Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
112 Cards in this Set
- Front
- Back
|
What is anemia? What is bad about this definition?
|
Decreased O2-carrying capacity of blood (we are unable to measure this clinically)
|
|
|
What usually causes a decreased O2-carrying capacity of blood? What is bad about this?
|
Decreased circulating RBC mass (we are unable to measure this clinically)
|
|
|
What do we measure to assess for anemia?
|
Decreased hemoglobin concentration of blood
|
|
|
What are the functional consequences of anemia?
|
- Decreased O2 delivery to tissues
- Tissue hypoxia in severe cases |
|
|
What are the compensatory mechanisms in Anemia?
|

- ↑ 2,3-DPG
- Shunting of blood from non-vital to vital areas - ↑ CO - ↑ RR - ↑ RBC production - (↑ plasma volume - this is not particularly effective) |
|
|
What are the signs/symptoms of Anemia?
|
- Weakness, malaise, easy fatigability
- Marrow expansion w/ potential bony abnormalities - Pallor - Tachycardia; cardiac ischemia in severe cases - Dyspnea on exertion |
|
|
What causes weakness, malaise, and easy fatigability in anemia?
|
Tissue hypoxia
|
|
|
What causes marrow expansion with potential bony abnormalities in anemia?
|
Increased RBC production (chronic)
|
|
|
What causes pallor in anemia?
|
Shunting of blood from non-vital to vital areas
|
|
|
What causes tachycardia and cardiac ischemia in severe cases of anemia?
|
Increased cardiac output
|
|
|
What causes dyspnea on exertion in anemia?
|
Increased respiration rate
|
|
|
What does the severity of symptoms of anemia depend on?
|
- Severity of anemia
- Rapidity of onset (gradual onset much less symptomatic d/t ability to ramp up compensatory mechanisms) - Pre-existing organ dysfunction |
|
|
What do you need to think if you diagnose an anemia?
|
- Anemia is NOT a disease, it is a symptom of other diseases
- All anemias need to be explained |
|
|
How can you functionally classify anemias?
|
- Blood loss
- Decreased production of RBCs - Accelerated destruction of RBCs |
|
|
How can you morphologically classify anemias?
|
Microcytic
- Normochromic - Hypochromic Normochromic / Normocytic Macrocytic |
|
|
What are the normochromic, microcytic anemias?
|
- Early iron deficiency
- Thalassemia trait - Some hemoglobinopathies (e.g., hemoglobin E) - (Anemia of chronic disease, but usually normochromic/normocytic) |
|
|
What are the hypochromic, microcytic anemias?
|
- Iron deficiency
- Thalassemia trait - Sideroblastic anemia - (Anemia of chronic disease, but usually normochromic/normocytic) |
|
|
What are the normochromic, normocytic anemias?
|
– Anemia of chronic disease
– Anemia of renal failure – Marrow infiltration – Aplastic anemia – Blood loss* – Hemolysis* * May be normocytic or macrocytic depending on degree of blood loss |
|
|
What are the macrocytic anemias?
|
– B12 and folate deficiency
– Liver disease – Myelodysplastic syndromes – Blood loss* – Hemolysis* – Some drugs * May be normocytic or macrocytic depending on degree of blood loss |
|
|
What do you use to investigate anemia?
|
- Clinical history
- Physical exam - CBC - Reticulocyte count - Exam of PB smear - Specific diagnostic tests |
|
|
What information for diagnosing anemia do you get from a CBC?
|
Measurements related to RBC mass:
- Hemoglobin - Hematocrit - RBC count Measurements related to characteristics of RBCs ("indices") - MCV - MCH - MCHC - RDW |
|
|
What is the most important parameter for assessing O2-carrying capacity of blood?
|
Hemoglobin concentration (Hb; g/dL or g/L)
|
|
|
How do you determine the Hemoglobin concentration? Units?
|
- Hb in lysed sample is reacted w/ proprietary reagents
- Resulting complexes measured spectrophotometrically - Measured in g/dL or g/L |
|
|
What is Hematocrit? How do you determine it? Units?
|
- Packed cell volume (percentage of blood volume comprised by RBCs)
- Determine by centrifugation (old method) or by calculating MCV x RBC - % |
|
|
How does Hematocrit compare to Hemoglobin? What information do you gain from calculating the Hematocrit?
