![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
186 Cards in this Set
- Front
- Back
|
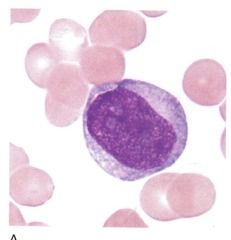
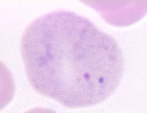
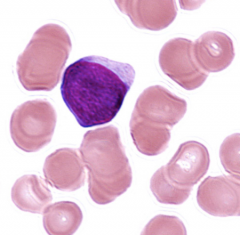
Myeloblast Cellsize: 12-20 um N/Cratio 4:1•Round-ovalnucleus, “round refrigerator corners”*•Centralor eccentric nucleus•Lightred-purple fine meshwork chromatin with no aggregation of material •1-5nucleoli*•Scantybasophilic cytoplasm•Nogranules•Maycontain Auer rods |
|
|
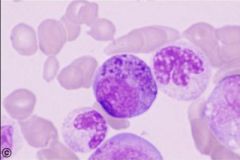
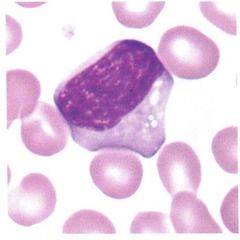
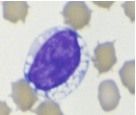
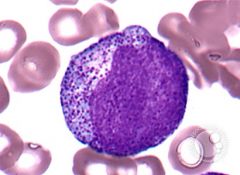
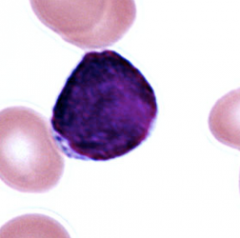
Promyelocyte (pretty much a blast with granules) •Coarse azurophilic nonspecific (primary) granules* •Cellsize: 15-23 um•N/Cratio 3:1•Round-ovalnucleus •Lightred-purple fine meshwork chromatin, possibly slight aggregation at nuclearmembrane•1-3nucleoli•Basophiliccytoplasm (may be slightly increased over blast) |
|
|
Myelocyte•Cellsize: 10-18 um•N/Cratio 2:1 or 1:1•Moreround-oval nucleus*•Centralor eccentric nucleus•Red-purplefine chromatin with slightly aggregated pattern*•Mayor may not have nucleoli Moderatebluish - pink cytoplasm nonspecific(primary=purple) and specific (secondary) granules* |
|
|
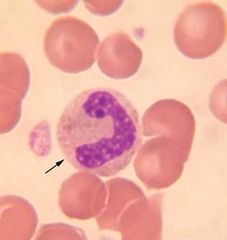
Metamyelocyte •Cellsize: 10-18 um•N/Cratio 1:1•Indented(kidney shaped) nucleus* •Centralor eccentric nucleus•Lightblue-purple with chromatin clumps easily distinguishable•Nonucleoli•Moderatebluish - pink cytoplasm (occasionally clear pink)•Specific(secondary) granules (few non-specific)• |
|
|
Band•Cellsize: 10-16 um•N/Cratio 1:1•Elongatednarrow band shape of uniform thickness, singular lobe*•Centralor eccentric nucleus•Deepblue-purple coarsely granular nuclear chromatin (distinctparachromatin)•Nonucleoli•Abundantpink cytoplasm•Fineviolet-pink specific granules• |
|
|
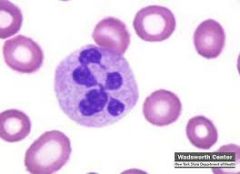
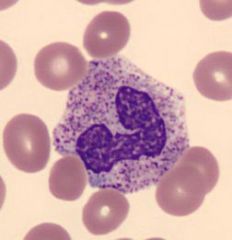
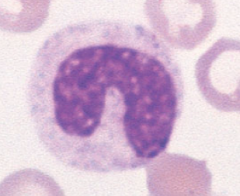
PMN•Cellsize: 10-16 um•N/Cratio 1:1•2-5distinct nuclear lobes (filament connecting lobes)*•Centralor eccentric nucleus•Deepblue-purple coarsely granular nuclear chromatin (distinct parachromatin)•Nonucleoli•Abundantpink cytoplasm•Fineviolet-pink specific granules |
|
|
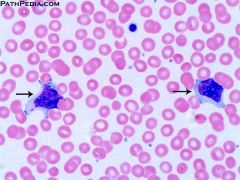
Basophilic Myelocyte |
|
|
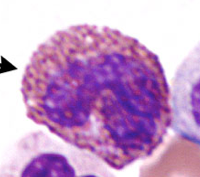
Eosinophilic Myelocyte (Immature eosinophil) |
|
|
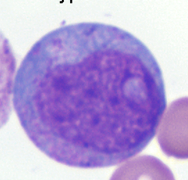
Monoblast•Cellsize: 12-20 um•N/Cratio 4:1•Round-oval,or slightly folded nucleus•Centralor eccentric nucleus•Palered-purple, minimal, fine threadychromatin •Usually1-2 nucleoli•Moderatebasophilic cytoplasm, regular border•Nogranules Maycontain Auer rods |
|
|
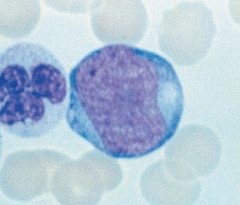
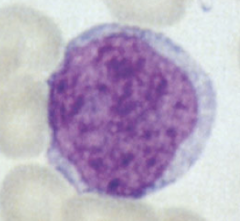
Promonocyte•Cellsize: 10-16 um•N/Cratio 3:1 or 2:1•Roundnucleus with chromatin creases or cerebriformfolding more distinct•Centralor eccentric nucleus•Palered-purple, very fine pattern, (aerated network of threads)•0-2nucleoli•Paleropaque gray-blue cytoplasm, more abundant, may see pseudopodia and vacuoles |
|
|
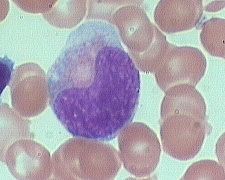
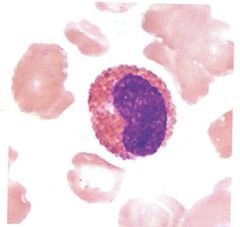
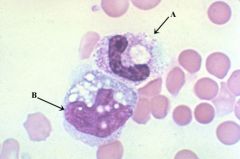
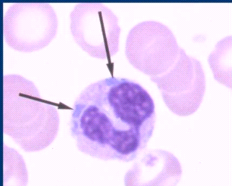
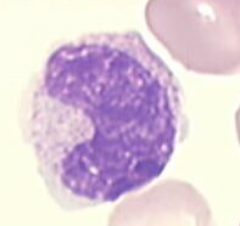
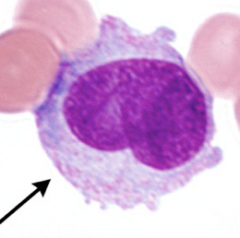
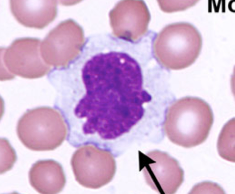
Monocyte•Cellsize: 12-20 um•N/Cratio 2:1 or 1:1•Cerebriformor horseshoe shaped nucleus•Centralnucleus•Blue-purple,fine reticular nuclear chromatin (less distinct parachromatin)•0-2Nucleoli •Abundantpale gray-blue cytoplasm, may seepseudopodia & vacuoles•Morenumerous very fine (dust like) red granules evenly dispersed• |
|
|
Megakaryoblast |
|
|
Promegakaryocyte |
|
|
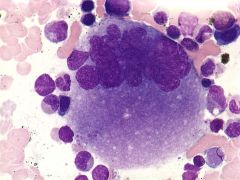
Megakaryocyte |
|
|
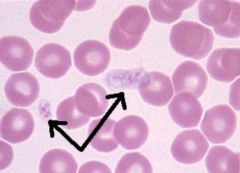
Thrombocytes |
|

|
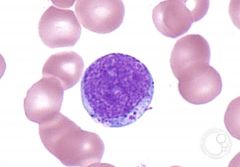
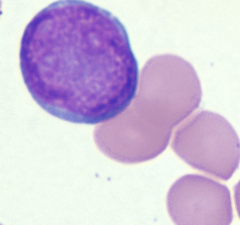
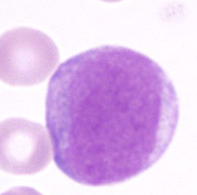
