem, capsula interna and thalami
|
|
|
Was ist das?
Was ist bildgebend typisch? |
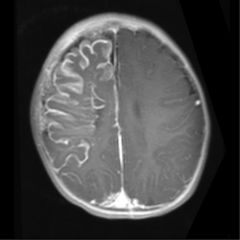
Sturge Weber
Cerebral hemiatrophy with "tram-track" gyral calcification, diffuse pial enhancement, prominence of choroid plexus, buphthalmos, and enhancement of the posterior globe are typical |
|
|
Was ist das? Warum?
|
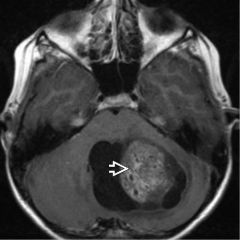
Juvenile pilocytic astrocytoma is a low grade astrocytoma (World Health Organization grade I) and is the most common primary brain tumor in children. The cerebellum is the most common site of origin (60%) with the optic chiasm being the next most frequent site (25%).
|
|
|

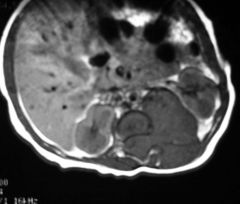
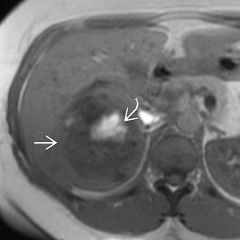
Was ist das ? warum?
|
Hepatoblastoma, häufigster lebertumor newborn häufig verkalkt.
A large, heterogeneous, hypoenhancing solid liver mass in a child less than 5 years of age is very suggestive of hepatoblastoma. Calcifications are seen in up to 50% of cases. |
|
|
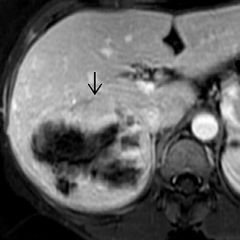
Was ist das ?
|
Hepatoblastoma is the most common pediatric primary hepatic malignancy, peaking in incidence between 1-2 year
|
|
|

Was ist das?
|
Cortical irregularity posteromedial portion of the distal femoral metaphysis, attachment of the medial head of the gastrocnemius muscle. characteristic location and lack of aggressive features on any imaging study should help . bilaterally in 50-100% of cases.
|
|
|
|
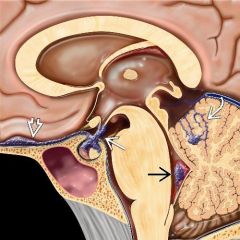
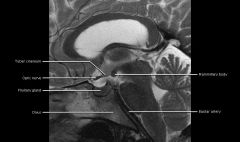
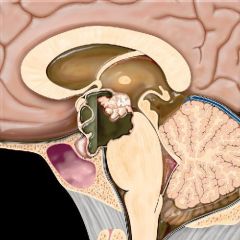
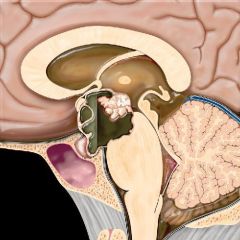
Anatomie Hypophyse sagittal
|
|
|
|
|
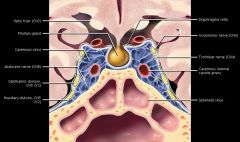
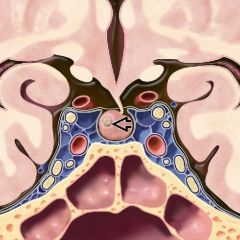
Anatomie Sinus cavernosus
|
|
|
|
|
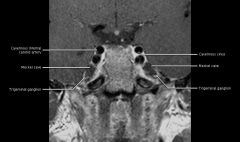
Anatomie Meckel
|
|
|
|
Was ist das?
|
lymphatic malformation
|
|
|
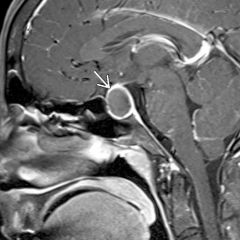
Was ist das?
|
Rathke cleft cyst
|
|
|
|
Wie ist die normale Form der Hypophyse?
Wann bei wem? |
8mm concave male! 6mm kinder
10mm young women childbearing age convex 12mm late pregnancy postparum convex superiorly |
|
|
Was ist das?
Was gibt es dazu zu sagen? |
Macroadenoma
compressive symptoms rare in children und adolescents most common suprasellar mass |
|
|