|
- Hematocrit is usually ~3x Hemoglobin
- Does not add independent information in vast majority of cases |
|
|
How do you determine the RBC count? Units?
|
- Directly measure # of RBCs per unit volume
- # x 10^9/L |
|
|
How does RBC count compare to Hemoglobin? What information do you gain from calculating the Hematocrit?
|
- Generally correlates well with Hb and hematocrit
- Adds little independent information |
|
|
What is MCV? How do you measure it? Units?
|
Mean Cellular (Corpuscular) Volume
- Measured directly based on either electrical impedance or light scatter - fL |
|
|
What information do you gain from the MCV?
|
Mean Cellular (Corpuscular) Volume
- Very useful in differential diagnosis of anemia (eg, microcytic, normocytic, and macrocytic anemias) |
|
|
What is the differential diagnosis for Microcytic Anemias?
|
- Iron deficiency
- Thalassemia - Anemia of chronic disease - Other (rare) |
|
|
What is the differential diagnosis for Macrocytic Anemias?
|
Megaloblastic (impaired DNA synthesis)
- B12 and folate deficiency - Some drugs - Myelodysplastic syndrome Non-Megaloblastic (other mechanisms) - Reticulocytosis - Liver disease - Hypothyroidism - Some drugs |
|
|
What is MCH? How do you measure it? Units?
|
Mean Corpuscular Hemoglobin
- Calculated as Hb/RBC - Measure of average amount of hemoglobin / RBC - High correlation w/ MCV (so rarely used) - Units: pg |
|
|
What is MCHC? How do you measure it? Units?
|
Mean Corpuscular Hemoglobin Concentration
- Measure of degree of hemoglobinzation or "chromicity" of RBCs - Calculated as Hb/(MCV*RBC) - Units: g/dL |
|
|
What does MCHC help you determine?
|
- Decreased in hypochromic anemias
- Increased in a few "hyperchromic" states (Eg, hereditary spherocytosis, hemoglobin CC disease) |
|
|
What is RDW? How do you measure it?
|
Red Cell Distribution Width
- Measure of variability of RBC volume - Coefficient of variation of RBC volume = σvolume/MCV |
|
|
What is RDW useful for determining?
|
Separation of anemias with variable RBC size (eg, Iron deficiency) from those with uniformly-sized RBCs (eg, anemia of chronic disease)
|
|
|
Which type of anemia has very variable RBCs? How do you measure this?
|
Iron deficiency - elevated RDW value
|
|
|
What is the term for variable RBC shapes?
|
Poikilocytosis
|
|
|
What is the term for variable RBC sizes?
|
Anisocytosis
|
|
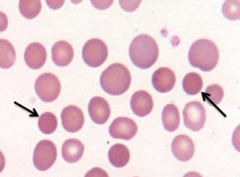
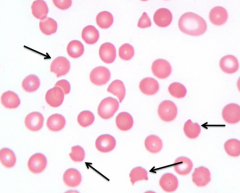
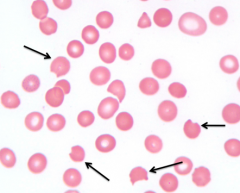
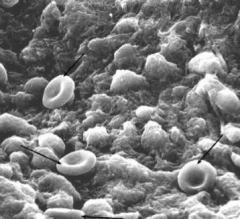
What does this image show? Examples of disorders that would cause this?
|
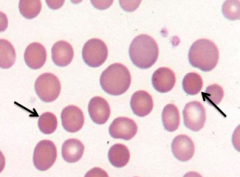
- Spherocytes (round, small diameter, more densely staining, lack of central pallor)
- Eg, hereditary spherocytosis, autoimmune hemolytic anemia |
|
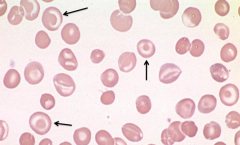
What does this image show? Examples of disorders that would cause this?
