![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
175 Cards in this Set
- Front
- Back
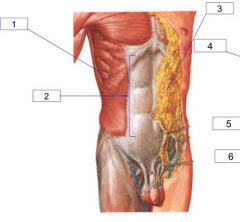
Label 1-3 |
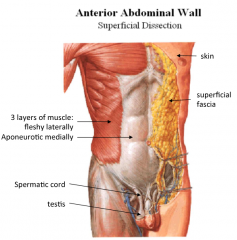
Anterior Abdominal Wall: 1. Muscle Body 2. Aponeurosis 3. Superficial Fascia |
|
![Label =]](https://images.cram.com/images/upload-flashcards/83/15/16/10831516_m.jpg)
Label =] |
A. Rectus Abdominis B. Linea Alba C. External Oblique Muscles D. Internal Oblique Muscles Transversus abdominus deep to IO |
|
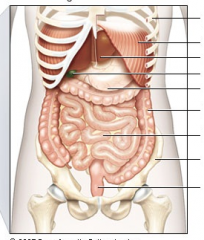
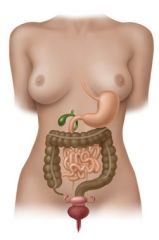
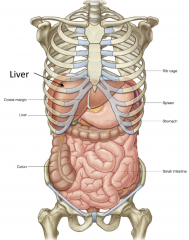
Name the structures from top to bottom |
Top 1. Rib Cage 2. Diaphragm 3. Liver 4. Gall Bladder 5. Stomach 6. Large Intestine 7. Small Intestine 8. Pelvis 9. Rectum Bottom |
|
|
What 6 structures would need to be punctured to reach the abdominal cavity from the anterior end? List from superficial to deep. |
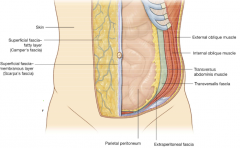
1. Skin 2. Superficial Fascia 3. 3 Layers of anterior abdominal muscle 4. Transversalis Fascia 5. Extraperitoneal Fat 6. Peritoneum (parietal + visceral) |
|
|
What are the 4 muscles of the anterior abdominal wall? How are they arranged in relation to each other? |
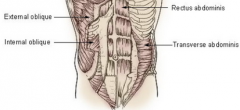
From superficial to deep:
1. External Oblique 2. Internal Oblique 3. Trasversus Abdominus Lieing laterally, within their 'rectus sheath' 4. Rectus Abdominus |
|
|
For the External Oblique Muscles: 1. How are the muscle fibres orientated? 2. What attachments does it have i) Superiorly? ii) Medially? iii) Inferiorly (laterally and medially)? |
1. Inferomedial fibre arrangement ('front pocket') 2. i) Superior = Ribs ii) Medially = Linear Alba iii) Inferolateral = Iliac Crest + Asis Inferomedial = Pubic Tubercle + Pubic Crest |
|
|
What structure do the EO, IO and TA muscles form medially? |
An aponeurosis |
|
|
For the Internal Oblique Muscles: 1. How are the muscle fibres orientated? 2. Where are its origins? 3. Where are its insertions? |
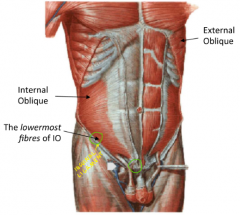
1. Superomedial fibre arrangement (perpendicular to EO) 2. Topmost fibres arise from post. ab wall fascia Lowermost fibres arise from lateral 2/3 of inguinal ligament and arch up 3. Topmost fibres insert on to costal margin Lowermost fibres Insert in the pubic crest via a conjoined tendon |
|
|
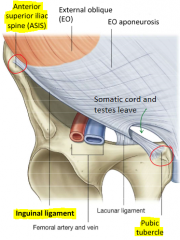
What is the Inguinal Ligament? |
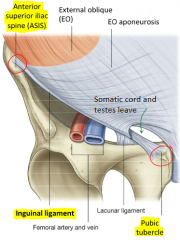
The free, thickened inferior border of the external oblique muscle aponeurosis extending from the ASIS to the pubic tubercle |
|
|
The EO aponeurosis attaches to both the pubic tubercle and pubic crest. This leaves a triangular hole between the aponeurotic attachment points. What structure does this form and what does this allow? |
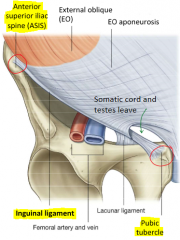
This forms the superficial ring of the inguinal canal which allows passage of the testes and spermatic cord |
|
|
For the Transversus Abdominus Muscle: 1. How are the muscle fibres orientated? 2. Where are its origins? 3. Where are its insertions? |
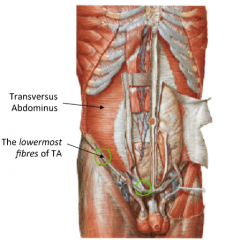
1. Transverse Fibre Arrangement 2. Topmost fibres arise from post. ab wall fascia Lowermost fibres arise from lateral 1/3 of the inguinal ligament and arch up 3. Topmost fibres insert on to costal margin Lowermost fibres Insert in to same conjoined tendon as IO and attach to pubic crest |
|
|
For the Rectus Abdominus Muscle: 1. How are the muscle fibres orientated? 2. Where are its origins? 3. Where are its insertions? 4. What special structural feature does it have and how does this relate to its function? 5. How is it enclosed? |
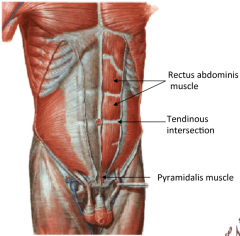
1. Vertical Fibre Arrangement 2. Pubic symphisis and pubic crest origins 3. Xyphoid process and costal cartilage insertions 4. Has tendonous insertions in between to make the muscles short and therefore much stronger whilst still allowing the full length of contraction 5. Enclosed by 'rectus sheath' (within the aponeurosis of the other abdominal muscle) |
|
|
What is the pyramidalis muscle? |
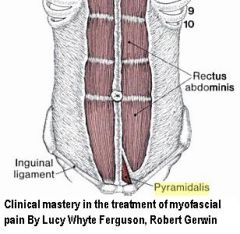
- Small triangular muscle
- Anterior to the rectus abdominis (enclosed in rectus sheath) - Supports ab wall muscle but not a large function |
|
|
How does the rectus sheath enclose the Rectus Abdominus muscle? |
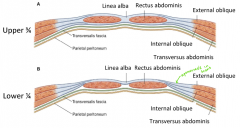
Upper 3/4 of abdomen wall (above arcuate line): - EO aponeurosis anterior - IO bifurcates, one layer anterior, one posterior - TA aponeurosis posterior Lower 1/4 of abdomen wall (below arcuate line): - All aponeuroris anterior |
|
|
How do the testes descend in embryonic development? |
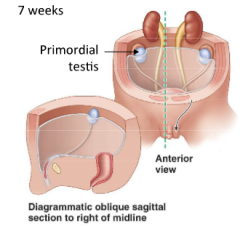