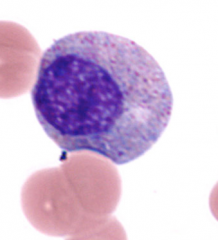
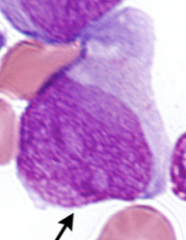
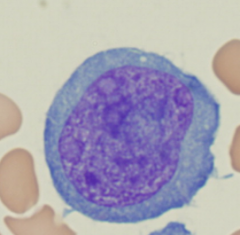
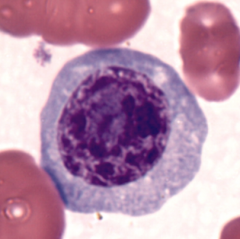
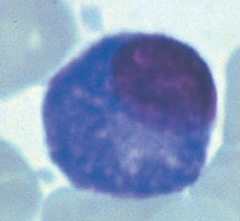
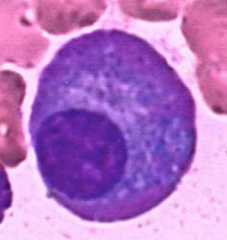
Lymphoblast•Cellsize: 10-20 um•N/Cratio 4:1•Roundor oval nucleus•Centralor eccentric nucleus•Undifferentiatedsparse red purple chromatin •1-2indistinct nucleoli•Scanty,often nearly absent, clear basophilic cytoplasm* •Nogranules |
|
|
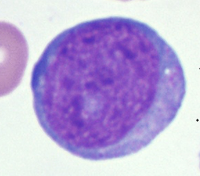
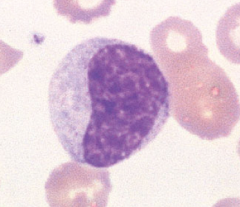
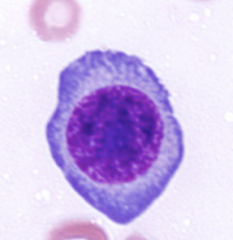
Prolymphocyte•Cellsize: 9 - 18 um•N/Cratio 4:1 (occasionally 3:1)•Roundor oval and flat nucleus•Centralor eccentric nucleus•Combinationof condensed clumped blue-purple chromatin with red-purple parachromatin*•0-1more distinct nucleoli*•Oftenscanty, but visableclear basophilic cytoplasm •Nogranules• |
|
|
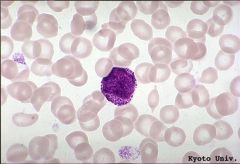
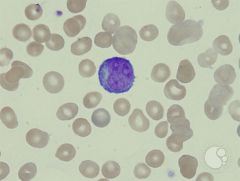
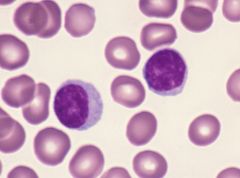
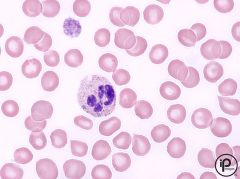
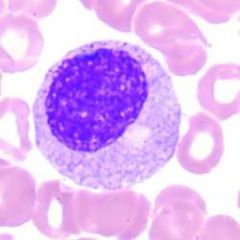
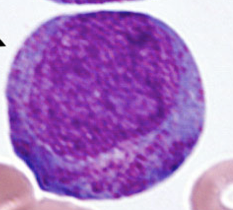
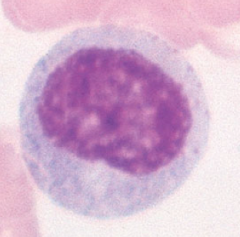
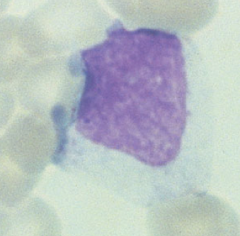
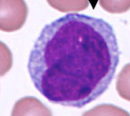
Lymphocyte•Cellsize: 7-18 um (usually 9-12)•N/Cratio 4:1 (occasionally 3:1)•Roundor indented nucleus•Eccentricnucleus often with scanty cytoplasm •Homogeneous,coarse blue-purple nuclear chromatin (smudged)•Nucleoliusually absent , rarely one seen in mature forms•Lightto dark blue cytoplasm, scanty to moderate•Occasionallya few azurophilicgranules seen• |
|
|
Reactive Lymphocyte (Increased in viral infections) |
|
|
Plasmacytoid Cell |
|

|
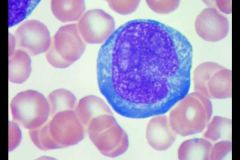
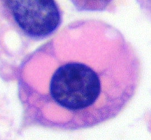
Plasma Cell•Cellsize: 8 - 20 um•N/Cratio 2:1 or 1:1•Roundor oval nucleus•Usuallyeccentric nucleus•Blue- purple, dense chromatin w/ largeclumps near nuclear margin•Nonucleoli•Moderate,basophilic cytoplasm, with perinuclearclear zone adjacent to nucleus, may contain vacuoles•Nogranules (may see Russell Bodies)• |
|
|
Flame Cell Brilliant red staining cytoplasm (Plasma cell that produces IgA) |
|
|
Mott Cell (Plasma cell with immunoglobulins abnormally packaged) |
|
|
Auer Rods Due to abnormally formed granules, usually a sign of malignancy |
|
|
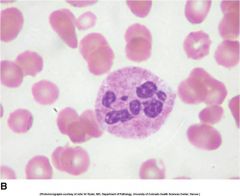
Hypersegmented neutrophils Due to megaloblastic changes, will also see macrocytic anemia |
|
|
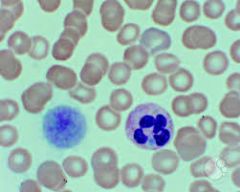
Pince-nez PMNs Due to Pelger-Huet anomaly: Benign, congenital hyposegmentation |
|
|
Toxic granulation Fewer mitotic divisions results in less dilute granules (Usually seen with: shift to the left, toxic vacuolization, dohle bodies) |
|
|
Toxic vacuolization Due to increased phagocytosis (Usually seen with: shift to the left, toxic granulation, dohle bodies) |
|
|
Dohle bodies Cause: Remnant RNA (Usually seen with: shift to the left, toxic granulation, toxic vacuolization) |
|
|
May-Hegglin anomaly Dohle-like bodies and giant/bizarre platelets Rare autosomal dominant condition; at risk for infections and bleeding |
|
|
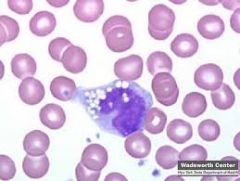
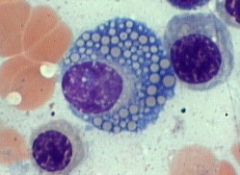
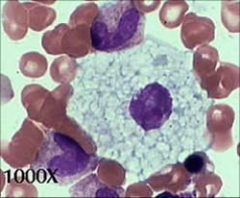
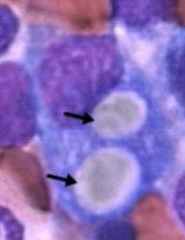
Foam cell (indistinct "bubbles") Nieman-Pick Disease Deficient enzyme: sphingomyelinase Lipid storage disorder Cannot degrade sphingomyelin so accumulates in spleen, liver, lungs, brain, and bone marrow |
|
|
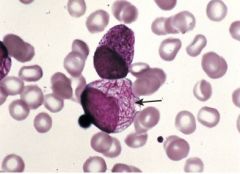
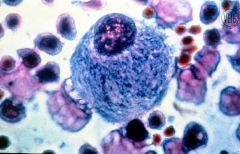
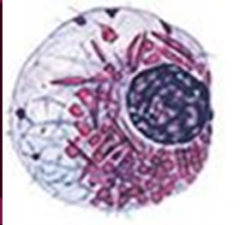
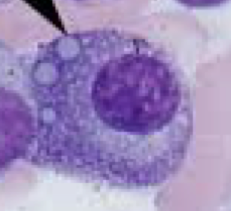
Gaucher cell ("Chicken scratch") Gaucher's Disease Deficient enzyme: beta-glucocerebrosidase Lipid storage disorder Cannot degrade glucocerebrosidase so accumulates in monocytes and macrophages |
|

|
Gaucher cell ("Chicken scratch") Gaucher's Disease Deficient enzyme: beta-glucocerebrosidase Lipid storage disorder Cannot degrade glucocerebrosidase so accumulates in monocytes and macrophages |