|
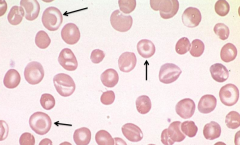
- Target Cells (too much surface area for amount of cytoplasm
- Eg, liver disease, splenectomy, and hemoglobinopathies |
|
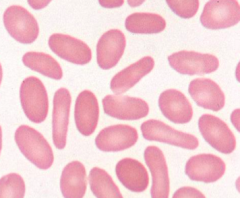
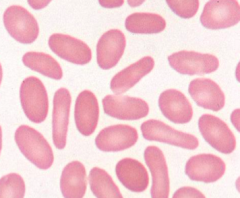
What does this image show? Examples of disorders that would cause this?
|
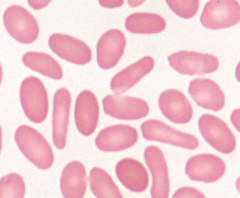
- Ellipotocytes (or ovalocytes)
- Eg, hereditary ellipotocytosis, megaloblastic anemia, iron deficiency, myelofibrosis |
|
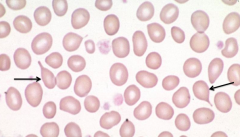
What does this image show? Examples of disorders that would cause this?
|
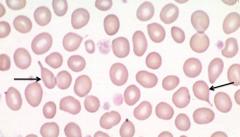
- Teardrop Cells
- Megaloblastic anemia, myelofibrosis, extramedullary hematopoiesis |
|
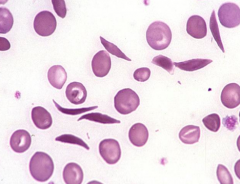
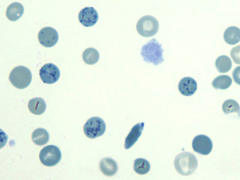
What does this image show? Examples of disorders that would cause this?
|
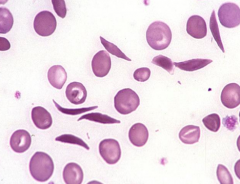
- Sickled Cells
- Caused by sickle cell disease |
|
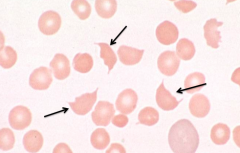
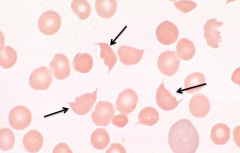
What does this image show? Examples of disorders that would cause this?
|
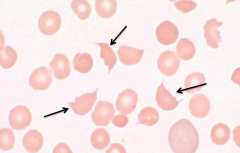
- Schistocytes / RBC fragments
- Eg, TTP (Thrombotic thrombocytopenic purpura), DIC, malignant HTN |
|
What does this image show? Examples of disorders that would cause this?
|
- "Bite Cells"
- Eg, oxidant hemolysis (G6PD deficiency) |
|
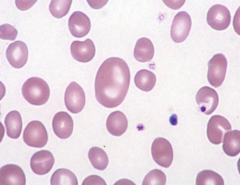
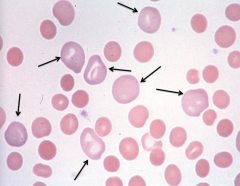
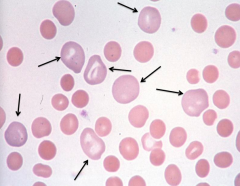
What does this image show? Examples of disorders that would cause this?
|
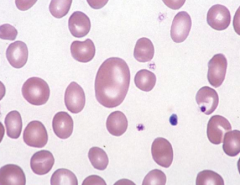
Macrocytic RBCs
– B12 and folate deficiency – Liver disease – Myelodysplastic syndromes – Blood loss** – Hemolysis** – Some drugs |
|
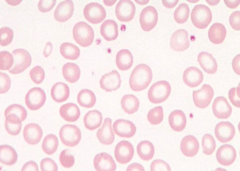
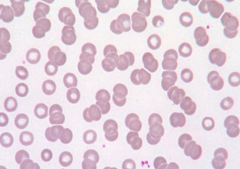
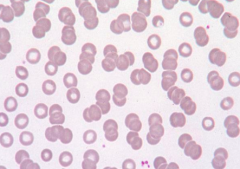
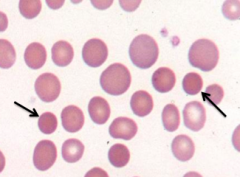
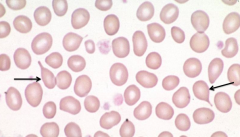
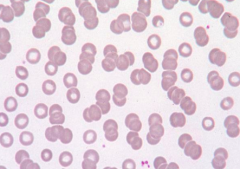
What does this image show? Examples of disorders that would cause this?