1. Starts high up in posterior ab wall 2. At ~7 months, reaches anterior ab wall, 1/2 way down the inguinal ligament 3. At ~9 months, passes through the layers of the inguinal canal, dragging blood vessels, nerves, duct system and abdominal walls into scrotum |
|
|
An opening of what structure forms the deep inguinal ring? What about the superficial inguinal ring? |
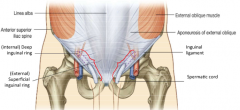
The deep inguinal ring is formed by a circular opening in the transversalis fascia (halfway down inguinal ligament) The superficial inguinal ring is formed by a triangular opening in the aponeurosis of the EO muscle |
|
|
What is the spermatic cord? |
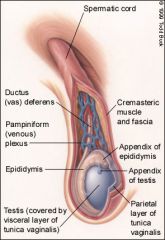
The spermatic cord is the cord like structure composed of the vas deferens + surrounding tissue (i.e. blood vessels, nerves, muscle, fascia) that runs from the deep inguinal ring down to the testicles |
|
|
In regards to the boundaries of the inguinal canal, what forms: 1. The floor? 2. The roof? 3. Anterior wall? 4. Posterior wall? |
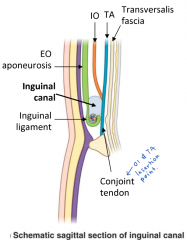
1. Inguinal ligament 2. i) Arch of internal oblique muscle ii) Transversus abdominus 3. i) External oblique aponeurosis ii) Internal oblique muscle (laterally) 4. i) Transversalis fascia ii) Conjoint Tendon (medially) |
|
|
What is an abdominal hernia? What are the 2 types of inguinal hernia? How can they occur? |
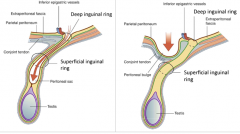
An abdominal hernia is a protrusion of abdominal contents through a defect in the abdominal wall 1. Indirect Inguinal Hernia - Protrusion or passage through the deep ring obliquely into inguinal canal 2. Direct Inguinal Hernia - Protrusion or passage through the posterior wall of the inguinal canal They occur due to high abdominal cavity pressure and weakness in the abdominal wall |
|
|
Which bones form the framework of the abdominal wall? |

L1-5 Vertebra & IV discs 12th ribs |
|
|
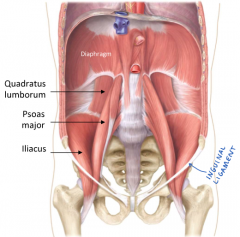
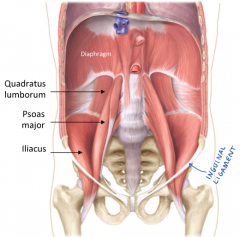
What 3 muscles form the posterior abdominal wall? |
1. Psoas Major 2. Quadratus Lumborum 3. Ilacus *Psoas Minor presence variable in population |
|
|
Where does the Psoas Major originate and insert? What structure does it pass? |
Origin = Lumbar vertebrae transverse processes Insertion = Lesser Trochanter of Femur Passes the inguinal canal inferomedially |
|
|
Where does the Quadratus Lumborum originate and insert? |
Origin = 12th ribs + lumbar transverse processes Insertion = Iliac crest |
|
|
Where does the Iliacus originate and insert? |
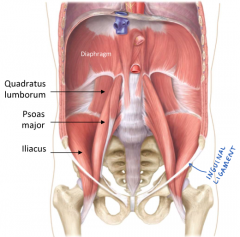
Origin = Iliacus fossa Insertion = Lesser Trochanter of Femur |
|
|
How do the anterior abdominal wall muscles connect with the posterior abdominal wall muscles? |
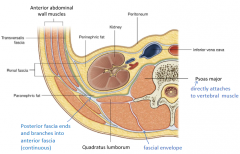
The anterior fascia of the anterior muscles is continuous with the posterior fascia |
|
|
What 5 hollow viscera of the GIT may be found in the abdominal cavity? |
1. Esophagus
2. Stomach 3. Gall Bladder 4. Small Intestine 5. Large Intestine |
|
|
What 3 solid viscera of the GIT may be found in the abdominal cavity? |
1. Liver 2. Spleen 3. Pancreas |
|
|
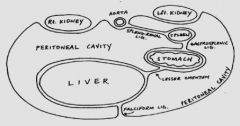
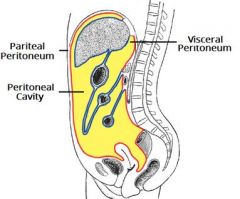
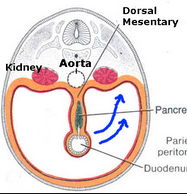
What is the peritoneum and peritoneal cavity? |
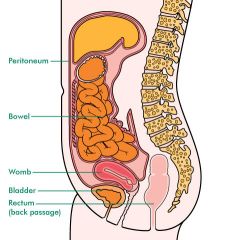
The peritoneum is the serous membrane that lines the structures within the abdominal cavity The peritoneal cavity is the potential space between parietal and visceral layers which contains lubricative serous fluid |
|
|
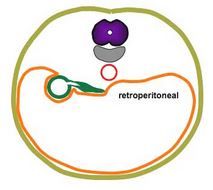
What is the difference between and intraperitoneal and retroperitoneal viscus? |
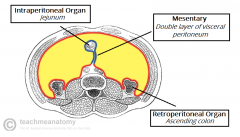
Intraperitoneal = suspended within peritoneal cavity with mesentery (high mobility) e.g. jejunum Retroperitoneal = outside the peritoneal cavity without mesentery (low mobility) e.g. kidney |
|
|
At what vertebral levels does the esophagus start and end? What are the 3 areas the esophagus constricts and for what reason? |
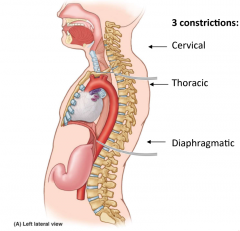
Starts: C6 Ends: T11 Constrictions: 1. C6 = anatomical pharyngeal sphincter 2. T4/5 = constriction due to bronchus division 3. T10 = funcitonal diaphragmatic sphincter |
|
|
Does the esophagus enter the stomach from the left or right? |
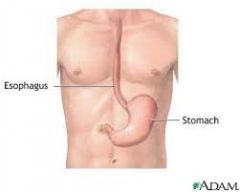
The right |
|
|
Which quadrant is the stomach located in? |
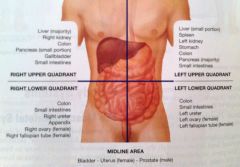
The left upper quadrant |
|
|
Is the stomach intraperitoneal or retroperitoneal? |
Intraperitoneal |
|
|
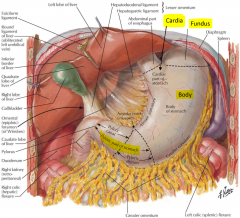
How many orifices does the stomach have, and what are they? How many curvatures does the stomach have, and what are they? |