|
|
May-Hegglin anomaly Dohle-like bodies and giant/bizarre platelets Rare autosomal dominant condition; at risk for infections and bleeding |
|
|
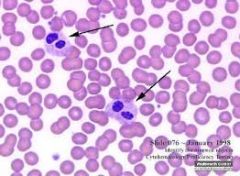
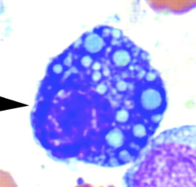
Vacuolated lymphocyte Tay-Sachs Disease Deficient enzyme: Hexosaminidase A Congenital nerve disease, accumulation of unmetabloized ganglioside in almost all tissues Death occurs by 4 years of age |
|
|
Vacuolated lymphocyte Tay-Sachs Disease Deficient enzyme: Hexosaminidase A Congenital nerve disease, accumulation of unmetabloized ganglioside in almost all tissues Death occurs by 4 years of age |
|
|
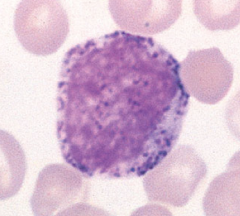
Promyelocyte |
|
|
Myelocyte •Cell size: 10-18 um •N/C ratio 2:1 or 1:1 •More round-oval nucleus* •Central or eccentric nucleus •Red-purple fine chromatin with slightly aggregated pattern* •May or may not have nucleoli Moderate bluish - pink cytoplasm nonspecific (primary=purple) and specific (secondary) granules* Chromatin=white spaces |
|
|
Which blast cell(s) can contain Auer Rods? What are the rods? Example of a pathology: |
Monoblast Myleoblast Abnormally formed lysosomal granules Found in pathologies: acute myeloid leukemia (AML) |
|
|
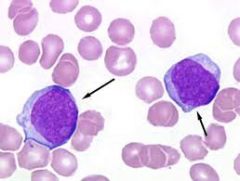
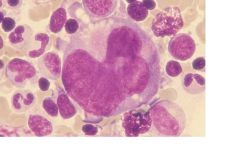
MyeloblastCell size: 12-20 um N/C ratio 4:1 •Round-oval nucleus, “round refrigerator corners” * •Central or eccentric nucleus •Light red-purple fine meshwork chromatin with no aggregation of material •1-5 nucleoli* •Scanty basophilic cytoplasm •No granules •May contain Auer rods |
|

|
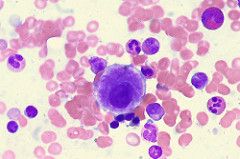
Myeloblast with Auer Rods (top left) MyeloblastCell size: 12-20 um N/C ratio 4:1 •Round-oval nucleus, “round refrigerator corners” * •Central or eccentric nucleus •Light red-purple fine meshwork chromatin with no aggregation of material •1-5 nucleoli* •Scanty basophilic cytoplasm •No granules |
|
|
What is the lineage of the granulocytic series? Also, what's the other name for it? |
Granulocytic (or Myelocytic series) Myleoblast Promyelocyte Myelocyte Metamyelocyte Band Neutrophil |
|
|
Promyelocyte (pretty much a blast with granules) •Coarse azurophilic nonspecific (primary) granules* |
|
|
Type I blast (myeloblast) is devoid of granules and referred to as an agranularblast. |
|
|
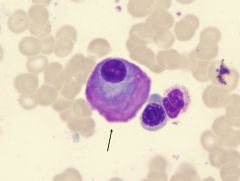
Type II blast (myeloblast) has <20 granules and is referred to as granular blast |
|
|
Type III blast (myeloblast) has >20 granules but is still an immature cell thatdoes not fit the definition of a promyelocyte. Also referred to as granular blast. |
|
|
Pappenheimer bodies Iron granules Due to excessive iron or under-utilization of iron |
|
|
Myelobast Type II |
|
|
Myelobast |
|
|
Promyelocyte |
|
|
Myelocyte •Cell size: 10-18 um •N/C ratio 2:1 or 1:1 •More round-oval nucleus* •Central or eccentric nucleus •Red-purple fine chromatin with slightly aggregated pattern* •May or may not have nucleoli Moderate bluish - pink cytoplasm nonspecific (primary=purple) and specific (secondary) granules* |
|
|
Myelocyte •Cell size: 10-18 um •N/C ratio 2:1 or 1:1 •More round-oval nucleus* •Central or eccentric nucleus •Red-purple fine chromatin with slightly aggregated pattern* •May or may not have nucleoli Moderate bluish - pink cytoplasm nonspecific (primary=purple) and specific (secondary) granules* |
|
|
Metamyelocyte •Cell size: 10-18 um •N/C ratio 1:1 •Indented (kidney shaped) nucleus* •Central or eccentric nucleus •Light blue-purple with chromatin clumps easily distinguishable •No nucleoli •Moderate bluish - pink cytoplasm (occasionally clear pink) •Specific (secondary) granules (few non-specific) • White spaces=chromatin |
|
|
Metamyelocyte •Cell size: 10-18 um •N/C ratio 1:1 •Indented (kidney shaped) nucleus* •Central or eccentric nucleus •Light blue-purple with chromatin clumps easily distinguishable •No nucleoli •Moderate bluish - pink cytoplasm (occasionally clear pink) •Specific (secondary) granules (few non-specific) White spaces=chromatin |