Was ist das?
|
Invasives Macroadenom
>1000ng/ml invasion des sinus cavernosus Prolactinoma galactorhea, amenorrhea |
|
|

Was ist das?
|
Invasives Macroadenom
>1000ng/ml invasion des sinus cavernosus Prolactinoma galactorhea, amenorrhea |
|
|

Invasive macroadenoma erzählen MR
cavernous invasion |
iso t1 und t2 zu Gray matter
hemorrhage, cystic, extension through diaphragma sella schneemann heterogenes enhancement, encasement of ica, prolactin |
|
|
Microadenoma erzählen
|
kleiner 10mm, lateral enhancen weniger als übrige Hypophyse
|
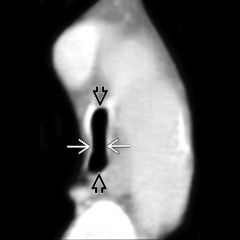
|
|
Mrimaging Microadenoma
|
dynamic phases 10-30% nur dann zu sehen, image every 10-15sec
|
|
|

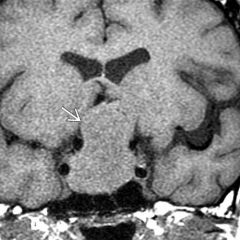
Was ist das?
erzählen |
Tuber cinereum hamartoma
>2jahre, precocoius puberty, M, zwischen infundibular stalk and mamillary bodies signal follows grey matter, no enhancement |
|
|
Was ist das?
|
Craniopharyngioma
bizarre, 90% verkalkt, 90% zystisch, fluid debris levels, 90%enhance, often heterogen |
|
|
craniopharyngioma age und allgenein
|
bimodale age range 5-15 und 50-60, present with mass effect headache, nausea, pituitary dysfunction
|
|
|

charakteristika neurosarkoid
|
klinik lack of adh diabetes insipidus
kann intra- und suprasellär sein |
|
|
|
germinom verteilung
|
60 - 80 % pineal region mass
suprasellar 2.häufigste lokalisation |
|
|
|
germinom synonyme
|
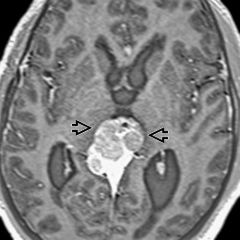
seminom, atypisches teratom, dysgerminom
|
|
|
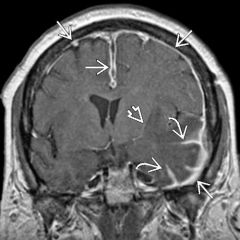
was ist das?
|
sarkoidose
dural and leptomeningeal thickening with enhancement |
|
|

wieso nicht bone infarct?
|
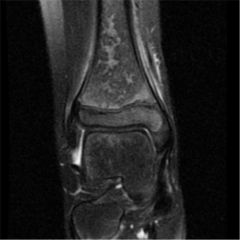
bone infarct is in children selten ohne underlying disease like sickle cell disease
|
|
|

was ist das?
|
apophysitis der rechten anterior superior spina iliaca
adolescents sportlich |
|
|
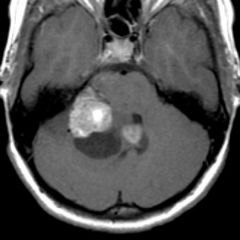
was ist das? reasonable alternative?
|
epenymom, alternative pilocystisches astrocytom
floor of the 4th ventricle. Calcifications, cysts, and hemorrhage |
|
|
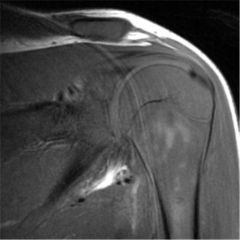
was ist hier nicht in ordnung?
|
bone marrow signal too low, muskuloskeletal leukemia
|
|
|

Was ist das und wieso?
Was ist das nicht? |
Exudative tracheitis
weil tracheawand verdickt. Epiglottitis nicht da es nicht wie ein Daumen aussieht, könnte angeblich Croup sein aber die anamnese passt nicht und die tracheitis auch nicht |
|
|
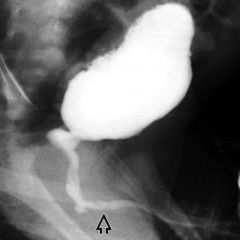
Was ist das?
Charakteristika? |
Posterior urethral valves, häufigste Ursache für bilaterale Hydronephrose, auch unilateral nur boys
VCUG: valve tissue and or abrupt calibersprung |
|
|