|
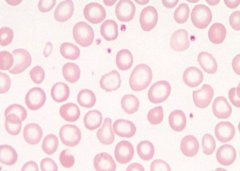
Hypochromic RBCs (central pallor >1/3 diameter)
- Iron deficiency - Thalassemia trait - Sideroblastic anemia - (Anemia of chronic disease) |
|
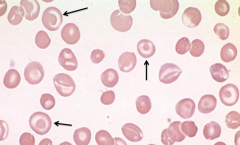
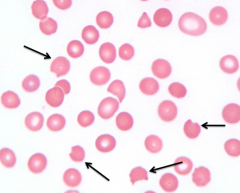
What does this image show? Examples of disorders that would cause this?
|
Polychromtophilic Cells / Reticulocytes
- RBCs are larger and have purplish tinge - Immature cells w/ residual organelles in cytoplasm giving it a bluish tinge - Can be caused by acute blood loss (sign that the BM is rapidly trying to make RBCs) |
|
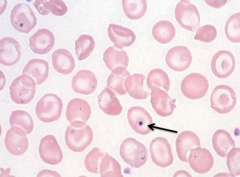
What does this image show? Examples of disorders that would cause this?
|
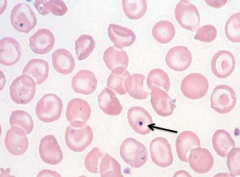
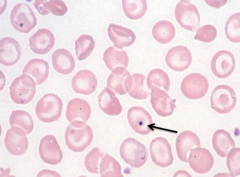
- Howell-Jolly Bodies (nuclear fragments)
- Eg, Splenectomy, megaloblastic anemia - Marker of poorly functioning spleen because spleen normally should be removing these before releasing into PB |
|
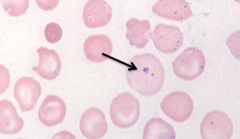
What does this image show? Examples of disorders that would cause this?
|
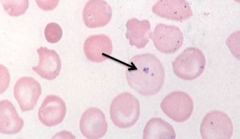
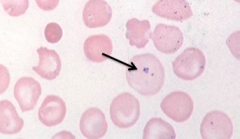
- Pappenheimer Bodies (iron granules)
- Eg, splenectomy and iron overload |
|
What does this image show? Examples of disorders that would cause this?
|
- Basophilic stippling (coarse) - disordered Hb synthesis
- Eg, Thalassemias, MDS, lead poisoning |
|
What does this image show? Examples of disorders that would cause this?
|
- Hemoglobin C crystals
- Eg, Hb CC disease, Hb SC disease |
|
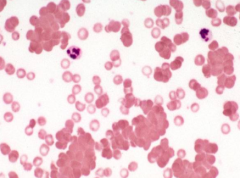
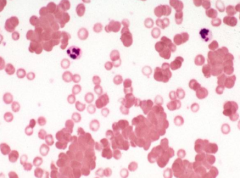
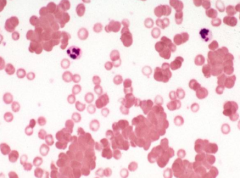
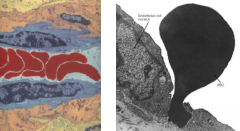
What does this image show? Examples of disorders that would cause this?
|
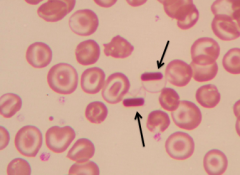
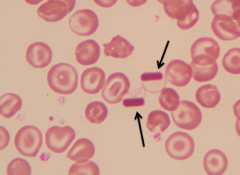
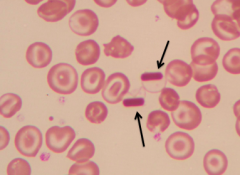
- Rouleaux
- Decreased repulsive forces between RBCs - Eg, increased serum proteins (Ig, fibrinogen) |
|
What does this image show? Examples of disorders that would cause this?