|
|
Band •Cell size: 10-16 um •N/C ratio 1:1 •Elongated narrow band shape of uniform thickness, singular lobe* •Central or eccentric nucleus •Deep blue-purple coarsely granular nuclear chromatin (distinct parachromatin) •No nucleoli •Abundant pink cytoplasm •Fine violet-pink specific granules |
|
|
Immature eosinophil |
|
|
What is a Leukomoid Reaction? |
Transient, reactive condition- normal response to infection, bacteria, parasites, etc. Characterized by moderate to severe increased WBC and a 'Shift to the Left' (increased immature granulocytes in blood) |
|
|
Neutrophils in the peripheral blood exist in either the ___________ or the __________ pool. |
Neutrophils in the peripheral blood exist in either the circulating or the marginating pool. |
|
|
Which white blood cells of the peripheral blood is actually considered immature? |
Monocytes After only a few hours in the blood it migrates into the tissues and matures further into the macrophage or histocyte. |
|
|
Monoblast Although almost identical to a myeloblast, mono blasts can be identified by the presence of a single large nucleolus, an irregularly shaped nucleus and a delicate chromatin |
|
|
Monoblast Although almost identical to a myeloblast, mono blasts can be identified by the presence of a single large nucleolus, an irregularly shaped nucleus and a delicate chromatin |
|
|
Promonocyte •Cell size: 10-16 um •N/C ratio 3:1 or 2:1 •Round nucleus with chromatin creases or cerebriform folding more distinct •Central or eccentric nucleus •Pale red-purple, very fine pattern, (aerated network of threads) •0-2 nucleoli •Paler opaque gray-blue cytoplasm, more abundant, may see pseudopodia and vacuoles |
|
|
Promonocyte •Cell size: 10-16 um •N/C ratio 3:1 or 2:1 •Round nucleus with chromatin creases or cerebriform folding more distinct •Central or eccentric nucleus •Pale red-purple, very fine pattern, (aerated network of threads) •0-2 nucleoli •Paler opaque gray-blue cytoplasm, more abundant, may see pseudopodia and vacuoles |
|
|
Promonocyte •Cell size: 10-16 um •N/C ratio 3:1 or 2:1 •Round nucleus with chromatin creases or cerebriform folding more distinct •Central or eccentric nucleus •Pale red-purple, very fine pattern, (aerated network of threads) •0-2 nucleoli •Paler opaque gray-blue cytoplasm, more abundant, may see pseudopodia and vacuoles |
|
|
Lymphoblast |
|
|
Lymphoblast |
|
|
"small lymphoblast" |
|

|
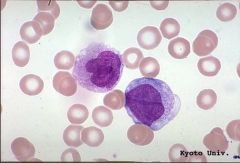
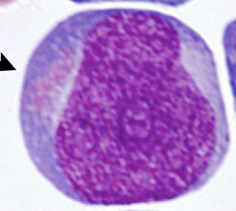
Prolymphocyte •Cell size: 9 - 18 um •N/C ratio 4:1 (occasionally 3:1) •Round or oval and flat nucleus •Central or eccentric nucleus •Combination of condensed clumped blue-purple chromatin with red-purple parachromatin* •0-1 more distinct nucleoli* •Often scanty, but visable clear basophilic cytoplasm •No granules • |
|
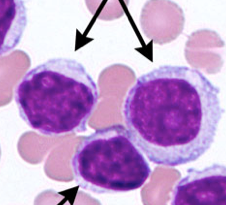
What are the top two cells (Same)? What is the bottom? |
Top two = prolymphocytes bottom = lymphocytes |
|
|
If a B lymphoblast produces antibody it is called a ________________. |
Plasmablast |
|
|
If a B-prolymphocyte produces antibody it is called a _______________. |
Proplasmacyte |
|
|
Plasmablast •Cellsize: 16-18 um•N/Cratio 4:1•Roundnucleus•Centralor eccentric nucleus•Palered- purple, fine stippled chromatin •Usually1-3 nucleoli•Scantyto moderate, paler bluethan more mature forms, occasionally perinuclearclear zone •Nogranules• |
|
|
Proplasmacyte •Cellsize: 15 -25 um•N/Cratio 3:1•Roundor oval nucleus•Centralor eccentric nucleus•Red-purple, increased granularity of chromatin •Usually1-3 nucleoli•Moderate,basophilic cytoplasm, may or may not have perinuclearclear zone adjacent to nucleus•Nogranules• |
|
|
Plasma Cell •Cell size: 8 - 20 um •N/C ratio 2:1 or 1:1 •Round or oval nucleus •Usually eccentric nucleus •Blue - purple, dense chromatin w/ large clumps near nuclear margin •No nucleoli •Moderate, basophilic cytoplasm, with perinuclear clear zone adjacent to nucleus, may contain vacuoles •No granules (may see Russell Bodies) • |
|
|
