Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
|
Five Essential Components of the Labor and Delivery Process (The Five P's)
|
-Passageway (Birth Canal)
-Passengers (Fetus and Placenta) -Powers (Uterine Contractions) -Position of the Mother -Psychological Response |
|
|
PASSAGEWAY
|
-Mother's bony pelvis
-Soft tissues (Cervix, Pelvic Floor, Vagina, and Introitus) |
|
|
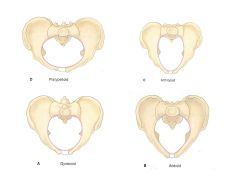
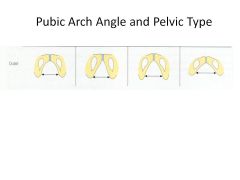
1. Gynecoid rounded inlet (typical female inlet)
•50% of female •All diameters are adequate for child birth 2. Android heart-shaped inlet (typical male inlet) •20% of female •Not all diameter are adequate for child birth 3. Anthropoid oval inlet (“apelike” pelvis) •Usually adequate for child birth 4. Platypelloid flat tranverse oval inlet (female pelvis) Not adequate for child birth Clients usually have features of two or more pelvic types. |
|
|
The bony pelvis is divided into two parts:
|
1. False Pelvis - The flaring part above the brim or inlet. (nothing to do with child birth)
2. True Pelvis - Bony canal through which the fetus must pass. |
|
True pelvis is divided into three parts:
|
|
|
|
Inlet
|
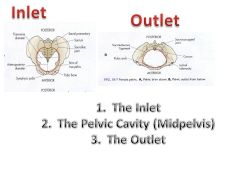
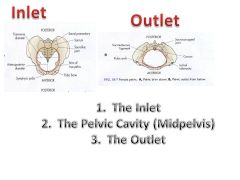
The Inlet - Upper boundary of the true pelvis
- A ridge or brim Continuous from the sacral promontory and extending along the ilium on each side in a circular fashion |
|
|
Pelvic Cavity
|
Pelvic Cavity - The area between the inlet and the outlet.
- A curved passage - Has a short anterior wall and much longer concaved posterior wall. Boundaries: - Posterior aspect of the symphysis pubis. - The ischium - A portion of the ilium, the sacrum, and the coccyx. Varying diameters with the upper portion cylindrical and lower portion curved. |
|
|
Outlet
|
The Outlet - Lower boundary of the true pelvis.
- Diamond-shaped. Boundaries: - In the back by the coccyx. - On the sides by the ischial tuberosities. - In the front by the inferior aspect of the symphysis pubis. |
|
|
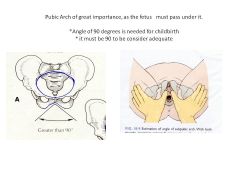
Childbirth process centers on the safe passage of the fetus through the pelvis.
|
Childbirth process centers on the safe passage of the fetus through the pelvis.
|
|
|
Internal pelvic measurements are a means of estimating the size of the pelvis.
|
Internal pelvic measurements are a means of estimating the size of the pelvis.
|
|
|
Inlet diameters
|
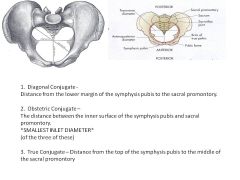
1. Anteriorposterior - the distance from the symphysis pubis to the sacrum.
Shortest Inlet Diameter |
|
|
Three different measurements:
Inlet diameters |
|
|
|
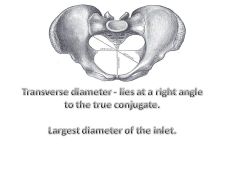
Transverse diameter
|
|
|
|
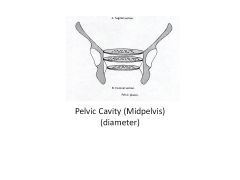
Has varying diameters
(upper) Largest: "Plane of greatest dimensions" (lower) Smallest:"Plane of least dimensions" Interspinous diameter (Transverse diameter) - the distance between the ischial spines. SMALLEST PELVIC DIAMETER *out all the diameters *where the rest of labor is, baby can not fit and must change position |
|

|

|
|
|
ischial tuberosities
|
The ischial tuberosities come closer together with the narrowing of the pubic arch -> transverse diameter is shorter.
|
|
|
|
|
|
Maternal pelvis is affected by the hormone
|
Maternal pelvis is affected by the hormone relaxin (secreted by the placenta).