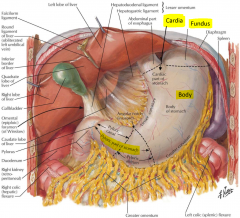
2 Orifices:
1. Cardiac orifice 2. Pyloric orifice 2 Curvatures: 1. Greater curvature 2. Lesser curvature |
|
|
What are the 4 regions of the stomach and where are they? |
1. Cardia - junction of esophagus and stomach 2. Fundus - region above the cardia 3. Body - majority of stomach (centre) 4. Pylorus - junction between stomach and duodenum |
|
|
What 2 regions are the pylorus of the stomach divided in to? Which one is more proximal along the course of the GIT? |
1. Pyloric Antrum 2. Pyloric Canal Antrum is more proximal |
|
|
What surrounds the pyloric orifice? |
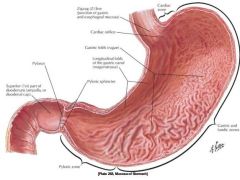
Pyloric sphincter (anatomical) |
|
|
What are the gastric folds of the stomach called? |
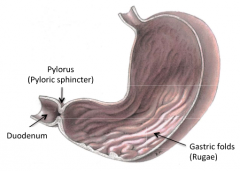
Rugae |
|
|
What are the 3 sections of the small intestine from proximal to distal along the GIT? |
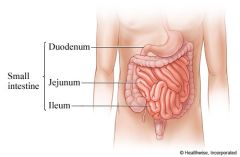
1. Duodenum 2. Jejunum 3. Ileum |
|
|
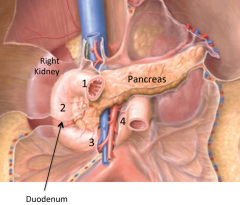
What abdominal viscera does the duodenum surround? |
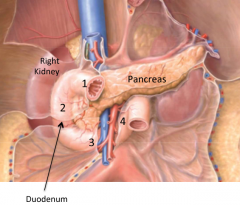
The pancreas (head) |
|
|
Is the duodenum intraperitoneal or retroperitoneal? |
Retroperitoneal |
|
|
What direction does each of the 4 duodenum segments travel? |
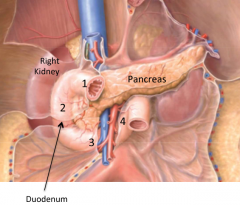
Part 1: Superior & Posterior (against psoas major)
Part 2: Inferior (against medial aspect of right kidney) Part 3: Left Part 4: Superior |
|
|
Which part of the duodenum crosses the midline? At what vertebral level does this occur? |
The 3rd part at L2/L3
|
|
|
Where is the major duodenal papilla found, and what function does it serve? What about the minor? |
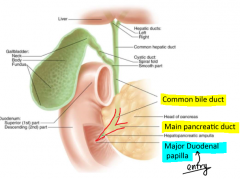
The major duodenal papilla is found on the interior of the 2nd part of the duodenum (same as minor). It allows entry of pancreatic juices (main pancreatic duct) and bile (common bile duct) The minor duodenal papilla serves a similar function however it is negligible, and not all people have it |
|
|
Which abdominal quadrant is the Jejunum located? What about the Ileum? |
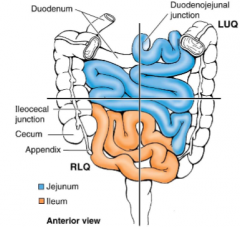
Jejunum = left upper Ileum = right lower |
|
|
What are the 5 differentiating features between the Jejunum and Ileum? What main functional purpose do these differences allow? |

1. Jejunum larger in diameter 2. Jejunum has more mucosal folds (higher SA) 3. Jejunum is more vascular 4. Jejunum mesentery is less fatty 5. Jejunum has thicker walls Allows higher absorption in the jejunum (proximal) |
|
|
What 2 muscle layers does the wall of the small intestine have? Which is internal and which is external? |
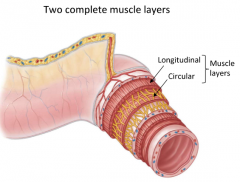
1. Longitudinal (external)
2. Circular (internal) |
|
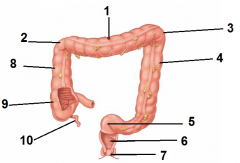
Label (specify whether structures are intraperitoneal/ retroperitoneal where appropriate) |
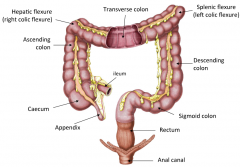
1. Transverse Colon (intraperitoneal) 2. Hepatic Flexure 3. Splenic Flexure 4. Descending Colon (retroperitoneal) 5. Sigmoid Colon (intraperitoneal) 6. Rectum 7. Anus 8. Ascending colon (retroperitoneal) 9. Caecum (intraperitoneal) 10. Appendix (intraperitoneal) |
|
|
What are the 5 differences between the large intestine and the small intestine? Give details |
1. Position
-> LI is on the outside forming a 'frame' around SI 2. Diameter -> LI is much broader 3. Tenia Coli -> 3 longitudinal bands of muscle (incomplete) that run along the length of the LI (except appendix and rectum) in comparison to complete longitudinal muscle layer in SI 4. Haustra -> presence of baggy folds in the LI mucosa formed by inner circular muscle contraction 5. Omental appendicis -> fatty tags specific to LI |
|
|
Where does the large intestine start? |
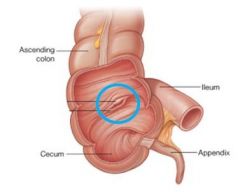
At the ileo-caecal junction |
|
|
In which abdominal quadrant is the caecum located? |
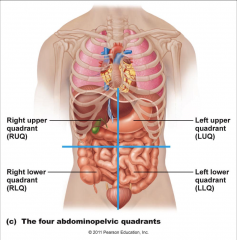
The right lower quadrant |
|
|
Where does the appendix attach? What direction is orientated? |
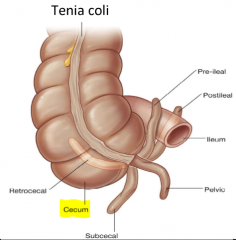
Base of the appendix attaches to the inferior aspect of the caecum where the 3 tenia coli meet Orientation and size of appendix variable between people |
|
|
Are the retroperitoneal or intraperitoneal viscera more mobile and why? |
The intraperitoneal are most mobile as they are just hanging from mesentery whilst the retroperitoneal are fixed to the posterior abdominal wall |
|
|
What 3 structural differences are there between the rectum and the rest of the large intestine? |
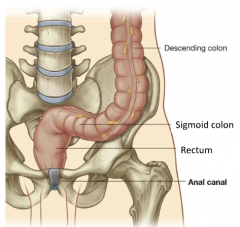
1. No tenia coli 2. No haustra 3. No omental appendicis |
|
|
Which solid viscera is the largest? |
The Liver
|
|
|
What abdominal quadrant is the liver primarily located?