|
- Agglutination
- Eg, IgM RBC antibodies (cold agglutinins) |
|
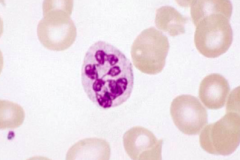
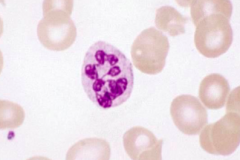
What does this image show? Examples of disorders that would cause this?
|
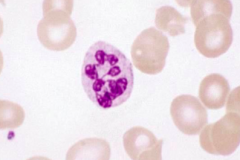
- Hypersegmented neutrophil
- Eg, megaloblastic anemia |
|
|
What RBC abnormality is caused by Hereditary Spherocytosis and Autoimmune Hemolytic Anemia?
|
Spherocytes
- Round - Small diameter - More densely staining - Lack of central pallor |
|
|
What RBC abnormality is caused by liver disease, splenectomy, and hemoglobinopathies?
|
Target Cells
- Too much surface area to amount of cytoplasm - Cell gets floppy/redundant |
|
|
What RBC abnormality is caused by hereditary elliptocytosis, megaloblastic anemia, iron deficiency, and myelofibrosis?
|
Ellipotocytes (ovalocytes)
|
|
|
What RBC abnormality is caused by megaloblastic anemia, myelofibrosis, and extramedullary hematopoiesis?
|
Teardrop Cells
|
|
|
What RBC abnormality is caused by TTP (Thrombotic Thrombocytopenic Purpura), DIC, and malignant HTN?
|
Schistocytes / RBC fragments
|
|
|
What RBC abnormality is caused by oxidant hemolysis like G6PD deficiency?
|
Bite cells
|
|
|
What RBC abnormality is caused by splenectomy and megaloblastic anemia?
|
Howell-Jolly Bodies (nuclear fragments)
|
|
|
What RBC abnormality is caused by splenectomy and iron overload?
|
Pappenheimer bodies (iron granules)
|
|
|
What RBC abnormality is caused by thalassemias, MDS, and lead poisoning?
|
Basophilic Stippling (coarse)
- Disordered hemoglobin synthesis |
|
|
What RBC abnormality is caused by Hb CC or SC disease?
|
Hemoglobin C crystals
|
|
|
What RBC abnormality is caused by decreased repulsive forces between RBCs, such as when there are increased serum proteins (Ig or fibrinogen)?
|
Rouleaux
|
|
|
What RBC abnormality is caused by IgM RBC antibodies (cold agglutinins)?
|
Agglutination
|
|
|
What WBC abnormality is caused by megaloblastic anemia?
|
Hypersegmented neutrophils
|
|
|
What happens in acute blood loss as it relates to anemia?
|
- Initially no anemia by CBC parameters despite decrease in blood volume
- Anemia develops as tissue fluid enters vascular space to restore blood volume producing dilution of cellular elements - Reticulocytes increase after 2-3 days and peak at 7-10 days |
|
|
What happens 2-3 days after acute blood loss? 7-10 days?
|
- 2-3 days: reticulocyte count increases
- 7-10 days: reticulocyte count peaks |
|
|
What happens in chronic blood loss as it relates to anemia?
|
- No anemia initially because BM is able to compensate
- Slight reticulocytosis - Eventual development of iron deficiency w/ resultant iron deficiency anemia |
|
|
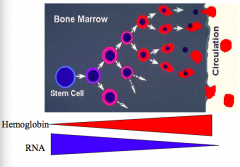
Where are RBCs produced?
|
- Embryo: yolk sac
- Fetus (3 months gestation until birth): liver - Shortly after birth through adult life: bone marrow |
|
|
How is RBC production regulated?
|
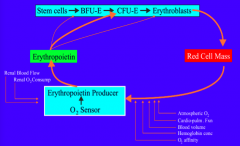
- Decreased O2 delivery induces production of epo by kidneys
- Epo causes proliferation and differentiation of committed progenitor cells |
|
|
What are normoblasts?