•The presence of relaxin relaxes the pelvis -> slight increase in the pelvic diameters. During labor, the pelvic diameters can increase with positioning ie: squatting or lateral sims position |
|
|
SOFT TISSUES:Cervix
(EFFACEMENT) |
Effacement –the shorting and thinning of the cervix during the first stage of labor
•Described as a percentage, ranging from "0" (noneffaced and thick) to "100%" (fully effaced and paper thin). •Fully effaced - Uterine neck is obliterated and the cervix becomes continuous with the lower uterine segment. |
|
|
SOFT TISSUES:Cervix
(DILATION) |
Dilation – is enlargement or widening of cervical opening and that occurs Once labor has begun (must be 10cm)
|
|
|
Pelvic Floor & Vagina
|
Pelvic Floor (muscle layer that separates the pelvic cavity from the perineal space below).
•Helps the fetus rotate anteriorly as it passes through the birth canal. Vagina - composed of rugae or folds of vagina mucosa-> allows distention to permit fetus to pass through to external environment. |
|
|
THE PASSENGER
|
The fetal head has the major effect on the birth process r/t its size and rigidity.
Fetal head bones: 2 frontal bones; 2 parietal bones; 2 temporal bones; and 1 occipital bone. |
|
|
THE PASSENGER
Bones are united by membranous sutures: |

|
|
|
At the intersections of the sutures are enlarged soft spots termed "fontanelles"
|
Anterior fontanelle (aka BREGMA).
*diamond shape:1-6cm *close by 16-18 months *sagittal and coronal Posterior fontanelle *triangle shape: 1-2cm *close by 2 months *sagittal and lamboidal Since the sutures are not firmly united -> overlapping of the bones "Molding" is permitted in L&D. - Molding of the sagittal and coronal sutures can be palpated at birth. - Frontal bones fused -> are not molding. |
|
|
Areas of the fetal head: Divided into five areas.
|

|
|
|
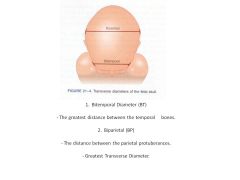
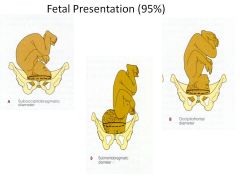
Diameters of the fetal skull:
Four Anteroposterior Diameters |

|
|
|
Diameters of the fetal skull:
Two Transverse Diameters |
|
|
|
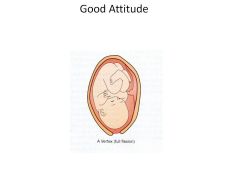
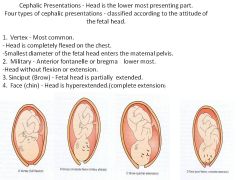
Fetal Attitude – the relationship of the fetal parts to another
•Describes the Degree of Flexion that the fetus assumes. Good Attitude - Fetus completely flexed. •Spinal column bowed forward. •Head flexed forward, so that chin touches sternum •Arms flexed and folded on chest. •Thighs flexed onto the abd. •Calves pressed against the posterior aspect of the thighs. •This position helps the fetus present the smallest anteriorposterior diameter of the skull to the pelvis. |
|
|
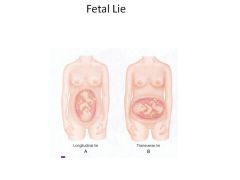
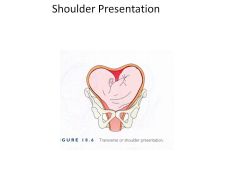
Fetal Lie – the relationship of the long axis of the fetus to the long axis of the mother
Two types of Lies 1. Longitudinal Lie (Vertical)- parallel to the mother spine 2. Transverse Lie (Horizontal)- perpendicular to the mother spine |
|
|
Fetal Presentation
Presentation – the part of the fetus that lie closest to the true pelvis or has enter the true pelvis This part of the fetal body is termed the "Presenting Part". (the part that come out first) Three types of fetal presentations: Cephalic; Breech; and Shoulder. |
|
|
Fetal Presentation: Cephalic
(95% Cephalic Presentation) |
|
|
|
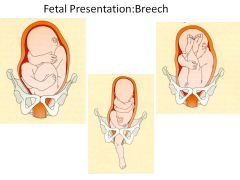
Breech Presentation (Breech = Buttocks)