Plasma Cell •Cell size: 8 - 20 um •N/C ratio 2:1 or 1:1 •Round or oval nucleus •Usually eccentric nucleus •Blue - purple, dense chromatin w/ large clumps near nuclear margin •No nucleoli •Moderate, basophilic cytoplasm, with perinuclear clear zone adjacent to nucleus, may contain vacuoles •No granules (may see Russell Bodies) • |
|

|
Russell Bodies Red or white globular inclusions of Ig in the cytoplasm. Maybe so voluminous as to obliterate the other cell structures (mott cell or grape cell) May also be in crystals or rods |
|
|
Russell Bodies Red or white globular inclusions of Ig in the cytoplasm. Maybe so voluminous as to obliterate the other cell structures (mott cell or grape cell) May also be in crystals or rods |
|
|
Russell Bodies Red or white globular inclusions of Ig in the cytoplasm. Maybe so voluminous as to obliterate the other cell structures (mott cell or grape cell) May also be in crystals or rods |
|
|
Russell Bodies Red or white globular inclusions of Ig in the cytoplasm. Maybe so voluminous as to obliterate the other cell structures (mott cell or grape cell) May also be in crystals or rods |
|
|
Russell Bodies Red or white globular inclusions of Ig in the cytoplasm. Maybe so voluminous as to obliterate the other cell structures (mott cell or grape cell) May also be in crystals or rods |
|
|
Mott cell |
|
|
Flame Cell Brilliant red staining cytoplasm (Plasma Cell that produces IgA) |
|
|
What is the defect that causes toxic granulation? |
Fewer mitotic divisions So less dilution of non-specific (primary) granules. |
|
|
What is a 'shift to the left'? |
More immature cells in peripheral blood Can be caused by malignancy or leukomoid reaction |
|
|
What are the two typical causes of a 'shift to the left'? |
-Leukomoid reaction -Malignancy |
|
|
If you see toxic granulation what will you usually find along with it? |
Toxic vacuolization Dohle bodies Shift to the left |
|
|
What is the cause of toxic vacuolization? |
Increased phagocytosis
|
|
|
What is a Dohle body? |
Remnant RNA in cytoplasm of granulocytes and monocytes (not usually visible in monos) |
|
|
If you had hypersegmented polys as a result of a disruption of DNA synthesis, what would you also expect to see? |
-Macrocytic RBCs (because would cause fewer divisions thus larger cells) -Asynchronous development of nRBCs |
|
|
What constitutes hypersegmentation? |
Mature polys with six or more lobes |
|
|
What typically causes hypersegmented polys? |
Megaloblastic changes (disruption of DNA synthesis) |
|
|
What constitutes the Pelger-Huet Anomaly? |
-Hyposegmentation of PMNs and increased bands -No granulocytes with >2 nuclear lobes (Pince-nez: two lobes, Stodtmeister: one lobe) |
|
|
What distinguishes a Stodtmeister cell from a band nuetrophil or a myelocyte? |
Stodtmeister cell with have very clumped chromatin |
|
|
What is the distinction of pseduo Pelger-Huet and why is it important to note? |
Some normal PMNs will be present Important because will have increased bands, which could seem like a shift to the left/bacterial infection |
|
|
What are reactive lymphs in peripheral blood usually associated with? |
Infectious mono, hepatitis, other viral infections |
|
|
What are two older terms for reactive lymphs? |
Atypical or downey lymph |
|
|
What are the main characteristics of a plasmacytoid lymph? |
Dark blue cytoplasm Heavily clumped chromatin (Less eccentric nucleus than plasma cell and slight or absent golgi halo) |
|
|
What is a Barr body? |
Extra X chromosome unnecessary for normal nuclear function |
|
|
What is pyknotic degeneration? |
Cell break down (undergoing apoptosis, necrobiosis) (Nuclear material loses chromatin pattern and can be seen as one or several dense masses) |
|
|
What are smudge cells caused by and what are they often associated with? |
Cells destroyed by making smear Associated with cell fragility (Often seen with chronic lymphocytic leukemia and acute lymphocytic leukemia) |
|
|
What can you do to help avoid smudge cell artifact? |
Add albumin and remake smear |
|
|
What is septicemia and what can be mistaken for it? |