|
Nucleated RBC precursors
|
|
|
Where do normoblasts get their iron from for hemoglobin synthesis?
|
Plasma transferrin
|
|
|
How many reticulocytes can be produced from each pronormoblast (earliest morphologically recognizable erythroid precursor)?
|
Up to 16
|
|
|
How does the number of reticulocytes compare to the number of normoblasts in BM?
|
Roughly equal numbers
|
|
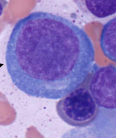
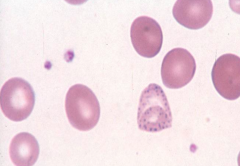
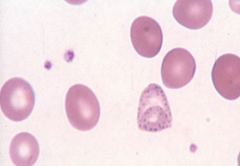
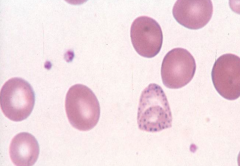
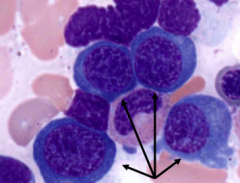
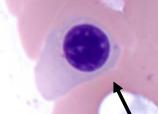
What is the big cell in this image?
|
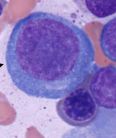
Pronormoblast
|
|
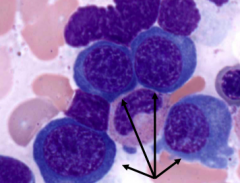
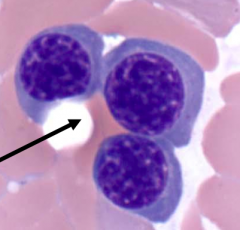
What are the cells in this image?
|
Basophilic Normoblasts (nucleated RBC precursors)
|
|
What are the cells in this image?
|
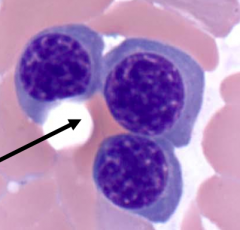
Polychromatophilic Normoblasts
|
|
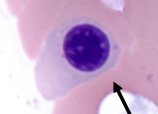
What is the cell in this image?
|
Orthochromic Normoblast
|
|
|
What is the earliest anucleate erythroid form?
|
Reticulocytes
|
|
|
What are the structural/morphologic characteristics of Reticulocytes?
|
- First anucleate erythroid form
- Larger than mature RBCs - Contain residual RNA which gives cytoplasm a blue tinge on routinely stained blood smears (polychromasia) - Circulate for ~1 day before losing residual ribosomes, mitochondria, and other organelles to become mature RBCs |
|
|
What do Reticulocytes do in BM?
|
Stay in BM 1-2 days synthesizing Hb before released into circulation
|
|
|
How common are Reticulocytes in the PB? How are they detected?
|
- Normally 1% of peripheral erythrocytes
- Detected using RNA stains |
|
|
What are reticulocytes a measure of? How does the number of these inform you about the type of anemia?
|
Informs you about status of BM RBC production:
- No increased reticulocytes: ↓ RBC production anemia - ↑ Reticulocytes: adequate BM response to blood loss or ↑ RBC destruction |
|
|
What is the problem with calculating the reticulocyte count? Solution?
|
- Reticulocyte % varies if the denominator (total RBC count) varies
- Solution is to correct reticulocyte percentage: Retic% x (patient HCT/45) - Another solution is to do an absolute reticulocyte count |
|
|
What can cause decreased RBC production?
|
- Ineffective erythropoiesis
- Decreased RBC precursors (marrow failure) - Anemia of chronic disease (anemia of inflammation) |
|
|
What is the definition of Ineffective Erythropoiesis?
|
- Decreased RBC production despite increased RBC precursors in BM
- Characterized by defects in maturation |
|
|
What are some examples of Ineffective Erythropoiesis?
|
- Iron deficiency (cytoplasmic maturation defect)
- Megaloblastic anemia (nuclear maturation defect) - Myelodysplastic disorders |
|
|
What happens to RBCs in Ineffective Erythropoiesis?
|
- Prominent morphologic abnormalities of RBCs d/t disordered maturation
- Increased RDW (variability in sizes) |
|
|
What are the implications of Ineffective Erythropoiesis?