Was ist das?
|
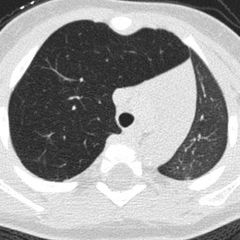
congenital lobar emphysema
Dichte unterschied der Lungen im CT und Überblähung des rechten Oberlappens mit mediastinalshift nach links |
|
|

lung cysts bei Adolescents
1. DD, Charakteristika |
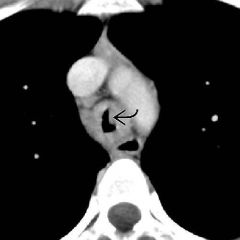
Papillomatosis
HPV, maternale Übertragung, dg vor 5, benigne, lung nodules cavitieren häufig |
|
|

Bilateral lung cysts Dx. Adolescents?
|
Papillomatosis
|
|
|

Alter 14j, diaphyseal, was ist das?
|
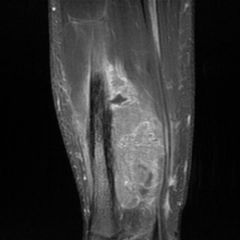
Ewing Sarkom
permeation and remodeling being frequent features. The associated soft tissue mass is frequently out of proportion to the radiographically visible bony findings. |
|
|

Was sieht man?
Was ist das? |
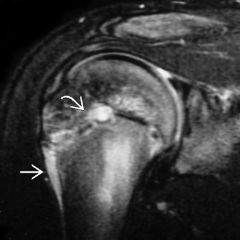
little league shoulder
Salter 1 fracture lateral gap and high signal intensity epiphysär und metaphysär |
|
|
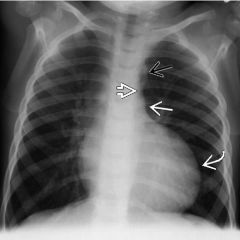
dg, sign?
4j, hypertension |

3 sign aortic coarction, poststenotic dilataion
associated with other cardiovascular abnormalities, especially patent ductus arteriosus (66%), bicuspid aortic valve (50%), ventricular septal defect (33%), and transposition of the great vessels. |
|
|
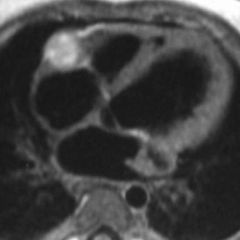
Was ist das?
|
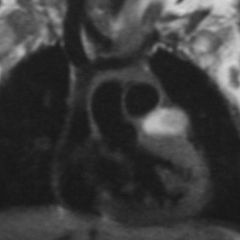
coronary artery aneurysm
kawasai disease thrombus hell in koronararterie koronaraterienaneurysma kinder kawasaki disease vaskulitis der koronarien, idiopathisch, akut myokarditis später das hier |
|
|

was sieht man?
|

Scimitar syndrome, Triad
Partial anomalous pulmonary venous return (PAPVR), hypoplastic right lung, and systemic arterial supply to the right lower lobe which can cause heart failure. |
|
|
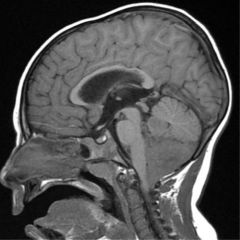
was ist das?
|
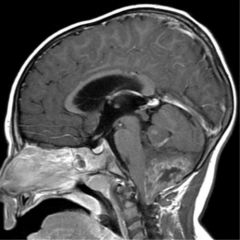
Ependymom
Ependymomas peak during the ages of 1-5 years and have a 60-70% 5-year survival rate. Spine imaging! heterogenous enhancement,classically extends through the outlets of the 4th ventricle (such as the foramen of Magendie, seen here, and the foramina of Luschka) |
|
|
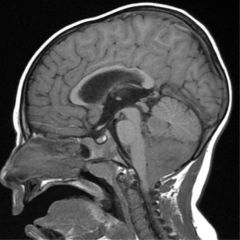
Wieso ist das kein Cpp oder Medulloblastom?
|
may arise in the 4th ventricle of adults, lateral ventricular atria in children. CPP is typically a hyperenhancing, lobulated intraventricular mass with hydrocephalus.
Medulloblastom is in 4th ventricle bt does not extend through foramina of luschkae and is hyperdense on CT. |
|
|