Occurs @ 3% of term births. Three types - Classified according to the attitude of the fetal hips and knees. 1. Complete Breech - Fetal knees and hips both flexed, placing the thighs on the abd. - Calves on the posterior aspect of the thighs. 2. Frank Breech - Flexion of the hips and extension of the knees. - Fetal Legs extend onto the abd and chest. - Buttocks alone presenting part. 3. Footling Breech - Extension of the hip &/or knee. - One (single) or two (double) feet or knees have prolapsed lower than the buttocks. |
|
|
1% of babies, transverse lie
|
|
|
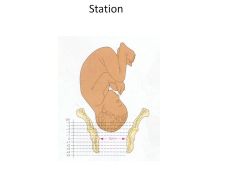
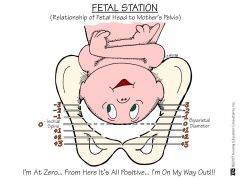
the relationship of the presenting part to the level of the ischials spine
- Level of the ischial spines = 0 station. - Above the spines = minus station in cms. - Below the spines = plus station in cms. |
|
|
Presenting part High
-4"Floating" -3"Dipping" -2"Fixed but not 1engaged" -1"Fixed but not 1engaged" At the Ischial spines 0"Engagement" Presenting part low +1"Engagement" +2"Engagement" +3"On the pelvic floor" +4"Bulging on the perineum" |
|

|
Position- the relationship of the presenting part to a specific quadrant in the mother's pelvis
|
|
|
Fetal Reference Points
|
Fetal Reference Points:
O = Occiput M = Mentum S = Sacrum |
|
|
What is the presenting part?
|
cephalic, breech, shoulder
|
|
|
What is fetal reference point of the presenting part?
|
occiput, mentum, sacrum
|
|
|
Is the fetal reference on the mother's right or left side?
|
Right/left
|
|
|
where in the pelvis is the fetal reference point?
|
anterior, posterior, transverse
|
|
|
Powers
|
Powers - Involuntary and voluntary contractions (cxs) combine to expel the fetus and placenta out of the uterus.
|
|
|
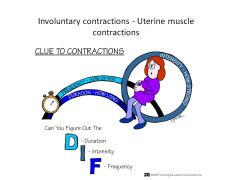
Involuntary cxs - Uterine muscle contractions
•A cx begins as a result of "pacemaker" action in the myometrial cells near the right or left uterotubal junction. •From the pacemaker point, cx moves downward over the uterus in waves. •Uterine cxs are rhythmic, but intermittent.Period of relaxation: - allows the uterine muscles to rest. - provides rest for the laboring mother. - restores uteroplacental circulation. - restores adequate circulation in uterine blood vessels. |
|
|
Cxs of the uterine muscle causes the uterus to become divided into an upper and lower portion.
|
Upper segment - Active contractile portion.
Lower segment-passive |
|
|
Upper segment
|
Upper segment - Active contractile portion.
- Its function is to expel the uterine contents. - It displays a decreasing gradient of intensity of cx from the fundus downward. |
|
|
Lower segment
|
As labor progresses a passive lower segment develops.
Muscle fibers of the upper segment retract -> becoming shorter and thicker as the fetus descends. Muscle fibers of the lower segment stretch and become thinner. Creates distinct boundary -> termed "Physiological Retraction Ring". |
|
|
Force of Contrations
|
The force generated by each cx is applied to the
uterine contents. The presenting part is pushed downward into the cervix each time the uterus contracts,. The upper segment pulls the lower segment -> dilating the cervix. Completely dilated -> permits fetal passage |
|
|
Characteristics of Cxs:
|
Characteristics of Cxs:
1. Frequency-the time of the beginning one contractions to the beginning of the next contrations in (minutes) 2. Duration- the length of the contraction in (seconds) 3. Intensity-the strength of the contraction |
|
|
Voluntary Contractions
|
Voluntary Contractions - Bearing down effort (pushing).