|
- Prominent morphologic abnormalities of RBCs
- Dysmaturation of RBC precursors in BM - Decreased reticulocyte count despite increased erythroid mass in BM - Inappropriately increased iron absorption from gut |
|
|
What causes decreased RBC precursors?
|
Failure of BM - d/t defects in proliferation
|
|
|
What is responsible for the decrease in BM mass of RBC precursors?
|
- Decreased RBC progenitors available for RBC production OR
- Decreased proliferative capacity of numerically adequate erythroid progenitors |
|
|
What are the general features of Decreased RBC Precursors causing anemia?
|
- Normochromic / normocytic anemia
- Usually little anisopoikilocytosis (compared to maturation defects / ineffective erythrpoiesis) - Normal RDW - Decreased reticulocyte counts |
|
|
What can cause Decreased RBC Precursors?
|
1) Stem cell defects w/ adequate epo
- RBC aplasia (pure) vs pan-aplasia (aplastic anemia) - Congenital and acquired causes 2) Marrow replacement - Leukemias/lymphomas - Metastatic carcinoma - Fibrosis - Storage disease 3) Decreased Epo - Anemia of renal failure |
|
|
What is the normal structure of a RBC: Shape? Diameter? Volume?
|
- Biconcave disc
- 7.5-8.7 µm diameter - Average volume of 90fL |
|
|
How big can a RBC swell up to? Normal?
|
150 fL (normal is 90 fL)
|
|
|
How small of a capillary can a RBC squeeze through? Normal diameter?
|
- 2.8 µm diameter capillary
- Normally 7.5-8.7 µm RBC diameter |
|
|
How do RBCs normally get removed?
|
Intravascular:
- Breach of membrane in circulation - Very low frequency under normal conditions Extravascular: - Clearance in reticuloendothelial system as a result of RBC senescence |
|
|
What are the sequence of events that leads to clearance of RBCs from the circulation?
|
1. Modified Hb binds Band 3
2. Modification of Band 3 3. Binding of autologous IgG 4. Disruption of Band 3 anchorage of membrane and cytoskeleton 5. Formation of vesicles w/ exposure of cellular antigens and phosphatidylserine on surface of vesicles 6. Recognition of vesicles by scavenger receptors 7. Clearance of RBCs without membrane breach and loss of cellular contents, mainly by Kuppfer cells in liver |
|
|
What are the initial events that cause clearance of RBCs from the circulation?
|
1. Modified Hb binds Band 3
2. Modification of Band 3 3. Binding of autologous IgG |
|
|
What happens to RBCs after binding autologous IgG during clearance from circulation?
|
4. Disruption of Band 3 anchorage of membrane and cytoskeleton
|
|
|
What happens to RBCs after disruption of Band 3 anchorage of membrane and cytoskeleton?
|
5. Formation of vesicles w/ exposure of cellular antigens and phosphatidylserine on surface of vesicles
6. Recognition of vesicles by scavenger receptors |
|
|
What happens to RBCs after recognition of vesicles by scavenger receptors?
|
7. Clearance of RBCs without membrane breach and loss of cellular contents, mainly by Kuppfer cells in liver
|
|
|
What does increased destruction (hemolysis) of RBCs result in?
|
Increased marrow production (8x normal in ideal circumstances)
|
|
|
What is necessary for there to be increased BM production of RBCs following hemolysis of RBCs?
|
Need enough iron, folate, and be in otherwise good health
|
|
|
When does anemia develop d/t RBC destruction (hemolysis)?
|
When rate of destruction exceeds BM ability to compensate (forms new steady state at lower Hb level)
|
|
|
What are the methods of RBC destruction?
|
- Intravascular
- Extravascular - Combination |
|
|
What form of hemolysis predominates in Hemolytic Anemia?
|
Extravascular Hemolysis
|
|
|
What is the final common pathway of Extravascular Hemolysis?
|
Decreased RBC deformability
– Rigid, non-deformable cells have trouble traversing narrow slits between splenic cords and sinusoids – Cells are damaged further with prolonged exposure to splenic cordal environment – Damaged cells phagocytized by cordal macrophages |