|
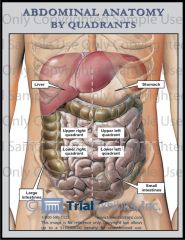
The right upper quadrant
|
|
|
What are the 3 main functions of the liver? |
1. Bile production 2. Blood filtration 3. Metabolism (e.g. glycolysis) |
|
|
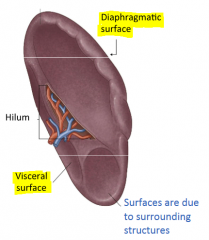
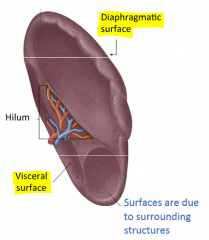
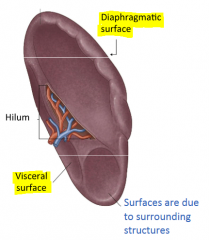
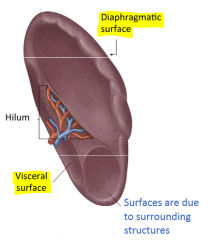
What 2 surfaces does the liver have? In what anatomical plane (i.e. anterior, posterior, superior, inferior) do the surfaces respectively lie? |
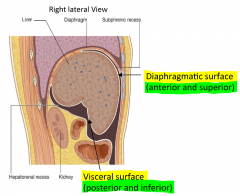
1. Diaphragmatic Surface - Anterior and Superior 2. Visceral Surface - Posterior and Inferior |
|
|
Out of the diaphragmatic or visceral surface of the liver, which one is smooth and which one is concave? |

The diaphragmatic surface is smooth and the visceral is concave |
|
|
Is the right lobe or left lobe of the liver larger? What divides the two? |
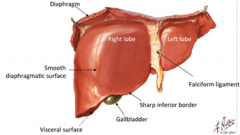
The right lobe is larger, and it is divided from the left lobe by the falciform ligament
|
|
|
Do the gallbladder and IVC sit on the diaphragmatic or visceral surface of the liver? |
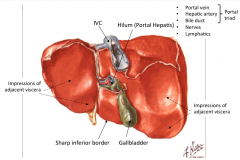
They both sit within grooves of the interior visceral surface
|
|
|
What is the hilum of the liver called? What 5 structures run through the hilum? |
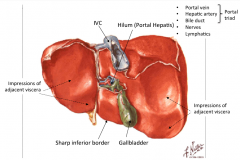
The Portal Hepatis 1. Portal Vein 2. Hepatic Artery 3. Bile Duct 4. Nerves 5. Lymphatics |
|
|
What 3 structures form the portal triad? What are their respective functions? |
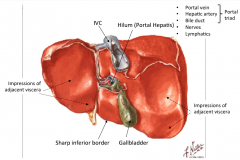
1. Portal Vein - Vascular input which brings venous blood from GIT to liver for metabolism 2. Hepatic Artery - Liver's own blood supply 3. Bile Duct - Dumps bile into duodenum |
|
|
What are the 4 lobes of the liver? |
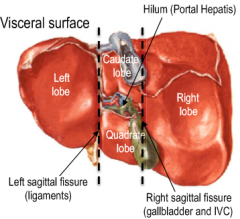
Anatomical Lobes (2):
1. Left Lobe 2. Right Lobe Accessory Lobes (2): 3. Caudate (superior) 4. Quadrate (inferior) |
|
|
In the liver, what separates the quadrate lobe from the caudate lobe? |
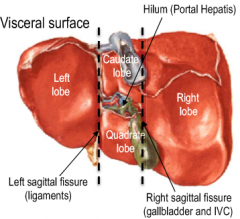
The transverse portal hepatis
|
|
|
In the liver, what separates the anatomical lobes from the accessory lobes? What demarcates these lines of separation? |
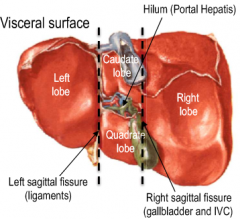
Left lobe separated by left saggital fissure (demarcated by ligaments)
Right lobe separated by right saggital fissure (demarcated by gallbladder and IVC) |
|
|
Is the gallbladder covered by peritoneum? |
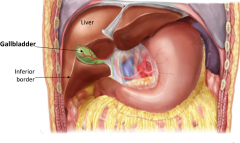
No (does not have mesentery) |
|
|
What is the function of the gallblader? |
Storage of bile |
|
|
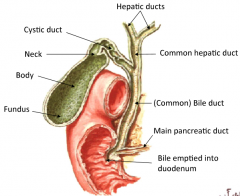
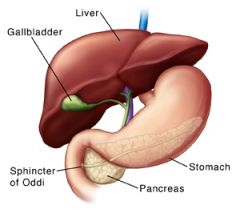
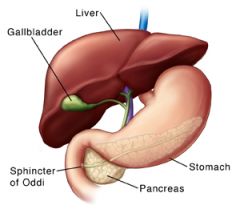
Explain the passage of bile from the liver to duodenum |
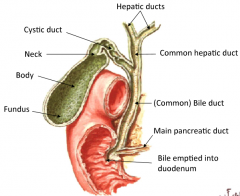
2 Hepatic bile ducts join to form the common hepatic duct The common hepatic duct joins the cystic duct coming from the gallbladder to form the common bile duct The common bile duct then meets with the main pancreatic duct which also empties in to the 2nd part of the duodenum via the major duodenal papilla |
|
|
What anatomical structure regulates the delivery of bile and pancreatic juices in to the duodenum?
What stimulus does this structure respond to? |
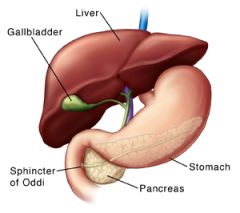
An anatomical sphincter called the spincter of oddi surrounds the major duodenal papilla, regulating delivery in to the duodenum.
Normally constricted, but high fat content in the duodenum causes its relaxation, allowing bile and pancreatic enzymes to enter and digest the fat. |
|
|
What are gallstones and what structure do they typically block? |
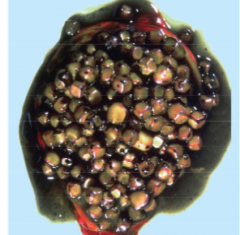
Highly concentrated bile that has crystallised. Usually blocks the cystic duct, causing severe abdominal pains |
|
|
What abdominal quadrant is the pancreas located in? |
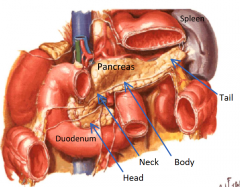
The left upper quadrant |
|
|
What are 2 the general functions of the pancreas? |
1. Endocrine Secretion
-> Insulin & glucagon production and delivery to blood 2. Exocrine Secretion -> Pancreatic enzyme production and delivery via the main pancreatic duct to the major duodenal papilla (also an accessory pancreatic duct that goes to minor duodenal papilla) |
|
|
What is the largest lymphatic organ in the body? |
The Spleen
|
|
|
What abdominal quadrant is the spleen located in? |
The left upper quadrant
|
|
|
What are the 2 surfaces of the spleen and on what surface does the hilum enter? |
1. Diaphragmatic surface 2. Visceral surface Hilum enters via the visceral surface |
|
|
What 2 structures are in the hilum of the spleen? |
1. Splenic artery 2. Splenic vein |
|
|
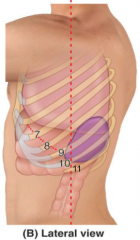
What ribs does the spleen sit in front / lateral to? What clinical significance does this have? |
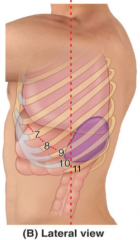
Ribs 9 - 11 on the left side Fracture of these ribs can cause profuse bleeding in to the peritoneal cavity due to the high vascularity of the spleen |
|
|
What is the purpose of the spleen, and how does its anatomy facilitate this? |