Bacteria in the blood and can be mistaken for stain precipitate (Needs to be pretty concentrated to see) |
|
|
What are myeloid and myelocytic referring to? |
Myeloid: Non-lymph WBCs Myelocytic: Granulocytic WBCs |
|
|
Alterations in granulocyte number and maturity are usually caused by? |
-Malignancy -Leukomoid reaction |
|
|
What is the difference between the storage pool in the bone marrow and the marginal pool in the peripheral blood for PMNs? |
Shift from marginal pool is immediate (example bacterial infection), but shift from storage pool requires maturation, so takes longer |
|
|
What are the two categories of macrophages? |
Free: found in body fluids, sites of inflammation Fixed: tissue macrophages found in specific sites (examples: microglial cells, Kupffer cells) |
|
|
What is the normal development of plasma cells? |
(Lymphoblast, Prolymphocyte, B Lymphocyte) Activated B lymph --> Plasmacytoid lymph (Ab production) --> Plasma cell (Ab release) |
|
|
When are plasma cells seen in peripheral blood? |
Normally they are not seen. Often seen in during long-term infections, chronic allergic syndromes |
|
|
What is a plasmablast? |
A B-lymphoblast malignant clone that produces antibody (Immature plasma cell- not normal) |
|
|
What is a proplasmacyte? |
A B-prolymphocyte malignant clone that produces antibody (Immature plasma cell- not normal) |
|
|
What is the pathological development of plasma cells? |
Plasmablast --> proplasmacyte --> plasma cell (antibody production occurs at all stages) |
|
|
In certain pathological states, plasma cells can undergo morphological changes when producing antibody. Five examples are... |
-Flame cell -Russell bodies -Giant cell size -Multinucleated -Rouleaux of RBCs |
|
|
What is endomitosis? |
Nucleus matures and divides, but cytoplasm does not |
|
|
What is necessary for platelet function that the megakaryocyte must have? |
Granules |
|
|
What are the normal stages of myelopoiesis for the myelocytic series (neutrophil model)? |
Myeloblast Promyelocyte Myelocyte Metamyelocyte Band PMN |
|
|
What is the normal development of megakaryocytopoiesis? |
Megakaryoblast Promegakaryocyte Megakaryocyte Thrombocyte |
|
|
What causes primary thrombocytosis? |
Malignant proliferation of platelets |
|
|
What causes secondary thrombocytosis? |
Congenital, reactive (to cytokines) In response to: trauma, blood loss, tissue destruction, inflammatory disease, exercise, etc. |
|
|
What are two forms of thrombocytopenia? |
-Decreased production -Increased consumption (destruction of platelets) |
|
|
Bone marrow is typically comprised of... |
50% cells and 50% fat |
|
|
What are the typical indications for a bone marrow exam? |
-To monitor course of disease/effectiveness of treatment (example: monitor leukemia) -Confirm suspected diagnosis |
|
|
What are some examples of diseases states that require bone marrow exam for diagnosis? |
-Lipid metabolism disorders -Tumor metastasis -Pancytopenia -Aplasia -Thrombocytopenia -Lymphomas |
|
|
What is the ideal site for bone marrow aspiration? |
Iliac crest (Another typical site is the sternum, but more traumatic) |
|
|
How do you make a bone marrow direct aspirate smear? |
Pull prep method: -Blood on slide at angle, leave spicules -Sandwich w/another slide, push and pull apart (Note: Make as many as fast as possible before needing to place in preservatives) |
|
|
What preservatives are typically used for bone marrow aspirates and for what test disciplines? |
EDTA- Flow cytometry, molecular studies Sodium heparin- Cytogenetics |
|
|
How do you prepare a slide of a bone marrow biopsy? |
Touch prep method: -Touch slide to piece of core biopsy tissue (Allows cells to come out in the same configuration as they were in the bone marrow in body) |
|
|
What is a focal infiltrate in the bone marrow? |
Localized aggregates of potentially malignant cells |
|
|
What is performed/counted in marrow interpretation? |
Low power (100X) -Cellularity, Megakaryocyte estimate (3-6/lpf), Scan for focal infiltrates Oil immersion (1000X) -Confirm focal infiltrates, differential, M:E ratio |