After full dilation has occurred, mother contracts her diaphragm and abd muscles with the uterine cxs. Pushing increases the intraabdominal pressure -> Pressure compresses the uterus on all sides -> this pressure Pushes out the contents of the birth canal. |
|
|
Position of the Mother - Can affect the frequency and intensity of cx's.
Supine - Cxs less intense, but more frequent. Lateral - Cxs more intense, but less frequent. |
|
|
Upright (standing, walking, or squatting) - uses gravity to assist with the descent of the fetus.
Cxs stronger and more efficient in effacing and dilating -> shorter labors. Lower incidence of umbilical cord compression. Increase cardiac output of women -> increase in blood to uteroplacental unit. Reduces compression on the maternal vessels. Squatting - moves the uterus forward -> straightening the long axis of the birth canal. With sitting or squatting - abd muscles work in greater synchronicity with the uterine cxs during pushing. |
|
|
Mechanisms of Labor
|
The fetus must make seven cardinal movements to be born.
Occur in the vertex presentation. Cardinal movements are: Engagement; Descent; Flexion; Internal Rotation; Extension; External Rotation(Restitution); and Expulsion. This movements present the smallest possible diameter of the presenting part to the irregular shape of the pelvic canal -> least resistance is encountered. As these cardinal movements occur, uterine cxs are bringing about modifications in the attitude of the fetus. |
|
|
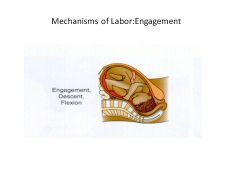
Engagement - The largest section of the presenting part (Biparietal diameter) has passed the pelvic inlet and entered the true pelvis.
•Top of the head level with the ischial spines. |
|
|
Mechanisms of Labor:Descent
|
Descent:The process of the presenting part through the pelvis.
- Continuous downward movement. - Begins with engagement and continues until the birth of the baby. |
|
|
Mechanisms of Labor:Flexion
|
Flexion
As fetus descends -> meets resistance from the: - soft tissues of the pelvis - muscles of the pelvic floor - cervix This causes the fetal head to bend forward -> so that the fetal chin is brought into contact with the chest. Flexion permits the smallest anteroposterior diameter of the head to be presented to the outlet. |
|
|
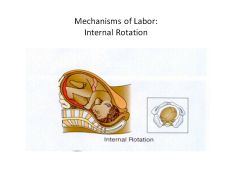
Internal Rotation
Maternal pelvic inlet widest in the transverse diameter. Outlet is widest in the anterioposterior position. Therefore, the fetus must change position. oInternal rotation begins at the level of the ischial spines. oOcciput rotates anteriorally, and the face rotates posteriorally. o Eventually the occiput is midline beneath the pubicarch. |
|
|
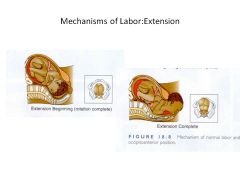
Extension
Head is greatly flexed as it reaches the pelvic floor, and must extend to be born. The occiput passes under the lower border of the symphysis pubis first -> pubic arch acts as a pivot for the rest of the head. Then the head emerges by extension: - first the occiput - then the face - finally the chin. |
|
|
Mechanisms of Labor:
Restitution or External Rotation |
Restitution or External Rotation
After delivery of the head -> the head rotates to a transverse position (returns to the position it occupied when it was engaged in the inlet is termed "restitution"). Rotates a little more -> shoulders now in a anteriorposterior position. The anterior shoulder descends first -> is delivered from under the pubic arch -> the posterior shoulder is delivered. |
|
|
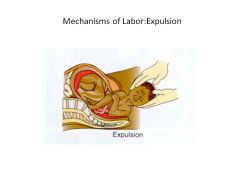
Expulsion
After the shoulders are delivered -> the rest of the body is easily delivered r/t its smaller size. The head and the shoulders is lifted upward -> trunk of the body is delivered. |
|
|
Psychological Response to Labor r/t stress of labor:
Fear, Fatigue, Pain |
Fear
*fear of the unknown *fear unknown hospital *surpise of the speed *myths *own expectations Fatigue *tired of the extra weight *backach *not sleeping well *sleep hungry *overwhelmed Pain *quick tempered *reduce one ability to cope |