It removes old blood cells and also has an important role in immune function. Its large volume and high blood flow facilitates this. |
|
|
What are the 3 types of parietal artery branches (from superior to inferior) of the abdominal aorta? Which ones are paired? What do they respectively supply? |

1. Phrenic Arteries (paired) - supply diaphragm 2. Lumbar Arteries (paired) - supply abdominal wall & spinal cord 3. Median Sacral Artery Branch (unpaired) - supply nothing (vestigial in humans) |
|
|
What are the 3 types of paired visceral artery branches (from superior to inferior) of the abdominal aorta? What do they respectively supply? |

1. Middle Suprarenal Arteries - Supply adrenal gland 2. Renal Arteries - Supply kidneys 3. Testicular/Ovarian Arteries - Supply testicles/ovaries |
|
|
What are the 3 types of unpaired visceral artery branches (from superior to inferior) of the abdominal aorta? What do they respectively supply? |

1. Celiac Trunk - Foregut 2. Superior Mesenteric Artery - Midgut 3. Inferior Mesenteric Artery - Hindgut |
|
|
What structure/region demarcates the start of the foregut? What about the end? |
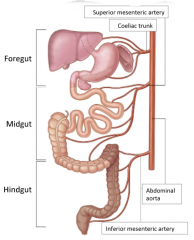
Start = mouth End = major duodenal papilla |
|
|
What structure/region demarcates the start of the midgut? What about the end? |
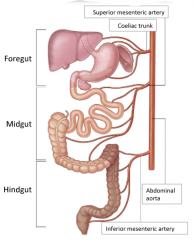
Start = major duodenal papilla End = distal 1/3 of transverse colon (just before the splenic flexure) |
|
|
What structure/region demarcates the start of the midgut? What about the end? |
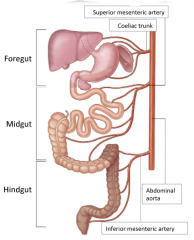
Start = distal 1/3 of transverse colon (just before the splenic flexure) End = anal canal |
|
|
How do the paired viscera of the abdominal cavity drain their blood back in to venous circulation? |
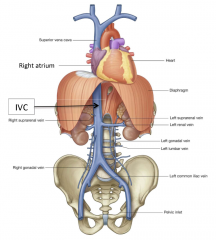
Drain directly in to the IVC
|
|
|
How do the unpaired viscera of the abdominal cavity drain their blood back in to venous circulation? What is the exception? |
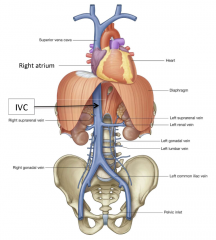
1. Drains blood through portal vein 2. Blood filtered by liver 3. Drains from hepatic vein in to IVC The liver itself is the exception, draining its own blood supply directly to the hepatic vein and then IVC |
|
|
Where are the adrenal glands situated? |
Superior and posterior to the kidneys |
|
|
What are the 4 main structures of the urinary system? |
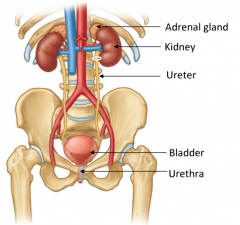
1. Kidneys
2. Ureters 3. Bladder 4. Urethra *adrenal gland is part of endocrine system |
|
|
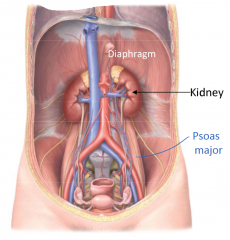
Which kidney sits higher up and why? |
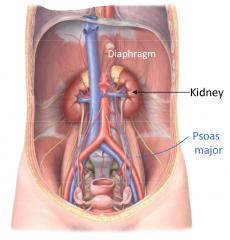
The left kidney sits higher up as it does not have the liver pushing down on it superiorly
(right renal arteries/veins also slightly lower) |
|
|
What shape could the kidney be described as? What is the approximate length of the kidneys? |
Kidneys are described as 'bean shaped' They are roughly 10cm long |
|
|
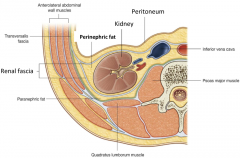
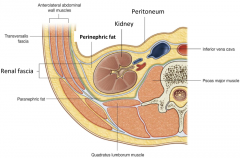
Are the kidneys intraperitoneal or retroperitoneal? |
Retroperitoneal
|
|
|
What 2 structures does the posterior surface of the kidney sit against? |
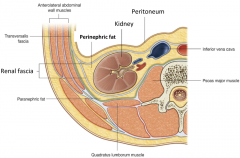
1. Psoas Major Muscle 2. Quadratus Lumborum |
|
|
From what orientation does the hilum of the kidney enter/exit it? |
Enters and exits anteromedially |
|
|
What surrounds the kidney all around, and extends in to the hilum? |
Perinephric fat |
|
|
What does the renal fascia surround? |
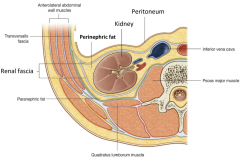
Surrounds the perinephric fat and the kidney deep to it |
|
|
What are the 4 anatomical structures of the kidney (excluding hilum)? |
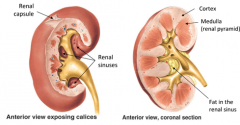
1. Renal capsule - fibrous layer surrounding kidney - darker interior 3. Cortex - paler exterior 4. Renal Sinuses - cavity within hilum filled with perinephric fat |
|
|
Starting at the medulla of the kidneys, explain how urine is excreted from the body |
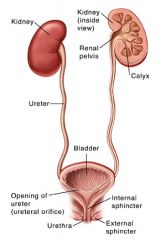
1. Urine collected from apex of the medulla 2. Urine enters a minor calyx (chamber) which join to form major calices 3. Major calices converge to form a renal pelvis which provides a passageway for urine through the renal hilum 4. From the renal pelvis, urine flows through to the ureters 5. Ureters descend down the posterior abdominal wall against the psoas major entering the urinary bladder obliquely via the ureteric orifices 6. From the base of the bladder, urine passes through an internal urethral orifice, passing in to the urethra 7. Urine then exits body via the external urethral orifice |
|
|
What does the abdominal aorta split in to at its terminal end? At what vertebral level does this occur? |
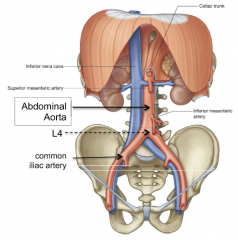
The left and right common iliac arteries At L4 |
|
|
From anterior to posterior, what 3 main structures are in the renal hilum (exclude nerves/lymphatics)? |
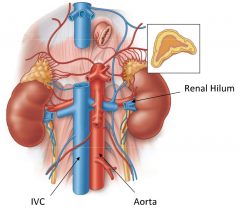
1. Renal vein 2. Renal artery 3. Renal pelvis |
|
|
How many segmental arteries does each renal artery give rise to? What clinical significance does this have? |
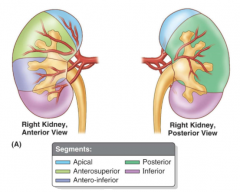