Was ist das?
Charakteristika |
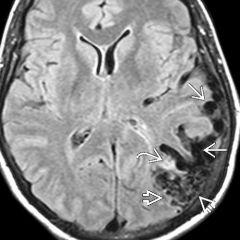
AVM, anywhere
imaging: large feeding artery, nidus, early draining vein bleeding risk 2-4%/Jahr, Spetzler criteria, size, location, venous drainage MRI: bag of worms, flow voids, stark enhancing, blooming n t2*, |
|
|
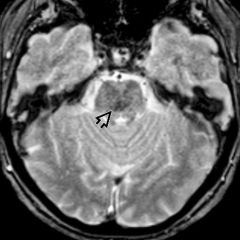
Was ist das Charakteristika?
|
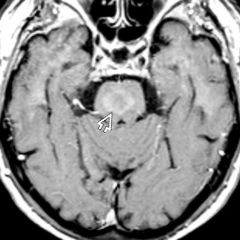
Capillary teleangiectasy
Def. dilated capillaries interspersed with normal brain, asymptomatic, rare blutung, brainstem, pons, T2 hell T2* dunkel, ill defined enhancement, stippled, keine therapie |
|
|
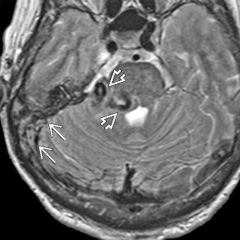
Was ist das?
|
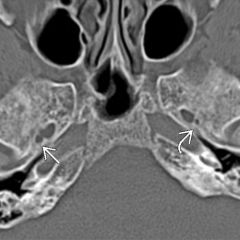
dural AVF
AV shunts in Dura 2 Types: erwachsene kleine Gefässe, Kinde multiple high flow shunts involving several thrombosed sinuses, Grading Cognard most common near skull base, hemorrhage wie avf 2-4%/jahr, cct dural feeders&enlarged dural sinus, MR flow voids, corkscrew, angio multiple feeders, involved sinus often thrombosed, pseudophlebitic pattern |
|
|
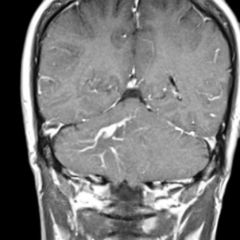
Was ist das, charakteristika?
|
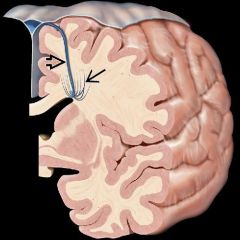
DVA, isolated oder
assoziert mit cavernom häufig, enlarged medullary veins, solitary, hemorrhage unusual, surrounding t2hyperintensity, acute edema in thrombosis, gliosis from chronic outflow obstruction, kein treatment! da venous infarct möglich |
|
|
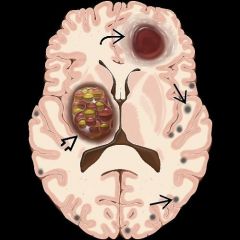
Was ist das und Charakteristika?
|
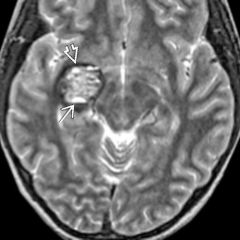
Cavernous malformation
variable sized intercapillary vascular spaces, no intervening brain, 2 types inherited und sporadic, little - no mass effect, hemosiderin black halo, ct verkalkungen, mr popcorn ball, surrounding edema in acute hemorrhage, angio occult |
|
|
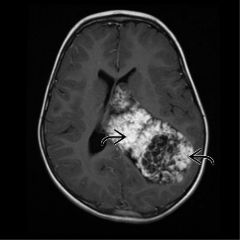
Was ist das?
Charakteristika? |
Choroidplexustumor (papillom und ca nicht unterschiedbar)
Charakteristika: WHO 1, lateral ventriclemost common 4th in boys, multiple sites, hydrocephalus, seeding, BLUMENKOHL, intense enhacement, enlarged choroideal artery, ca WHO 3 necrosis und parenchymal invasion, heterogen, |
|
|
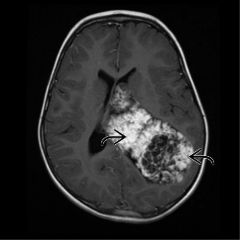
Was ist das?
Charakteristika? |
Choroidplexustumor (papillom und ca nicht unterschiedbar)
Charakteristika: WHO 1, lateral ventriclemost common 4th in boys, multiple sites, hydrocephalus, seeding, BLUMENKOHL, intense enhacement, enlarged choroideal artery, ca WHO 3 necrosis und parenchymal invasion, heterogen, |
|
|