|
|
What is the normal cellularity for bone marrow and what specimen is it performed on? |
Normal ratio of fat to hematopoietic tissue is 50:50 Performed on touch prep of biopsy specimen on 100X |
|
|
How do you perform a bone marrow differential? |
Performed on aspirate smears and count 300-1000 cells (count nRBCs too - note stages) (Note: need to count so many to get an adequate sense of distribution-usually "like" cells are in clumps) |
|
|
What is the M:E ratio? |
Myeloid to Erythroid ratio Reference range- 3:1 or 4:1 (Note:myeloid=lymphocytes excluded from ratio) |
|
|
What is the normal concentration of lymphocytes and plasma cells in bone marrow? |
Lymphocytes are usually few in number Plasma cells can comprise ~5% of WBCs |
|
|
What is an osteoblast and what cell type does it look similar to? |
Bone forming cell Looks like a plasma cell (slightly larger, very eccentric nucleus, halo separate from nucleus) |
|
|
What is an osteoclast and what cell type does it look similar to? |
Bone break down, reabsorption Looks like a megakaryocyte (multinucleated, nuclei round and separate from each other) |
|
|
What are the physical characteristics of fat cells in bone marrow? |
Very large, pale, pink, nongranular cytoplasm with very small single nucleus Extremely fragile, usually destroyed in slide prep Leave large empty spaces |
|
|
What is a mast cell and what is associated with increased numbers in bone marrow? |
Tissue basophil (looks similar to blood basophil) Increased in: -chronic infections -autoimmune diseases -systemic mastocytosis |
|
|
What do you look for when staining bone marrow for iron stores and what stain do you use? |
Prussian blue stain -3 to 6 iron laded macrophages (nurse cells)/lpf -rbc precursors (normal is 20-50% RBCs contain iron granules) |
|
|
What is a siderocyte? |
Non-nucleated RBC with Fe granules |
|
|
What is a sideroblast? |
Nucleated RBC with Fe granules |
|
|
What are indications of sideroblastic anemia? |
Increased siderocytes OR Ringed sideroblasts |
|
|
Increased iron can be defined as... |
Increased number per field OR Increased intensity (increased blue) |
|
|
What is a nurse cell? |
A centrally located macrophage, surrounded by a ring of erythroid cells, that may provide substances for growth for the erythroid cells |
|
|
What is an erythroblastic island? |
The collective structure of a nurse cell surrounded by erythroid cells |
|
|
What is characteristic of Alder-Reilly anomaly? |
Prominent red to purple granules in all WBCs (occ surrounded by halo) (Note: Difficult to distinguish between toxic granulation or can look like normal granules) |
|
|
Abnormal red to purple granules in WBCs is found in what disorder? |
Alder-Reilly anomaly |
|
|
What type of disorder is Alder-Reilly anomaly and what are possible manifestations? |
Manifestation of rare, inherited recessive disorders -Enzyme deficiency for breakdown of mucopolysaccharides -Gargoylism (Hunters of Hurlers syndrome) |
|
|
What is characteristic of Chediak-Higashi syndrome? |
-Giant lysosomes in most cells of the body -Abnormally formed lysosomal granules in WBCs -Decreased platelets with large granules and defective function |
|
|
A person with what syndrome can expect a shortened lifespan due to increased susceptibility to infection and bleeding problems? |
Chediak-Higashi syndrome |
|
|
What type of disorder is Chediak-Higashi syndrome? |
Rare autosomal recessive disorder |
|
|
What disorder would you suspect if you saw giant, bizarre platelets and Dohle like bodies? |
May-Hegglin anomaly |
|
|
What is the manifestation of Chronic Granulomatous disease? |
Defective NADPH oxidase so cannot generate superoxide/respiratory burst. (Note: Normal looking phagocytes that can phagocytize bacteria, but can't kill them) |
|
|
What is the diagnosis for Chronic granulomatous disease? |
-Nitroblue tetrazolium test Precipitation=normal No precipitation=defect/absence of enzyme -Flow cytometry |
|
|
What is the manifestation of Myeloperoxidase deficiency (MPO)? |
