![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
Gonorrhea & Chlamydia: Comparison |
-2 most common bacterial STDs -bacteriologically very diff -similar clinical syndromes: "Inflammatory STDs" -Cannot be distinguished clinically
|
|
|
Gonnorhea- Physiology & Structure
|

-Gram--, "coffee bean": aerobic diplococcus w/ adjacent flattened sides
-*Note: Neisseria meningitidis & Neisseria gonorrheae are only clinically important Gram--- cocci -Fastidious: requires special media & 5% CO2 for culture isolation |
|
|
Gonorrhea- Virulence Factors |
|
|
|
Gonorrhea: Pathogenesis |
-Attaches to mucosal cells via pill & penetrates into cells -Establishes infection in sub epithelial space -Lipooligosaccaharide stimulates inflammatory response
|
|
|
Gonorrhea- Epidemiology |
-Humans are only natural host -always a pathogen - never commensal -route of transmission: direct mucosal contact w/ infected mucous membrane/fluids -does not survive well outside body |
|
|
Gonorrhea Epi- Symptomatic or Not? |
-90% of males --> symptomatic within 5-7 days -50% of females --> symptomatic within 2 wks -screening is essential! |
|
|
Gonorrhea- Lab Diagnosis |
-gram stain or urethral discharge -Culture:
-Non-culture based diagnostics: BEST, highly specific, low cost
|
|
|
Gonorrhea- Tx |
Ceftriaxone: (3rd generation cephalosporin) only reliable drug -1/3 of gonococcal isolates- resistant to PCN, tetracycline, ciprofloxacin -Always treat for chlamydial co-infection bc you can't distinguish clinically |
|
|
Chlamydia- Physiology and Structure |
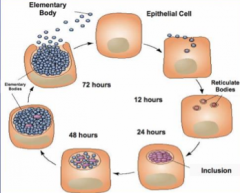
-obligate intracellular bacterium -Small Gram--- bacillus -Chlamydia Trachomatis (CT)- various serotypes
-Requires living tissues or cells for culture -exists in 2 forms:
|
|
|
Pathogenesis & Immunity |
-EB enters cells at mucous membranes, replicates, and infects outer cells -causes cellular destruction -Inflammatory host immune response: granulocytes, lymphocytes, plasma cells -No lasting immunity: re-infection is common and together w/ inflammation can lead to end organ damage (blindness- destruction of eye cells, sterility- destruction of FTs) |
|
|
Epidemiology |
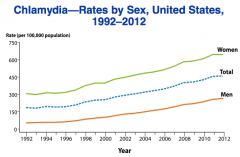
-Humans- only natural human host -Route of transmission: direct mucosal contact w/ infected mucous membranes/fluids -Most commonly reported ID in US -Difference bw men & women: largely explained by screening techniques focused on women |
|
|
"The Silent Epidemic" |
-75% of female & 50% male infections- asymptomatic -can persist as long as 2 yrs in female genital tract --> then cause Silent PID -asymptomatic infection- thought to be primary reason for tubal infertility -SCREENING ESSENTIAL! |
|
|
Lab Diagnosis |
-Non-culture based diagnostics = gold standard -POCT (point of care testing) available -Single swab to distinguis GC & CT |
|
|
Tx |
Azithromycin: single dose Doxycycline: -both equally efficacious, Azithromycin preferable bc single dose
|
|
|
Urehtritis |

-caused by both GC & CT S/S: dysuria, discharge, burning of urethra Exam: discharge varies in color and amount Diagnosis: Gram stain -Intracellular Gram--- diplococci: GC -WBCs w/ no organisms: NGU, caused often by CT
|
|
|
Non-Gonoccoal Urethritis (NGU) |
Etiology -50% - chlamydida Diagnosis: -discharge, Gram stain, leukocytes esterase on urine dip, or U/A |
|
|
Epidiymtis |

-Subacute onset of pain, swell in, erythema or scrotal sac, usually unilateral -Exam: tenderness -may not see concurrent urethritis -young sexually active males almost always GC or CT- but MSM may also get from E. Coli -Diagnosis: clinical w/ Gram stain/test coonfirmation |
|
|
Mucorpurulent Cervicitis |
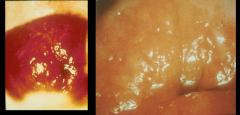
*Women -Often asymptomatic -cause by GC, CT, both or neither S/S: cervical mucopurulent discharge (not vaginal!), dyspareunia (painful sex), bleeding, dysuria, lower abdominal pain Exam: friability (tissue is easily torn apart), edema, erythema (redness), endocervical discharge, or normal appearance (though positive test) Diagnosis: -clinical - Positive swab test -Gram stain: has too of low sensitivity (not usually done) -Cultures/test to confirm diagnosis
|
|
|
Pelvic Inflammatory Disease |
-S/S: Salpinigitis, tubo-ovarian abscess, endometritis, or peritonitis -10% need surgery -1/4 women w/ PID develop chronic sequelae |
|
|
PID: Chronic Sequelae |
-Antimicrobial therapy has no effect on subsequent rates of sequelae
-Ectopic pregnancy: 7-fold increased risk -Infertility: 10-15% risk -Chronic pelvic pain |
|
|
Microbio of PID |
N. gonorrheae, CT, Anaerobes, Gram-- aerobes, ureaplasma spp & mycoplasma spp |
|
|
Fitz-Hugh Curtis Syndrome |

-unusual complication where organisms goes out of FT thru fimbriae into peritoneum --> cause violin-like striations bw peritoneum and external liver wall -Chlamydia infection |
|
|
Gonococcal infections at other sites |

Pharyngitis: often asymptomatic, non-exudative, but may see erythema Conjunctivitis: pain, erythema, discharge Exam: Gram stain discharge Perirectal: tenesmus, pain, discharge, Exam: friable mucosa w/ discharge
|
|
|
Disseminated Gonococcal Infection |

-result of gonococcal bacteremia -may present as:
-culture all exposure sites -Treat w/ IV cetriaxone intially -change ot oral therapy after 7-10 days |
|
|
Lymphogranuloma Venereum |

-caused by L1-L3 serovars of CT -Endemic in Africa, India, SE Asia, etc -LGV outbreak in Netherlands - 2004 -*MSM: primary concern S/S: -Inguinal lymphadenopathy -Proctitis (rectum lining)
|
|
|
"Reiter's Syndrome" aka Reactive Arthritis
|
-More common after CT than GC
-S/S: Classic triad 1. Arthritis 2. Conjunctivitis 3. Urehtritis -Also skin lesions: 1. keratoderma blenorrhagicum: start in soles & feet but may spread to scrotum, etc 2. Circinate balanitis: |