Woraus besteht der Clubfoot?
|

combination of hindfoot varus (decreased talocalcaneal angle of less than 20 degrees on AP and lateral views), hindfoot equinus (increased tibiocalcaneal angle of greater than 90 degrees on lateral view), and forefoot varus (long axis of 1st metatarsal lies medial to long axis of the talus on AP) seen in this case gives the classic talipes equinovarus (or clubfoot)
|
|
|

dg?
|

salter harris 2 with widening of physis and metaphyseal fragment
|
|
|

dg?
|

metaphysäre cornerfracture in 2 ebenen bei child abuse
|
|
|

was ist das?
|
There are 2 major types of right aortic arch: right arch with mirror image branching (where the arch branching pattern is a mirror image of normal) and a right arch with aberrant left subclavian artery (SCA), which is what is shown here.
|
|
|
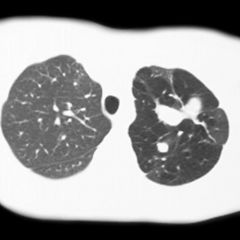
was ist das?
|
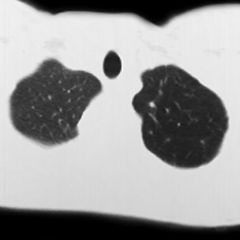
segmental, noncommunicating bronchus filled with mucus. The distal lung segment is hyperlucent and overexpanded.
Well-defined margins and branching configuration to the atretic bronchus, in concert with the distal hyperinflation, is an Aunt Minnie. |
|
|

was ist das?
|

increased perihilar markings and hyperinflation seen in this case are hallmarks of viral lung infection, asthma wäre auch nicht falsch...
|
|
|

was ist die normale Verteilung des congenital lobar emphysema?
|
normally found in the upper (left more than right) and right middle lobes.
|
|
|

was ist das?
unterschied zu |
gastrochisis
omphalocele it sack gastrochisis ohn, keine organe ausserhalb des adomens |
|
|
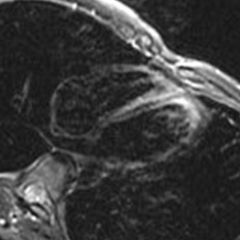
was ist das?
|
MR perfusion images in a patient with myocarditis, there is typically enhancement of the myocardium that spares the subendocardium and does not correspond to a coronary vascular distribution.
|
|
|

Was ist das und wieso?
|
RSV Bronchiolitis
Rx macht man um viral vs. bakteriell zu unterscheiden. Hier typisch für RSV: Consolidation OL und Air trapping, bact consolidation und preferably Pleuraeerguss, bakt ist seltener. |
|
|

Was ist da pathologisch?
|
Diffuse zu helles Knochenmark, an Leukemia denken, wenn keine Speichererkrankung oder chronische Osteomyelitis bekannt ist.
|
|
|
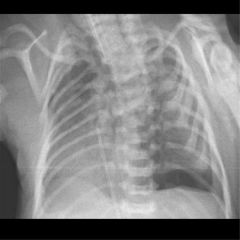
An was muss man denken wenn man das sieht?
History of oliguria. |
Pneu in newborn an pulmonary hypoplasie und oligurie, oligohydramnios denken und an bilaterale renale agenesie!!
|
|
|
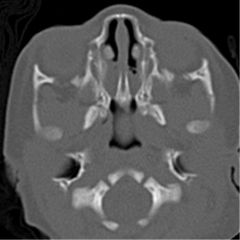
Was ist das?
|
focal and severe bony narrowing of the posterior nasal cavities seen in this case is diagnostic of choanal atresia.
|
|