Each renal artery (right & left) gives rise to 5 segmental arteries These each supply their own renal segment meaning if there is pathology associated with a single segment, it can be resected without greatly affecting the others |
|
|
What are the accessory renal arteries? |
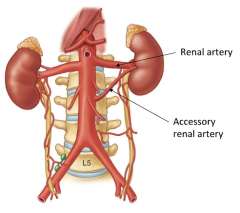
Arteries lower on the abdominal aorta that supplied the kidneys during development, however due to upward migration of the kidney and new blood supply by the actual renal arteries, become redundant and are generally destroyed. |
|
|
Where are the 3 narrowings of the ureter? Which narrowing acts as a functional sphincter, and what purpose does it serve? What clinical significance do the 3 narrowings have? |
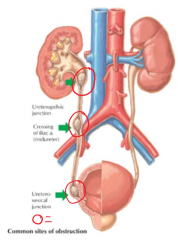
1. Uretopelvic junction 2. Pelvic brim and iliac artery 3. Ureterovesical Junction -> has a functional sphincter which contracts when the bladder expands, stopping urine from flowing backwards These narrowings are often regions of kidney stone lodging |
|
|
What is the name of the triangular region formed by the 2 ureteric orifices and the urethral orifice? |
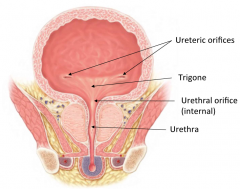
The trigone |
|
|
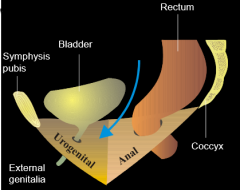
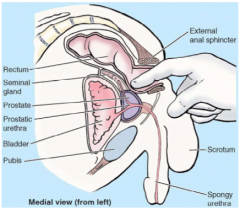
Where does the urinary bladder sit with respect to other pelvic viscera? How does this differ in males/females? |
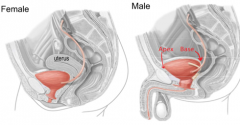
The urinary bladder is a triangular viscus which sits anterior to all other pelvic viscera Its apex (anterior) presses against the pubic bone whereas the base (posterior) presses against the rectum in males and the uterus (also superior) in female |
|
|
Is the bladder freely mobile? |
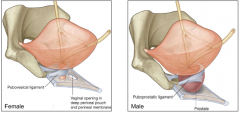
Mostly, however the bladder neck is fixed firmly by ligaments (type differs between sex) which surround the neck and attach to the pubic bones |
|
|
What is the main difference between the male and female urethras? What clinical significance does this have? |
The male urethra is much longer (20cm compared to 4cm) This means males are much less prone to urinary tract infections, however a catheter is harder to insert |
|
|
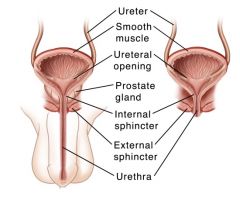
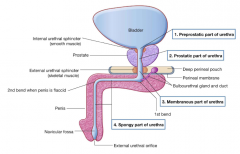
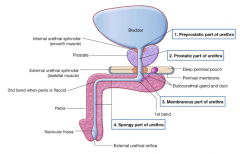
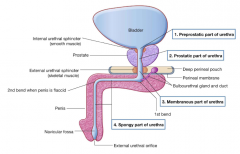
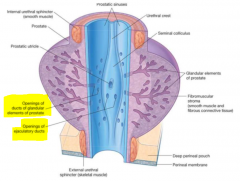
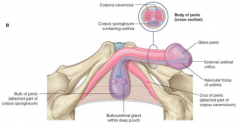
What are the 4 main parts of the male urethra? (list in order from proximal to distal) What is each part surrounded by? |
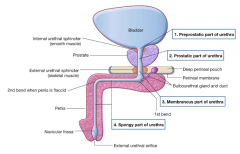
1. Preprostatic part
- surrounded by the internal urethral sphincter 2. Prostatic part - surrounded by prostate 3. Membranous part - surrounded by external urethral sphincter and perineal membrane 4. Spongy part - surrounded by corpus spongiosum |
|
|
Where/when does the spongy part of the penis bend? |
1st bend where it traverses the pelvic floor
2nd bend only when the penis is flacid |
|
|
How many sphincters does the male urethra have and where are they found? |
2 sphincters: 1st is just superior to the prostate 2nd is in the deep perinal pouch |
|
|
What clinical significance does the prostatic part of the urethra have? |
As it is surrounded by the medial lobe of the prostate, benign hypertrophy of the prostate can constrict the urethral pathway, causing pissing difficulty |
|
|
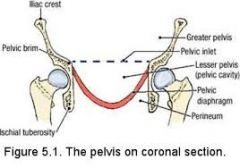
What does the pelvic diaphragm separate? |
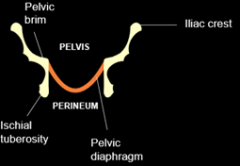
The pelvis and the perineum
|
|
|
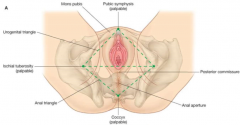
What is the perineum? |
The space inferior to the pelvic diaphragm, between the pubic symphisis (anterior) and the coccyx (posterior)
|
|
|
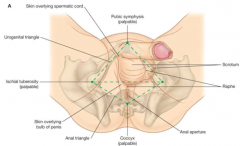
What are the 2 divisions of the perineum? Which one is anterior/posterior? Give examples of structures that can be found in each? |
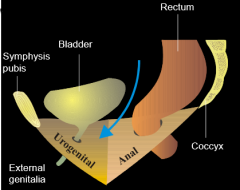
1. Urogenital Triangle (anterior)
- Internal and External Genitalia - Urethra - Associated muscles and structures 2. Anal Triangle (posterior) - Anal canal - Associated muscles and structures |
|
|
What are the 3 main functions of the pelvic diaphragm? |
1. Separates pelvis and perineum 2. Suspends and supports the pelvic viscera 3. Forms site of attachment for external genitalia |
|
|
What 3 muscles are the pelvic diaphragm formed by? Where are their respective origins & insertions? |
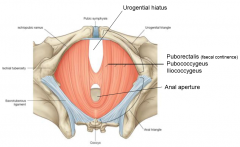
3 Levator Ani muscles: 1. Puborectalis Origin = pubis Insertion = sling posterior to anal aperture 2. Pubococcygeus Origin = pubis Insertion = coccyx 3. Iliococcygeus Origin = Ilium Insertion = coccyx *Origin and insertions are self-explanatory |
|
|
How many openings does the pelvic diaphragm have and what are their names? |
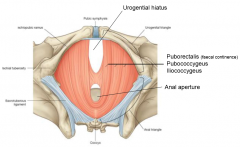
2 openings: 1. Urogenital hiatus (anterior) 2. Anal aperture (posterior) |
|
|
Which levator ani muscle is responsible for faecal continence? How does its structure allow this? |
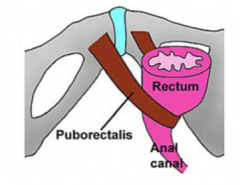
The puborectalis muscle is responsible for faecal continence as it forms a sling around the anal canal, its constriction restricting the passage of faeces.