Neutrophils have decreased enzymes so longer killing time of bacteria (Note: cells look normal) |
|
|
What conditions associated with WBC abnormalities have normal appearing WBCs? |
-Chronic granulomatous disease -MPO |
|
|
What is the cause of MPO? |
Gene mutation |
|
|
What is usually seen with increased plama cells? |
Rouleaux due to increased protein... |
|
|
What is the Diabetes mellitus associated dysfunction? |
-Poor neutrophil function -High glucose levels result in abnormal oxidative burst |
|
|
What characterizes leukocyte adhesion disorders? |
Inability of neutrophils and monocytes to adhere to endothelial cells and migrate from blood to tissues |
|
|
What causes leukocyte adhesion disorders? |
Gene mutation
|
|
|
What is the associated result of leukocyte adhesion disorders? |
Increased, potentially lethal bacterial infections |
|
|
What characterizes Lazy leukocyte syndrome? |
-Cells cannot respond properly to chemotaxins -Cells have poor directional and random movement |
|
|
What characterizes hairy cell leukemia and what type of condition is it? |
Few to many "hairy" cells A malignancy of WBC variants |
|
|
What is a hairy cell? |
A "confused" cell of B-lymphocyte origin with monocytic qualities |
|
|
What are the lab findings associated with Hairy cell leukemia? |
-Splenomegaly (enlarged spleen) -Moderate to severe pancytopenia (<4000/mm3) -Few to many hairy cells -TRAP stain positive |
|
|
What is Sezary syndrome? |
Malignancy of cells that appear as mature lymphs with convoluted, cerebriform nuclear folds |
|
|
What type of condition is Gaucher's disease? |
Lipid storage disease
Enzyme deficiency of beta-glucocerebrosidase |
|
|
What type of disorder is Niemann-Pick disease? |
Lipid storage disorder Enzyme deficiency of sphingomyelinase |
|
|
What condition is associated with "foam" cells? |
Niemann-Pick disease |
|
|
What is a foam cell? |
Large macrophage with bubbly appearance (bubbles are NOT distinct like vacuoles) |
|
|
What type of condition is Tay-Sachs disease? |
Lipid storage disorder Enzyme deficiency of hexosaminidase A |
|
|
What condition is associated with vacuolated lymphs? |
Tay-Sachs disease (and other conditions) NOT diagnostic |
|
|
What disease is associated with a beta-glucocerebrosidase deficiency? |
Gaucher's disease |
|
|
What disease is associated with a sphingomyelinase deficiency? |
Niemann-Pick disease |
|
|
What disease is associated with a hexosaminidase A deficiency? |
Tay-Sachs disease |
|
|
What is a mott cell? |
Plasma cell with abnormal immunoglobulins packaged up into bubbles |
|
|
What are auer rods? |
Abnormally formed lysosomal granules Usually seen in malignant cells (usually myeloblasts and monoblasts) |
|
|
What is physiologic leukocytosis? |
Transient, "normal" increase in WBC, generally not associated with a specific pathology |
|
|
What is the main function of a neutrophil? |
Phagocytic granulocyte Primarily to deal with bacterial infections |
|
|
What is the main function of an eosinophil? |
Granulocyte Primarily to deal with parasitic infections, allergic reactions |
|
|
What is the main function of a basophil? |
Granulocyte Primarily to aid in inflammatory response |
|
|
What is the main function of a monocyte? |
"Garbage" collector - phagocytize bacteria, etc. |
|
|
What are the main functions of lymphocytes? |
Mediators in nearly all immune responses and deal with viral infections |
|
|
What are Russell bodies? |
Abnormal, large, homogeneous, immunoglobulin containing inclusions usually found in plasma cells |
|
|
Define petechia. |
Small, red or purple spot on the skin caused by a minor bleed (broken capillary) |
|
|
Define purpura. |
Rash of purple spots (4-10mm diameter) on the skin caused by internal bleeding (of small blood vessels) |
|
|
What is TPO, where is it made, and what is its function? |
-Thrombopoietin
-Made in the liver and spleen -Regulates platelet production by inhibiting megakaryocyte apoptosis (Binds to platelets and is degraded, so if plts low, more TPO, and more inhibition of apoptosis) |