|
|
|
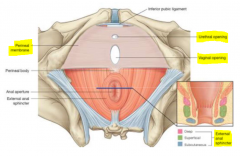
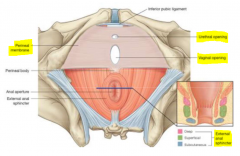
Is the perineal membrane located inferior or superior to the pelvic diaphragm? |
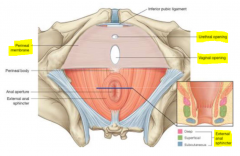
Inferior |
|
|
What region does the perineal membrane cover from above? |
The urogenital triangle |
|
|
What openings does the perineal membrane have in males vs females? |
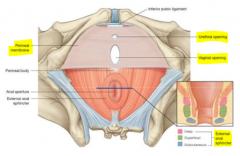
1. Urethral opening (both sexes)
2. Vaginal opening (only females) |
|
|
Where is the perineal membrane attached? |
The pubic arches |
|
|
What is the deep perineal pouch? |
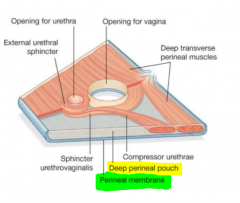
The space above the perineal membrane and below the superior fascia of the urogenital diaphragm
|
|
|
What structures are contained in the deep perineal pouch? |
1. Skeletal muscles that form sphincters around urethra and vagina (females only)
2. Glands (e.g. bulbourethral) 3. Neurovascular structures |
|
|
What main structure is contained in the testes? |
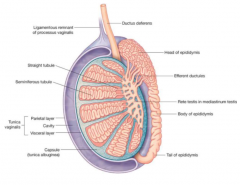
Seminferous tubule network |
|
|
What is the thick connective tissue surrounding the testes called? |
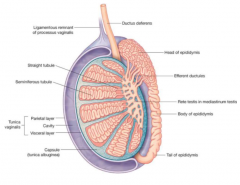
Tunica Albuginea |
|
|
Where are the spermatazoa produced? Where do they mature? |
Produced in the seminieferous tubules and matures in the epididymis (single supercoiled tube) |
|
|
What structure in the testes collects spermatazoa from the seminiferous tubules |
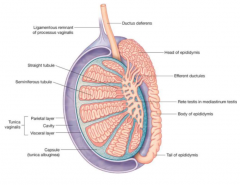
The rete testes |
|
|
Why is the epididymus external to the body? |
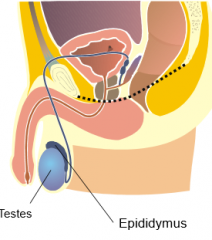
A cooler temperature is needed for spermatazoa to mature
|
|
|
What function does the gubernaculum serve? |
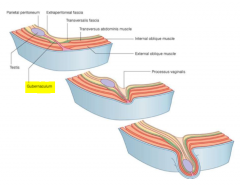
The gubernaculum anchors the testes to the front of what is to become the scrotum. In development, as the scrotum extends downwards, the gubernaculum pulls the testes down with it. |
|
|
What is the vas deferens (or ductus deferens) and what is its function? |
The Vas is a smooth muscular duct which transports spermatazoa from the epididymus to the ejaculatory duct |
|
|
Is penile erection mediated by the SNS or PN? What about ejaculation? |
Erection = PN Ejaculation = SNS parasympathetic pulls the gun out, sympathetic shoots it |
|
|
What is a vasectomy and how is it conducted? |
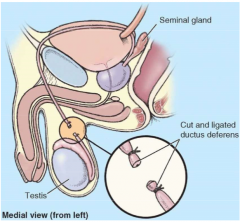
A vasectomy involves severing the vas deferens and then sealing them shut so there is no sperm present in the ejaculate (ejaculatory fluid still present). It is an easy procedure as the vas can be palpated, and a small incision in the scrotum allows access to it. |
|
|
What are the 3 accessory glands that contribute to penile ejaculate? Where are they located? What are their respective contributions to the ejaculate? |
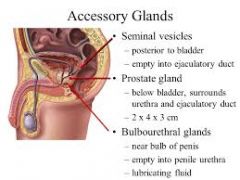
1. Seminal Vesicle - posterior to bladder and anterior to rectum - contributes to volume, provides fructose for sperm energy and excretes a coagulating agent (helps keep semen in vagina) 2. Prostate - inferior to bladder and superior to perineal membrane - contributes to ~20% of volume, activates sperm and secretes white alkaline fluid which protects sperm from acidic vagina 3. Bulborethral gland - in deep perineal pouch, opening in to spongy urethra - Forms the pre-ejaculate which has a mucous type secretion for lubrication |
|
|
How does the prostate add its contribution to the urthera? |
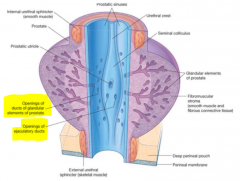
There are multiple ducts within the prostatic portion of the urethra which the prostate can directly secrete its contents in to |
|
|
How do the seminal vesicles add their contributions to the urethra? |
Seminal vesicles have excretory ducts which join the vas deferens to form the ejaculatory duct. This pierces the prostate then opens in to the urethra via 2 ejaculatory ducts. |
|
|
How do the bulbourethral glands add their contributions to the urethra? |
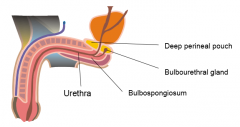
The bulbourethral gland opens in to the spongy part of the urethra |
|
|
What is benign prostatic hypertrophy?
|
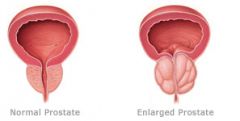
A disease, occuring mostly in old fellas where swelling of the prostate causes urethral compression and blockage, leading to failure to excrete ejaculate and to urinate
|
|
|
How can prostate cancer be diagnosed? |
Via a digital rectal exam (DRE) - someone shoves a finger up your pooper to palpate the prostate which is thickened and feels 'rock hard' if you've got cancer |
|
|
What 2 structures form the attachment points for the roots of the penis? |
1. Perineal membrane 2. Pubic arch |
|
|
What erectile tissues are found in the penis? |
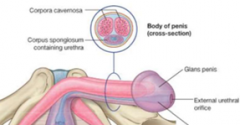
2 corpora cavernosa 1 corpus spongiosum |
|
|
What is the glans penis? |
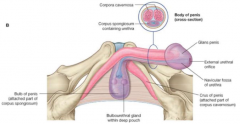
The distal expansion of the corpus spongiosum |
|
|
What is found within the corpus spongiosum? |
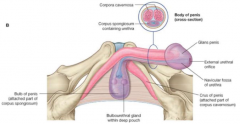
The urethra which terminates at the glans penis, ending as an external urethral orifice |
|
|
What happens during erection? What 2 muscles facilitate this, and how so? Is this different in males and females? |
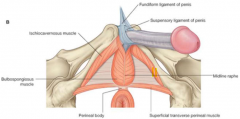
The PN causes relaxation of arteries within the penis, causing blood to flood the erectile tissue. 1. Ischiocavernosus Muscle 2. Bulbospongiosus Muscle These muscles serve to move blood from the root of the penis into the body, and constrict venous drainage of the blood. Similar process in females but the muscles push blood in to glans clitoris. |
|
|
What is the scrotum raphe? |
The fusion of scrotum skin in the midline, which forms a pouch |
|
|
What is the homologue of the scrotum in females? |
The labia majora |
|
|
What is the skin over the glans penis called? |
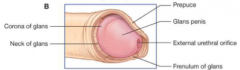
The prepuce of penis
|
|
|
What is the frenulum of prepuce of penis? |
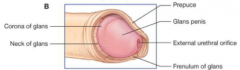
The elastic band of tissue at the back of the penis which connects the mucosa of the glans with the foreskin |
|
|
What 3 main structures are commonly damaged during child birth? What clinical symptoms develop as a result of this damage? |
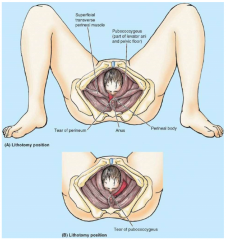
Structures of the pelvic floor:
1. Perineum 2. Levator Ani (pubococcygeus and puborectalis often torn) 3. Perineal Fascia *deep perineal pouch muscles can also be damaged Can cause urinary stress incontence, faecal incontinence and prolapse of uterus as the muscles support the uterus, vagina and rectum |
|
|
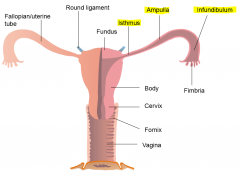
What is the uterus? |
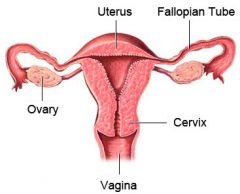
A thick walled, muscular organ that facilitates embryo and fetus develpoment.
|
|
|
What is the endometrium? |
The mucous membrane that lines the internal surface of the uterus, supporting pregnancy and shedding if conception does not occur during the menstrual cycle |
|
|
What are the 3 sections of the uterus? (list from superior to inferior) In which section is the uterus best supported and why is this? |
1. Fundus 2. Body 3. Cervix Best supported at the cervix as there are a number of ligaments on the lateral sides anchoring in place |
|
|
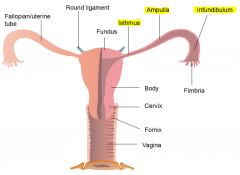
What are the 3 sections of the fallopian tube? (list by closest from ovary, to furthest from ovary) |
1. Infundibulum 2. Ampulla 3. Isthmus |
|
|
What special structures does the infindibulum of the fallopian tube have, and what purpose do they serve? |
They have fimbria which sweep the ovary (unattached to fallopian tube), sucking the oocyte up |
|
|
What is the vaginal fornix? |
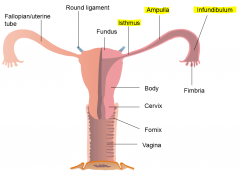
An extension of the vagina (lateral and posterior) near the cervix of the uterus |
|
|
What are the 3 functions of the vagina? |
Serves a thick walled, muscular passage for: 1. Menses 2. Babies 3. Penis/ejaculate |
|
|
What 2 bends does the uterus have? What is the purpose of these bends, and what happens when they are abnormal? |

1. Anteversion (AV) - 1st forward bend (~ 90 Deg relative to vagina) 2. Anteflexion (AF) - 2nd bend (bends over uterus) The bends allow the uterus to lie over the bladder which gives support to it inferiorly. In the case of retroversion (bends oppositely), an increase in pelvic pressure can cause vagina to prolapse as it is no longer supported by the bladder. |
|
|
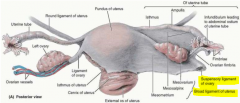
Where are the ovaries located? How are they attached to the uterus? |
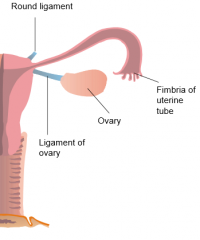
Ovaries are found in the peritoneal cavity, adjacent to the lateral wall of the pelvis and posterior to the broad ligament
They are attached to the uterus via the ligament of ovary |
|
|
What artery supplies the:
1. Ovarian vessels? 2. Uterine vessels? 3. Vaginal vessels? |
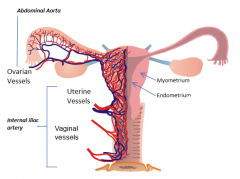
1. Abdominal aorta 2. Internal iliac artery 3. Internal iliac artery |
|
|
Do vessels of the ovary, uterus and vagina anastamose with each other?
|
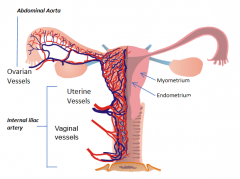
Yep |
|
|
In what structure does fertilization usually occur?
What about implantation? |
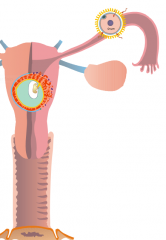
Fertilization typically in the ampulla of the fallopian tubes and implants in the body of the uterus.
|
|
|
What's an ectopic pregnancy? What clinical significance do ectopic pregnancies have? |
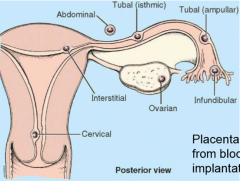
Ectopic pregnancy is when an embryo implants somewhere other than the uterus
The area of implantation may be too small to house the developing fetus (e.g. fallopian tube) or it may not have the high vascular supply needed (e.g. abdomen) |
|
|
Does the peritoneum cover the pelvic viscera superiorly or inferiorly? |
Superiorly (like a sheet that's been draped over the pelvic viscera) |
|
|
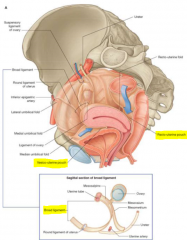
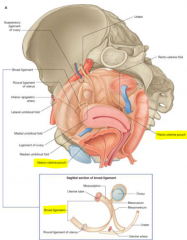
What is the broad ligament of the uterus?
|
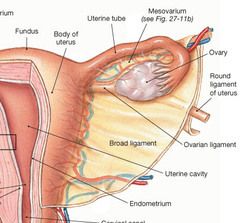
When the peritoneum is 'draped' over the uterus, it forms 1 sheath anteriorly and 1 sheath posteriorly. These 2 sheaths fuse to form a double sheath called the 'broad ligament' which encloses the other structures and connects the sides of the uterus to pelvic wall and floor. |
|
|
What is the only pelvic viscus which is intraperitoneal? |
The ovaries |
|
|
What is the suspensory ligament of the ovary formed by? |
The ovarian vessels and the layer of peritoneum surrounding them |
|
|
What 2 pouches are formed by the peritoneum coverings of the pelvic viscera? |
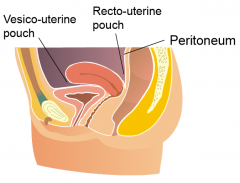
1. Recto-uterine pouch
2. Vesico-uterine pouch |
|
|
What is the clinical significance of the recto-uterine pouch? |
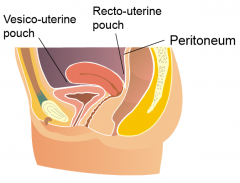
Also known as the pouch of douglas, the recto-uterine pouch is the most inferior projection of the peritoneal cavity in the female, and is thus prone to fluid accumulation when bed ridden |
|
|
What 2 structures form the points of attachment for the roots of the external female genitalia? |
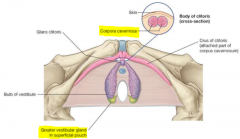
1. Perineal membrane 2. Pubic arch |
|
|
What erectile tissues are found in the female external genitalia? |
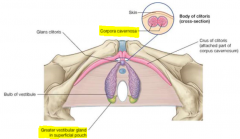
2 Corpora cavernosa
2 Bulbs of vestibule Glans clitoris (in between) |
|
|
What are the bulbs of vestibule homolagous to in the male? |
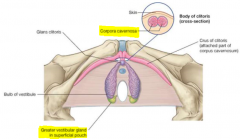
The corpus spongiosum |
|
|
What is the glans clitoris homologous to in the male? |
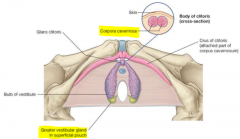
The glans penis |
|
|
What are the greater vestibular glands? Where are they located? What is their function? |
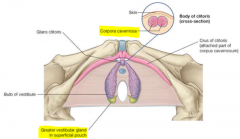
Two glands that are located posterior to the bulbs of vestibule, to the left and right of the vaginal opening which secrete lubricative mucous during arousal |
|
|
What is the vulva? |
The external genitalia of females, including the erectile tissues and overlying skin
|
|
|
What are the labia? What is the difference between the labia minora and major? |

Folds of skin over the vagina. Minora is thinner, more vascular (pink) and comes together anteriorly at the glans clitoris Majora is thicker, more fatty and runs lateral to the minora, folding over the bulbs of vestibule |